
Abstract
Background
Exercise oscillatory ventilation in chronic heart failure has been suggested as a factor related to adverse cardiac events, aggravated prognosis and higher mortality. Exercise training is well known to affect exercise capacity and mechanisms of pathophysiology beneficially in chronic heart failure. Little is known, however, about the exercise training effects on characteristics of exercise oscillatory ventilation in chronic heart failure patients.
Design and methods
Twenty (out of 38) stable chronic heart failure patients exhibited exercise oscillatory ventilation (age 54 ± 11 years, peak oxygen uptake 15.0 ± 5.0 ml/kg per minute). Patients attended 36 sessions of high intensity interval exercise. All patients underwent cardiopulmonary exercise testing before and after the programme. Assessment of exercise oscillatory ventilation was based on the amplitude of cyclic fluctuations in breathing during rest and exercise. All values are mean ± SD.
Results
Exercise training reduced (P < 0.05) the percentage of exercise oscillatory ventilation duration (79.0 ± 13.0 to 50.0 ± 25.0%), while average amplitude (5.2 ± 2.0 to 4.9 ± 1.6 L/minute) and length (44.0 ± 10.9 to 41.0 ± 6.7 seconds) did not change (P > 0.05). Exercise oscillatory ventilation patients also increased exercise capacity (P < 0.05).
Conclusions
A rehabilitation programme based on high intensity interval training improved exercise oscillatory ventilation observed in chronic heart failure patients, as well as cardiopulmonary efficiency and functional capacity.
Keywords
Introduction
The phenomenon of periodic breathing is known to occur at rest, during sleep or during exercise in chronic heart failure (CHF) provoking in each case different disorders in ventilation. Interest has focused on periodic breathing during exercise or else exercise oscillatory ventilation (EOV) in heart failure that consists of cycle fluctuations of waxing and waning in minute ventilation (VE) and it is distinct during cardiopulmonary exercise testing (CPET). 1 The incidence of EOV among CHF patients is about 19–51%. 2 A meta-analysis recently suggested EOV as a significant variable of CPET, which is related to adverse cardiac events, aggravated prognosis and higher mortality. 3 Pathophysiological mechanisms of EOV are based either on increased circulatory delay or increased chemosensitivity due to pulmonary congestion, which both lead to ventilatory instability and periodic breathing. 1
Exercise rehabilitation ameliorates exercise capacity and quality of life and induces benefits in factors related to CHF pathophysiology. 4 So far, studies have shown beneficial effects of exercise rehabilitation on improvement of peripheral myopathy, 5 strengthening of respiratory muscles, 6 reversion of left ventricular remodeling, 7 ameliorating peripheral microcirculation, 8 vascular endothelium,9,10 autonomic nervous system11,12 and respiratory drive at rest and during exercise. 13 All the above could be related to the genesis of periodic breathing. There is now great interest in aerobic high intensity interval training, alone or in combination with strength training, as it has been shown to enhance exercise rehabilitation benefits further.5,7, 9,14,15
However, the beneficial role of exercise training on breathing pattern in CHF patients has not yet been fully investigated. We hypothesised that exercise training would improve characteristics of the EOV pattern in CHF through the improvement of cardiorespiratory parameters. The main aim of this study was to investigate the effects of an exercise rehabilitation programme on characteristics of EOV in CHF patients.
Methods
Study population
Inclusion criteria for study participants were stable systolic heart failure with New York Heart Association (NYHA) functional class III or less and left ventricular ejection fraction less than 50%. Exclusion criteria of the study was moderate-to-severe chronic obstructive pulmonary disease, severe valvular disease and contraindications for performing CPET. 16 All CHF patients were under optimal medication for at least 2 months without any hospitalisation during that time. During the whole intervention period, CHF treatment and medication remained unchanged.
Design of the study
Eligible patients were randomly assigned, as previously described,5,14 to high intensity aerobic interval training or combined high intensity aerobic interval and strength training. The primary end-point of the study was the investigation of exercise training effects on EOV characteristics in CHF patients. The secondary end-point was the exploration of exercise training effects on exercise capacity of CHF patients with EOV. For the purpose of the primary end-point, CHF patients exhibiting EOV were separated from the whole cohort based on quantifying characteristics. The study conformed to the principles outlined in the Declaration of Helsinki. The study was approved by the human bioethics committee of our institution, and informed consent was provided by the participants.
