
Abstract
Aims
To explore the predictive and explanatory factors on the incidence of cardiovascular disease and the impact of visit-to-visit variability (VVV) of risk factors on incident cardiovascular disease in people with type 2 diabetes with no history of prior cardiovascular disease.
Methods
We performed a historical cohort study (2008–2011) on 481 people with type 2 diabetes and no history of cardiovascular disease. Cardiovascular risk factors were assessed at baseline and repeatedly during follow-up. The predictive analysis included the variables at enrollment, and explanatory analyses were based on mean of the variables measured repeatedly. VVV of the main variables was measured using the standard deviation and coefficient of variation of the measured variables. Separate multivariate binary logistic models were constructed for each parameter with the incident cardiovascular disease.
Results
Mean age of the participants was 54.9 years, mean glycated hemoglobin was 56 mmol/mol, and mean blood pressure was 125/78 mmHg. Incident cardiovascular disease developed in 14.3% of the participants. The 2-h post breakfast blood glucose was associated with incident cardiovascular disease (odds ratio 1.44; confidence interval = 1.08–1.90; p = 0.01). For each 1 mmol/l increase in postprandial glucose there was a 44% increase in risk of incident cardiovascular disease. VVV of glycemic indices, blood pressure, lipids, body mass index and creatinine were not associated with occurrence of cardiovascular events.
Conclusion
In this population of patients with type 2 diabetes and no history of cardiovascular disease in whom other cardiovascular risk factors are within or near to the recommended targets, 2-h post breakfast blood glucose level is associated with incident cardiovascular disease.
Introduction
Type 2 diabetes mellitus (T2DM) is a major risk factor of cardiovascular diseases (CVDs), including coronary artery disease, stroke and atherosclerotic peripheral arterial disease (PAD). 1 Common coexisting conditions associated with T2DM, including hypertension and dyslipidemia, are clear risk factors for CVD. 2 CVD is 2–4 times more common in people with T2DM 3 and is associated with a higher morbidity and mortality rate. 4 Furthermore, a number of people with T2DM do not survive their first event, and if they do, their mortality rate over the subsequent years is generally greater than that of the general population. 5 Therefore, primary prevention of CVD in patients with T2DM with no known CVD is a critical issue that requires understanding of the important factors leading to CVD events. 6
Multiple modifiable risk factors for cardiovascular complications, namely hypertension, dyslipidemia, central adiposity and cigarette smoking, are commonly present in people with T2DM.7,8 In a recent study, reduced renal function measured as a decrease in glomerular filtration rate was also shown to be a strong and independent risk factor for cardiovascular events and mortality in patients with T2DM. 9 Another study highlighted the roles of coronary artery calcified plaque and albuminuria as independent predictors of mortality in people with T2DM. 10 However, these studies did not exclude patients with a history of CVD. Many other studies have also evaluated the best predictors for cardiovascular events in individuals with T2DM, but only a few were performed in a real-world setting with repeated measurements of the main known risk factors to determine their impact on the incidence of cardiovascular events.
In addition to the above, intensive glycemic control must be considered in the context of multifactorial risk reduction.11,12 Numerous studies have shown the efficacy of control of the individual cardiovascular risk factors in preventing or slowing the progression of CVD in people with T2DM.13,14 However, large benefits are seen when multiple risk factors are addressed simultaneously.15,16 On the basis of results of such clinical trials, recent international guidelines recommend an intensified multifactorial approach for the treatment of patients with T2DM, although the effect of this approach has not been confirmed in large and multicenter long-term studies. Although there are some evidences with regard to the improvements in risk factor control,17–19 some uncertainty still exists about how aggressively cardiovascular risk factors in patients with diabetes should be treated.20,21 On the other hand, recent clinical evidences have raised the possibility that visit-to-visit glycemic and blood pressure variability independently predict macro-vascular complications and/or all-cause mortality in patients with T2DM.22,23
The present retrospective cohort study is focused on patients with T2DM with no history of prior CVD events. We explored the predictive and explanatory factors of the incidence of CVD and the impact of glycemic variability as well as variability in other known risk factors, namely blood pressure (BP), total cholesterol, low density lipoprotein cholesterol (LDL-c), high density lipoprotein cholesterol (HDL-c), triglyceride, body mass index (BMI) and creatinine on incident CVD in patients with T2DM in a real-world setting.
