
Abstract
Background
Smartphone manufacturers offer mobile health monitoring technology to their customers, including apps using the built-in camera for heart rate assessment. This study aimed to test the diagnostic accuracy of such heart rate measuring apps in clinical practice.
Methods
The feasibility and accuracy of measuring heart rate was tested on four commercially available apps using both iPhone 4 and iPhone 5. ‘Instant Heart Rate’ (IHR) and ‘Heart Fitness’ (HF) work with contact photoplethysmography (contact of fingertip to built-in camera), while ‘Whats My Heart Rate’ (WMH) and ‘Cardiio Version’ (CAR) work with non-contact photoplethysmography. The measurements were compared to electrocardiogram and pulse oximetry-derived heart rate.
Results
Heart rate measurement using app-based photoplethysmography was performed on 108 randomly selected patients. The electrocardiogram-derived heart rate correlated well with pulse oximetry (r = 0.92), IHR (r = 0.83) and HF (r = 0.96), but somewhat less with WMH (r = 0.62) and CAR (r = 0.60). The accuracy of app-measured heart rate as compared to electrocardiogram, reported as mean absolute error (in bpm ± standard error) was 2 ± 0.35 (pulse oximetry), 4.5 ± 1.1 (IHR), 2 ± 0.5 (HF), 7.1 ± 1.4 (WMH) and 8.1 ± 1.4 (CAR).
Conclusions
We found substantial performance differences between the four studied heart rate measuring apps. The two contact photoplethysmography-based apps had higher feasibility and better accuracy for heart rate measurement than the two non-contact photoplethysmography-based apps.
Introduction
Mobile electronic devices such as smartphones or tablets are gaining increasing popularity worldwide. Recent estimates suggest 7.7 billion mobile broadband subscriptions in 2020, while the number of smartphone subscriptions is expected to equal about 70% of the world’s population. 1 The ubiquitous use of smartphones coupled with expanding mobile broadband connectivity could change the way healthcare is accessed, monitored and delivered (‘mobile health technologies’, mHealth). mHealth is defined by the practice of medicine supported by portable diagnostic devices. 2 For healthcare systems, the importance of mHealth strategies has been demonstrated as they may play an important role in the control of epidemic disease such as cholera 3 or Ebola. 4 On an individual patient level, mHealth technology can be used, for example, to increase medication adherence5,6 or control of blood glucose levels and insulin doses in patients with diabetes. 7 For cardiac patients, a wide array of smartphone-connected cardiac monitoring devices and health apps for the diagnosis and prevention of cardiovascular disease is available. 8
Overall, it is estimated that the number of health-related wearable sensors will reach 80 million in 2017. 9 To reach the transformative potential of mHealth, validation of the technical capabilities and accuracy as well as the clinical impact of these technologies is needed. 10 As heart rate monitoring is an essential component of almost all clinical situations, in the present study we evaluated the usability and accuracy of four different heart rate measuring apps. The accuracy of the apps was compared to the electrocardiogram (ECG) and pulse oximeter-derived heart rate using medically approved professional devices.
Methods
Basic principles
Photoplethysmography (PPG) is based on the principle that blood absorbs more light than the surrounding tissue. In addition, variations in blood volume (i.e. in systole and diastole) affect the transmission or reflectance of light. 11 These two principles can be used to detect blood flow. The PPG technique is commercially used in pulse oximeters for the determination of arterial blood oxygen saturation (SaO2), achieved by computing the differences of light absorption in the red and infrared range by oxygenated and deoxygenated haemoglobin. 12 In contrast, heart rate detection (but not SaO2 measurement) based on PPG is feasible using only light in the visible range. 11
Two different concepts of measuring heart rate by PPG are known: contact and non-contact PPG. In contact PPG, the subject places a finger on the built-in camera of the phone. The camera is placed directly on the skin and the built-in flash provides the necessary light source in the visible range for reflection by blood cells (Figure 1(a)). In non-contact PPG, the camera is used in the classic way by holding the camera in front of the patient’s face (up to 1.5 m away) without the need for direct skin contact (Figure 1(b)). There is no need for a dedicated light source, ambient light is sufficient.