Exercise training programme
Participants exercised three times per week for 12 weeks. If any sessions were missed, the duration of the programme was extended so that the 36 sessions were accomplished. Aerobic and combined regimes have previously been described in detail.5,14 In short, the aerobic group (n = 18) performed 40 minutes of interval training (30 seconds effort – 60 seconds passive rest) at intensities greater than 100% peak oxygen uptake (V
Cardiopulmonary and exercise capacity variables
All CHF patients underwent a maximum, symptom-limited, ramp-incremental CPET on an electromagnetically braked cycle ergometer (Ergoline 800; Sensormedics, Anaheim, CA, USA) at the beginning and the end of the programme, as previously described in detail.
13
Individualised workload increments were estimated according to the equation of Hansen et al.,
17
while respiratory indicators measured breath by breath during CPET with an on-line system (Vmax229D; Sensormedics) were oxygen uptake (V
CPET was used to evaluate a number of variables; these were V
Assessment of EOV and quantification of its characteristics
As recommended by the American Heart Association (AHA) and European Society of Cardiology (ESC), breath-by-breath VE data of CPET were averaged in 10 seconds so as to prevent breath-by-breath signal noise.
21
Determination of the EOV pattern was based on the amplitude of cyclic fluctuations in breathing during rest and exercise (cyclic fluctuations in ventilation lasting ≥60% of exercise duration, with amplitude ≥15% of the average amplitude of cyclic fluctuations at rest, Figure 1). The above definition is a declaration of the AHA and ESC statements21,22 and was originally formulated by Corra et al.,
23
who in turn modified criteria according to the proposal of Kremser et al.
24
Graph plot of a chronic heart failure patient demonstrating the exercise oscillatory ventilation (EOV) pattern. Definition criteria of EOV were: percentage of EOV duration ≥60% of total exercise duration with an amplitude of each oscillation ≥15% of the average amplitude resting value. VE: minute ventilation; h: amplitude of oscillation; λ: length of oscillation.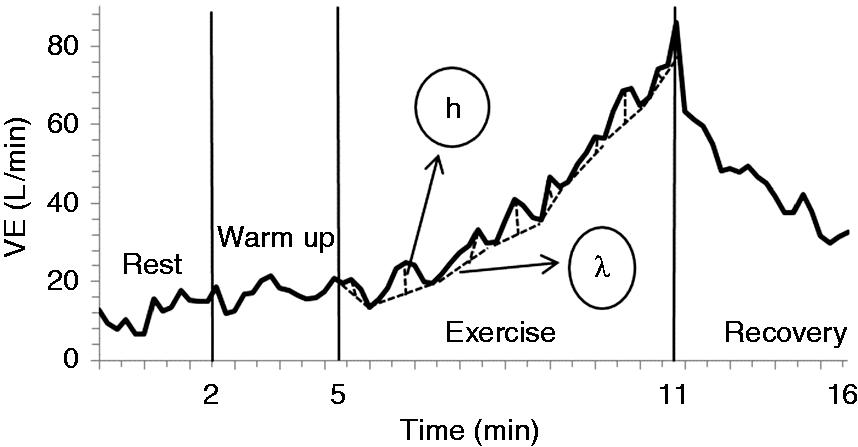
Based on this definition, oscillatory cycles were determined and EOV pattern characteristics were evaluated; these were the percentage of EOV duration, average amplitude and average length of cyclic fluctuations in breathing during exercise. These were manually quantified by using the 10-second averaged VE data. Cycle length duration is defined as the time (expressed in seconds) between two consecutive nadirs. 2 The percentage of EOV duration expresses the percentage of the average duration of oscillatory cycle lengths during exercise. 25 Regarding the amplitude of each cycle fluctuation, this was referred to the difference between the value of peak VE and the average value of the two consecutive nadirs. 2
Statistical analysis
Normality of distribution was estimated by the Shapiro–Wilk test. As far as the demographic, anthropometric and clinical characteristics of CHF are concerned, group means of continuous variables were compared by independent Student’s t-test, while categorical variables were compared by the chi-square test. Comparison within groups concerning EOV characteristics and cardiopulmonary measurements at the start and the end of the exercise rehabilitation programme was based on the paired samples t-test or Wilcoxon signed-rank test, as appropriate. Variable differences between groups were estimated by factorial analysis of variance (ANOVA) 2 × 2 (time × group). Effect size, where appropriate, was calculated as mean of the difference/SD of the difference or was based on η 2 , in the case of ANOVA (G*Power version 3.1.0). All continuous variables are reported as mean ± standard deviation (SD) and categorical variables are presented as frequency or percentage. A P value less than 0.05 was considered statistically significant. Statistical analyses were made with the IBM SPSS 22.0 software.