Materials and methods
We reviewed the electronic medical records of patients with T2DM with no history of CVD who first visited a tertiary care center in Tehran, Iran from 2008 to 2011. Those who had been followed in their routine clinical care setting up to 30 October 2015 and had at least one visit per year were included in this study. T2DM was diagnosed according to the criteria established by the American Diabetes Association. 24 Incident CVD was defined as the first occurrence of fatal or non-fatal myocardial infarction (MI), sudden cardiac death, ischemic heart disease (IHD) including angina and unstable angina, as well as coronary atherosclerosis documented by imaging, heart failure, fatal or non-fatal stroke, transient ischemic attacks, and PAD defined according to the ICD-9 codes 410-440. Clinical data including age, gender, BMI, duration of T2DM, medication, smoking status, glycated hemoglobin (HbA1C), fasting blood sugar (FBS), 2-h post breakfast blood glucose, BP, total cholesterol, LDL-c, HDL-c, triglyceride and creatinine were extracted. These variables were measured at virtually every yearly visit. Documents including electrocardiograms, cardiac angiograms and/or scan, and documents of hospitalization related to any cardiac problem were thoroughly reviewed by one of the authors without knowing the main results of this study. Exclusion criterion was any known CVD prior to the date of enrollment. In addition, other chronic diabetes related complications, including end stage renal disease, proliferative diabetic retinopathy, diabetic foot ulcer as well as different kinds of malignancies were excluded. The follow-up period was defined from the date of the first visit in our clinic (which was not necessarily the date of diagnosis of diabetes) up to the occurrence of the first CVD event or death, or the date of the last visit before the end of the study (30 October 2015).
Separate multivariate binary logistic models were constructed for each parameter, including age, 2-h post breakfast blood glucose, insulin use, BMI and sex with the incident CVD.
To examine the association between incident CVD and variability of the measured variables, we assessed long-term glycemic variability based on variability of HbA1C, FBS and postprandial blood glucose (PPG). In addition, non-glycemic variability was defined as the variability of systolic and diastolic BP, total cholesterol, LDL-c, HDL-c, triglyceride, BMI and creatinine during the study period.
Statistical analysis
Data are reported as mean ± SD for normally-distributed variables and median ± IQR for non-normally-distributed variables or as number and percentage for categorical variables. The predictive analysis included the variables at enrollment. The explanatory analyses utilized the mean of the repeated measured variables during the follow-up period for each individual.
Univariate analysis was performed using Student’s t-test for continuous variables, Mann–Whitney U-test for non-normally-distributed variables, and chi-square test for categorical variables. Based on the outcomes of univariate analyses for each variable with a p value of less than 0.1, multivariate binary logistic regression analysis was performed to assess the independent association between each variable and incident CVD.
In order to test the impact of glycemic and non-glycemic variability on incident CVD, the intrapersonal mean, standard deviation (SD) and coefficient of variation of all recorded measurements (HbA1C, FBS, PPG, systolic and diastolic BP, total cholesterol, LDL-c, HDL-c, triglyceride, BMI and serum creatinine) were calculated for each patient. Statistical significance was considered to be p < 0.05.