Two different concepts of measuring heart rate by PPG are know: In contact PPG, the subject places a finger on the built-in camera of the phone directly on the skin and the built in flash provides the necessary light source in the visible range for reflection by blood cells (Figure 1a). In non-contact PPG, the camera is used in the classical way by holding the camera in front of the patients face without the need for direct skin contact (Figure 1b). (a) Contact photoplethysmography; (b) non-contact photoplethysmography.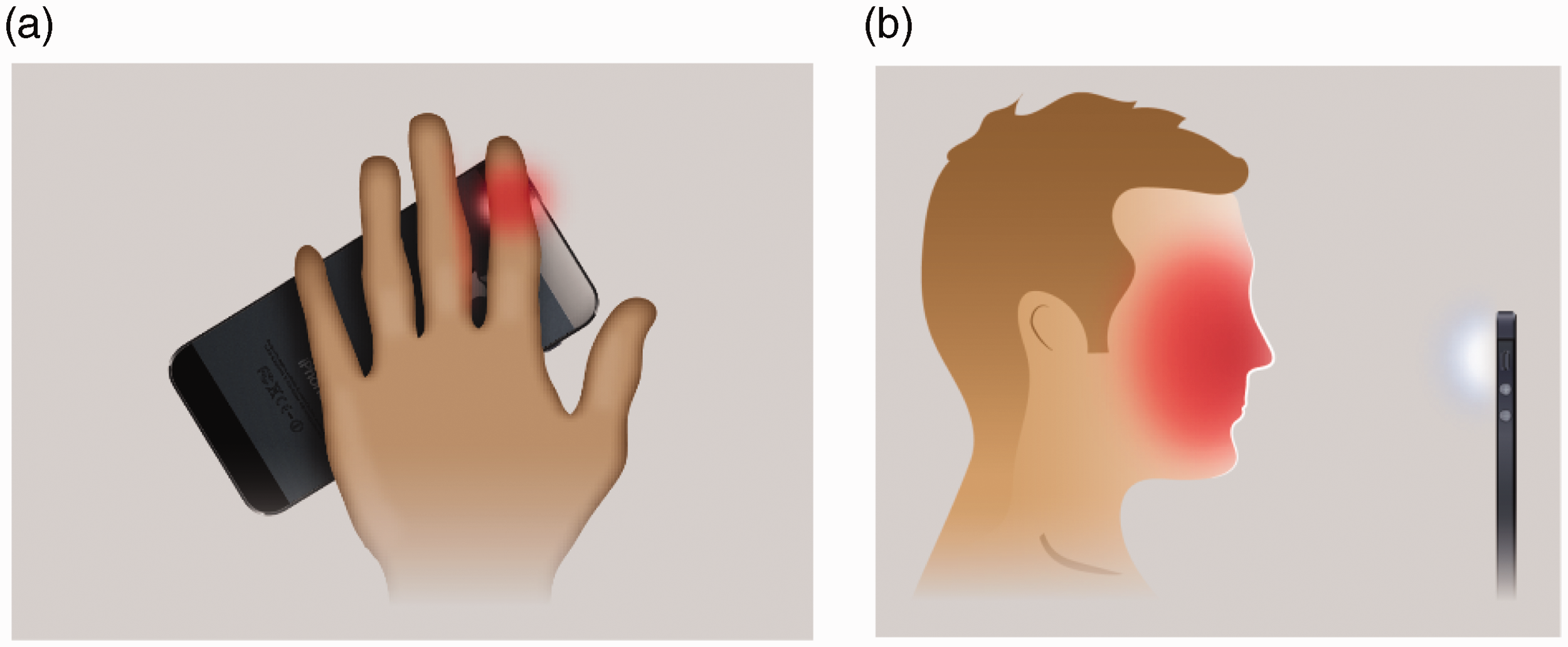
Technology
Applications (apps)
Overall, four commercially available apps have been tested (downloaded from iTunes store). For contact PPG, we used ‘Instant Heart Rate’ (IHR) (version 3.0.1; Azumio Inc., USA) and ‘Heart Fitness’ (HF) (version 2.0.3; Senscare SAS, France). For non-contact PPG, we tested ‘Whats My Heart Rate’ (WMH) (version 2.0; Vitrox Technologies, Malaysia) and ‘Cardiio’ (CAR) (version 2.0; Cardiio Inc., USA).
