
Abstract
Background
The risk of cardiovascular disease is closely connected to adipose tissue inflammation. The links between cardiovascular risk predictors and pro and anti-inflammatory macrophages in human adipose tissue were analysed to gain an insight into the pathophysiology of cardiovascular disease.
Design
Subcutaneous and visceral adipose tissues were obtained from 79 subjects, 52 living kidney donors (during nephrectomy) and 27 patients with peripheral artery disease (during arterial tree reconstruction).
Methods
Macrophage subsets were isolated from adipose tissues and analysed by flow cytometry using CD14, CD16, CD36 and CD163 monoclonal antibodies. The mutually adjusted differences of phagocytic pro-inflammatory (CD14 + CD16 + CD36high), anti-inflammatory (CD14 + CD16-CD163+) and transitional subsets of macrophages were analysed in relation to cardiovascular predictors (sex, age, body mass index, smoking, hypercholesterolaemia, hypertension and statin treatment).
Results
Age, male sex and hypercholesterolaemia were closely positively associated with the phagocytic pro-inflammatory macrophage subset in visceral adipose tissues. Interestingly, the proportion of phagocytic pro-inflammatory macrophages was relevantly decreased by statin therapy. A strong positive association of body mass index to the phagocytic pro-inflammatory subset was found in subcutaneous adipose tissues only. A minor transitional subpopulation, CD14 + CD16 + CD36lowCD163+, increased with age in both adipose tissues. This transitional subpopulation was also negatively associated with obesity and hypercholesterolaemia in visceral adipose tissues.
Conclusion
An effect of cardiovascular risk predictors on adipose tissue macrophage subpopulations was revealed. Interestingly, while age, male sex and hypercholesterolaemia were connected with the pro-inflammatory macrophage subpopulation in visceral adipose tissues, body mass index had a prominent effect in subcutaneous adipose tissues only. A decreasing effect of statins on these pro-inflammatory macrophages was documented.
Introduction
Several studies including large epidemiological studies on cardiovascular disease (CVD) have reported that adipose tissue enlargement is significantly correlated with blood pressure, dyslipidaemia, obesity and other factors.1,2 All these factors act in harmony to accelerate atherosclerosis, a slowly progressing disease in which lesions are formed in large and medium-sized arteries eventually to result in its main complication, CVD.
Since the 1990s, research has clearly shown that adipose tissue is an important component not only of the endocrine system but, based on accumulation of several immune cells and high production of cytokines, it has also been suggested as an immune organ. 3 Importantly, chronic inflammation in white adipose tissue was found to act as a link between obesity and metabolic disease.4,5
The relationship between adipose tissue dysfunction connected with inflammation, type 2 diabetes mellitus and CVD is supported by several studies.3,6 Although several cell types have been found in adipose tissue, adipose tissue macrophages seem to be the most important players in adipose tissue inflammation. 7 Macrophages make up as much as 40% of adipose tissue cells in obese mice compared to 10% in lean mice. 8 Macrophages are a highly heterogenic cell population and several activation states of macrophages have been described. This macrophage diversity led to an effort to categorise them, and the prevalent approach is to classify them as pro-inflammatory M1 and anti-inflammatory M2 macrophages. 9
Furthermore, several factors associated with an increased risk of CVD are known to be connected with the pro-inflammatory switch of adipose tissue macrophages; i.e. adipose tissue enlargement, 9 hypercholesterolaemia, 10 insulin resistance 11 and postmenopausal status in women. 12 However, there is scant evidence of the effect of other CVD risk factors on adipose tissue immune status.
