
Abstract
Background
Preliminary evidence suggests that peak exercise oxygen pulse – peak oxygen uptake/heart rate-, a variable obtained during maximal cardiopulmonary exercise testing and a surrogate of stroke volume, is a predictor of mortality. We aimed to assess the associations of peak exercise oxygen pulse with sudden cardiac death, fatal coronary heart disease and cardiovascular disease and all-cause mortality.
Design
A prospective study.
Methods
Peak exercise oxygen pulse was assessed in a maximal cycling test at baseline in 2227 middle-aged men of the Kuopio Ischaemic Heart Disease cohort study using expired gas variables and electrocardiograms. Relative peak exercise oxygen pulse was obtained by dividing the absolute value by body weight.
Results
During a median follow-up of 26.1 years 1097 subjects died; there were 220 sudden cardiac deaths, 336 fatal coronary heart diseases and 505 fatal cardiovascular diseases. Relative peak exercise oxygen pulse (mean 19.5 (4.1) mL per beat/kg/102) was approximately linearly associated with each outcome. Comparing extreme quartiles of relative peak exercise oxygen pulse, hazard ratios (95% confidence intervals) for sudden cardiac death, fatal coronary heart disease and cardiovascular disease, and all-cause mortality on adjustment for cardiovascular risk factors were 0.55 (0.36–0.83), 0.58 (0.42–0.81), 0.60 (0.46–0.79) and 0.59 (0.49–0.70), respectively (P < 0.001 for all). The hazard ratios were unchanged on further adjustment for C-reactive protein and the use of beta-blockers. The addition of relative peak exercise oxygen pulse to a cardiovascular disease mortality risk prediction model significantly improved risk discrimination (C-index change 0.0112; P = 0.030).
Conclusion
Relative peak exercise oxygen pulse measured during maximal exercise was linearly and inversely associated with fatal cardiovascular and all-cause mortality events in middle-aged men. In addition, relative peak exercise oxygen pulse provided significant improvement in cardiovascular disease mortality risk assessment beyond conventional risk factors.
Keywords
Introduction
Cardiorespiratory or aerobic fitness, as measured by peak oxygen uptake (VO2), has been one of the most widely examined cardiopulmonary exercise testing (CPX) variables, particularly as it relates to functional capacity and human performance.1,2 In previous cohort studies, peak VO2 has been shown to be inversely and independently associated with incident cardiovascular disease (CVD) events, cardiovascular and total mortality.3–7 Evidence also suggests that peak VO2 adds additional prognostic value beyond established risk factors in predicting vascular disease and mortality risk.3,8,9
Stroke volume response is one of the most important measures of cardiac performance during exercise.10,11 Exercise oxygen pulse, a surrogate for stroke volume, has emerged as an important variable which is obtained during CPX. Peak exercise oxygen pulse (peO2p) is expressed as oxygen consumed per heart beat at maximal CPX and it is related to the risk of cardiovascular events. 12
There is evidence to show that a high peO2p is inversely related to all-cause mortality.10,13 However, data on the value of utilising peO2p as a risk assessment tool for serious and specific adverse events such as sudden cardiac death (SCD) and fatal coronary heart disease (CHD) are lacking. Although in the literature, peO2p is often expressed by its absolute value (i.e. mL/beat), its magnitude is obviously related to body dimensions. Thus, ideally, similarly to peak VO2, it should be expressed in relative form, that is, by dividing its absolute value by body weight. 11 Given the relative ease in which this exercise testing variable can be assessed non-invasively using expired gases analysis, it will be clinically relevant to know if relative peO2p is a significant risk marker for fatal cardiovascular events and if it adds additional information beyond well-established cardiovascular risk factors. Our primary aim was to assess the nature and magnitude of the associations of relative peO2p with the risk of SCD, fatal CHD and CVD events, and all-cause mortality using a population-based prospective cohort study. A secondary aim was to evaluate whether the addition of relative peO2p measurements to conventional cardiovascular risk factors could improve the prediction of CVD mortality.
Methods
Study population
The strengthening the reporting of observational studies in epidemiology (STROBE) guidelines for reporting observational studies in epidemiology were used in this study (Supplementary Appendix). 14 Data analysis was undertaken in participants of the Finnish Kuopio Ischemic Heart Disease (KIHD) risk factor study, a prospective general population-based cohort study which aimed to study related risk factors for atherosclerotic CVD and other related chronic disease outcomes to aerobic performance. A detailed description of the study design, objectives and sampling strategy has previously been reported. 15 The KIHD cohort was recruited from a representative sample of 3433 men aged 42–61 years who were living in the city of Kuopio (Finland) and its surrounding communities. Of this number, 3235 men were found to be eligible for inclusion and 2682 (82.9%) volunteered to participate in the study. Baseline examinations were performed between March 1984 and December 1989. For the current analysis, 2227 men with complete information on relative peO2p, relevant covariates and fatal outcomes were included. The medical ethics committee of the University of Eastern Finland approved the study protocol, which was conducted in accordance with the Declaration of Helsinki. All study participants provided written informed consent.