Results
Demographic, anthropometric and clinical characteristics of CHF patients.
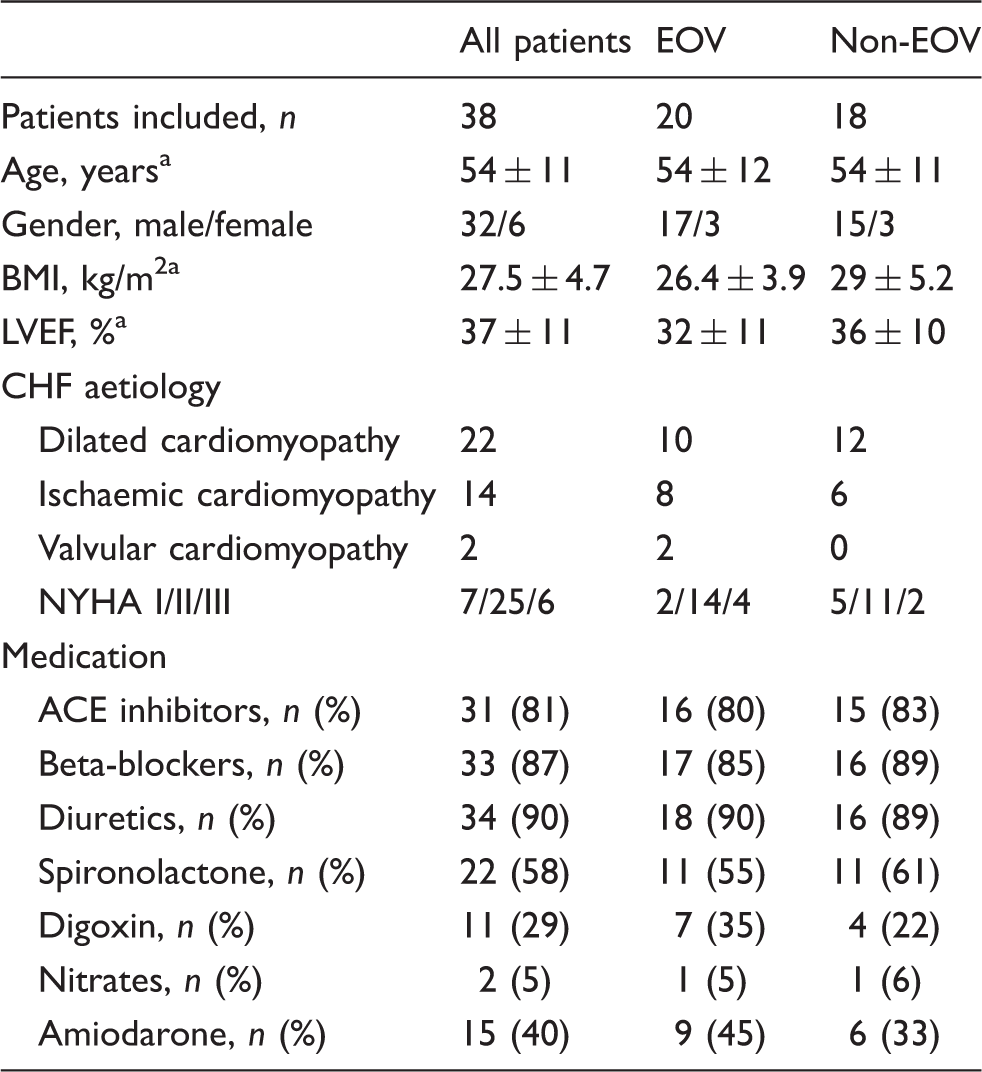
Data are expressed as means ± SD.