Results
Data on 481 patients who had at least yearly measurements of the main glycemic and non-glycemic cardiovascular risk factors during the follow-up of five or more years were included in the analysis. The mean age of the 481 participants was 54.9 ± 10.0 years, the mean diabetes duration was 12.1 ± 6.9 years, and the average BMI was 28.73 ± 4.61 kg/m2. The mean HbA1C was 56 mmol/mol, mean BP was 125/78 mmHg and mean LDL-c was 2.32 mmol/l. The percentages of patients who consumed antihypertensive medications were as follow: 37% one, 16% two, 6% three, and 1% four drugs. Angiotensin modulators were the most common antihypertensive medication used (54%). However, 40% of patients received no antihypertensive medication. The average number of repeated measurements of the main variables during the follow-up period was as follow: FBS = 9.3, 2-h post breakfast glucose = 7.3, Hb1AC = 7.8, systolic and diastolic BP = 6.6, total cholesterol = 6.2, LDL-c = 6.6, HDL-c = 5.3, and triglyceride = 6.7.
Baseline characteristics of the participants.
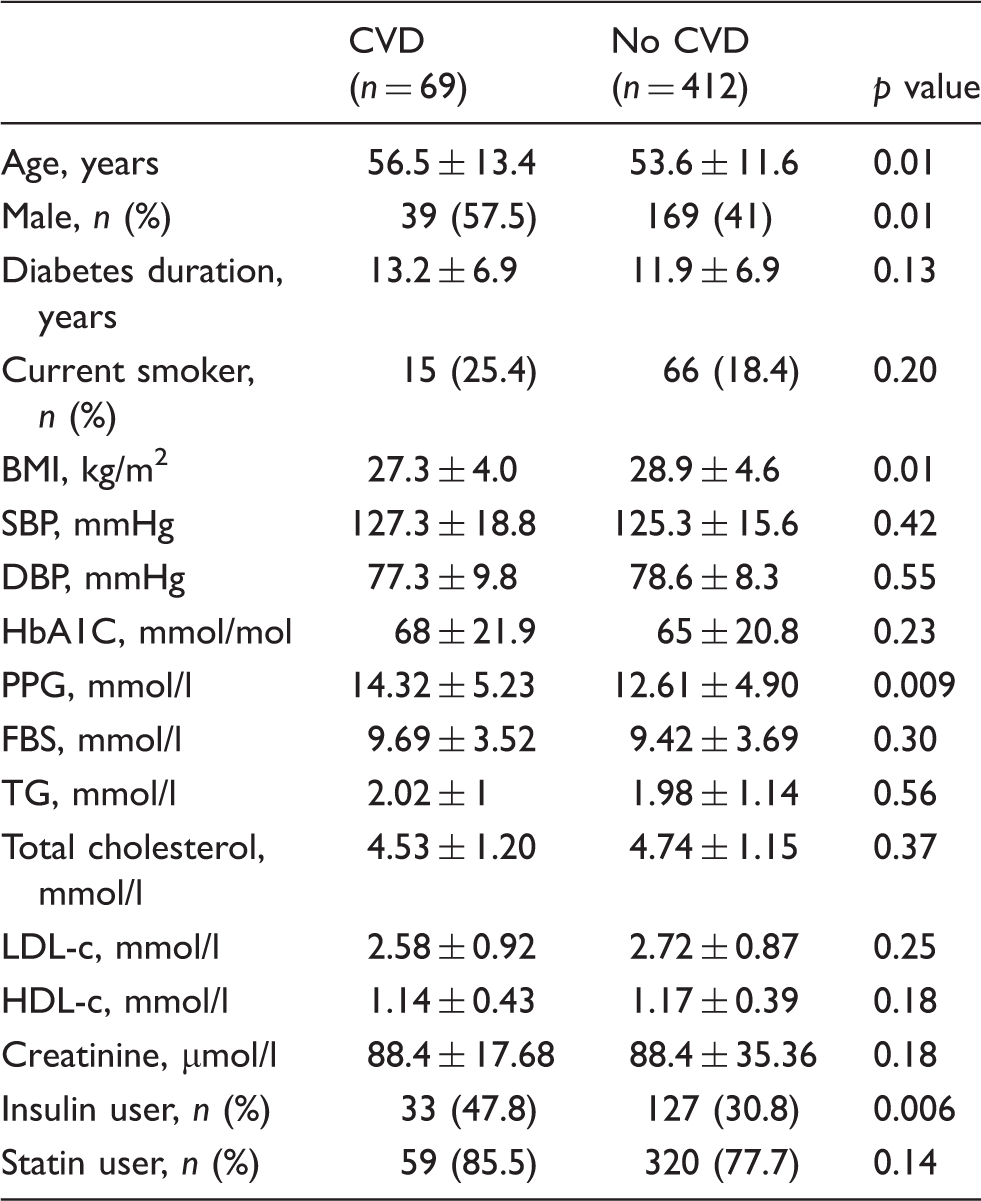
Data presented as mean (SD) or number (%).
