
Abstract
Background
Exercise is the cornerstone of rehabilitation programmes for individuals with cardiovascular disease (IwCVD). Although conventional cardiovascular rehabilitation (CCVR) programmes have significant advantages, non-conventional activities such as Nordic walking (NW) may offer additional health benefits. Our aim was to appraise research evidence on the effects of Nordic walking for individuals with cardiovascular disease.
Design
Systematic review and meta-analysis.
Methods
A literature search of clinical databases (PubMed, MEDLINE, Scopus, Web of Science, Cochrane) was conducted to identify any randomized controlled trials, including: (i) individuals with cardiovascular disease, (ii) analyses of the main outcomes arising from Nordic walking (NW) programmes. Data from the common outcomes were extracted and pooled in the meta-analysis. Standardized mean differences (SMDs) were calculated and pooled by random effects models.
Results
Fifteen randomized controlled trials were included and eight trials entered this meta-analysis. Studies focused on coronary artery disease, peripheral arterial disease, heart failure and stroke. In coronary artery disease, significant differences between NW+CCVR and CCVR were found in exercise capacity (SMD: 0.49; p = 0.03) and dynamic balance (SMD: 0.55; p = 0.01) favouring NW+CCVR. In peripheral artery disease, larger changes in exercise duration (SMD: 0.93; p < 0.0001) and oxygen uptake (SMD: 0.64; p = 0.002) were observed following NW compared with controls. In heart failure, no significant differences were found between NW and CCVR or usual care for peak VO2 and functional mobility. In post-stroke survivors, functional mobility was significantly higher following treadmill programmes with poles rather than without (SMD: 0.80; p = 0.03).
Conclusions
These data portray NW as a feasible and promising activity for individuals with cardiovascular disease. Further studies are necessary to verify whether NW may be incorporated within CCVR for individuals with cardiovascular disease.
Introduction
Regular exercise is beneficial to cardiovascular health and longevity. 1 The American College of Sports Medicine and the Center for Disease Control and Prevention recommend at least 30 minutes of moderate-intensity physical activity on most days of the week.1,2 It is well established that physical activity at and above these levels may decrease mortality by up to 27%. 3 Despite these recommendations, sedentary behaviour in developed countries is on the rise and contributes to the increase in cardiovascular mortality,2,3 thus justifying the growing attention towards exercise-based cardiovascular rehabilitation programmes for secondary prevention. 4 These programmes play a key role in improving the overall health status and quality of life (QOL) of participants by modifying cardiovascular risk factors, particularly sedentary behaviour.5,6 The efficacy of exercise-based programmes relies heavily on patient adherence, leading to a wide range of methods being attempted to increase participation and compliance.4–7 These include group activities that are both physically and socially engaging, which promote patient involvement. Nordic walking (NW) is one such activity. NW has its origins in Finland, where it was introduced in the late 1980s as a summer training for Nordic skiing. After 2000, it was spread out worldwide and, increasingly investigated, soon became an exercise component of the cardiovascular rehabilitation programmes.8,9
NW is a particular form of physical activity similar to Nordic skiing and combines active use of the trunk and upper limbs with classic walking, using specifically designed poles. The result is a full-body workout that combines the ease and accessibility of conventional walking with upper body conditioning, so that higher energy expenditure can be achieved. 10
Previous studies have shown that NW enhances aerobic capacity, muscular strength, balance and the overall well-being of healthy subjects. 8 Additionally, NW is effective in positively modifying traditional cardiovascular risk factors such as hypertension, diabetes mellitus and dyslipidaemia.8,9
Physical training in conventional cardiovascular rehabilitation (CCVR) programmes generally consists of aerobic training on a treadmill or cycle ergometer, often complemented by muscle strengthening exercises and calisthenics.5,6 NW has been proposed as a complementary tool to these programmes due to the additional engagement of the upper body (resulting in the involvement of approximately 70–90% of the body’s skeletal musculature) and the relatively higher energy expenditure compared with traditional walking by an estimated 8%. 10 In addition, the employment of the poles reduces loading stress at the knee joint by approximately 30% compared with walking without poles. 11 These characteristics support NW as a promising form of physical activity in individuals with cardiovascular disease (IwCVD), especially the elderly and those with multiple comorbidities.8,9
The aims of this systematic review and meta-analysis were: (i) to appraise the available evidence on the health effects and clinical relevance of NW in individuals with established CVD and, (ii) to determine a precise estimate of NW-induced changes on primary outcomes such as those cardiovascular and functional (i.e. exercise capacity, maximal oxygen consumption, exercise duration) and on secondary outcomes (i.e. QOL, non-motor symptoms) in individuals diagnosed with CVD. 12
Methods
Protocol registration and literature search
The systematic review protocol was registered in Figshare.com on October 2016 with the following digital object identifier: doi.org/10.6084/m9.figshare.3988974.v1.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and flow chart diagram were used as a reporting structure for this systematic review.13,14
We conducted electronic searches of citation databases from inception to November 2016. PubMed medical databases including MEDLINE, Scopus, Web of Science and the Cochrane Central Register of Controlled Trials (CENTRAL) were searched. A comprehensive search strategy for primary studies, developed and performed by two of the authors (LC and PPB), used the text word terms: ‘Nordic Walking’ OR ‘Polestriding’ OR ‘Walking Poles’. Only randomized controlled trials (RCTs) in English 15 were selected and the references of all included articles were further checked for relevant publications. A detailed literature search strategy for each of the databases can be found in Supplementary Material file 1 online.
Eligibility criteria and search strategy
The articles included in this systematic review and meta-analysis had to meet the following inclusion criteria based on the PICO model:14,16 (i) studies enrolling individuals with established cardiovascular disease (CVD); 12 (ii) studies employing a mid- to long-term (defined as ≥2 weeks) NW programme. Titles and abstracts of potentially relevant articles were independently assessed by two of the authors (LC and PPB) and duplicates were removed. A full-text article was evaluated when the title or abstract presented insufficient information to determine inclusion. In cases of disagreement, a mutual discussion to reach consensus was carried out and, if necessary, a third author (AM) contributed to the final decision.
Data extraction and quality assessment
Demographic characteristics of the samples (average age, gender and CVD area), trial methodologies and interventions (control groups or other comparative groups, NW programme characteristics and duration) and the primary (cardiovascular and functional outcomes) and secondary study outcomes (QOL and non-motor symptoms) of each trial were collected independently by the two authors (LC and PPB) using a standardized data extraction form.
Subsequently, the quality and risk of bias assessments were completed by employing the Physiotherapy Evidence Database (PEDro) scale. 17 The PEDro scale is based on the Delphi list developed by Verhagen and colleagues 17 to assess the methodological quality of RCTs in physical therapy. This scale consists of 11 items rating the internal validity (10 items) and external validity (one item) of clinical trials, with the total score ranging from one to 10 points (a higher score corresponds to a higher methodological study quality). 17 As above, in cases of disagreement, a third author (AM) made the final decision.
Statistical analysis
The clinical relevance of the intervention-induced changes reported as significant was estimated by calculating the Hedges g effect size (ES: small ≤ 0.5; moderate 0.51–0.79; large ≥ 0.8), according to the formulae of Hedges and Olkin.18,19 Absolute ESs were calculated for each study by comparing at the post-intervention NW versus other interventions and/or controls (i.e. NW versus CCVR, NW versus non-active control group, NW versus traditional walking and NW versus treadmill training).