Statins (3-hydroxy-metylglutaryl coenzyme A (HMG CoA) reductase inhibitors) are a potent class of inhibitors of cholesterol synthesis, and their ability to reduce levels of low-density lipoprotein (LDL) cholesterol has been confirmed by numerous studies. 13 In agreement with the decrease of LDL-cholesterol as one of the main cardiovascular risk factors, a reduction in cardiovascular mortality through statin therapy has also been found. However, the rapidity with which statins reduce cardiovascular risk lead to the conclusion that other effects of statins (apart from LDL lowering) may also participate in the beneficial effect of these drugs. It has been shown that, in addition to the lipid-lowering effect, statins also exert protective anti-inflammatory, 14 antioxidant 15 and plaque-stabilising effects. 16 All these effects might contribute to their anti-atherosclerotic action. This pleiotropic effect of statins has also been documented in clinical studies,17,18 including the large JUPITER population study. 13
The aim of the present study was to take advantage of our detailed adipose tissue macrophage phenotyping project to search for a potential link between the major CVD risk factors and statin treatment on the one hand and the proportion of macrophage subpopulations in subcutaneous adipose tissue (SCAT) and visceral adipose tissue (VAT) on the other.
Methods
Study participants
Adipose tissue was obtained intraoperatively during kidney transplantation from living kidney donors (LKDs), or during peripheral arterial tree reconstruction in patients with angiography-documented peripheral artery disease (PAD). Visceral adipose tissue of LKDs was obtained during cleansing of an isolated kidney (from the area outside of the Gerota’s fascia). Similarly, samples of VAT from the same location were obtained intraoperatively in the PAD group during arterial tree reconstruction. Abdominal SCAT was obtained from similar sites in both groups.
Clinical data were collected from clinical documentation of the enrolled subjects and from an interview targeting lifestyle factors. Prior to enrolment in the study, the subjects were thoroughly informed about the study and informed consent forms were signed. The study complied with the Declaration of Helsinki and was approved by the local ethics committee.
Adipose tissue processing and stromal vascular fraction isolation
Samples of subcutaneous SCAT and VAT were cooled, immediately transferred to the laboratory, minced with scissors (approximately 1 mm3 pieces) and exposed to collagenase (2 mg/ml; Sigma-Aldrich) in phosphate-buffered saline solution for 20 minutes at 37℃. The digestate was immediately cooled and subsequently filtered using two filters (150 µm and 50 µm). After repeated washing, the stromal vascular fraction was obtained. 19
Macrophage markers
The stromal vascular fraction was separated and analysed on the same day using a CyAn flow cytometry analyser (Beckman Coulter, Brea, CA, USA). Different monoclonal antibodies and fluorochromes (CD14 – phycoerythrin-cyanine 7 (PC7), CD16 – phycoerythrin-Texas red-X, ECD, CD36 – fluorescein isothiocyanate, FITC, CD163 phycoerythrin, PE/clone RM3/1) were used to identify different subsets of monocytes/macrophages. Flow cytometry data were analysed using Kaluza software (Beckman Coulter). 19 Subpopulations representing less than 5% were omitted from the analysis.
Based on data from the literature20–23 and our recent results,10,19 we defined a roughly distinguished CD14 + CD16+ subpopulation of macrophages isolated from adipose tissue as likely to be pro-inflammatory and its subset CD14 + CD16 + CD36high as phagocytic pro-inflammatory. In contrast, macrophages with no expression of CD16 (i.e. CD14 + CD16–, 95% of which were almost also CD36lowCD163+) were defined as anti-inflammatory macrophages,19,24,25 a subset referred to as CD14 + CD16-CD163+ hereafter.
Biochemistry
Fasting blood samples (minimally 12 hours of fasting) were obtained in both groups immediately before the procedure (prior to anaesthesia). Cholesterol was determined using an enzymatic method with commercial kits (Roche Diagnostics, Basel, Switzerland) using a Cobas Mira Plus Autoanalyser (Roche). The high-density lipoprotein (HDL) cholesterol concentration was measured after phosphotungstate precipitation of apolipoprotein B-containing lipoproteins and LDL-cholesterol was calculated.
Statistical analysis
In all parameters analysed, the subjects were grouped based on whether the appropriate predictors had met (1) or had not met (0) the criteria (Supplementary Tables 1 and 2). Crude differences in the proportion of various subsets of macrophages were estimated with 95% confidence intervals based on normal distribution.