Mobile devices
Camera specifications.
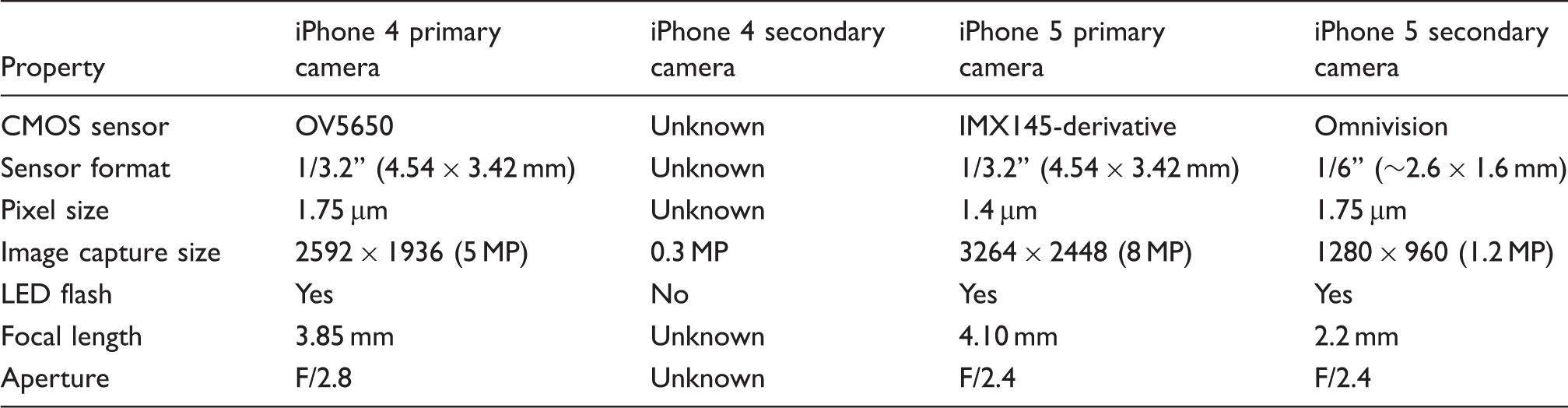
Source: AnandTech. 18
Study population
From April to December 2013 we randomly included adult patients requiring heart rate monitoring on the chest pain unit or the emergency room of the University Hospital Zurich, Switzerland. All patients willing to participate in the study were eligible; however, patients in critical medical conditions were excluded from this study. Patients participating in this study gave written informed consent. The study was approved by the ethics committee of the Canton of Zurich, Switzerland (KEK-ZH-NR: 2012-0524).
After recruitment, initial heart rate and rhythm was measured using a 12-lead ECG (Schiller AT-104 PC/SDS 101 and Schiller AT 102 Plus; Schiller AG, Baar, Switzerland). Heart rate was then measured simultaneously by pulse oximetry (Draeger Infinity Delta XL; Draegerwerk AG & Co. KG, Luebeck, Germany), an ECG-based monitor (Philips Intellivue X2; Koninklijke Philips NV, Amsterdam, the Netherlands) and by each app. The patient history was taken from medical records, and additional clinical characteristics were collected (age, body temperature, blood pressure and blood oxygen saturation). The graphic conceived by Jubran 13 was used for grading of the pulse oximetry curve quality.
Statistics
Continuous data are expressed as medians and interquartile ranges (IQRs) or as mean ± standard deviation (SD) as appropriate, and categorical data as number and percentage (%). Categorical data were analysed using the chi-square test. To compare the values provided by the four apps to the ECG and oximeter-derived heart rate we used Pearson’s correlation and Bland–Altman analysis. To assess the level of agreement between methods we computed the mean absolute error. 14 Linear and multiple regression analyses were performed to test the influence of the defined factors on the mean absolute error of the four different apps. A P value of less than 0.05 was considered statistically significant. Statistical analyses were performed using Stata SE, version 13.