A meta-analysis was planned if at least two studies reported data for the same outcome measure. 13 Heterogeneity across the studies was calculated using the Q-test (Chi-square) and the inconsistency I2 statistic. 20 An I2 with a value > 50% was considered indicative of high heterogeneity. All meta-analyses were performed using RevMan 5.3 (Review Manager, the Cochrane Collaboration). Raw data (means and standard deviation (SD)) were extracted or calculated from standard errors, 95% confidence intervals (CIs), p values, t values, or F values. In the case of missing data a formal request was sent to the corresponding and first authors of each study. Publication bias was assessed by funnel plot symmetry and Egger regression intercept. Pooling of data was carried out using a random rather than a fixed-effects model since many investigators consider it more appropriate in the context of medical decision-making. 21 In order to allow interpretation of the pooled estimate of the effects obtained, the standardized mean difference (SMD), which expresses the intervention effect in standard units rather than the original units of measurement, was reported. According to Cohen, 22 an SMD of 0.2 was considered as low, 0.5 as medium and 0.8 as large.
Lastly, in the case of studies originating from the same dataset, the sample was counted once to avoid sample size inflations.
Results
Study selection
The comprehensive flow chart for the study selection process is presented in Figure 1.
PRISMA flow diagram for selection of studies.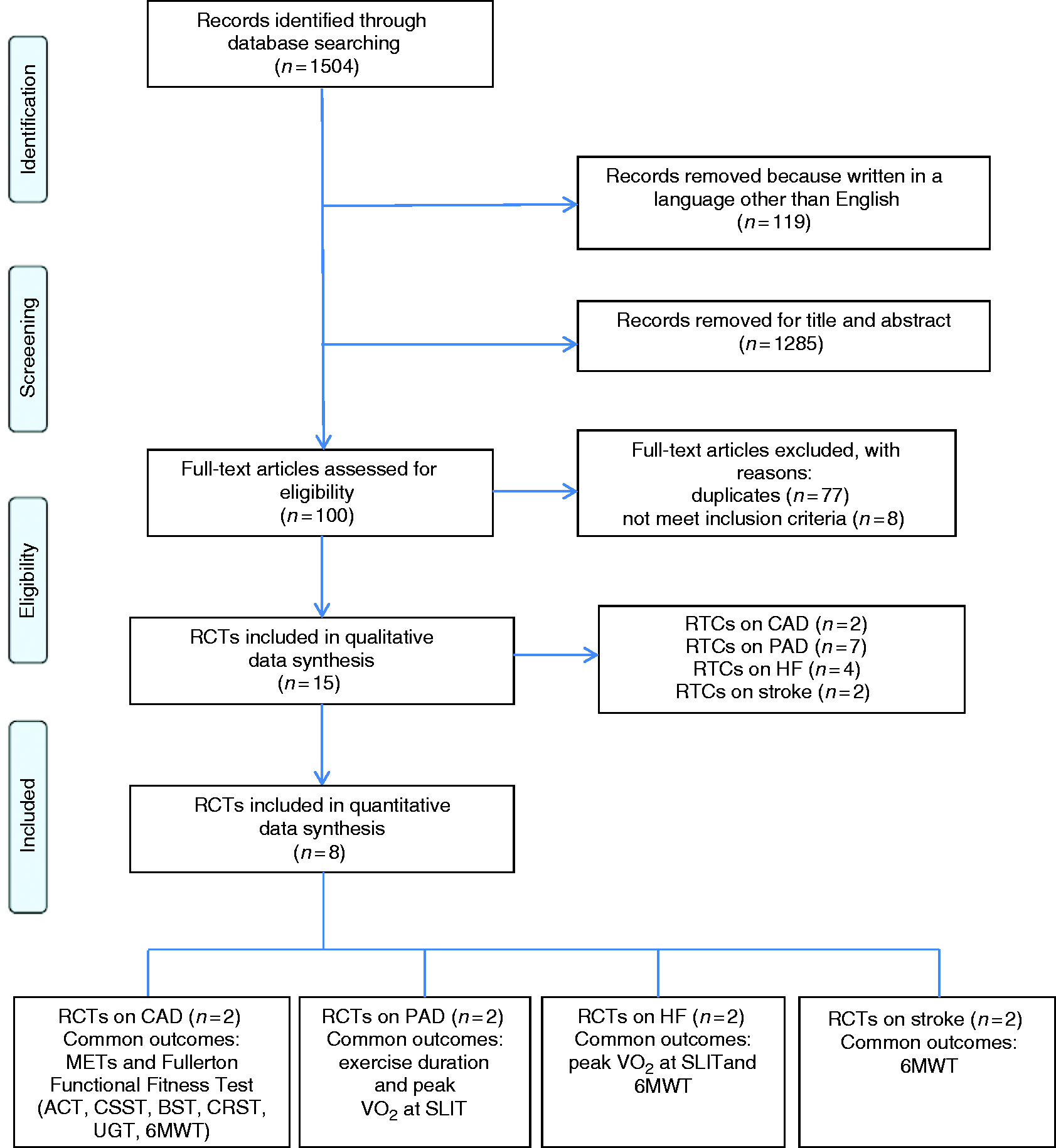
Fifteen RCTs focusing on NW as a form of rehabilitation for IwCVD met all the eligibility criteria and were included in the qualitative synthesis of this review.23–37 A detailed overview of the excluded studies and the main reasons for exclusion can be found in Supplementary Material file 2.
Of the 15 studies analysed, eight trials showing sufficient homogeneity in the pre-defined comparisons 13 were included in the quantitative meta-analysis23–25,27,32,33,36,37 (Figure 1).
Quality assessment
The PEDro scale score ranged from 3 to 6 (mean 4.8 ± 0.9, median 5 ± 0.2) out of a maximum score of 10.23–37 This was predominantly due to lack of blinding in all included studies. In addition, adequate follow-up outcomes were reported in only six out of the 15 studies.25–27,29,33,36 For all included studies, the results of between-group statistical comparison were reported, and point estimates and measures of variability were provided for at least one key outcome. Study and control/comparison groups were also similar at baseline in all of the included studies but one. 32 Four studies performed an intention-to-treat analysis28,29,32,35 and allocation was concealed in only one study. Participants were randomized in all of the studies but one. 31 The quality assessment of the included studies is reported in Supplementary Material file 3.
Qualitative data synthesis
The 15 selected studies were conducted between 2002 and 2016 and enrolled a total of 766 individuals, comprising 649 men (85%) and 87 women (11%). In one study (30 subjects) gender data were not available, 23 whereas in seven trials, participants’ mean age was not clearly stated.24,25,33–37 Subjects ranged in age from 40 to 80 years old.
Among the 15 RCTs selected, two focused on coronary artery disease (CAD),23,24 seven on peripheral arterial disease (PAD),25–31 four on individuals with heart failure32–35 and two on post-stroke survivors.36,37
All studies analysed mid- to long-term effects of NW training (from three to 24 weeks) performed as a standalone approach25,27–37 or in combination with CCVR programmes (i.e. aerobic training on a treadmill or cycle ergometer, complemented by muscle strengthening exercises and calisthenics)23,25 or compared with other interventions, such as integration with vitamin E or placebo. 26 Nine studies compared NW training with CCVR programmes23,24,30,32 or with control groups (usual medical therapy and normal activities of daily living without prescribed exercise) and usual care (UC; recommendations for suitable lifestyle changes and self-management).25,27,33–35 Six studies compared NW training with other types of exercise programmes than CCVR, such as traditional walking24,28,29 and treadmill training.31,36,37 Finally, in the two studies focusing on post-stroke survivors, NW training was performed on a treadmill (Nordic treadmill training, (NTT)).36,37
Different durations and frequencies of the NW programmes were tested in the trials, ranging from three to five times a week for a total of three to 24 weeks. On average, interventions were carried out with a frequency of 4 ± 1.1 times/week (95% CI 3.1–4.9) and for a total duration of 7.8 ± 6.2 weeks (95% CI 3.3–15.7).