The differences mutually adjusted for all considered predictors were obtained from univariate or multiple linear normal regressions with Bayesian estimation using the Metropolis–Hastings algorithm, allowing for the same small sample inference in the same manner as if having a large sample. The strict criteria in which differences were expressed as a mean and 99% highest posterior density interval were applied. The association of macrophage subsets proportion to the appropriate predictor of CVD was assessed with 99% credible interval of mutually adjusted difference between subjects with a present or absent predictor. If the credible intervals excluded 0 (either in positive or negative value), the mutually adjusted difference was considered relevant and the proportion of macrophage was shown to be influenced by the respective predictor. For a more detailed description of the statistical method see Supplementary material.
A proportion of macrophage subsets in the population at low CVD risk, further called zero population (i.e. non-smoking women, younger than 50 years, body mass index (BMI) <30 kg/m2, without hypercholesterolaemia and hypertension) was obtained from a mathematical model whose eligibility was verified in a small set of subjects meeting the criteria for the zero population.
Results
The total number of subjects included was 79 (52 LKD and 27 PAD patients), but only 70 SCAT samples were analysed as nine subjects did not agree with tissue removal.
Characteristics of study subjects.
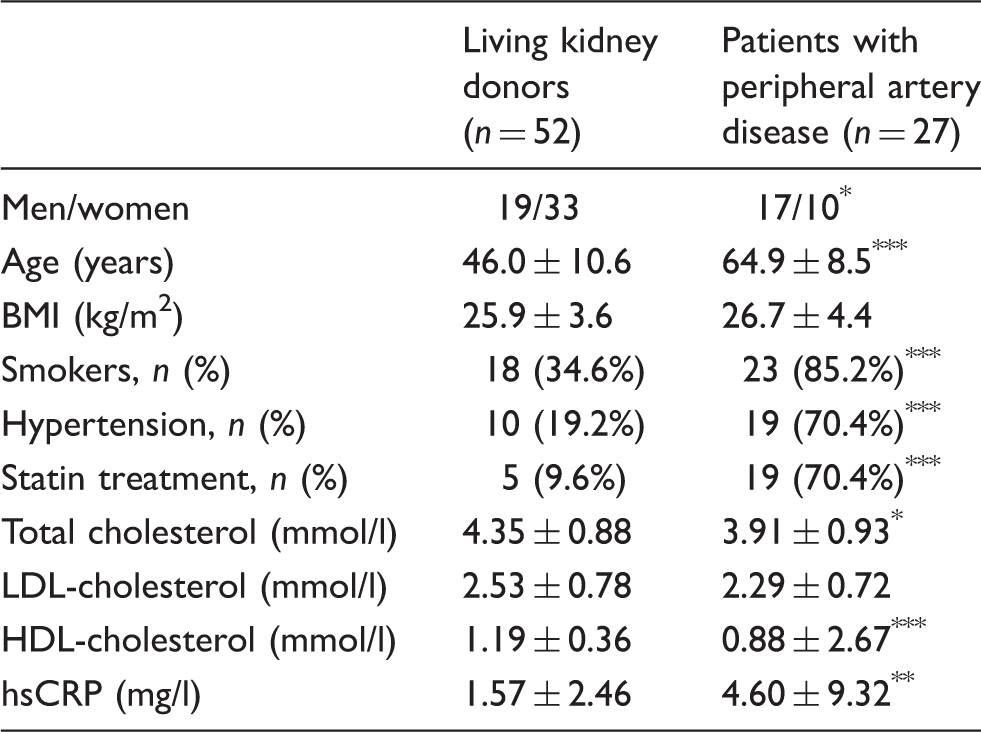
BMI: body mass index; LDL: low-density lipoprotein; HDL: high-density lipoprotein; hsCRP: high-sensitivity C-reactive protein.
Data are expressed as mean of the proportion ±SD or by risk factor incidence.
Statistical significance was determined with Fisher’s exact test for proportions and the Mann–Whitney unpaired test for continuous measurements (*P < 0.05; **P < 0.01; ***P < 0.001).
Different phenotypes of macrophages (%) isolated from adipose tissue.