Results
Clinical characteristics
Baseline characteristics of patients (n = 108).
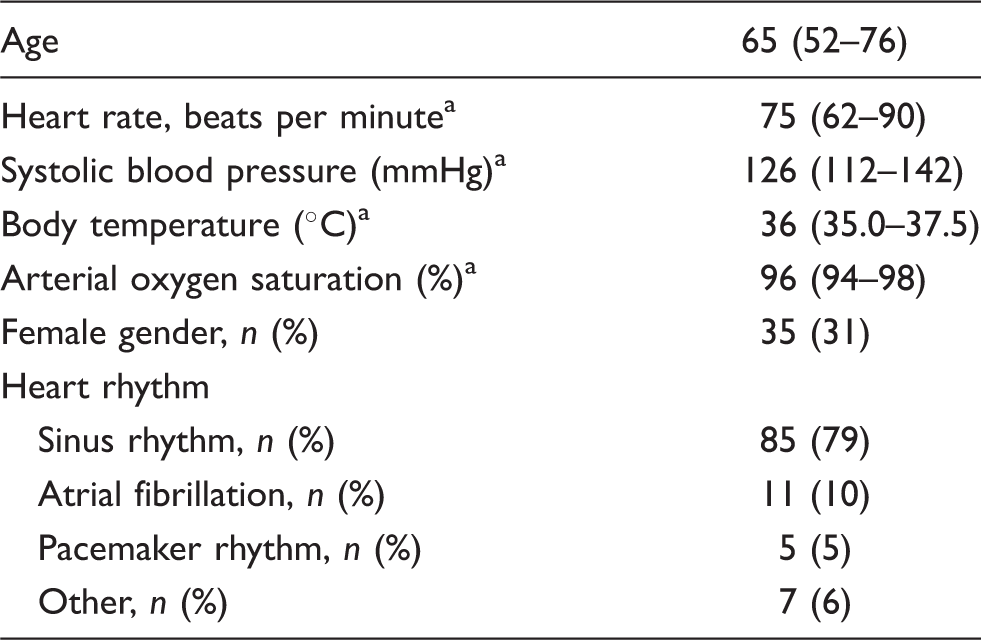
Data given as median (IQR 25–75).
ECG measurements compared to pulse oximetry measurements with approved medical devices
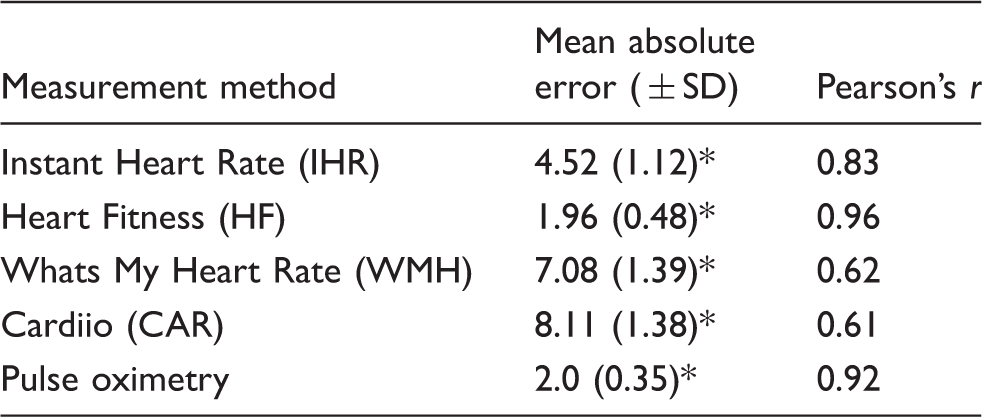
ECG-based measurements compared to heart rate measurement using the pulse oximetry device showed a very high level of agreement (Figure 2, Table 3). Pearson correlation r between the ECG determined heart rate and the oximetric heart rate was 0.92 (P < 0.001), showing a mean absolute error of 2 ± 0.35 bpm.