The effects of NW training on cardiovascular and functional outcomes were analysed by all included studies, while QOL and non-motor symptoms outcomes were assessed by eight trials.25–27,29,32,33,35,37
Regarding the three studies by Piotrowicz et al., which were found to originate from the same dataset,33–35 all the outcomes arising from their primary study 33 and any new additional outcomes reported in the secondary studies34,35 were considered. In the case of shared outcomes, those reported in the study with a greater number of individuals were considered (Table 3).
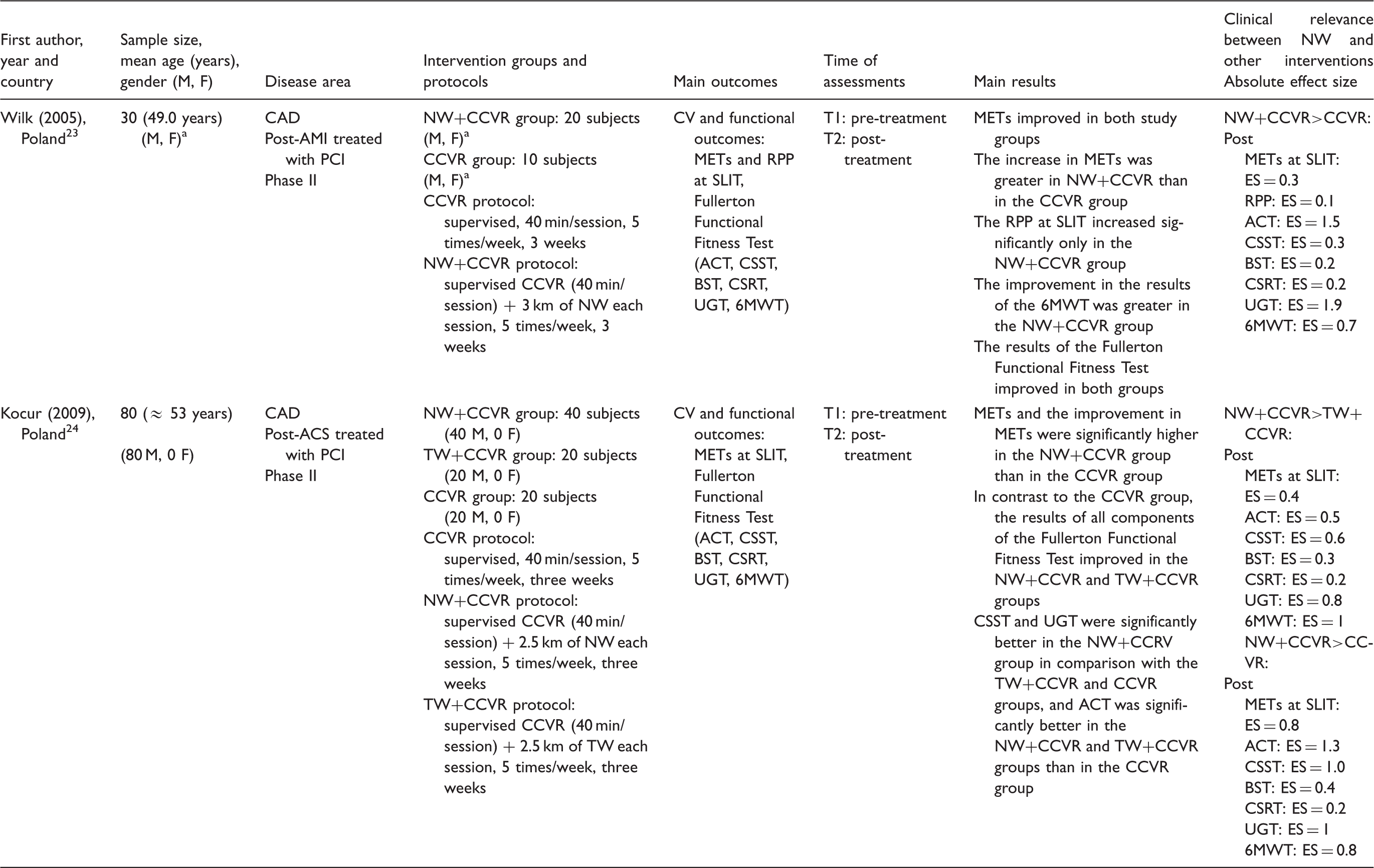
Effect size calculated by the Hedges g; small ≤ 0.5; moderate 0.51–0.79; large ≥ 0.8; 18 absolute effect size: calculated comparing NW versus other interventions or control at each time point. Effect size formulas according to Hedges and Olkin. 18
Data not reported in the final paper and/or not supplied by the authors upon request.