CVD: cardiovascular disease; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HbA1C: glycated hemoglobin; PPG: postprandial glucose; FBS: fasting blood sugar; TG: triglyceride; LDL-c: low density lipoprotein cholesterol; HDL-c: high density lipoprotein cholesterol
Binary logistic regression analysis for the association between baseline characteristics and incident cardiovascular disease.
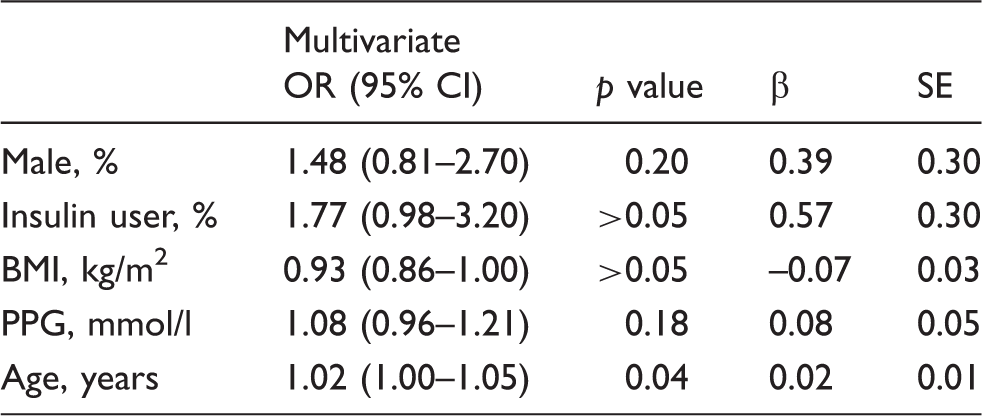
Binary logistic regression analysis, dependent variable is cardiovascular event and covariates are: gender, insulin user, BMI, PPG and age.
OR: odds ratio; CI: confidence interval; SE: standard error; BMI: body mass index; PPG: postprandial glucose