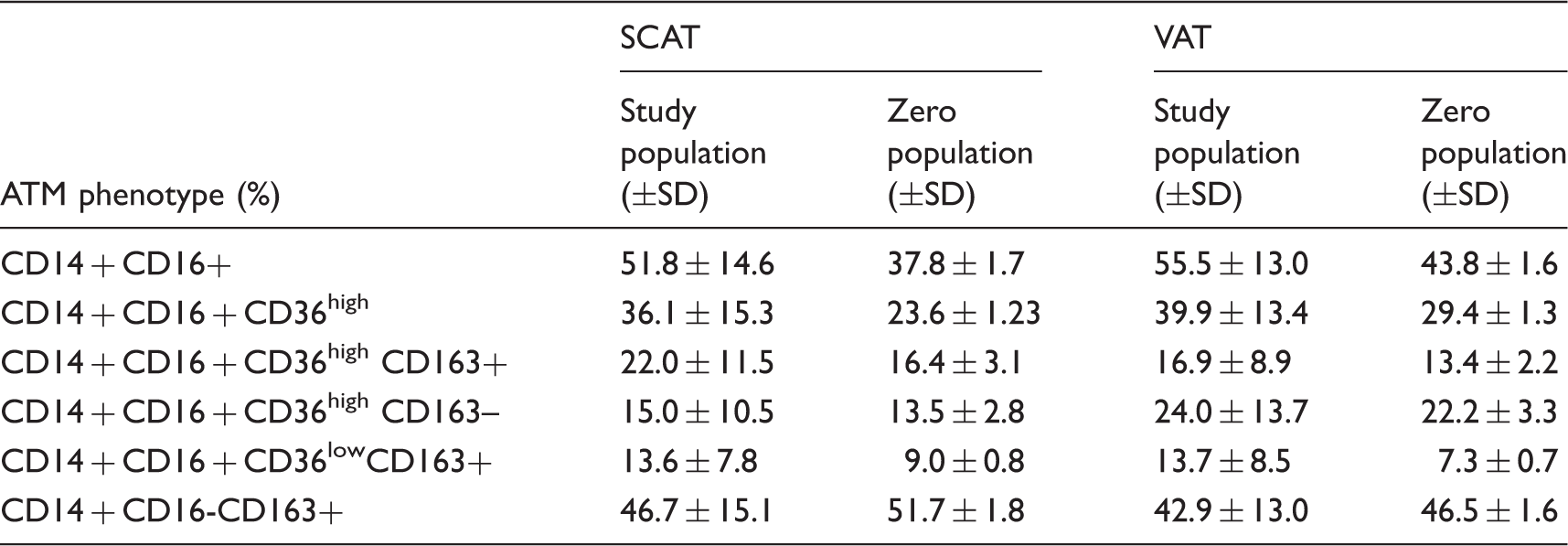
SCAT: subcutaneous adipose tissue; VAT: visceral adipose tissue; ATM: adipose tissue macrophages.
Proportions of ATM isolated from SCAT (n = 70) and VAT (n = 79) in study population and zero populations.
Results are expressed as mean of the proportion and standard deviation (±SD) in all study subjects or the zero population.