F: female; M: male; NW: Nordic walking; CAD: coronary artery disease; AMI: acute myocardial infarction; PCI: percutaneous coronary intervention; ACS: acute coronary syndrome; CCVR: conventional cardiovascular rehabilitation; TW: traditional walking; CV: cardiovascular; MET: metabolic equivalent; RPP: rate-pressure product; SLIT: symptom-limited incremental treadmill exercise test; ACT: Arm Curl Test; CSST: Chair Sit to Stand Test; BST: Back Scratch Test; CSRT: Chair Sit and Reach Test; UGT: Up and Go Test; 6MWT: Six-Minute Walking Test; ES: effect size
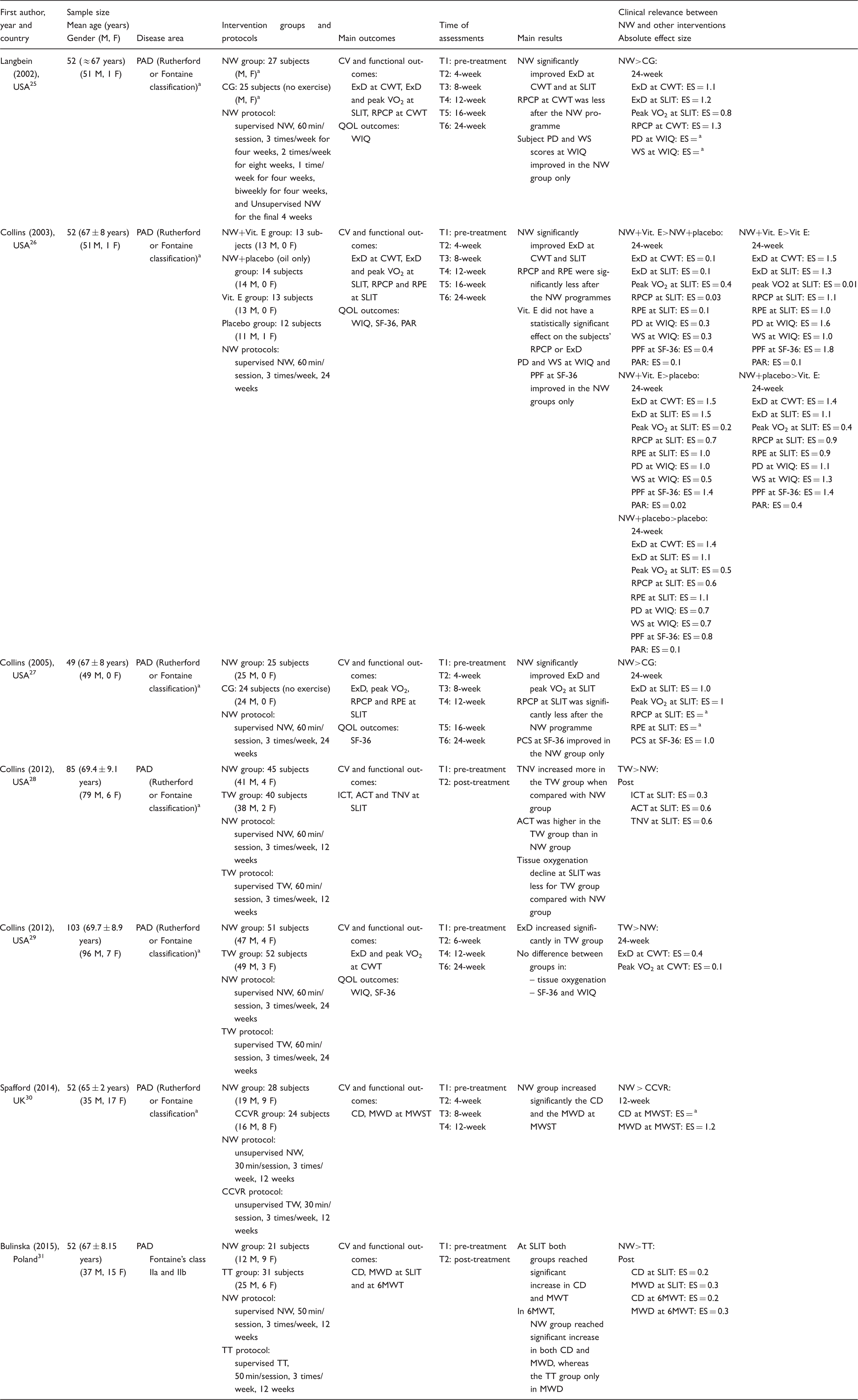
Effect size calculated by the Hedges g; small ≤ 0.5; moderate 0.51–0.79; large ≥ 0.8; 18 absolute effect size: calculated comparing NW versus other interventions or control at each time point. Effect size formulas according to Hedges and Olkin. 18
Data not reported in the final paper and/or not supplied by the authors upon request.
F: female; M: male; NW: Nordic walking; PAD: peripheral arterial disease; CG: control group; Vit. E: vitamin E (400 IU of vitamin E orally daily); TW: traditional walking; CCVR: conventional cardiovascular rehabilitation; CV: cardiovascular; ExD: exercise duration; VO2: oxygen uptake; SLIT: Symptom-limited Incremental Treadmill Exercise Test; RPCP: rating of perceived claudication pain; CWT: Constant Work-rate Treadmill Test; QOL: quality of life; WIQ: Walking Impairment Questionnaire; RPE: rating of perceived exertion; SF-36: 36-Items Short Form Questionnaire; PCS: Physical Component Summary (at SF-36); PAR: Physical Activity Recall Questionnaire; ICT: initial claudication time; ACT: absolute claudication time; TNV: time elapsed prior to reaching nadir StO2 values; CD: claudication distance; TT: treadmill training; MWD: maximum walking distance; MWST: Modified Walking Shuttle Test; PD: perceived distance (at WIQ); WS: walking speed (at WIQ); ES: effect size; PPF: perceived physical function (at SF-36); 6MWT: Six-Minute Walking Test.
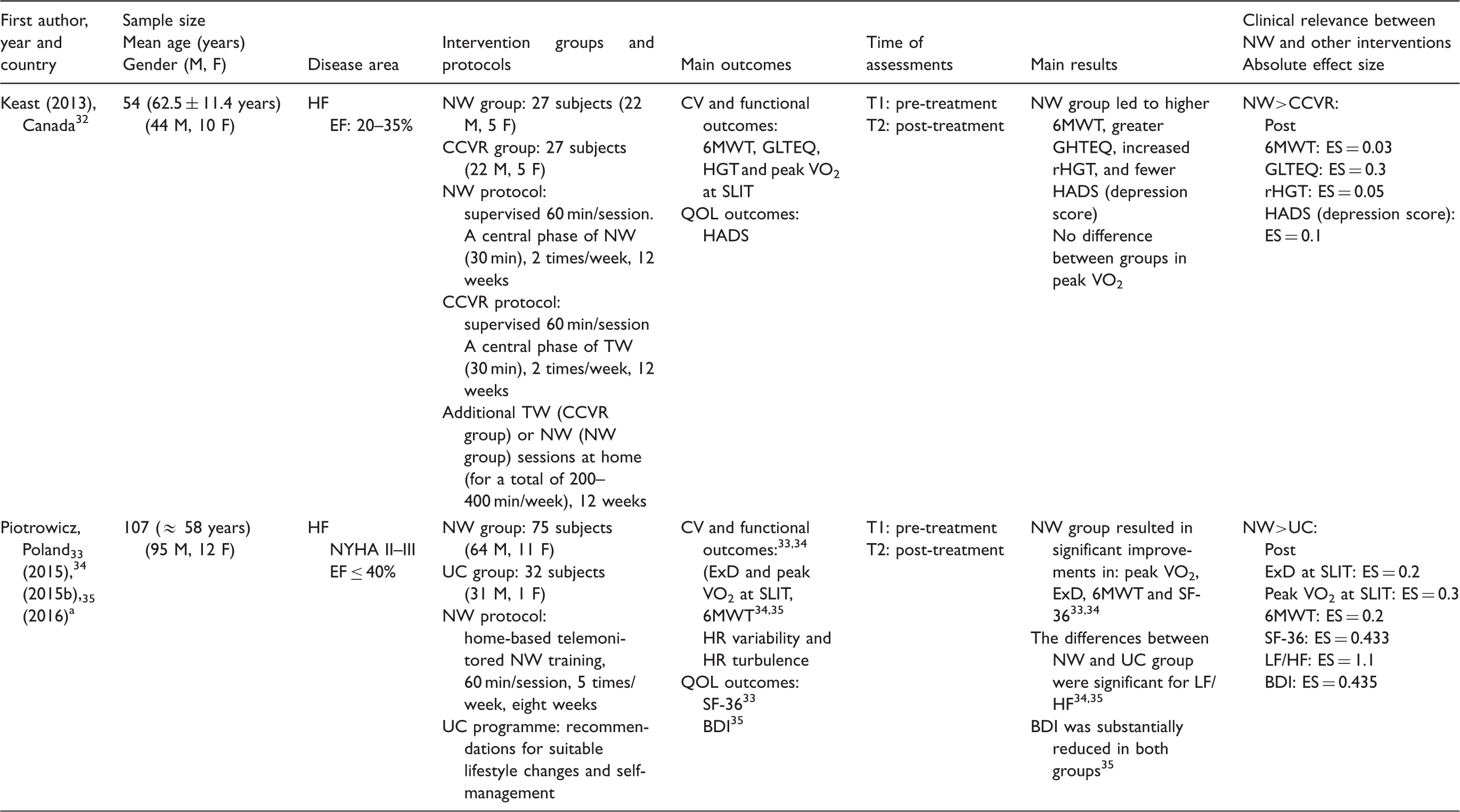
Effect size calculated by the Hedges g; small ≤ 0.5; moderate 0.51–0.79; large ≥ 0.8; 18 absolute effect size: calculated comparing NW versus other interventions or control at each time point. Effect size formulas according to Hedges and Olkin. 18
Studies found to originate from the same dataset.