Repeated measurements of the variables during follow-up.
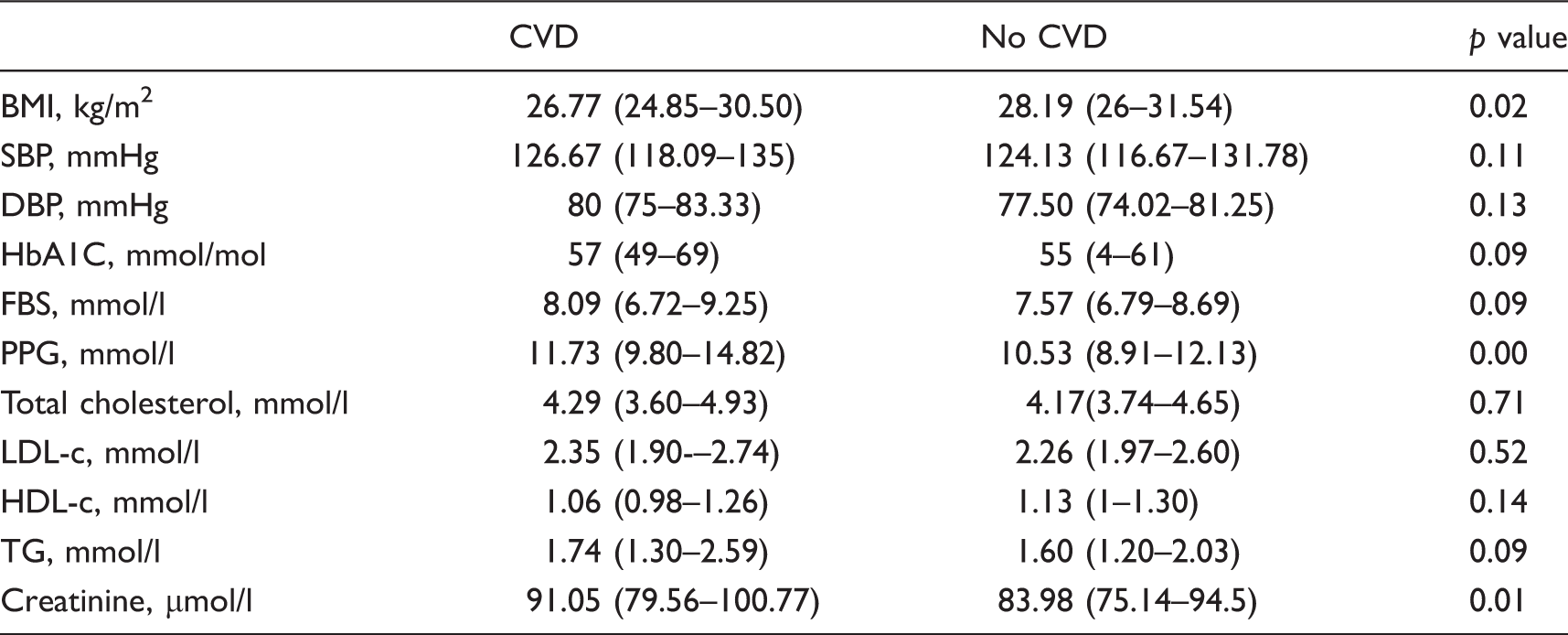
Data presented as median (IQR).
CVD: cardiovascular disease; BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HbA1C: glycated hemoglobin; FBS: fasting blood sugar; PPG: postprandial glucose; LDL-c: low density lipoprotein cholesterol; HDL-c: high density lipoprotein cholesterol; TG: triglyceride
Binary logistic regression analysis between the average value of variables and cardiovascular events during the follow-up period.
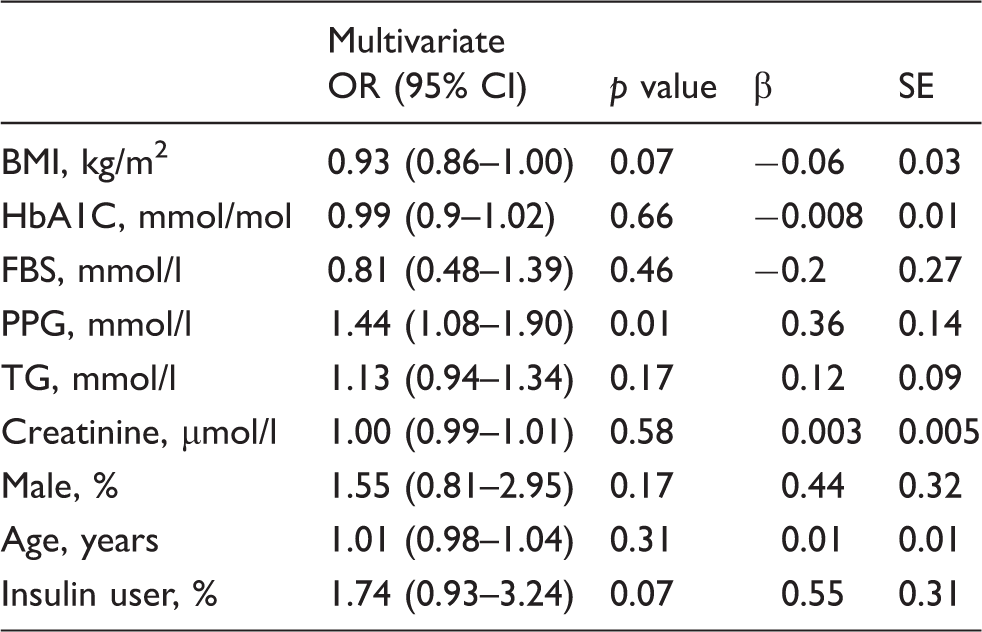
Binary logistic regression analysis, dependent variable is cardiovascular event and covariates are: BMI, HbA1C, FBS, PPG, TG, creatinine, gender, age and insulin user.
