
Abstract
Background
High levels of serum uric acid have been associated with adverse outcomes in cardiovascular diseases such as myocardial infarction and heart failure. The aim of the current study was to evaluate the prognostic role of serum uric acid levels in patients undergoing cardiac rehabilitation after myocardial revascularization and/or cardiac valve surgery.
Design
We performed an observational prospective cohort study.
Methods
The study included 1440 patients with available serum uric acid levels, prospectively followed for 50 ± 17 months. Mean age was 67 ± 11 years; 781 patients (54%) underwent myocardial revascularization, 474 (33%) cardiac valve surgery and 185 (13%) valve-plus-coronary artery by-pass graft surgery. The primary endpoints were overall and cardiovascular mortality while secondary end-points were combined major adverse cardiac and cerebrovascular events.
Results
Serum uric acid level mean values were 286 ± 95 µmol/l and elevated serum uric acid levels (≥360 µmol/l or 6 mg/dl) were found in 275 patients (19%). Overall mortality (hazard ratio = 2.1; 95% confidence interval: 1.5–3.0; p < 0.001), cardiovascular mortality (hazard ratio = 2.0; 95% confidence interval: 1.2–3.2; p = 0.004) and major adverse cardiac and cerebrovascular events rate (hazard ratio = 1.5; 95% confidence interval: 1.0–2.0; p = 0.019) were significantly higher in patients with elevated serum uric acid levels, even after adjustment for age, gender, arterial hypertension, diabetes, glomerular filtration rate, atrial fibrillation and medical therapy. Moreover, strong positive correlations between serum uric acid level and probability of overall mortality (p < 0.001), cardiovascular mortality (p < 0.001) and major adverse cardiac and cerebrovascular events (p = 0.003) were found.
Conclusions
Serum uric acid levels predict mortality and adverse cardiovascular outcome in patients undergoing myocardial revascularization and/or cardiac valve surgery even after the adjustment for age, gender, arterial hypertension, diabetes, glomerular filtration rate and medical therapy.
Introduction
The association is well documented between serum uric acid (SUA) levels and several cardiovascular conditions, including hypertension, 1 metabolic syndrome, 2 coronary artery disease, 3 cerebrovascular disease, 4 vascular dementia, 5 preeclampsia 6 and kidney disease.7,8 This relationship has been observed not only with hyperuricemia but also with SUA levels considered in the normal to high range9,10 and further studies have suggested that SUA may be an independent risk factor for both cardiovascular11–13 and renal disease. 14 In secondary cardiovascular prevention, high SUA levels have been associated with adverse outcomes in post-myocardial infarction 15 and heart failure patients 16 and, more recently, with the severity of mitral and aortic valve disease.17,18 However, no studies have so far evaluated whether hyperuricaemia also plays a role in the long-term outcome of subjects undergoing myocardial revascularization and/or cardiac valve surgery; therefore, the present work aimed to elucidate the prognostic significance of SUA levels in these patients.
Methods
From January 2007 to June 2012 we prospectively collected data of consecutive patients undergoing cardiac rehabilitation after myocardial revascularization and/or cardiac valve surgery. One thousand four hundred and forty patients (72% men, mean age of 67 ± 11 years), with available SUA levels were included in the current study; the internal review board approved data collection. All patients completed a standard in-hospital cardiac rehabilitation programme, lasting approximately two weeks, consisting in supervised exercise sessions (120 minutes per day), lifestyle and risk factor management, counselling and medical therapy optimization. Anamnestic data and demographics, clinical and laboratory variables including SUA levels, electrocardiographic and echocardiographic measurements, coronary angiography data, physical activity parameters and pharmacological therapy adherence were collected for each patient at the discharge from the cardiac rehabilitation programme. Outcomes were recorded by a medical doctor through a telephonic questionnaire, by collecting medical records and/or discussing with the general practitioner; all included patients provided oral informed consent. The primary endpoints were overall and cardiovascular mortality; secondary endpoints were combined major adverse cardiac and cerebrovascular events (MACCEs), including cardiovascular mortality, non-fatal acute coronary syndrome (ACS), heart failure or stroke.