F: females; M: males; NW: Nordic walking; HF: heart failure; EF: ejection fraction; CCVR: conventional cardiovascular rehabilitation; TW: traditional walking; CV: cardiovascular; 6MWT: Six-Minute Walking Test; GLTEQ: Godin Leisure Time Exercise Questionnaire; rHGT: right-hand Hand-grip Dynamometer Test; HGT: Hand-grip Dynamometer Test; VO2: oxygen uptake; SLIT: Symptom-limited Incremental Treadmill Exercise Test; QOL: quality of life; HADS: Hospital Anxiety and Depression Scale; NYHA: New York Heart Association; UC: usual care; ExD: exercise duration; HR: heart rate; SF-36: 36-Items Short Form Questionnaire; BDI: Beck Depression Inventory; LF/HF: low/high frequency ratio
Effect size calculated by the Hedges g; small ≤ 0.5; moderate 0.51–0.79; large ≥ 0.8; 18 absolute effect size: calculated comparing NW versus other interventions or control at each time point. Effect size formulas according to Hedges and Olkin. 18
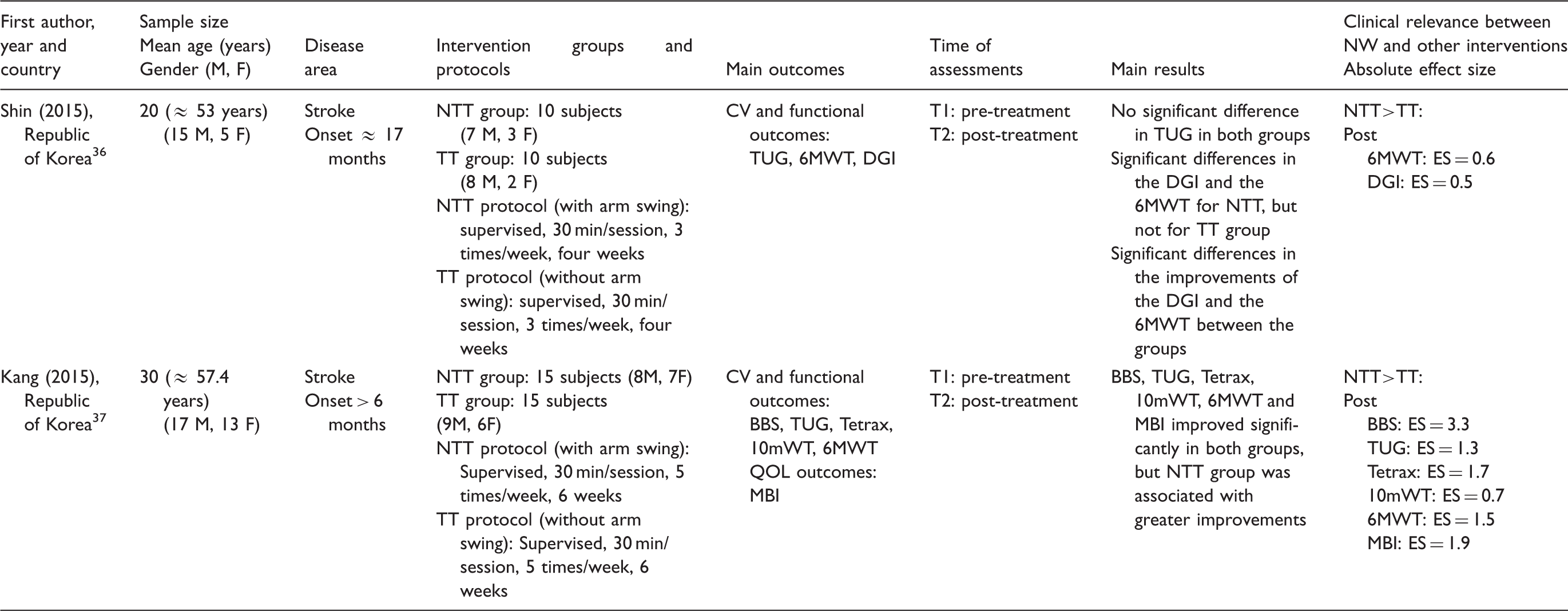
F: female; M: male; NTT: Nordic treadmill training; TT: treadmill training; CV: cardiovascular; TUG: Timed Up and Go Test; 6MWT: Six-Minute Walking Test; DGI: Dynamic Gait Index; BBS: Berg Balance Scale; Tetrax: Tetra-ataxiometric Posturography Test; 10mWT: 10-metre Walking Test; QOL: quality of life; MBI: Modified Barthel Index; ES: effect size
Quantitative data synthesis
A meta-analysis was performed for eight out of 15 studies (422 patients): two for CAD,23,24 two for PAD,25,27 two for heart failure32,33 and two for stroke36,37 due to the limited availability of RCTs and the high heterogeneity among the interventions. These included NW combined with other interventions, 26 differences in comparative exercise programmes28,29,31 and studies investigating the same population,33–35 as well as manifold evaluation protocols. 30
Studies on the effects of NW in individuals with CAD
Table 1 reports the main results from the two studies comparing a combined NW + CCVR programme with a CCVR programme alone for people with CAD.23,24 Both studies yielded improvements in exercise capacity in terms of metabolic equivalents (METs) and in several components of the Fullerton Functional Fitness Test, which were found to be superior following NW+CCVR (absolute ES, NW + CCVR > CCVR: from 0.1 to 1.9)23,24 (Table 1). Figure 2 reports the results of the quantitative analysis conducted on a pooled sample of 90 individuals. The studies were homogeneous (I2 < 50%). Statistically significant differences were observed between groups in achieved METs (SMD: 0.49, 95% CI 0.04, 0.93; p = 0.03) and in the Up and Go Test (UGT) (SMD: 0.55, 95% CI 0.11, 1.00; p = 0.01) in favour of NW+CCVR.