Assessment of peak oxygen pulse
All participants underwent a morning symptom-limited cycling exercise testing. 16 with breath-by-breath respiratory gas analysis (Medical Graphics, USA). Peak VO2 was assessed as previously described5,16 and peO2p was calculated by dividing the measured peak VO2 by the maximum exercise heart rate, obtained from electrocardiogram, and was expressed in mL/beat. To remove the influence of body weight on the magnitude of peO2p, values of peO2p were then divided by weight in kilograms to yield relative peO2p. All results were multiplied by 100 for easier readability, as previously described.11,17 To ensure safety, all tests were supervised by an experienced physician and nurse.
Assessment of covariates
Baseline data were obtained by history, questionnaire administration, physical examinations and measurements as detailed elsewhere.18,19 Fasting cholesterol contents of serum lipoprotein fractions, triglycerides, plasma glucose and serum high sensitivity C-reactive protein (hsCRP) were obtained from analysis of blood samples. Smoking, prevalent diseases and regular and current use of medications were assessed by standardised self-administered questionnaires. 18 Alcohol consumption was assessed using the Nordic alcohol consumption inventory. Resting blood pressure was measured before the CPX with a random-zero sphygmomanometer. The history of CHD was based on a previous myocardial infarction, angina pectoris, use of nitroglycerin for chest pain once a week or more frequently or typical chest pain. The amount of physical activity was assessed from a 12-month physical activity history modified from the Minnesota leisure-time physical activity questionnaire, 20 and expressed in kJ/day. 16
Ascertainment of outcomes
All SCD, fatal CHD and CVD, and all-cause mortality events were ascertained from hospital documents, discharge lists, death certificates, informant interviews, health practitioner questionnaires, study electrocardiograms, medico-legal reports and vital statistics offices from study enrollment through to the end of 2014. The diagnostic classification of SCDs was based on symptoms, electrocardiographic findings, cardiac enzyme elevations, autopsy findings and history of CHD plus clinical findings and information from hospital and paramedic staff, details of which have previously been described.5,19,21 CVD deaths were coded using the tenth International Classification of Diseases codes. Documents were cross-checked in detail by two physicians.
Statistical analysis
The baseline characteristics of study participants were summarised using descriptive statistics (i.e. means, medians and percentages). Cross-sectional associations of relative peO2p with risk markers were assessed by calculating age-adjusted partial correlation coefficients. Hazard ratios (HRs) with 95% confidence intervals (CIs) for SCD, fatal CHD and CVD events, and all-cause mortality were calculated using Cox proportional hazard models after confirmation of the proportionality-hazards assumption using Schoenfeld residuals. The shape of the association between relative peO2p and each fatal outcome was characterised by calculating the HRs within quartiles of baseline relative peO2p and plotting these against the mean values of relative peO2p within each quartile using floating variances as described previously.22,23 We modelled our exposure as both continuous (per standard deviation (SD) increase) and categorical (quartiles) variables. HRs were progressively adjusted for: (a) age (model 1); (b) systolic blood pressure (SBP), total cholesterol, high-density lipoprotein (HDL) cholesterol, smoking status, alcohol consumption, prevalent CHD, history of diabetes mellitus and amount of physical activity (model 2); and (c) hsCRP and use of beta-blockers (model 3). Subgroup analyses were performed using interaction tests to assess statistical evidence of effect modification by relevant clinical characteristics. To assess whether adding information on relative peO2p to documented established risk factors is associated with an improvement in prediction of CVD mortality risk, we calculated measures of discrimination for censored time-to-event data (Harrell’s C-index) 24 and reclassification.25,26 To investigate the change in C-index, we added relative peO2p to a CVD mortality risk prediction model (i.e. age, SBP, history of diabetes, total cholesterol, HDL-cholesterol and smoking). Reclassification analysis was restricted to the first 10 years and was assessed using the net reclassification improvement (NRI).25,26 Given that we used CVD mortality as the outcome, we followed European guidelines 27 to determine clinically meaningful risk categories. Reclassification analyses were based on predicted 10-year CVD mortality risk categories of low (<1%), intermediate (1 to <5%) and high (≥5%) risk. All statistical analyses were conducted using Stata version 14 (Stata Corp, College Station, USA).
Results
Baseline characteristics and correlates of relative peO2p
Baseline participant characteristics and correlates of relative peak exercise oxygen pulse.