OR: odds ratio; CI: confidence interval; SE: standard error; BMI: body mass index; HbA1C: glycated hemoglobin; FBS: fasting blood sugar; PPG: postprandial glucose; TG: triglyceride
We next examined the effect of 2-h post-breakfast blood glucose on CVD outcomes more closely. For each 1 mmol/l increase in PPG there was 44% increase in risk of incident CVD. Also, 73.4% of patients with incident CVD had 2-h post breakfast blood glucose greater than 10 mmol/l compared with 58.3% in the no CVD group (p = 0.017).
Finally, considering the explanatory effect of the main cardiovascular risk factors on all-cause mortality, significantly higher levels of systolic BP (130 vs. 124 mmHg, p = 0.04), HbA1C (66 vs. 55 mmol/mol, p = 0.001) and insulin use (60% vs. 32.6%, p = 0.03) were observed among the individuals who died. However, multivariate binary logistic models did not show any significant relationship between the mean of individual variables and the all-cause mortality. Furthermore, the mean SD and coefficient of variation for all variables showed no difference between the two groups (Supplementary Material Tables 1 and 2 online).
Discussion
Considering improvements in the well-established cardiovascular risk factors in patients with T2DM, including hyperglycemia, reflected in high levels of FBS and HbA1C, hypertension and dyslipidemia that have occurred in the past decades,17–19,25 the role of these risk factors together or individually in regard to incident CVD needs to be re-evaluated.
This historical cohort study, conducted in a real-world setting, showed that the 2-h post breakfast blood glucose level during the follow-up was associated with incident CVD in people with T2DM with no prior history of CVD in whom glycemic and non-glycemic risk factors had been adequately managed for a period of at least five years. In addition, no association was found between visit-to-visit variability (VVV) of HbA1C, FBS, PPG, BP, triglyceride, total cholesterol, LDL-c, HDL-c, BMI, creatinine and incident CVD.
Data from a systematic review showed a progressive relationship between glucose levels and CVD events even for glucose levels below the diabetic threshold. A fasting glucose level of 6.1 mmol/l and 2-h glucose level of 7.8 mmol/l, compared with a glucose level of 4.2 mmol/l, were associated with a relative cardiovascular event risk of 1.33 (95% CI 1.06–1.07) and 1.58 (95% CI 1.19–2.10), respectively. Thus, the fasting blood glucose was an important risk, but the postprandial glucose imposed greater risk, consistent with our finding. 26
Furthermore, some epidemiological studies have shown that the serum glucose level 2 h after an oral challenge test is a powerful predictor of cardiovascular risk.27,28 It is also notable that Smith et al. showed in their study 2-h glucose level is a better predictor of cardiovascular events than fasting glucose level in the elderly. 29 The Diabetes Epidemiology: Collaborative Analysis of Diagnostic Criteria in Europe (DECODE) study showed that there is a continuous relationship between PPG and mortality, but an independent relationship with fasting glucose is only seen above 7.0 mmol/l. 30 In addition, data from some interventional studies support the role of postprandial hyperglycemia in regard to CVD.31,32 The importance of PPG in incident CVD has been verified in more recent studies. 33 The first five years’ follow-up of the San Luigi Gonzaga Diabetes Study demonstrated that PPG (blood glucose level 2 h after lunch) predicts CVD events in patients with T2DM after adjustment not only for the main non-glycemic cardiovascular risk factors, but also for HbA1C. 33 Although our population was different from this Italian cohort, the results are consistent with their finding. However, we documented the predictive value of 2-h post breakfast blood glucose in regard to incident CVD while the San Luigi Gonzaga Diabetes Study did not find any association with 2-h post breakfast blood glucose. This may be due to the fact that ‘breakfast in the Piedmont is frequently a virtual meal, consisting only of a cup of coffee with, sometimes, a small piece of bread’, 33 which is actually a low calorie meal, whereas standard breakfast for Iranian people consists of a larger amount of calories. 34