Synthesis of results: NW+CCVR versus CCVR alone in coronary artery disease.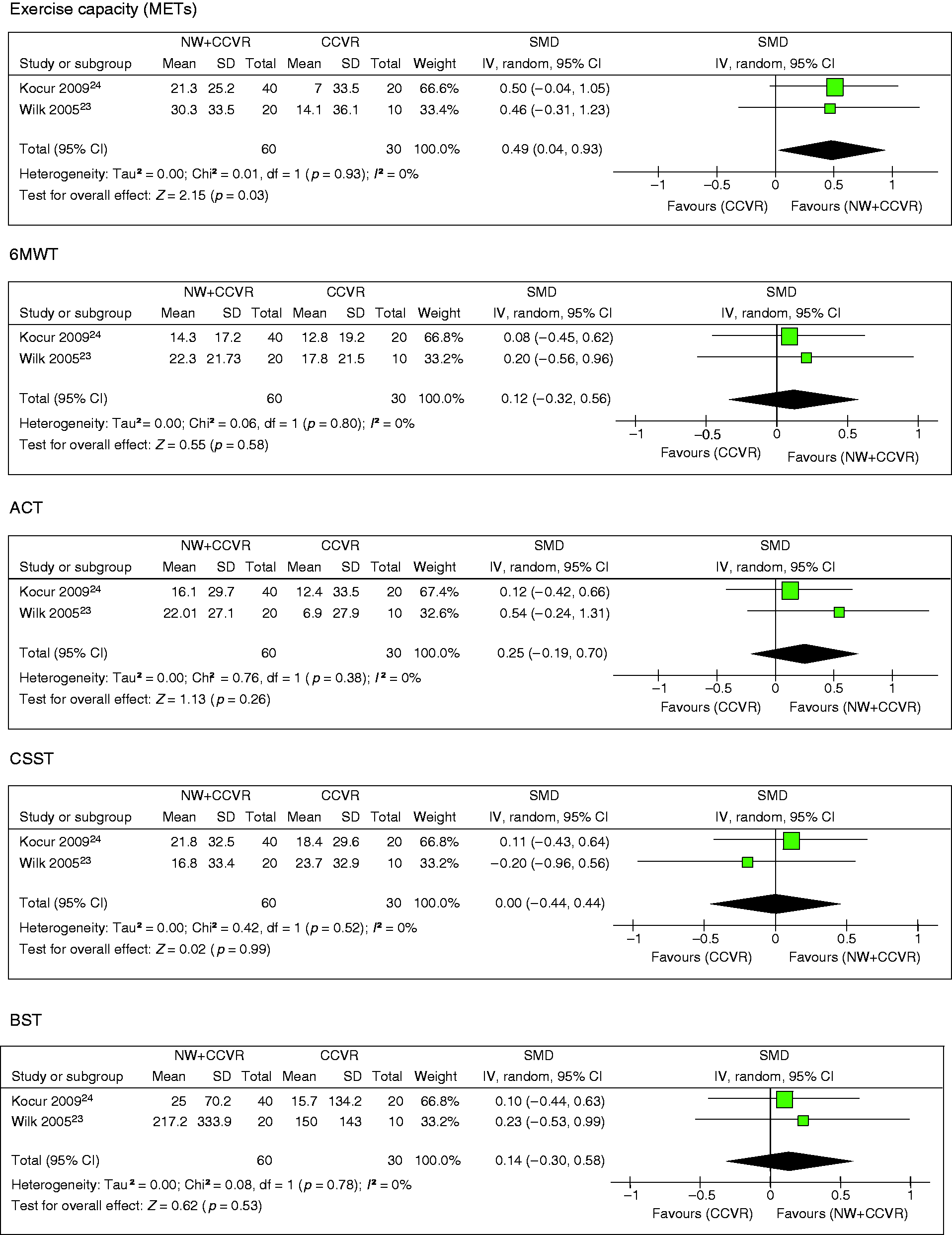
No significant differences were detected between NW+CCVR and CCVR in functional mobility (Six-Minute Walking Test (6MWT)), strength assessments (Arm Curl Test and Chair Sit to Stand Test) and flexibility of the upper and lower parts of the body (Back Scratch Test and Chair Sit and Reach Test).
Studies on the effects of NW in individuals with PAD
Table 2 reports the main results of the studies on the effects of NW in individuals with PAD.
Overall, the authors agree on the effectiveness of NW in improving cardiovascular, functional and QOL outcomes.25–27,30,31 Two studies comparing NW training with traditional walking (TW) reported larger improvements following the latter in terms of exercise duration (ExD) and oxygen uptake (peak VO2) (absolute ES, TW > NW: from 0.1 to 0.6).28,29 For the two studies involving PAD that were sufficiently homogeneous (I2 = 0%) to undergo meta-analysis (Figure 3; pooled sample: n = 101), pooled data demonstrated significant differences in ExD (SMD: 0.93, 95% CI 0.52, 1.34; p < 0.0001) and peak VO2 (SMD: 0.64, 95% CI 0.23, 1.04; p = 0.002) in favour of NW compared with control.25,27 Figure 3 displays the forest plots of the main effects for the ExD and peak VO2 outcomes.
Synthesis of results: NW versus control groups in peripheral arterial disease.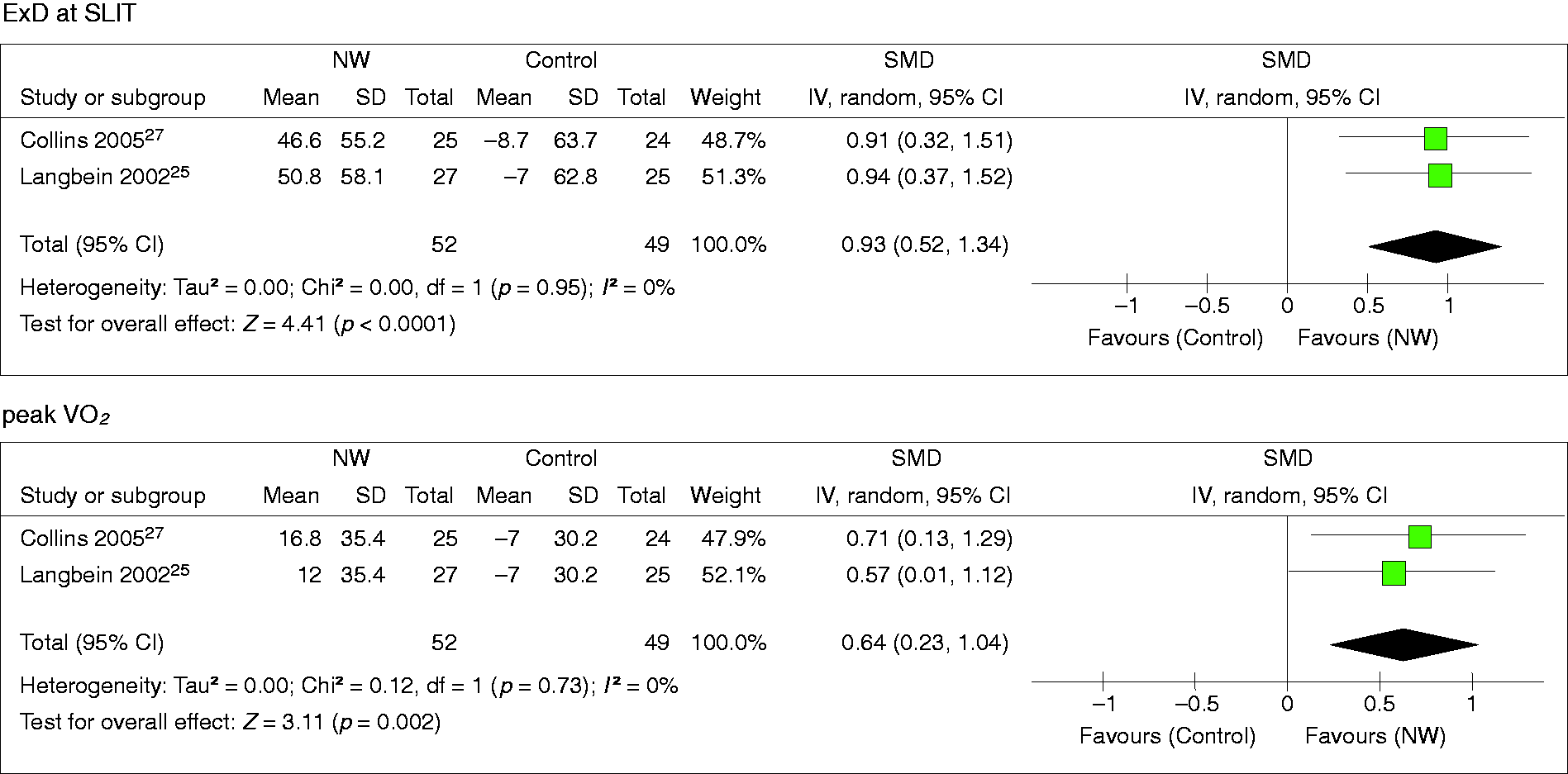
Studies on the effects of NW in individuals with heart failure
Table 3 reports the main findings arising from the comparison of NW training to CCVR 32 and usual care programmes33–35 in individuals with heart failure.