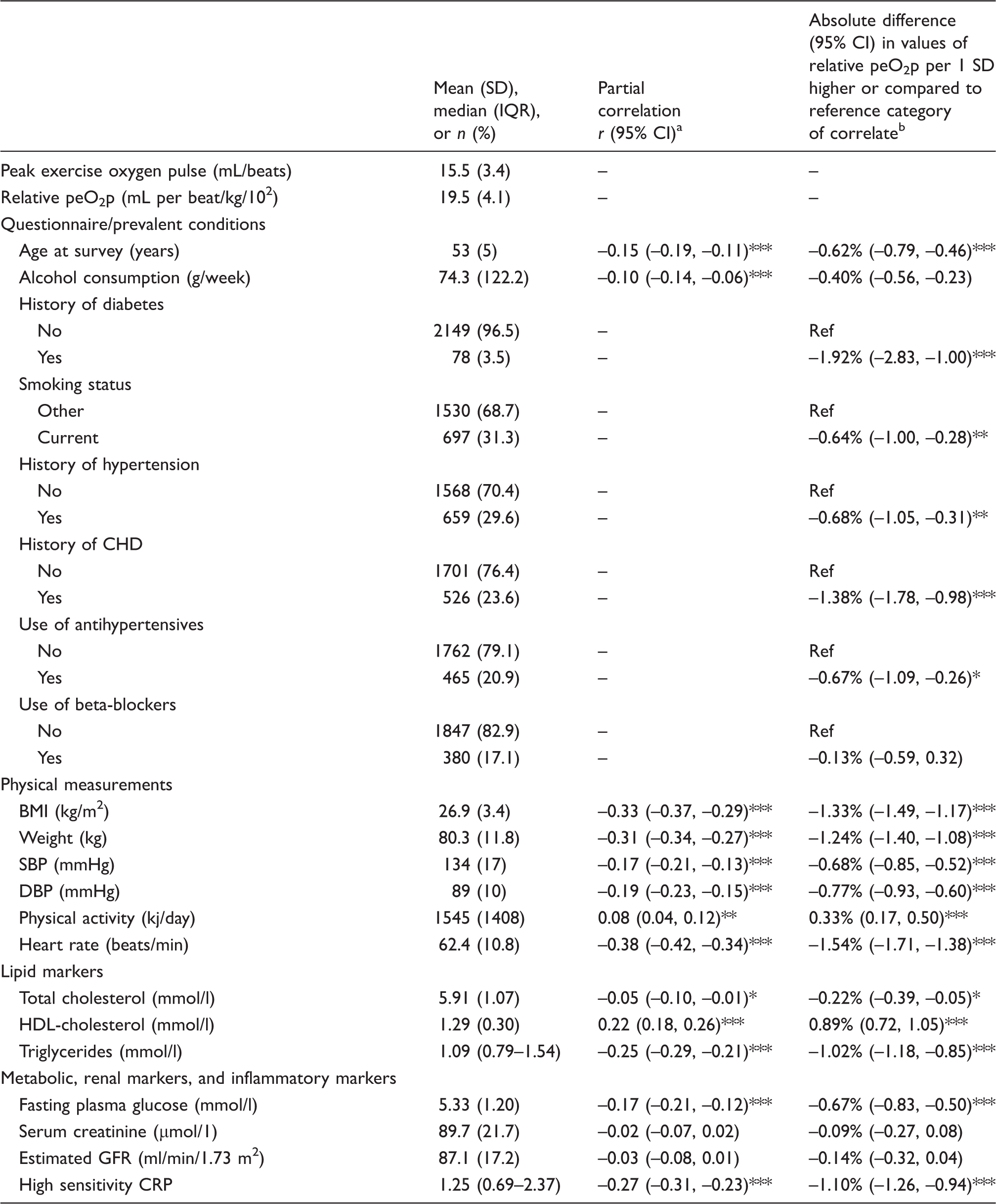
CI: confidence interval; BMI: body mass index; CHD: coronary heart disease; CRP: C-reactive protein; DBP: diastolic blood pressure; GFR: glomerular filtration rate; HDL: high-density lipoprotein; IQR: interquartile range; peO2p: peak exercise oxygen pulse; SD: standard deviation; SBP: systolic blood pressure.
Partial correlation coefficients between relative peO2p and the row variables.
Absolute change in values of relative peO2p per 1 SD increase in the row variable (or for categorical variables, the absolute difference in mean values of relative peO2p for the category vs. the reference) adjusted for age.
Asterisks indicate the level of statistical significance: *P < 0.05; **P < 0.01; ***P < 0.001.
Relative peO2p and mortality
Associations of relative peak exercise oxygen pulse with sudden cardiac death, fatal coronary heart disease, fatal cardiovascular disease, and all-cause mortality.