Statistical analysis
Continuous variables were expressed as mean and standard deviation (SD), categorical variables as number (n) and percentage (%). The Student two-sample t test and Pearson χ2 test were used to compare the differences between groups for continuous and categorical variables, respectively.
Binary regression was used to analyse the relationship between increasing SUA levels (continuous variable) and the risk of events. Cox proportional hazard regression analysis was performed to create event-free survival curves. Multivariate Cox regression analysis was used to create adjustment of hazard ratio for age, gender, arterial hypertension, diabetes, glomerular filtration rate (GFR), atrial fibrillation at discharge and medical therapy. The proportional-hazards assumption was checked for every Cox analysis. Time to event for survival-free analysis was measured from admission to the first event. Significance was defined as a p value <0.05. All statistics were performed with SPSS version 23 (IBM Corporation).
Results
Demographic and clinical characteristics
The study included 1440 patients; 870 patients (60%) reported arterial hypertension and 372 (26%) type 2 diabetes, 781 patients (54%) underwent myocardial revascularization, 474 (33%) cardiac valve surgery and 185 (13%) valve-plus-coronary artery by-pass graft surgery. Five hundred and seventy-three patients (40%) underwent cardiac revascularization after ACS and 213 (15%) after stable angina or silent ischaemia; 157 patients (11%) underwent cardiac surgery for mitral disease and 342 (24%) for aortic disease, 135 (9%) for valve plus coronary artery disease while 20 patients (1%) for other clinical indications (e.g. tricuspid valve disease, aortic aneurysm, atrial masses). At discharge, atrial fibrillation was reported in 483 patients (33%), while in 957 patients (67%) sinus rhythm was found.