Cardiovascular and functional outcomes, as well as QOL, all showed improvement,32–35 with changes significantly greater following NW than CCVR or a usual care programme. Table 3 details the clinical relevance of the intervention-related changes by group as Hedges g (absolute ES, NW>CCVR: from 0.03 to 0.3 and NW>UC: from 0.2 to 1.1).32,35
In the meta-analysis of heart failure trials, the included studies (Figure 4) reported high homogeneity (I2 = 0 and 26%, respectively), although no significant differences were detected between groups in peak VO2 (pooled sample: n = 161; SMD: 0.29, 95% CI −0.10, 0.68; p = 0.14) and in 6MWT distance (pooled sample: n = 161; SMD: 0.29, 95% CI −0.04, 0.62; p = 0.08).
Synthesis of results: NW versus CCVR or usual care in heart failure.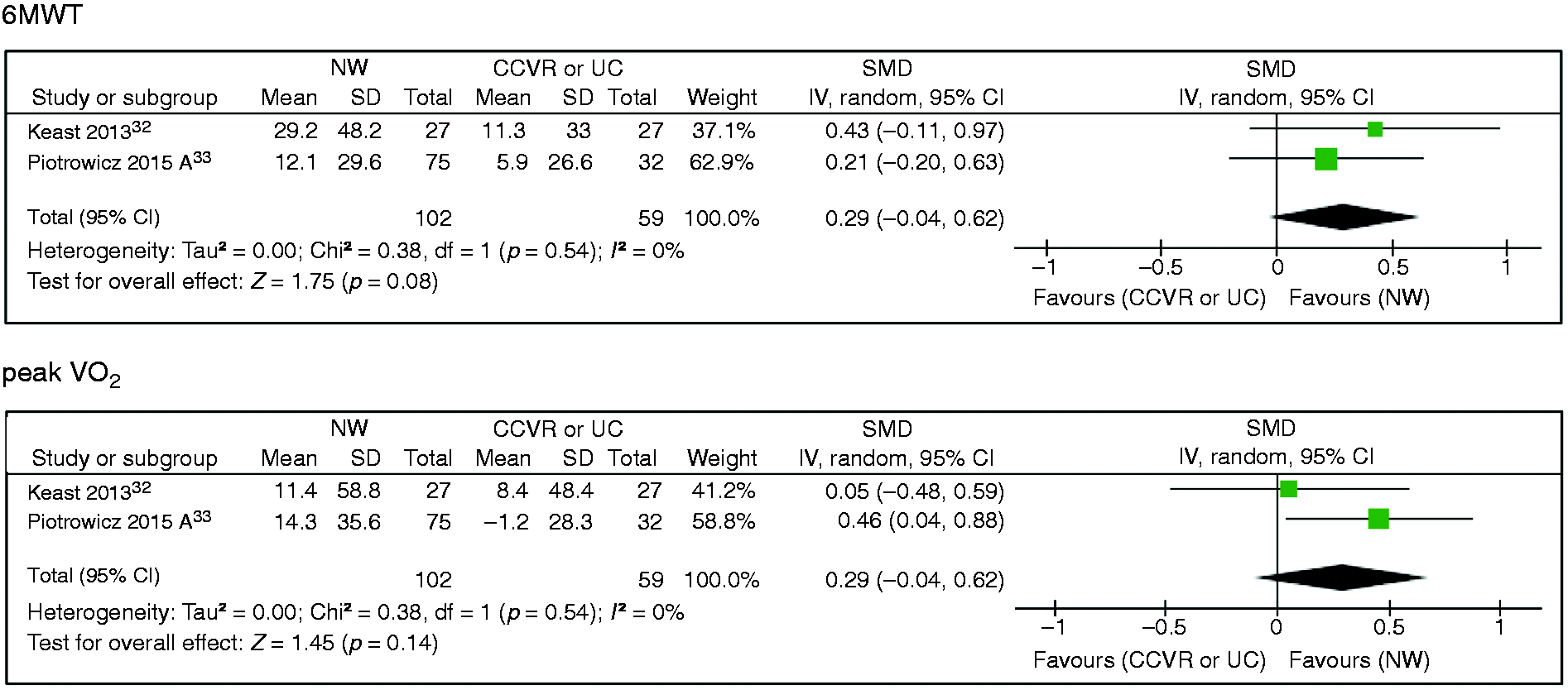
Studies on the effects of NW in post-stroke survivors
Table 4 outlines the two studies on the effects of NW performed on a treadmill (NTT) and a traditional treadmill training without arm swing (TT), in post-stroke survivors.36,37 Larger improvements were observed after NTT than TT with moderate to high ES (absolute ES, NTT>TT: from 0.5 to 3.3). Following meta-analysis (Figure 5, pooled sample: n = 50, heterogeneity test: I2 = 34%), a statistically significant difference in 6MWT distance was observed in favour of NTT compared with TT (SMD: 0.80, 95% CI 0.08,1.52; p = 0.03).
Synthesis of results: NTT versus TT in post-stroke survivors.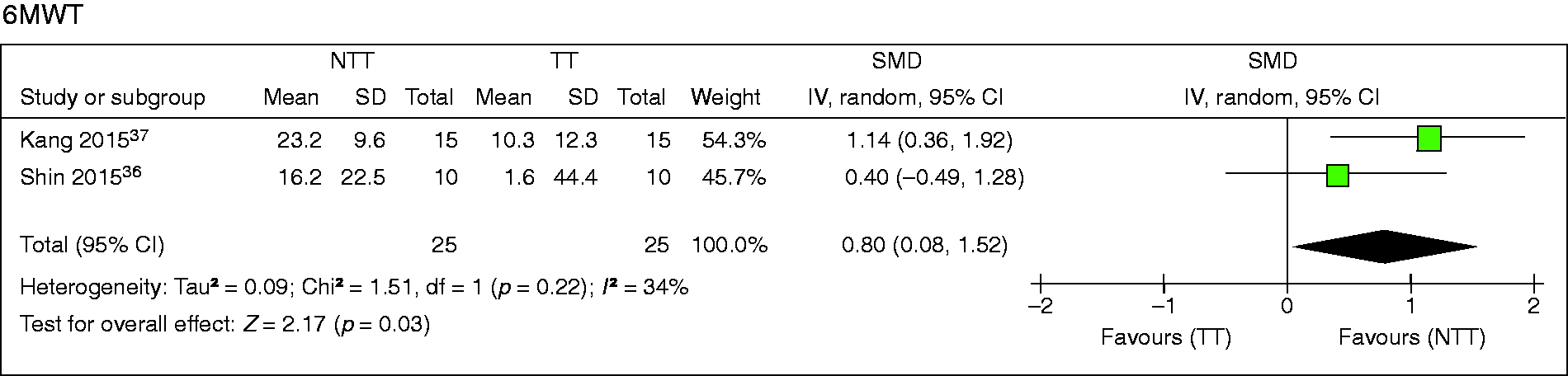
Publication bias
Visual inspection of the funnel plots (data not shown) revealed no asymmetry in each of the 12 outcome measures considered in the present meta-analysis, with studies gathered symmetrically around the centre of the funnel. The absence of substantial publication bias was further confirmed by the non-significant Egger regression coefficients (all one-tailed p values > 0.05).