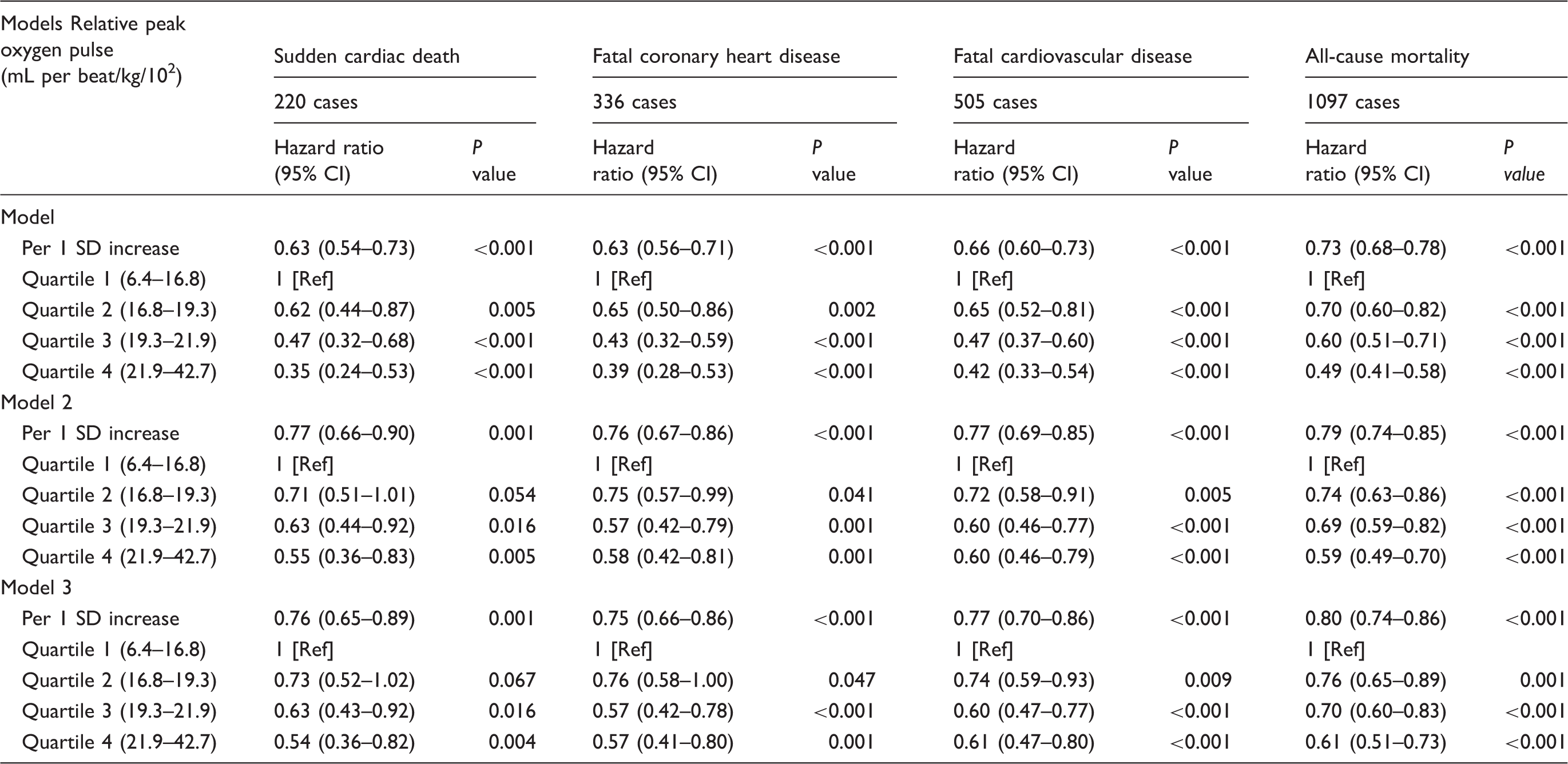
Model 1: adjusted for age.
Model 2: model 1 plus systolic blood pressure, total cholesterol, high-density lipoprotein cholesterol, smoking status, alcohol consumption, prevalent coronary heart disease, history of diabetes mellitus, and physical activity.
Model 3: model 2 plus high sensitivity C-reactive protein and use of beta-blockers.