CHF: chronic heart failure; EOV: exercise oscillatory breathing; BMI: body mass index; LVEF: left ventricular ejection fraction; NYHA: New York Heart Association; ACE: angiotensin-converting enzyme.
Oscillatory breathing pattern
In the whole cohort of EOV patients, the exercise rehabilitation programme reduced the percentage of EOV duration (79.0 ± 13.0% to 50.0 ± 25.0% of total exercise duration, P < 0.001). An improvement of 29 ± 31% was calculated, corresponding to an effect size of 0.94. No statistically significant change was observed in the average amplitude of cyclic fluctuation breaths (5.2 ± 2.0 to 4.9 ± 1.6 L/minute, P > 0.05), as well as in the average length of these fluctuations (44.0 ± 10.9 to 41.0 ± 6.7 seconds, P = 0.19) (Figure 2). No difference was observed between aerobic and combined groups (P > 0.05) in EOV duration (aerobic 74.0 ± 11.0 to 48.0 ± 23.0%, P < 0.05; combined 83.0 ± 13.0 to 51.0 ± 27.0%, P < 0.05), in average amplitude (aerobic 6.2 ± 1.4 to 5.8 ± 1.8 L/minute, P > 0.05; combined 4.5 ± 2.1 to 4.3 ± 1.2 L/minute, P > 0.05) or in average length (aerobic 49.1 ± 15.1 to 40.8 ± 5.5 seconds, P = 0.09; combined 40.3 ± 5.1 to 41.1 ± 7.6 seconds, P > 0.05).
Graphs of exercise oscillatory ventilation characteristics: (a) percentage of duration; (b) average amplitude; (c) average length (mean ± SD) before and after the exercise training programme in 20 chronic heart failure patients.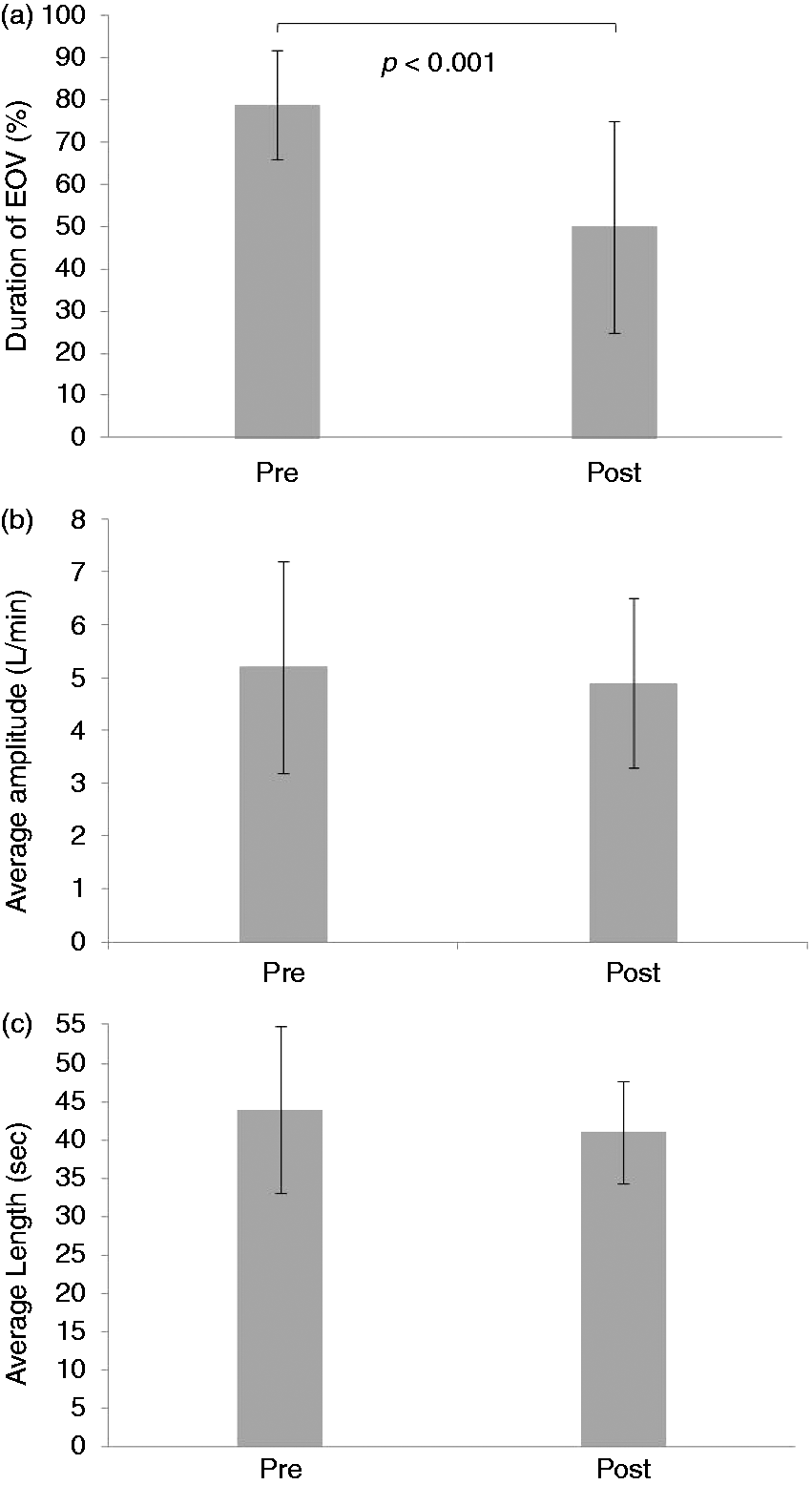
CPET and exercise capacity measurements
Cardiopulmonary testing and exercise capacity variables (mean ± SD) before and after completion of exercise training programme for CHF patients with (n = 20) or without EOV (n = 18).
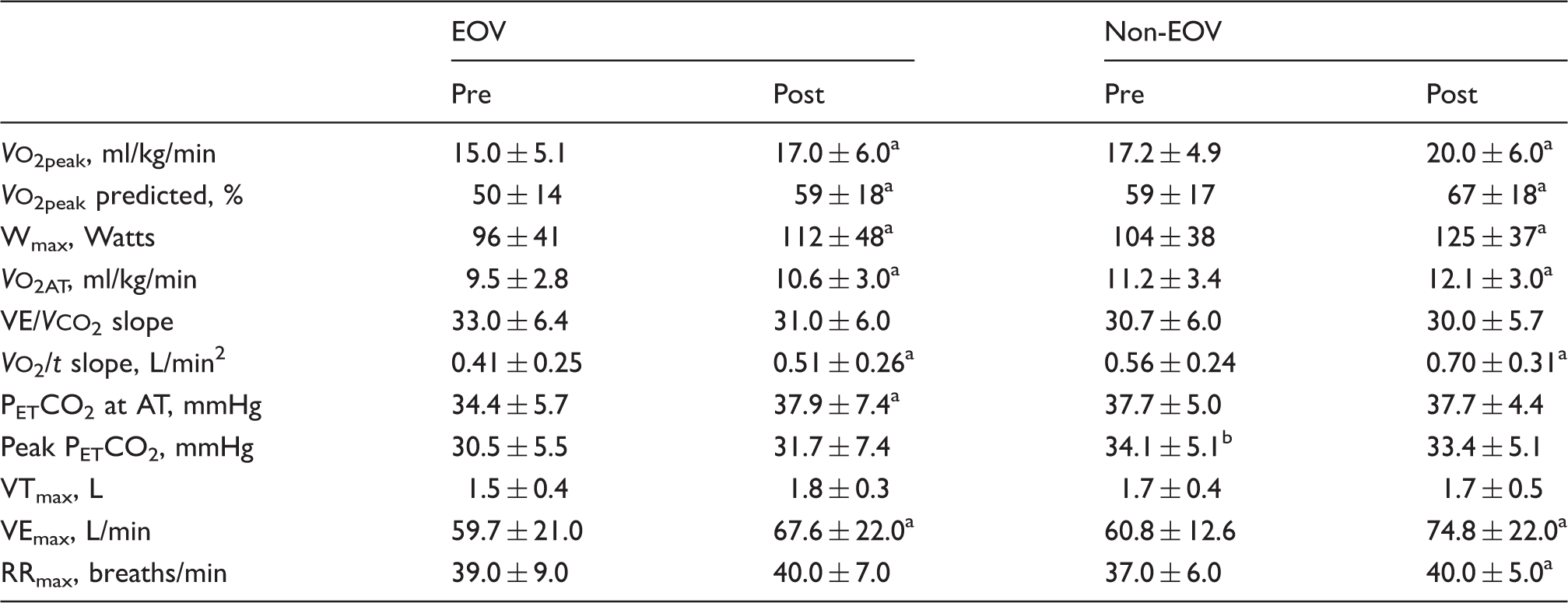
Significant within-group differences (P < 0.05).