Baseline characteristics.
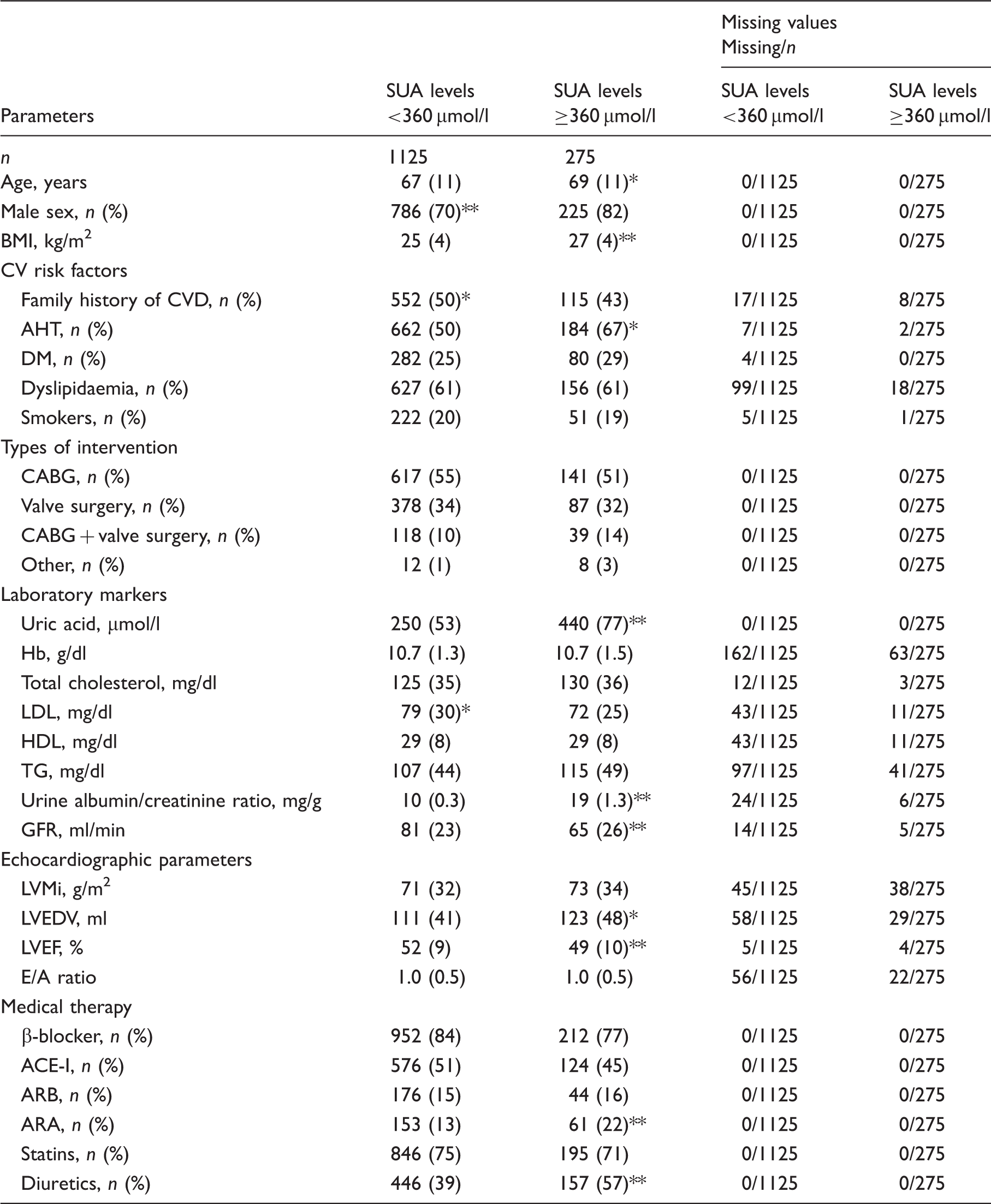
Values are expressed as mean and standard deviation or as number and percentage.
and **indicate differences at significance levels p < 0.05 and p < 0.01 respectively.
SUA: serum uric acid; CV: cardiovascular; CVD; cardiovascular disease; AHT; arterial hypertension; DM; diabetes mellitus; CABG; coronary artery by-pass graft; Hb: haemoglobin; HDL: high-density lipoprotein; LDL: low-density lipoprotein; TG: triglycerides; GFR: glomerular filtration rate; LVMi: left ventricular mass index; LVEDV: left ventricular end-diastolic volume; LVEF: left ventricular ejection fraction; ACE-I: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; ARA: aldosterone receptor antagonist
Mean follow-up was 50 ± 17 months. All-cause mortality rate was 11% (158 deaths); the total amount of MACCEs was 238 (16%), composed of 89 cardiovascular deaths (6%), 58 heart failure hospitalizations (4%), 59 ACSs (4%) and 32 strokes (2%).
Primary endpoints
Overall mortality rate was 2.3-fold higher in patients with elevated SUA level (hazard ratio = 2.3; 95% confidence interval (CI): 1.6–3.2; p < 0.001) (Figure 1(a)), which remained independent predictor of mortality even after adjustment for age, gender, arterial hypertension, diabetes, GFR, atrial fibrillation and concomitant use of diuretics, angiotensin-converting enzyme (ACE)-inhibitors, angiotensin receptor blockers (ARBs), aldosterone receptor antagonists (ARAs), beta-blockers and statins (hazard ratio = 2.0; 95% CI: 1.4–2.9; p < 0.001). Its predictive role for overall mortality was confirmed when ischaemic heart disease (hazard ratio = 2.5; 95% CI: 1.5–4.1; p < 0.001) and cardiac valve disease (hazard ratio = 2.9; 95% CI: 1.6–5.3; p < 0.001) were considered separately.