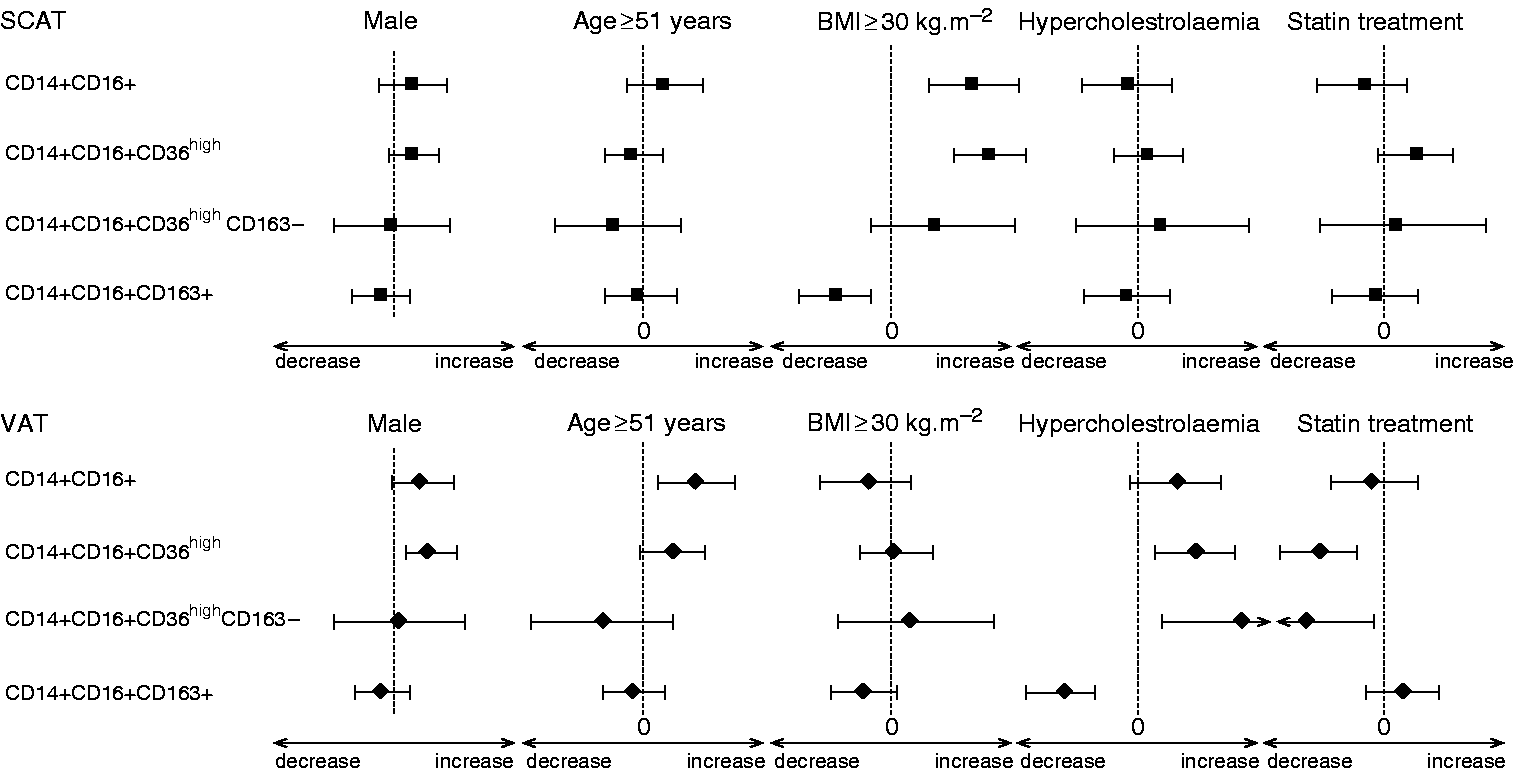
Predictors’ impact on the decrease or increase in macrophage subsets. Lines of forest plots represent differences of macrophage subsets between a present (1) and absent (0) predictor. If the line is outside zero, including the lower or upper limits, then the predictor increases or decreases the subset, respectively.
Populations with unclear phenotypes expressing both pro and anti-inflammatory markers (CD14 + CD16 + CD36high CD163+ and CD14 + CD16 + CD36lowCD163+) were designed as transitional macrophages and their relations to predictors are presented only in Supplementary materials.
Subcutaneous adipose tissue
No link of predictors of CVD with different phenotypes of macrophages in SCAT was displayed with the exception of BMI (Figure 1). Obese subjects (BMI ≥30 kg/m2) had a higher proportion of both likely pro-inflammatory as well as phagocytic pro-inflammatory phenotypes compared to the zero group (approximately 1.3 and 1.6-fold elevations, respectively). The anti-inflammatory fraction was proportionally decreased in obese subjects.