Heart rate measurement by electrocardiogram compared to pulse oximetry device. Comparison of heart rate assessed by the four different apps and medically approved pulse oximetry compared to electrocardiogram. P < 0.001.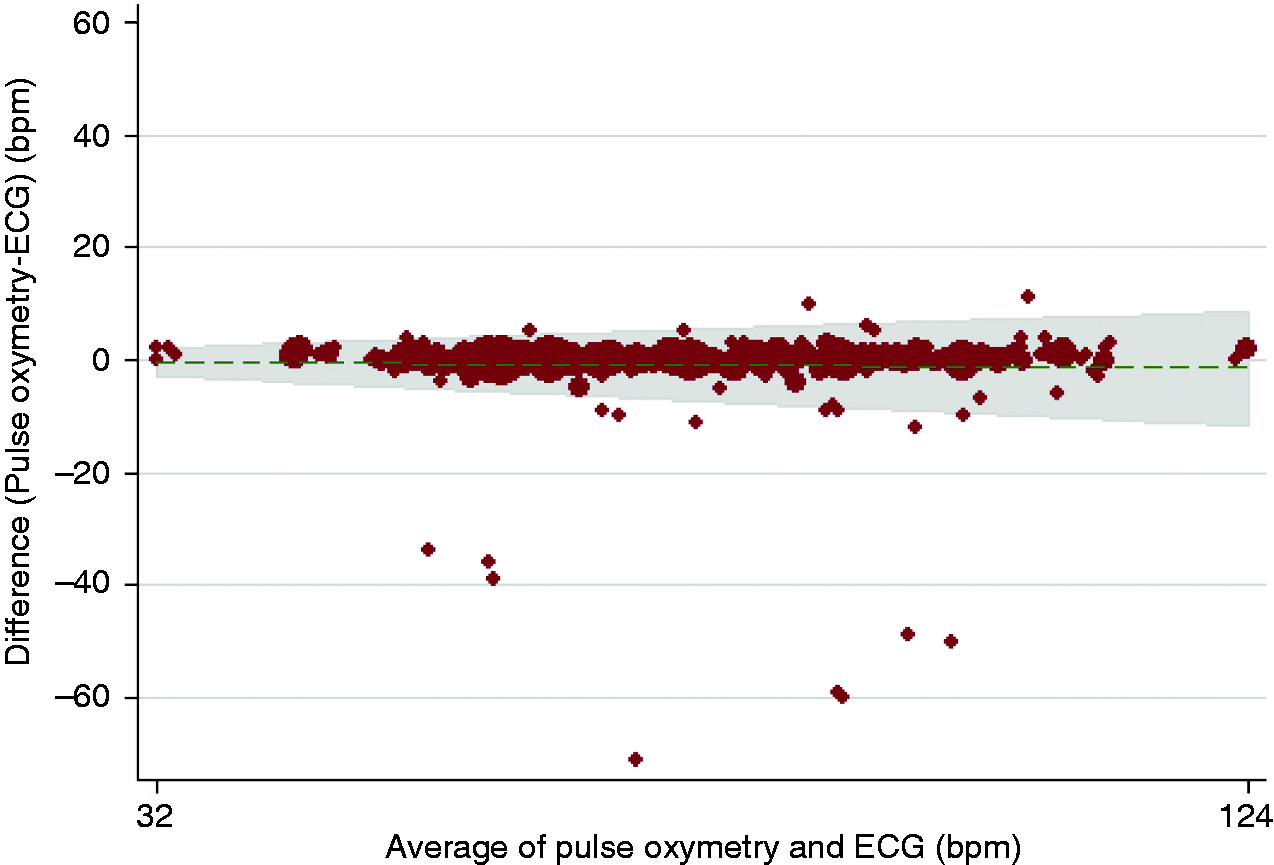
ECG measurements compared to app-based measurements
The accuracy of heart rate measured by apps as compared to ECG, reported as mean absolute error (in bpm ± standard error) was 4.5 ± 1.1 (IHR), 2.0 ± 0.5 (HF), 7.1 ± 1.4 (WMH) and 8.1 ± 1.4 (CAR). The ECG-derived heart rate correlated well with IHR (r = 0.83) and HF (r = 0.96), but less with WMH (r = 0.62) and CAR (r = 0.60) (see Table 3). The Bland–Altman plots (Figure 3) show considerable differences between the tested apps. Non-contact PPG measurements performed significantly worse compared to fingertip-based (contact) measurements. Both non-contact PPG-based apps performed significantly worse at higher heart rates. They also have a tendency to underestimate higher heart rates.