SUA levels and survival free from overall mortality (a), cardiovascular mortality (b) and MACCEs (c).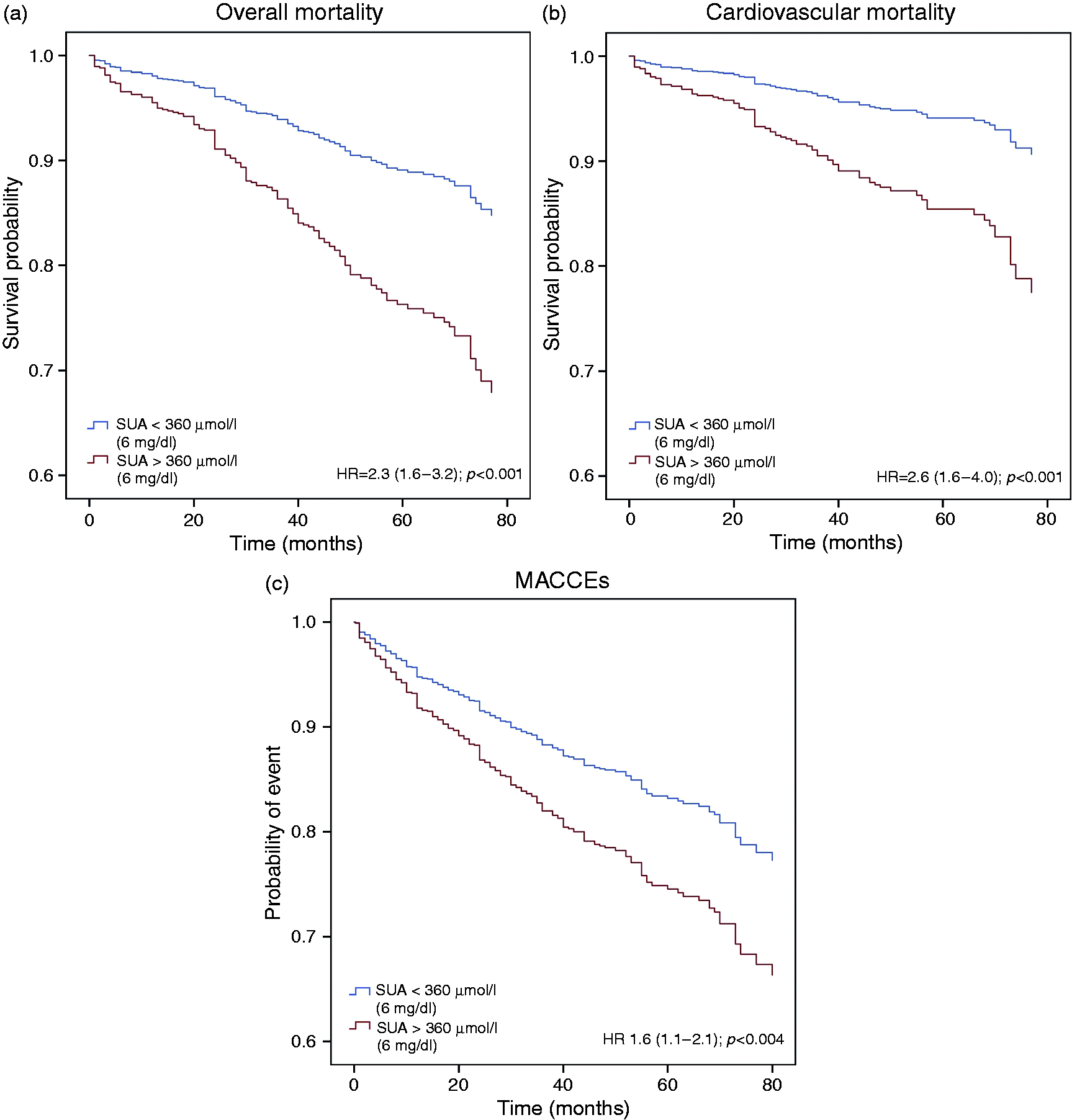
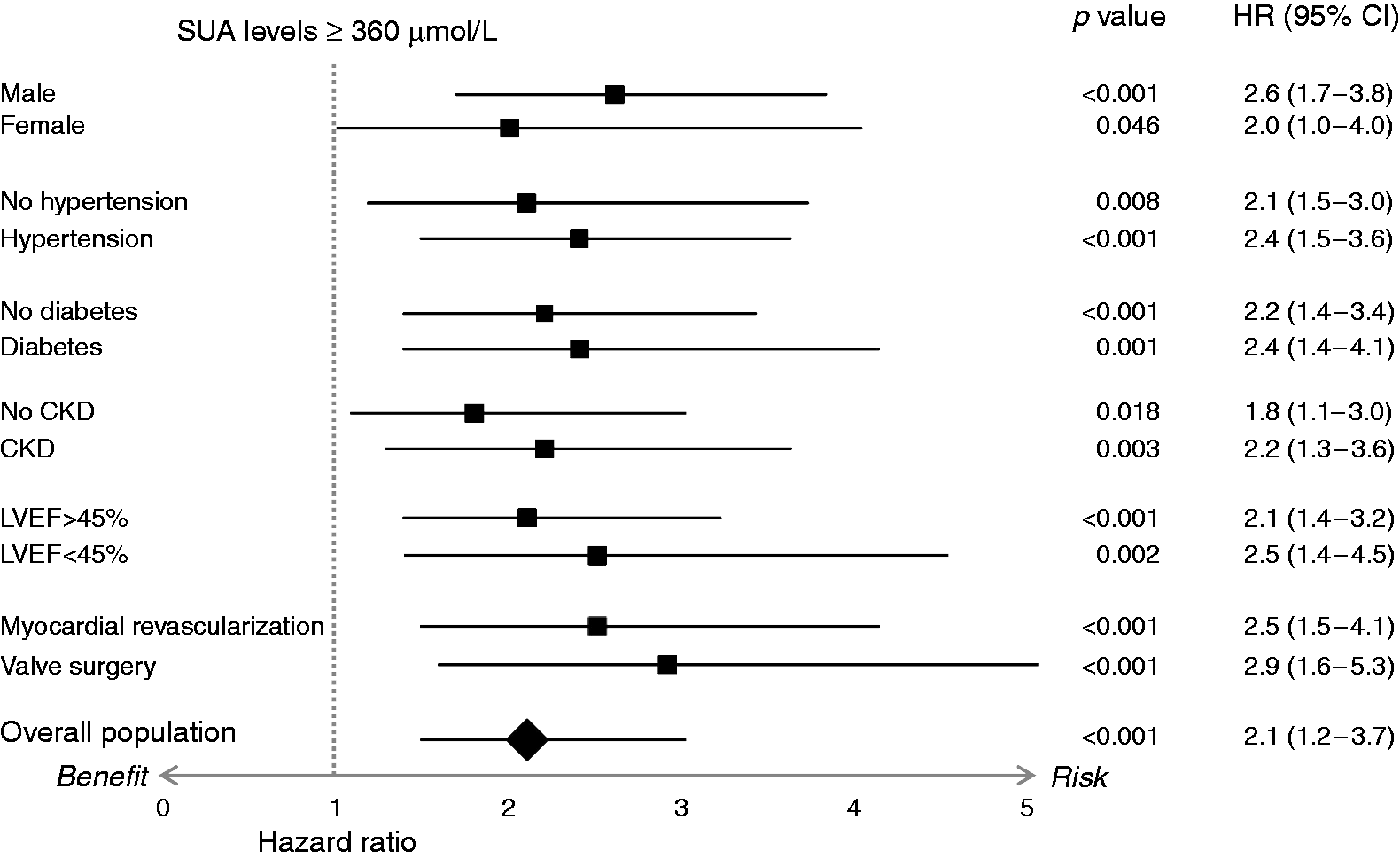
SUA levels and probability of overall mortality were strongly correlated (hazard ratio: 1.23; p < 0.001; Figure 2(a)) with 23% increase of relative risk for each 60 µmol/l (or 1 mg/dl) increase of SUA levels. After dividing the patients’ population according to gender, arterial hypertension, diabetes, GFR, LVEF and type of intervention, the overall mortality rate was significantly higher in patients with elevated SUA levels (Figure 3).