Discussion
This systematic review and meta-analysis highlights the benefits of NW training pertaining to four major subgroups of CVD (CAD, PAD, heart failure and stroke). Out of 15 RCTs that were systematically reviewed (n = 766), meta-analysis was performed for eight studies (n = 422). Regardless of CVD subgroups, NW proved superior to non-active control groups and, when combined with CCVR, it seems to lead to larger improvements than CCVR alone on exercise capacity and fitness. Findings proved less consistent when NW was compared with other exercise-based interventions.
In individuals with CAD, NW-based CVR revealed larger effect estimates in METs and dynamic balance (UGT).23,24 Improvements in exercise capacity have been previously associated with improved survival in IwCVD.38–41 As an example of such relationship, the increase of 1 MET in exercise capacity is associated with 12% improved survival. 42 However, it should be pointed out that in the CAD studies included in the present review23,24 NW was administered in combination with CCVR programmes, possibly resulting in an additive effect due to the increased workout volume. Further studies are warranted to determine the role played by the specific type of intervention rather than the volume of exercise.
In PAD populations, the significant improvements in ExD and peak VO2 observed in favour of the NW groups compared with controls25,27 can be interpreted as particularly appealing since increases in these variables have been previously associated with a higher QOL and with enhanced life expectancy. 43 However, such findings need to be verified by further adequately powered and supervised RCTs, 44 especially directed to compare and clarify the advantages of NW training with those that arise following a TW programme specifically addressed to individuals with PAD.
NW has been portrayed as a feasible form of exercise that can be adapted to different fitness levels, even in people with heart failure and low exercise tolerance. 45 In these individuals, no significant difference was found between NW-based interventions and CCVR or usual care programmes for peak VO2 and functional mobility.32,33 However, it should be taken into account that the individuals enrolled in these protocols showed a satisfying level of functional mobility already at baseline (6MWT) (Keast et al. NW: 430 ± 137 m; CCVR: 503 ± 106 m; Piotrowicz et al. NW: 428 ± 93 m; usual care: 439 ± 76 m),32,33 as demonstrated by the comparison with normative data available for this population (average distance walked: ranged from 310 to 427 m). 46
In post-stroke survivors, the observed improvements in 6MWT distance were compared with previously reported cut-offs for meaningful effects (Minimal Detectable Change (MDC); Minimal Clinically Important Difference (MCID)) to establish the practical relevance of the intervention-induced changes.36,37 Eng et al. estimated a MDC of +34.37 m to be exceeded in order to consider any improvement in 6MWT as meaningful in this population. 47 This cut-off was surpassed in both included studies (+38.9 and +50.1 m, respectively).36,37 In addition, Perera et al. 48 estimated the MCID for 6MWT as an increase of at least 50 m following rehabilitative interventions. This threshold was exceeded only in the study by Kang et al. 37 following NTT (NTT: +50.1) but not TT (+20.32 m). On a speculative level, we offer that the positive findings detected following NW may be partly explained by the additional engagement of the upper part of the body. In view of this specific feature, NW has been proposed as potentially helpful in the rehabilitation programmes of specific neurological diseases.49–51 Indeed, NW poles can provide further stability and better trunk posture over time, which is particularly appealing for individuals presenting motor-functional impairments, postural instability and fear of falling, as is the case in post-stroke survivors.
Critical appraisal of the findings and study limitations
Despite a comprehensive search strategy, our study highlights the paucity of data on NW in IwCVD, with only eight studies eligible for meta-analysis. Adequately powered RCTs with common outcomes across sub-categories of IwCVD remain necessary to validate our findings.
Due to the overall low to moderate quality of the studies included in the present review (median PEDro score: 5), cautious interpretation of the studies’ findings is recommended, particularly for studies with a higher risk of bias (PEDro score: ≤ 4).23,30,31,34,37 These studies lacked important methodological steps such as blinding of assessors and analysis based on intention-to-treat, which may have biased the present estimates.
High heterogeneity was detected among the studies, which prevented data pooling across larger samples. In particular, the protocols differed for the modalities of assessment even when similar variables were evaluated. For instance, although the secondary outcomes describing QOL and non-motor symptoms were assessed in the majority of the RCTs (eight studies), discrepancies in the evaluation protocols prevented proper aggregation of the data.
Gender bias needs to be taken into consideration since only 11% of the total population in the included studies were women, which raises concerns considering that CVD is still the major cause of death in women over the age of 65 years. 52 The risk of heart disease in women is often underestimated due to the misconception that females are ‘protected’ against CVD by their sex hormones. 53 Over the past two decades, however, the prevalence of CAD has increased in middle-aged women (35 to 54 years) while declining in similarly aged men. 53 Furthermore, traditional well-established risk factors such as sedentary behaviour, cigarette smoking and dyslipidaemia contribute to CVD at least as much in women as in men, if not more.54,55 In view of the gender imbalance, results of this study should be applied with caution to women.
Finally, the NW protocols reviewed in this study vary widely in terms of intensity, frequency, duration, progression of exercise and outcomes measured, contributing to a lack of generalizability.
Taken as a whole, these results reinforce the practical benefits of NW for IwCVD, but future prospective studies using standardized and structured training protocols are necessary to objectively quantify the benefits of NW training, especially in other CVD areas (i.e. patients with chronic kidney disease, congenital heart disease patients, heart transplant recipients), for which the cardiovascular effects of NW programmes have not yet been investigated.
Conclusion
Our systematic review and meta-analysis on NW-based interventions in secondary prevention of CVD has shown that NW training improves exercise capacity in IwCVD, whether performed as a standalone form of physical activity or in combination with CCVR programmes. However, existing studies are small, heterogeneous and of limited quality.
Given its feasibility, affordability and preliminary evidence supporting its health benefits, high quality, adequately powered RCTs evaluating NW are warranted to justify its inclusion as a complementary tool in CCVR programmes for IwCVD.
Footnotes
Author contribution
LC, AM, GM and JCK contributed to the conception and design of the work. LC, AM, TJY and PPB contributed to the acquisition, analysis and interpretation of data for the work. LC, AM and TJY drafted the manuscript. All the authors critically revised the manuscript and gave final approval. All agree to be accountable for all aspects of work ensuring integrity and accuracy. GM and JCK have equally contributed to this work.
Acknowledgements
The authors would like to thank Dr Kang Tae Woo and Prof. Jennifer Reed for the data supplied upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Fondazione Banco di Sardegna (Funds 2014) and by Grant 2015 from the Italian Society of Cardiology and MSD Italia-MERCK SHARP & DOHME CORPORATION for the implementation of the project: ‘Physical Exercise and Therapy: An integrated approach for the reduction of cardiovascular risk and health promotion’ at St. George’s, University of London.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.