The extension of the San Luigi Gonzaga Diabetes study showed that the predictive power of PPG in regard to incident CVD persists in the 14-year follow-up. 35 Furthermore, the high predictive power of postprandial blood glucose level in regard to all-cause mortality persisted when the effect of HbA1C was simultaneously taken into account. 35 It is also of significant importance that the International Diabetes Federation considers postprandial hyperglycemia independently harmful, promoting macro-vascular disease and associated with increased carotid intima media thickness, decreased myocardial blood volume and blood flow, oxidative stress, inflammation and endothelial dysfunction. 36
It is important to mention that the contribution of FBS and PPG in achieving glycemic control is relative. In a prospective interventional trial, 64% of patients who achieved FBS < 5.51 mmol/l achieved HbA1c ≤ 53 mmol/mol, whereas 94% of patients who achieved target PPG ≤ 7.71 mmol/l achieved an HbA1c ≤ 53 mmol/mol. 37
Our study confirms the predictive power of postprandial blood glucose in regard to incident CVD even after adjustment for HbA1C and FBS. However, we did not find its predictive role in regard to all-cause mortality, perhaps due to limitation in our sample size and the low rate of mortality. The mean glucose value was 1.20 mmol/l (24 mg/dl) higher in patients who developed incident CVD during the follow-up. In addition, the multivariate analysis showed that for each 1 mmol/l increment in 2-h post breakfast blood glucose level there was 44% increase in the odds of CVD.
The positive and continuous impact of HbA1C on both CVD and total mortality has been established;38,39 however, in the present study, neither FBS nor HbA1C predicted incident CVD. This could be explained by the fact that the mean for both FBS (7.88 mmol/l) and HbA1c (56 mmol/mol) during the follow-up period were very close to the currently recommended targets. Moreover, the reason why the San Luigi Gonzaga Diabetes Study documented the predictive value of HbA1C in regard to incident CVD but we did not may be due to the difference between the populations of these two studies. In the San Luigi Gonzaga Diabetes Study, one-third of the participants had experienced previous CVD events, 33 while any history of CVD was an exclusion criterion in our study. Furthermore, there are still conflicting data with regard to how aggressively HbA1C should be treated to reduce cardiovascular events. Some studies showed benefits from reduction of HbA1C in cardiovascular events and all-cause mortality,40,41 while others did not.42,43 Moreover, a number of studies found a U-shaped relationship between mean HbA1c levels and mortality and cardiac events.44,45 Nevertheless, lower HbA1c and blood glucose levels are universally recommended because of their well-established effect on reducing the development and progression of micro-vascular complications. 46
In addition, we found that when important non-glycemic risk factors, including systolic and diastolic BP, total cholesterol, HDL-c, LDL-c and triglyceride, are adequately controlled, their role in predicting cardiovascular events is diminished and eliminated (as expected). More than 80% of our participants achieved and maintained BP and LDL-c targets simultaneously. In this context, the role of PPG in incident CVD becomes apparent.