Visceral adipose tissue
Surprisingly adipose tissue accumulation did not influence the proportions of pro and anti-inflammatory macrophages in VAT. On the other hand, all other predictors of CVD (Figure 1) were related to macrophage subset proportions in this tissue. The older group of individuals (over 51 years of age) showed elevated proportions of the likely pro-inflammatory subpopulation and also the phagocytic pro-inflammatory fraction. In addition, an effect of sex on macrophage subsets was found in VAT. The phagocytic pro-inflammatory fraction was relatively higher in men than in women, with no effect on the proportion of the anti-inflamatory macrophages phenotype proportion.
Hyperchoesterolaemia, defined as a current cholesterol concentration higher than 5 mmol/l or statin treatment (based on previous medical examination), increased the proportion of phagocytic pro-inflammatory fractions (Figure 1). The hypercholesterolaemia-based 1.3-fold elevation of the proportion of phagocytic pro-inflammatory macrophages (Supplementary material and Supplementary Table 2) was highly relevant and also the increase in the proportion of the potentially pro-inflammatory fraction was very close to reach a relevant level. A substantial increase was also observed in the subfraction not expressing CD163 (CD14 + CD16 + CD36high and CD163–). In addition, subjects with hyperchosterolaemia had lower levels of the subset of anti-inflammatory macrophages in VAT.
Statin therapy had a notably decreasing impact on phagocytic pro-inflammatory macrophages in VAT. Although the hypercholesterolaemia-based 1.3-fold elevation of these populations, it was completely counterbalanced by the effect of statin treatment (by a factor of 0.7) (Figure 1 and Supplementary Table 2). However, our analysis did not document any effect of statin therapy on the subset of anti-inflammatory macrophages.
It is of interest that contrary to SCAT all three cardiovascular predictors, age, sex and hypercholesterolemia stimulated the proportion of pro-inflamatory fractions in VAT.
Discussion
Analysis of the proportions of pro-inflammatory, anti-inflammatory and transitional macrophages in human adipose tissue documented a different impact of the risk factors of CVD (sex, age, BMI and hypercholesterolaemia) as well as statin use on adipose tissue inflammatory status. The main contribution of our analysis is the finding of a direct effect of statin therapy on dampening of the pro-inflammatory changes of adipose tissue macrophages connected with hypercholesterolaemia independent of other risk factors.
As it is widely accepted that adipose tissue macrophages in vivo adopt the full spectrum of non-fully differentiated phenotypes,21,26 and their surface receptors have not yet been fully identified, we decided also to include transitional phenotypes of macrophages into Bayesian analysis. Based on current knowledge it can only be speculated that transitional phenotypes (both CD14 + CD16 + CD36highCD163+ and CD14 + CD16 + CD36low (CD163+)) are unpolarised subsets with a capacity to switch towards either side.
In accordance with our previous data analysing the proportion of pro-inflammatory macrophages in LKDs only, 27 BMI was related to these macrophages only in the SCAT of the whole set of LKDs and patients with established atherosclerosis (Figure 1). Relatively higher proportions of likely pro-inflammatory macrophages (CD14 + CD16+) as well as fully defined pro-inflammatory phagocytic macrophages were documented by mutually adjusted differences in accordance with crude differences (Supplementary Table 1). No effect of obesity was demonstrated in VAT (with the exception of a minor transitional fraction) in disagreement with published data 28 (Figure 1 and Supplementary Table 2). Nevertheless, other authors 29 also found a higher contribution of obesity to inflammation in SCAT compared to VAT.
Consistent with our earlier data, the effect of age, unlike obesity, was more pronounced in VAT 12 (Figure 1). In VAT, older age was associated with an increase in the proportion of the potentially pro-inflammatory phenotype when mutually adjusted and crude differences were evaluated (Figure 1 and Supplementary Table 2). Although, in the case of the most important pro-inflammatory phagocytic subset, the effect of age did not reach relevance, it is probable that this subset was also influenced by age as suggested by the marginal value of the lower limit of the 99% credibility interval. The effect of older age also manifested itself in the transitional CD14 + CD16 + CD36low(CD163+) fraction. These data are generally in agreement with our analysis of macrophages in the adipose tissue of healthy individuals; 12 while no effect of age was noted in men, a correlation was shown in women, especially postmenopausal individuals.