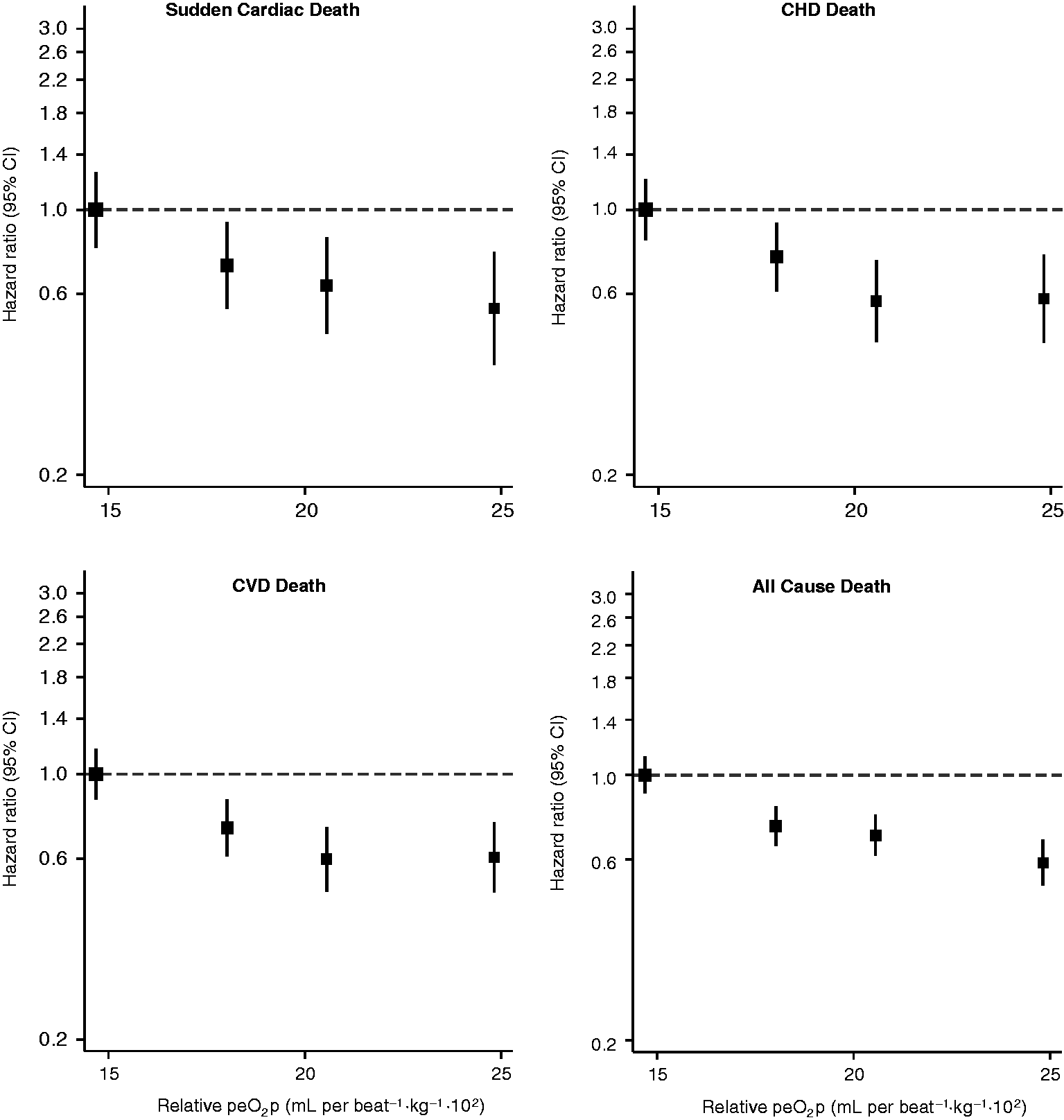
Hazard ratios (HRs) for sudden cardiac death, fatal coronary heart disease (CHD), fatal cardiovascular disease (CVD), and all-cause mortality by quartiles of relative peak exercise oxygen pulse (peO2p). HRs were adjusted for age, body mass index, systolic blood pressure, total cholesterol, high-density lipoprotein cholesterol, smoking status, alcohol consumption, prevalent CHD, a history of diabetes mellitus and physical activity. CI: confidence interval.
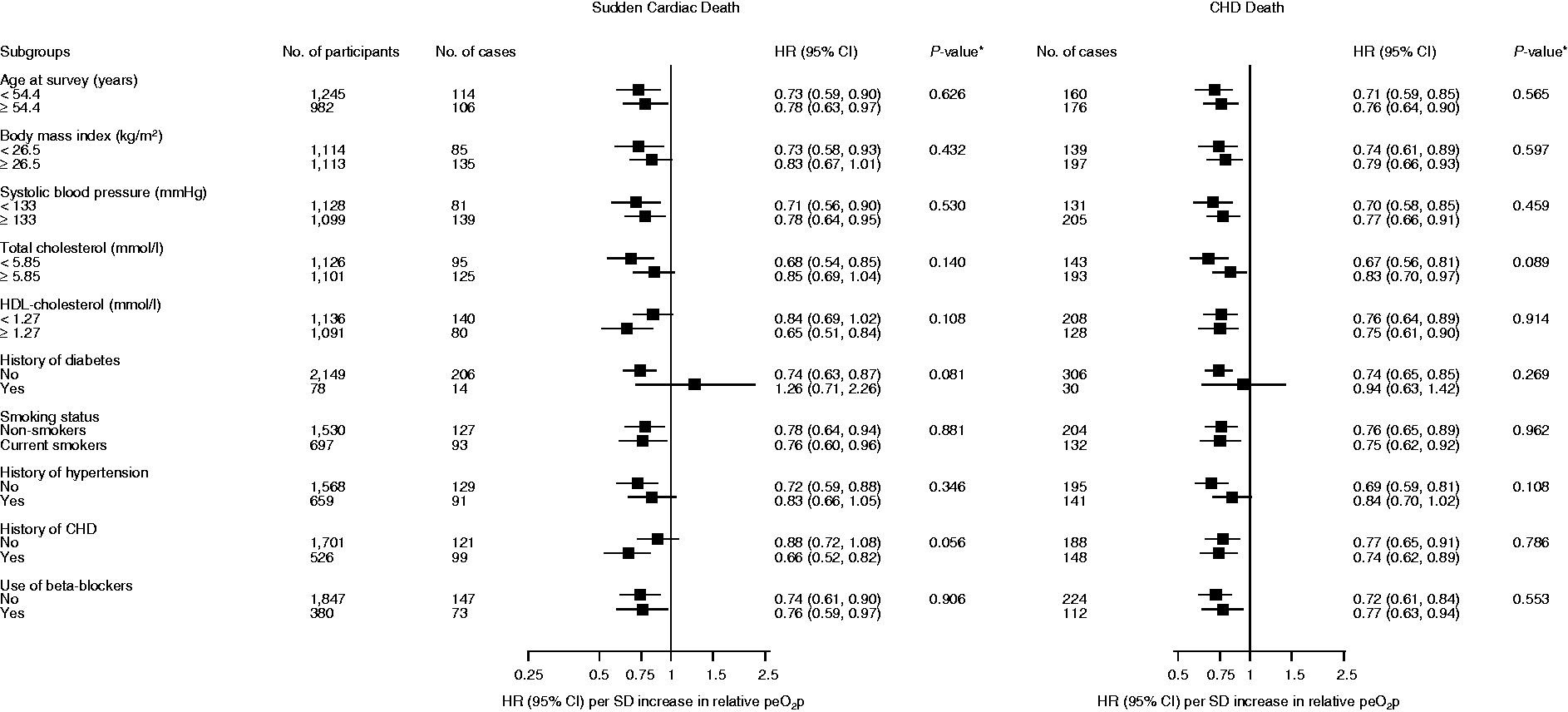
Hazard ratios (HRs) per one standard deviation (SD) change (4.1 mL per beat/kg/102) in relative peak exercise oxygen pulse (peO2p) for sudden cardiac death and fatal coronary heart disease (CHD) by several participant characteristics. HRs were adjusted for age, systolic blood pressure, total cholesterol, high-density lipoprotein (HDL) cholesterol, smoking status, alcohol consumption, prevalent CHD, a history of diabetes mellitus and physical activity. *P value for interaction; cut-offs for age, body mass index, systolic blood pressure, total cholesterol and HDL-cholesterol are based on median values. CI: confidence interval.
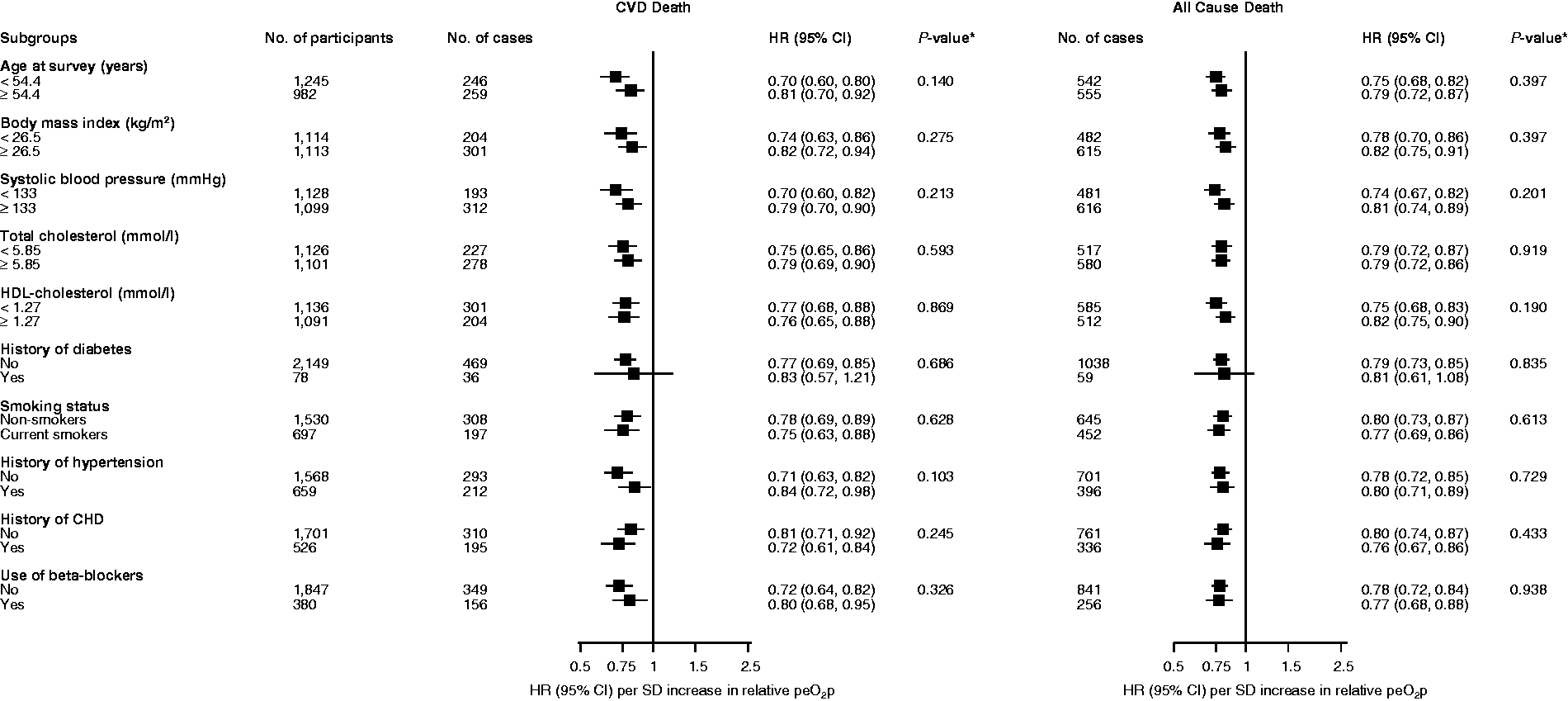
Hazard ratios (HRs) per one standard deviation (SD) change (4.1 mL per beat/kg/102) in relative peak exercise oxygen pulse (peO2p) for cardiovascular and all-cause mortality by several participant characteristics. HRs were adjusted for age, systolic blood pressure, total cholesterol, high-density lipoprotein (HDL) cholesterol, smoking status, alcohol consumption, prevalent coronary heart disease (CHD), a history of diabetes mellitus and physical activity. *P value for interaction; cut-offs for age, body mass index, systolic blood pressure, total cholesterol and HDL-cholesterol are based on median values. CI: confidence interval; CVD: cardiovascular disease.
Relative peO2p and CVD mortality risk prediction
A CVD mortality risk prediction model containing established risk factors yielded a C-index of 0.7009 (95% CI 0.6784–0.7234). After the addition of information on relative peO2p, the C-index changed to 0.7121 (95% CI 0.6899–0.7344), representing a significant increase of 0.0112 (95% CI 0.0011–0.0214; P = 0.030). However, there was no improvement in the classification of participants into predicted 10-year CVD mortality risk categories (NRI 4.18%, –3.24 to 11.61%; P = 0.269).
In an approach to compare the predictive ability of relative peO2p with peak VO2, which has been consistently shown to improve CVD risk prediction above that of traditional cardiovascular risk factors,3,8,28 peak VO2 measurements was added to the CVD mortality prognostic model. There was a C-index change of 0.0348 (95% CI 0.0199–0.0497; P < 0.001) and it yielded a NRI of 16.40% (8.21 to 24.59%; P < 0.001) for the predicted 10-year CVD mortality risk categories.
Furthermore, in a prediction model containing established risk factors plus peak VO2, the C-index change was 0.0028 (95% CI –0.0011–0.0068; P = 0.161), on the addition of information on relative peO2p and NRI it was 1.15% (–3.17 to 5.48%; P = 0.601).
Discussion
In this population-based prospective cohort study of apparently healthy Finnish men with a median follow-up period of over 25 years, we found approximately significant, linear and inverse associations of relative peO2p with distinct fatal cardiovascular and all-cause mortality outcomes. The associations were independent of several established and emerging cardiovascular risk factors. The magnitude and directions of the associations were generally consistent across several clinically relevant subgroups including the use of beta-blockers (yes vs. no), except by the possible effect modification by a history of CHD on the relative peO2p and SCD association. The stronger inverse association between relative peO2p and SCD risk in men with a prevalent history of CHD may corroborate existing evidence that exercise training has more beneficial effects on adverse outcomes in individuals with pre-existing cardiometabolic disease. 29 Furthermore, findings from the assessments of improvements in risk discrimination indicate that relative peO2p provides a significant improvement in CVD mortality risk prediction but not beyond that provided by established cardiovascular risk factors and peak VO2. Further analyses showed that the improvement provided by peak VO2 assessment in the prediction of CVD mortality risk was better than that of relative peO2p, which further confirms the superiority of peak VO2 as a prognostic tool.