The Bland-Altman plots show considerable differences between the tested apps. Non-contact PPG measurements performed significantly worse compared to contact measurements. Both non-contact PPG based apps performed significantly worse at higher heart rates. They also have a tendency to underestimate higher heart rates. (a) Contact photoplethysmography; (b) non-contact photoplethysmography.
Influencing factors in app-based measurements
Influencing factors in App-based measurements.

P < 0.05.
Discussion
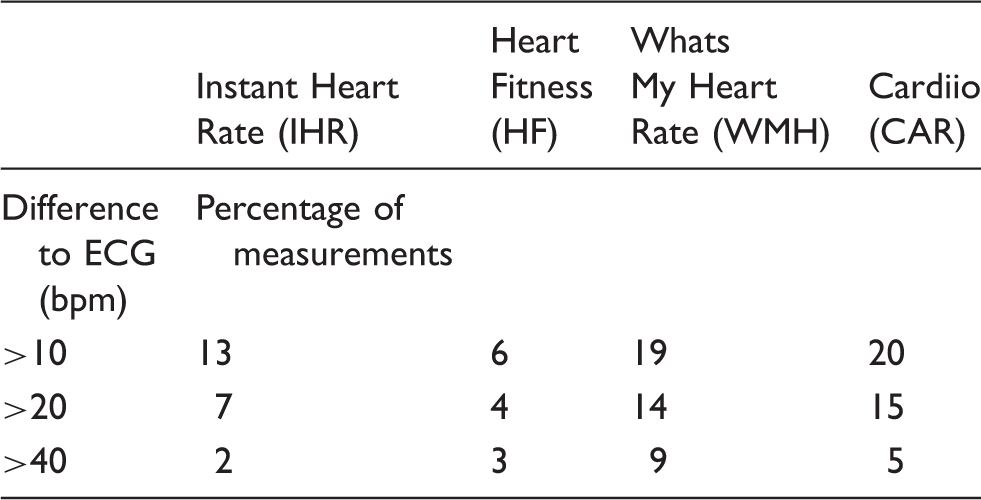
App-performance grouped by differences (bpm) to ECG.
While some apps are developed using evidence-based guidelines and are continuously evaluated, 17 most remain unevaluated. The sheer number of unregulated apps can lead to consumer confusion, reluctant promotion by healthcare providers and unnecessary consumption of healthcare resources. It is largely unclear how we should develop the resources necessary for administrating digital health services and the requirement for healthcare personnel to monitor the wave of incoming patient-generated data. Besides these logistic aspects, several other issues are problematic and need to be addressed (medico-legal liability, personal data safety, health insurance collaborations, reimbursement, incorporation in governmental healthcare systems/programmes, etc.).
Nevertheless, mHealth technologies potentially offer amazing opportunities for patients, healthcare providers, researchers and healthcare delivery systems. To identify the most effective and robust technologies for clinical use it is mandatory to create an evidence base that validates generated measurements and assesses the impact of specific mHealth products and concepts on healthcare quality, cost and outcomes.
Conclusion
We found substantial performance differences between the four studied heart rate measuring apps. The two contact PPG-based apps had higher feasibility and better accuracy for heart rate measurement than the two non-contact PPG-based apps. Careful analysis of app accuracy is warranted before using these apps in clinical practice.
Footnotes
Author contribution
TC, CT, CAW, AB, PB, JH and TFL contributed to the conception of the work. TC, CT, CAW, AB, AAT, FS and SM contributed to the acquisition, analysis, or interpretation of data for the work. TC, CAW and PB drafted the manuscript. All authors critically revised the manuscript, gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgements
The use of the phones in the study was provided by Swisscom for free. At the end of the study, all data were deleted on the phones, and all phones were returned to Swisscom. Measurements were performed by the medical and nursing staff of the cardiology clinic at the University Hospital of Zurich.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.