Significant between-group differences at baseline (P < 0.05).
CHF: chronic heart failure; EOV: exercise oscillatory ventilation; V
Discussion
This randomised clinical trial investigated the effects of an aerobic high intensity interval exercise regime, with or without strength training, on the oscillatory breathing pattern in CHF patients. Furthermore, description of the oscillatory breathing pattern was based on defining quantified EOV characteristics during CPET; these were the percentage of EOV duration, average amplitude and average length. To our knowledge, this is the first study to explore EOV and exercise effects on heart failure employing these approaches. EOV patients improved the oscillatory pattern after exercise rehabilitation, which is in line with previous studies. Reversal of EOV after an exercise programme has been observed in a case study, 26 and that was also the case in a retrospective study, 27 which observed EOV disappearance in 71% of CHF patients. The latter explored and discussed the role of improvements found in indices of EOV amplitude in rest and exercise. Ιn another retrospective study, a rehabilitation programme reduced EOV amplitude, which was associated with decreased brain natriuretic peptide (BNP) levels, but not cycle lengths. 28 A direct comparison in terms of EOV characteristics, however, does not sound feasible, as in fact different variables and EOV criteria were employed in our study.
Periodic breathing derives from pathophysiological mechanisms, such as delay in transferred information (increased circulatory time, because of impaired cardiac index), 25 increased chemosensitivity to PaCO2 and PaO2, or baroreflex impairment. 29 These mechanisms result in instability of the ventilatory feed-back control system between pulmonary gas exchange capillaries, peripheral chemoreceptors in the carotid bodies and central chemoreceptors in the medulla. 29 In particular, pulmonary congestion has been shown to overstimulate the ventilatory control centre, 30 which increases chemosensitivity, provokes hyperventilation and reduces PaCO2. As a result, hypoventilation supervenes until PaCO2 starts to increase again and hyperventilation restarts.
Exercise training improves microcirculation, endothelial function, inflammation, neuro-hormonal, muscular, ventilatory and peripheral haemodynamic abnormalities,4,5,8,9,11,13,31 finally increasing exercise capacity. The VEmax increase observed in this study most likely reflects an improvement in abnormalities of central and peripheral control of VE. Overall, exercise capacity improvement, in line with other studies, 27 could be related to improvement in haemodynamic disorder (resulting in increased circulatory time), baroreflex impairment and chemosensitivity to PaCO2 and PaO2. These mechanisms could, finally, explain the decrease in EOV percentage after exercise training.