The concept of oxygen pulse is more than 100 years old. 30 Notwithstanding this, studies on the associations of peO2p with cardiovascular and mortality outcomes are limited and have been based on populations with smaller sample sizes or with pre-existing disease, and have rarely taken into account the body weight, that is, the relative peO2p. In a French study that compared the long-term prognostic value of peO2p and peak VO2 in 178 patients with chronic heart failure, peO2p was found to have a lower prognostic value for survival compared with peak VO2. 12 However, in a larger sample of 998 heart failure patients, 31 the age-predicted peO2p (an indirect way to adjust peO2p per body weight) has complemented peak O2 in the prediction of risk for mortality, while Lavie et al. 32 studied 209 patients with mild to moderate heart failure and found that peO2p/lean body mass outperforms peak oxygen. These apparently contradictory findings may be explained by different ways to analyse peO2p data, either as an absolute value or in the same way related to body weight or lean body mass. Our data have shown that relative peO2p is independently associated with several long-term cause-specific cardiovascular mortality outcomes as well as all-cause mortality in a general middle-aged population. In addition, we showed that relative peO2p provided prognostic value for CVD mortality beyond established risk factors, although there was no significant improvement beyond that of peak VO2. Considering that these two CPX variables are mathematically related and that both improve with exercise training, 33 these relatively similar results are not surprising. Indeed, whether relative peO2p or peak VO2 will be a better prognostic indicator may vary according to the characteristics of the subjects being studied and the outcomes that are being examined.34,35 Considering the ease of determining relative peO2p from expired gas analysis, it seems quite logical to include this result in CPX reports.
There is growing evidence on the clinical usefulness of CPX variables, as supported by several guidelines.36,37 Notwithstanding, the incorporation of these CPX variables in clinical practice is still limited. Currently, peak VO2, VO2 at ventilatory/anaerobic threshold and ventilatory efficiency (i.e. the minute ventilation/carbon dioxide production relationship) are the only three CPX variables that have been consistently proved to show prognostic significance. 38 peO2p is gaining attention as a clinically useful variable and can easily be obtained during CPX and computed as the ratio of maximum values of VO2 and heart rate. In addition, the interpretation of exercise oxygen pulse curves could also be clinically relevant, as abnormal and flat oxygen pulse curves during CPX have been shown to reflect left ventricular dysfunction 39 and myocardial ischaemia40,41 or fibrosis. 42 The prognostic utility of the peO2p curves deserves further study.
Strengths and limitations
We have reported the first prospective evaluation of the associations of relative peO2p, that is, peO2p/body weight, with the risk of major fatal cardiovascular events and all-cause mortality outcomes in a general population setting. The KIHD cohort was characterised by a high participation rate, and no losses to follow-up were recorded, which minimised potential selection bias. In addition, outcomes were confirmed and validated.5,8 We have utilised comprehensive analysis, which included adjustment for several lifestyle and biological markers, assessment of the dose–response relationships, subgroup analyses and risk prediction analyses. Oxygen pulse is an indicator of stroke volume response to exercise that might be influenced by body dimensions and heart size, 43 and adjustments for body size and/or weight should ideally be included in studies on peO2p, especially if data from male and female subjects are to be compared in different populations. The lack of control for confounding variables such as body weight might have limited the interpretation of previous reports.10,41 In our analyses, we used a relative peO2p which took into account body weight, thus strengthening the validity of the results.
When interpreting the results, some limitations should be considered. The KIHD study included middle-aged Caucasian men from eastern Finland, so extrapolation to other populations and age groups, and particularly for women, might not be valid and more research is needed in this regard. Although we adjusted for a comprehensive panel of covariates, residual confounding remains a potential alternative explanation for our findings, due to the observational design of the study. According to the Fick equation, oxygen pulse equals the product of stroke volume and arteriovenous oxygen difference, while oxygen pulse tends to exhibit a quasi-linear increase throughout maximal exercise. 11 We have previously shown that left ventricular diastolic and systolic diameter are directly associated with peO2p. 10 Even though direct measurements of stroke volume were not available in the current study, there is convincing evidence that oxygen pulse correlates well with direct measurements of stroke volume during submaximal and maximal exercise in healthy and unhealthy subjects of different age groups.39,43–45
In conclusion, the findings of this large prospective cohort study in middle-aged Finnish men with long-term follow-up indicate strong linear and inverse associations of relative peO2p with fatal cardiovascular and all-cause mortality events. In addition, the incorporation of relative peO2p during a maximal cycling CPX provides a significant improvement in CVD mortality risk assessment beyond several conventional risk factors.
Supplemental Material
Supplemental material for Relative peak exercise oxygen pulse is related to sudden cardiac death, cardiovascular and all-cause mortality in middle-aged men
Supplemental material for Relative peak exercise oxygen pulse is related to sudden cardiac death, cardiovascular and all-cause mortality in middle-aged men by Jari A Laukkanen, Claudio Gil S Araú jo, Sudhir Kurl, Hassan Khan, Sae Y Jae, Marco Guazzi and Setor K Kunutsor in European Journal of Preventive Cardiology
Footnotes
Author contribution
JAL, CGA and SKK contributed to the conception or design of the work. JAL, CGA, SK and SKK contributed to the acquisition, analysis, or interpretation of data for the work. JAL and SK drafted the manuscript. JAL, CGA, SK, HK, SYJ, MG and SKK critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Acknowledgements
The authors thank the staff of the Kuopio Research Institute of Exercise Medicine and the Research Institute of Public Health and University of Eastern Finland, Kuopio, Finland for the data collection in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this work was supported by the Finnish Foundation for Cardiovascular Research, Helsinki, Finland.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.