Given the significant role of postprandial hyperglycemia in regard to CVD, identification and treatment of the contributors to PPG are of great importance. Low glycemic index diet has a positive effect on cardiovascular risk factors. 47 Similarly does low fiber diet, thus, dietary fiber is essential in the modulation of PPG and in the decrease of other main cardiovascular risk factors.48,49 In addition, consumption of soluble dietary fiber reduces postprandial glucose responses after carbohydrate-rich meals. 50 Furthermore, calorie restriction and weight loss positively impact postprandial dysmetabolism. 51
Considering the impact of postprandial glucose control on prevention of CVD, targeting PPG with various therapeutic agents seems reasonable. There is a variety of agents, including a-glucosidase inhibitors, glinides, short-acting sulphonylureas and rapid-acting insulins, glucagon-like peptide-1 derivatives and dipeptidyl peptidase-4 inhibitors, that by their mode of action act on post-meal hyperglycemia. 36 In choosing a drug for a patient, the efficacy, safety and cost–benefit aspects should be always taken into account. Interestingly, postprandial glucose monitoring motivates patients to improve lifestyle and behavioral parameters that result in increased physical activity and reduced intake of calories, refined carbohydrates and saturated fats. 52
We found no association between VVV of the glycemic and main non-glycemic risk factors measured (HbA1C, FBS, PPG, BP, triglyceride, total cholesterol, LDL-c, HDL-c, BMI, serum creatinine) with incident CVD during the follow-up period. A few studies have explored the association of ‘long-term’ variability in glycemic and non-glycemic measures and CVD. In one study, BP variability strongly predicted all-cause and cardiovascular mortality independently. 53 The large Action in Diabetes and Vascular Disease: PreterAx and Diamicron Modified Release Controlled Evaluation (ADVANCE) trial showed that VVV of systolic BP is an independent risk factor for macro-vascular and micro-vascular complications in patients with T2DM. 54 They also found that glycemic variability is an independent risk factor for macro-vascular events. 22 A more recent study showed that VVV in HbA1c and systolic BP confers an additive risk for the occurrence of cardiovascular events in patients with T2DM. 23 While the reasons for the discrepancy between our finding and the above reports are not clear, potential explanations could include differences in the frequency and methods by which measurements were made. For example, in ADVANCE, VVV was greatly affected by the number of measurements. 22 Another study found that the number and timing of visits as well as the device used to measure BP influenced VVV. 55 Moreover, the interval between measurements of the main variables in our study was not rigidly scheduled. Finally, all measurement of the parameters in our study was performed in the same setting.
The strengths of our study include the repeated and frequent comprehensive risk factor assessment, defining the incident CVD based on rigorous criteria, and reasonable follow-up period. Moreover, this retrospective cohort study was conducted in a real-world setting. However, our study has some limitations, including that it was conducted in a single tertiary care center and did not include a very large number of patients. Also, because ours is an observational study, conclusions cannot be made about the potential cause and effect relationship between post-breakfast blood glucose level and incident CVD; it is also possible that unmeasured confounders contributed to our results. In addition, the impact of post-breakfast blood glucose level on incident CVD was observed in a population who were managed adequately for their main glycemic and non-glycemic cardiovascular risk factors, which might limit generalization to other populations.
Conclusion
In conclusion, this retrospective cohort study that was conducted in a real-world setting in a selective population of patients with type 2 diabetes who had adequate metabolic control showed that 2-h post breakfast blood glucose level is associated with incident CVD.
Footnotes
Author contribution
NHM, MEK and MM contributed to the conception or design of the work. FI-B, MEK, MM, NHM and AEV contributed to the acquisition, analysis or interpretation of data for the work. MEK, MM, NHM and AEV drafted the manuscript. FI-B and MEK critically revised the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgement
We do appreciate the staff of the Endocrine Research Center at Iran University of Medical Sciences (IUMS), especially Dr. Zahra Emami, Ms. Setareh Shamardani, and Ms. Moloud Etemadi for their assistance during our study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded and supported by Iran University of Medical Sciences (grant number 9311330003).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.