Correlation between increasing SUA levels and probability of overall mortality (a), cardiovascular mortality (b) and MACCEs (c). Hazard ratio for overall mortality rate in total population and after dividing it according to gender, arterial hypertension, diabetes, CKD, LVEF and type of intervention.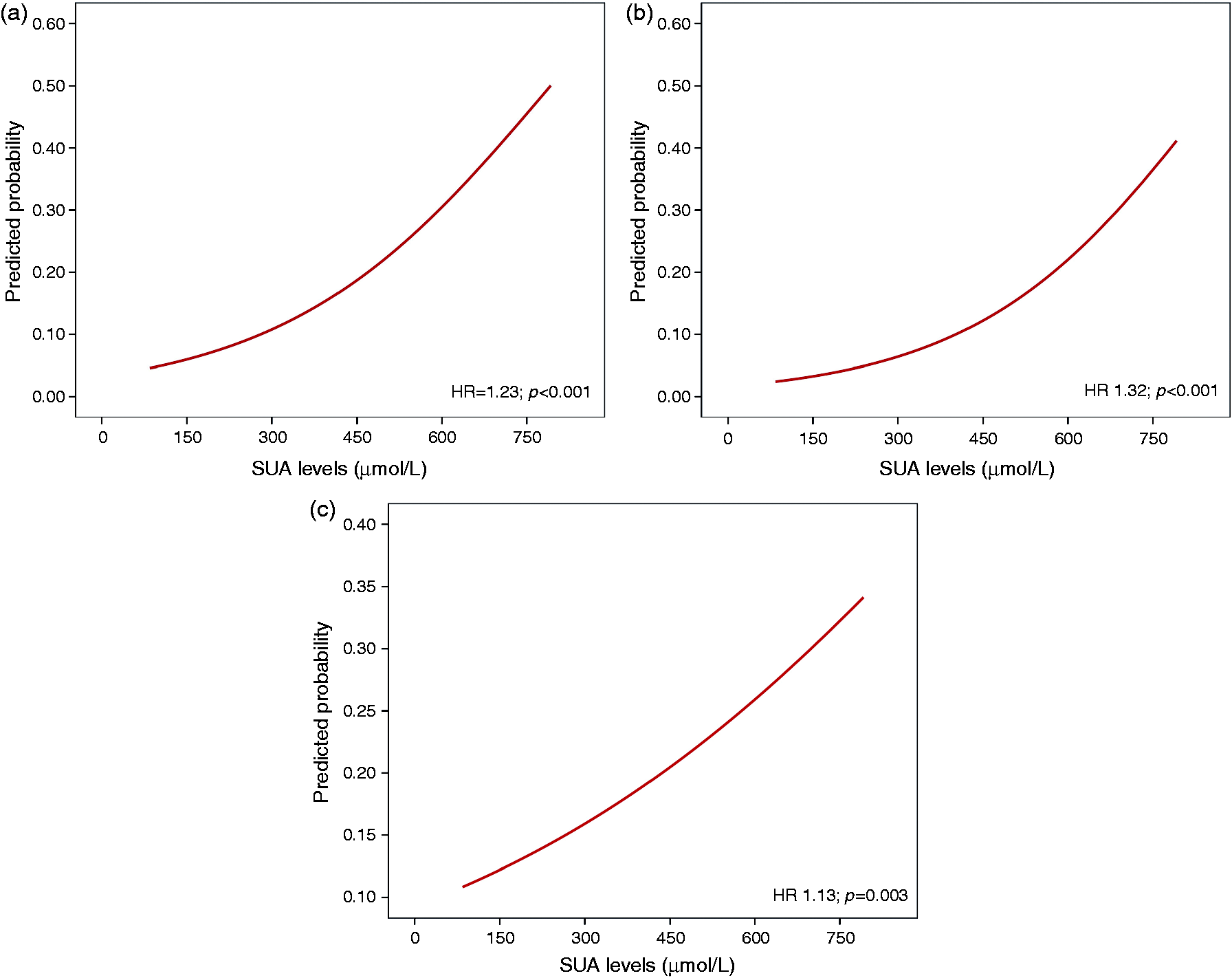
Cardiovascular mortality rate was 2.6-fold higher in patients with elevated SUA levels (hazard ratio = 2.6; 95% CI: 1.6–4.0; p < 0.001; Figure 1(b)). Elevated SUA levels remained an independent predictor of cardiovascular mortality even after adjustment for age, gender, arterial hypertension, diabetes, GFR, atrial fibrillation, type of intervention, and concomitant use of diuretics, ACE-inhibitors, ARBs, ARAs, beta-blockers and statins (hazard ratio = 2.0; 95% CI: 1.2–3.2; p = 0.003). Moreover, a strong correlation between increasing SUA levels and increasing probability of cardiovascular mortality was found (hazard ratio: 1.32; p < 0.001) with 32% increase of relative risk for each 60 µmol/l (or 1 mg/dl) increase of SUA levels (Figure 2(b)).