Interestingly, the oscillatory pattern after exercise intervention was improved by decreasing EOV duration rather than the average length and amplitude of oscillated cycles. To some extent, these findings may be related to the sample size; results, especially those on average length, are underpowered to reach definite conclusions. To a much larger degree, these findings are associated with the methodology applied to define EOV. In EOV patients, ventilatory cycles during CPET were determined as oscillated cycles, if amplitude was 15% or greater of the average amplitude of cyclic fluctuations at rest. The average amplitude and length reported is related only to oscillated cycles. The finding of the reduced EOV duration, from 79.0 ± 13.0 to 50.0 ± 25.0%, after exercise training in fact implies that fewer ventilatory cycles of post-CPET were determined as oscillated cycles in comparison to pre-CPET. If all ventilatory cycles (oscillated or not) were considered, average amplitude would most likely be lower and therefore improved; that was the case in another study that examined the effects of exercise training on EOV. 27 Overall, exercise training reduced the number of oscillated cycles; however, in the remaining oscillated cycles, average amplitude and length did not alter. Amplitude and length have been suggested to relate to ventilatory disorders and disturbed circulatory time, respectively;1,2 the exact mechanisms of exercise training benefits remain to be decided.
Another finding was that PETCO2 was decreased in EOV in comparison to non-EOV patients, which might be explained on the basis of lower ventilatory efficiency and exercise capacity due to pulmonary congestion. 32 However, exercise capacity was improved similarly in EOV and non-EOV patients. In addition, although our findings were not observed to support lower ventilatory efficiency in EOV compared to non-EOV patients, this could be related to the small sample size employed. In this study, a high intensity interval regime was applied as the exercise intervention. This kind of training has gained attention in recent years as a modality with the potential to induce superior effects than continuous regimes. 7 Strength training has also been increasingly employed, especially in combination with aerobic exercise, because it can further enhance cardiorespiratory capacity, muscle strength and endothelial function.5,9,14 Strength levels have been associated with CHF prognosis. 33 Strength training can benefit endothelial function and structural remodeling of the vessels when compared to aerobic training alone. 34 A combined regime has also exerted greater benefits on left ventricle function than endurance training. 35 Overall, these findings suggest that the inclusion of resistance regimes to rehabilitation programmes has the potential to optimally affect the benefits of CHF rehabilitation, including haemodynamic disorders and consequently oscillatory breathing. In this study, both exercise regimes were found to improve the oscillatory pattern in terms of the percentage of EOV duration.
Overall, the findings of this and previous studies 27 underpin the role of exercise rehabilitation to act as a non-pharmacological therapy in oscillatory breathing patterns in CHF patients. There is no consensus yet on the definition of EOV and its characteristics, while manual quantification of EOV is time consuming. The development of appropriate software in the future will allow a better exploration of this pathological phenomenon and its consequences on CHF. Future studies could address the optimal modality and exercise characteristics to affect oscillatory breathing patterns, especially in relation to disease severity, and the mechanisms of improvement, as well as exploring EOV in the follow-up period after a rehabilitation programme.
A limitation of the study was the small sample size of patients, and comparison between groups was underpowered to demonstrate differences in EOV pattern characteristics and CPET variables. However, the variable of EOV duration was powered to exhibit a significant improvement in breathing pattern; this was also reflected by the effect size value. Comparison of the different exercise regimes’ effects on the EOV pattern in CHF patients was also underpowered to reach definite conclusions. The lack of a control group (no exercise training) might also be another minor limitation. However, EOV is a poor prognostic indicator in CHF patients, rather unlikely to improve after 3 months of medical treatment and clinical stabilisation. In addition, another recent study did not find any improvement of the EOV pattern on the control group of no training in contrast to the exercise intervention group. 27
In conclusion, an exercise training programme, based on a high intensity interval regime improved periodic breathing during exercise in CHF by reducing the duration of EOV pattern. Moreover, participants improved cardiopulmonary efficiency and functional capacity. The role of exercise modality and characteristics, as well as the mechanisms of improvement, warrant further investigation.
Footnotes
Author contribution
EK, SD and SN contributed to the conception and design of the research. NP, EK, AT, JT and SV contributed to the acquisition of data. NP and SD defined characteristics of the oscillatory pattern and EK contributed to the exercise programme application. Analysis of data and interpretation was done by NP, EK and SN and the drafting of the manuscript by NP and EK. Moreover, AT, JT, SV and AS contributed to the clinical assessment of patients. AS, CG and SN critically revised the manuscript, while CG and SN supervised the study. All authors read and agreed on the final version of the manuscript, while EK and SN gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by the Special Account for Research Grants, National and Kapodistrian University of Athens, Greece.