Relevant differences were also found between men and women. It must be emphasised that this result might be influenced by important and opposite differences between the sex ratio in LKDs and PAD patients (Table 1). A higher proportion of pro-inflammatory highly phagocytic and transitional macrophages was documented in the VAT of men; it should be stressed that diet and specially saturated fatty acids might be an important contributor. 30
An effect of age was likewise detected on likely pro-inflammatory macrophages and can be tracked also in a highly phagocytic subpopulation, but the relevance was only borderline. No effect of sex on anti-inflammatory macrophages was found.
While no relevant impact of hypercholesterolaemia on any of the different macrophage phenotypes was found in SCAT, this factor had a major effect on macrophage subsets in VAT (Figure 1). Subjects with hypercholesterolaemia showed increased proportions of pro-inflammatory, pro-atherosclerotic phenotypes either ‘likely’ or completely defined macrophages in VAT, whereas the proportion of the anti-inflammatory phenotype was relevantly lower in this tissue.
A large epidemiological prospective study 13 demonstrated an additional effect of statins on LDL lowering. A decreasing effect of statins on hsCRP concentrations suggested an influence on the pro-inflammatory status of the whole body. Many studies have demonstrated that adipose tissue is not only an energy regulator and endocrine organ, but plays a very important role in the body’s immune status. Our main results document a decreasing effect of statins on the proportion of pro-inflammatory macrophages in VAT (Figure 1). This might explain the proposed pleiotropic positive effect of statins.
A Bayesian analysis of the effects of sex, age, obesity, smoking, hypertension and hypercholesterolaemia on the proportion of pro-inflammatory phenotypes documented a fairly relevant effect of higher BMI (>30) in SCAT, but no effect in VAT. This is surprising as VAT is generally believed to play a dominant role in the adverse effects of adiposity. Other cardiovascular risk factors affected VAT more, in accordance with the prevalent approach.3,31 The effect of hypercholesterolaemia on the proportion of the pro-inflammatory macrophage phenotype was counterbalanced by including statin administration as an additional factor.
Based on our data we suppose that an unquestionably negative effect of smoking on atherosclerosis progression 32 is not mediated by adipose tissue inflammation status. The same seems to apply to hypertension so these two predictors of CVD manifest themselves through different mechanisms.
There are some limitations of the study that should be considered. First, we were not able to distinguish between the effect of hypertension and antihypertensive therapy as all hypertensive subjects were receiving some type of antihypertensive treatment at the same time. Second, based on our data we are unable to demonstrate causality of the association documented in our analysis.
Due to the wide spectrum of risk factor combinations (particularly in patients with confirmed atherosclerosis), we have been able to demonstrate a link among CVD risk factors, statin treatment and pro and anti-inflammatory macrophage subpopulations within adipose tissue. Our results also suggest the ambivalence of the transitional macrophage subpopulations. We also believe that the results of this study indicate an explanation for statin’s pleiotropic effect mechanisms. It might only be speculated whether dampening of adipose tissue inflammation is crucial to decrease the pro-inflammatory status of the organism as a whole. We believe that, regardless of causality, the reported links in our findings might be important for primary and secondary CVD prevention.
In conclusion, our analysis of the relationship of CVD risk factors and markers of macrophage polarisation in human adipose tissue showed that the pro-inflammatory status of adipose tissue is related to major CVD predictors.
Footnotes
Author contribution
IKL and RP contributed to the conception or design of the work, interpretation of data for the work and drafted the manuscript. MP and TT performed data analysis and critically revised the manuscript. SC, AK, LJ and JF contributed to data acquisition and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring its integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Ministry of Health, Czech Republic (00023001- institutional support and the grants 17-28103A and NT14009/3) to the Institute for Clinical and Experimental Medicine, Prague, Czech Republic.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.