Secondary endpoints
Serum uric acid levels ≥360 µmol/l and unadjusted hazard ratio for overall mortality and MACCEs.
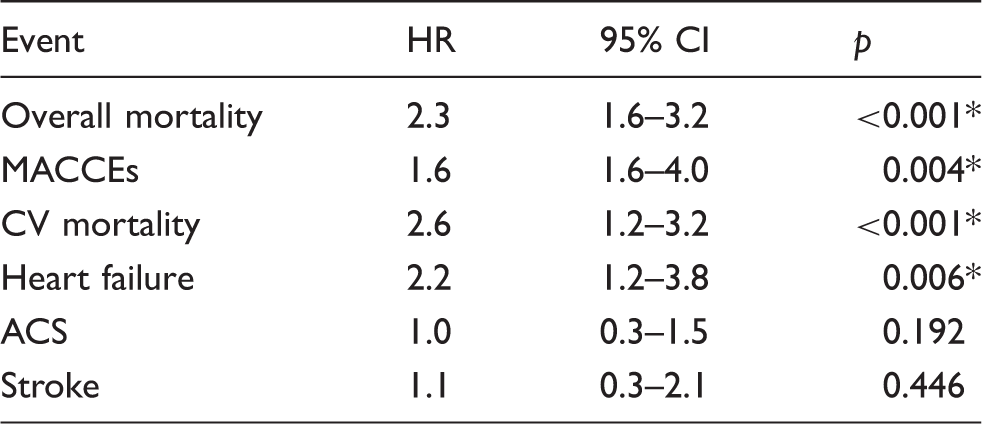
MACCE: major adverse cardiovascular and cerebrovascular event; HR: hazard ratio; CI: confidence interval; CV: cardiovascular; ACS: acute coronary syndrome. *indicate differences at significance levels p<0.05.
Discussion
This study demonstrates an independent prognostic role of SUA levels in secondary cardiovascular prevention. More specifically, our data indicate that SUA level predicts overall and cardiovascular mortality as well as MACCEs independently of age, gender, arterial hypertension, diabetes, GFR, LVEF, atrial fibrillation and medical therapy. They also show a strong correlation between increasing SUA levels and risk of death and MACCEs. Furthermore, our results seem to confirm not only the previously reported prognostic value of SUA levels in patients with ischaemic heart disease, but also in subjects never investigated before such as those undergoing cardiac valve surgery.
Although an association of gout with arterial hypertension, diabetes, renal and cardiovascular disease has been observed since the late 19th century, the role of uric acid in the development of cardiovascular disease was largely ignored until the mid-1950s 19 and early 1960s, 1 when it was rediscovered. Since then, a large number of epidemiologic studies have suggested an association between SUA levels and several cardiovascular conditions, including hypertension, 1 metabolic syndrome, 2 coronary artery disease, 3 cerebrovascular disease, 4 vascular dementia, 5 preeclampsia 6 and kidney disease.7,8 Experimental and human studies have provided several possible pathophysiological links between SUA and cardiovascular disease, showing an association between SUA levels and endothelial dysfunction, 20 activation of the renin–angiotensin system, 21 cellular proliferation, 22 systemic inflammation, 23 oxidative stress 24 and salt-sensitive kidney-dependent hypertension. 25 Nevertheless, the relative importance of the above-cited associations remains controversial and whether SUA can be considered an independent cardiovascular risk factor is still an open issue.26,27
In primary cardiovascular prevention, the role of SUA levels as independent risk factor for all-cause and cardiovascular death was demonstrated in a general population in the MONICA Augsburg study, 28 in The First National Health and Nutrition Study 11 and also in hypertensive patients, in whom the prognostic value of SUA levels was confirmed even when adjusted for the use of diuretics and the presence of other cardiovascular risk factors. 12 Furthermore, Niskanen et al. reported a strong correlation between SUA levels and cardiovascular mortality in healthy middle-aged men, independent of variables commonly associated with gout or the metabolic syndrome. 13 Similar results were also confirmed in the Rotterdam Study and in the Atherosclerosis Risk in Communities (ARIC) Study, in which high SUA levels strongly predicted both myocardial infarction (MI) and stroke, independently of other vascular risk factors, and in the ARIC study this association was also found in subjects not taking diuretics.29,30 More recently, a Mendelian randomization analysis including 17 prospective observational studies showed a modest independent causal association between SUA and risk of coronary heart disease. 31
In comparison with the relevant amount of data available in primary cardiovascular prevention, the evidence in favour of a prognostic role of SUA levels in a setting of secondary cardiovascular prevention is quite scarce.
In patients with established coronary artery disease, SUA levels predicted mortality 32 and, in Multiple Risk Factor Intervention Trial database, multivariable regression analysis indicated SUA levels as an independent risk factor after acute MI. 33 Finally, in patients with moderate to severe chronic heart failure, high SUA levels represented an independent marker of adverse prognosis.16,34
In a specific condition of secondary cardiovascular prevention never considered before, such as ischaemic heart disease and/or cardiac valve disease undergoing cardiac rehabilitation, our data confirm the strong prognostic significance of SUA levels, and an interesting finding of the current study was the demonstration of a prognostic role of SUA levels in predicting overall and cardiovascular death also in patients with cardiac valve disease. Although an association between SUA levels and the severity of both mitral regurgitation 17 and aortic stenosis 18 has been recently shown, to the best of our knowledge our results provide the first evidence of the prognostic relevance of SUA levels in patients undergoing cardiac valve surgery. Given that cardiac valve calcification and atherosclerosis share similar pathophysiologic pathways, 35 it cannot be excluded that SUA levels could influence, through common mechanisms, long-term prognosis of both valve and ischaemic heart disease.
Limitations include the lack of information concerning urate-lowering drugs effect or specific markers of oxidative stress and endothelial dysfunction; in fact, this study was designed to assess the prognostic role of SUA levels and not the safety or efficacy of reducing SUA concentration through a targeted therapeutic approach such as urate-lowering drugs or anti-inflammatory drugs. 36 Moreover, this observational study is prone to the classical biases of this type of design, such as confounding, selection and information biases. Finally, as SUA level was measured only at the discharge from the cardiac rehabilitation programme, our study cannot provide information on the effect of SUA level changes over time.
In conclusion, SUA level independently predicted mortality and adverse cardiovascular outcome in subjects undergoing myocardial revascularization and/or cardiac valve surgery. Future randomized, controlled trials or meta-analyses will be needed to determine whether SUA level should be a target for specific medical therapy in these patients.
Footnotes
Author contribution
DL, MB, UC, PCo: contributed to the conception, design, acquisition, analysis and interpretation of data. DB, SG: contributed to the acquisition and analysis of data. PCa: contributed to the analysis and interpretation of data. LM, PTU, LB, VB: contributed to the interpretation of data. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Acknowledgement
We thank all the students of Parma University Medical School who took part in the creation of our registry; their time spent on data collection was essential for the realization of the present study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.