
Abstract
Aims
Patient-reported quality of life and anxiety/depression scores provide important prognostic information independently of traditional clinical data. The aims of this study were to describe: (a) mortality and cardiac events one year after hospital discharge across cardiac diagnoses; (b) patient-reported outcomes at hospital discharge as a predictor of mortality and cardiac events.
Design
A cross-sectional survey with register follow-up.
Methods
Participants: All patients discharged from April 2013 to April 2014 from five national heart centres in Denmark.
Main outcomes
Patient-reported outcomes: anxiety and depression (Hospital Anxiety and Depression Scale); perceived health (Short Form-12); quality of life (HeartQoL and EQ-5D); symptom burden (Edmonton Symptom Assessment Scale). Register data: mortality and cardiac events within one year following discharge.
Results
There were 471 deaths among the 16,689 respondents in the first year after discharge. Across diagnostic groups, patients reporting symptoms of anxiety had a two-fold greater mortality risk when adjusted for age, sex, marital status, educational level, comorbidity, smoking, body mass index and alcohol intake (hazard ratio (HR) 1.92, 95% confidence interval (CI) 1.52–2.42). Similar increased mortality risks were found for patients reporting symptoms of depression (HR 2.29, 95% CI 1.81–2.90), poor quality of life (HR 0.46, 95% CI 0.39–0.54) and severe symptom distress (HR 2.47, 95% CI 1.92–3.19). Cardiac events were predicted by poor quality of life (HR 0.71, 95% CI 0.65–0.77) and severe symptom distress (HR 1.58, 95% CI 1.35–1.85).
Conclusions
Patient-reported mental and physical health outcomes are independent predictors of one-year mortality and cardiac events across cardiac diagnoses.
Keywords
Introduction
Background
Heart disease influences patients’ perception of health and quality of life. 1 Studies suggest that patient-reported outcomes (PROs) can predict future quality of life, morbidity and mortality in cardiac patients;2,3 however, not all cardiac diagnoses have been covered in the research. Patient-reported quality of life and anxiety/depression scores provide important prognostic information independently of traditional clinical data, as better outcome scores have been associated with longer survival in patients with ventricular arrhythmias and coronary artery disease.4,5 The connection between patient-reported physical health and mortality and morbidity has been established and it is important to note that PROs may be better predictors of outcomes than healthcare staff’s assessments or clinical measures. 6 The association between patient-reported mental outcomes and mortality and morbidity may be explained by both physiological and behavioural processes. Psychological factors stimulate the autonomic nervous system, which triggers the production of catecholamine, increases blood pressure, constricts coronary arteries and increases platelet activity. Consequently, patients suffer increased thrombogenesis, arrhythmogenesis, reduced heart rate variability, myocardial ischaemia and impaired ventricular function. 7 Behavioural mechanisms are another link between mental distress and cardiac disease. Individuals with anxiety have a more unhealthy food intake, smoke more, consume more drugs and/or alcohol, adhere less to treatment, sleep poorly and are less physically active. 8 These elements are risk factors associated with the progression of cardiac disease. 9 PROs may facilitate disease surveillance and quantify populations’ health; however, additional research is needed to understand better the predictive value of PROs on mortality and cardiac events in cardiology.
Objectives
The objectives of this paper were to describe across cardiac diagnostic groups: (a) mortality and cardiac events one year after hospital discharge; (b) PROs at hospital discharge as a predictor of mortality and cardiac events. (In this paper PROs refers to patients’ self-reported symptoms of anxiety, symptoms of depression, perceived health, quality of life and symptom burden.)
Methods
Study design
The DenHeart study is a cross-sectional survey combined with follow-up data from national registers. All patients hospitalised at a heart centre were asked to fill out a questionnaire at hospital discharge to evaluate PROs across cardiac diagnostic groups. The methods have been thoroughly described in the published study protocol. 10
Setting and participants
Over one year (15 April 2013 to 15 April 2014) all patients discharged or transferred from the five Danish heart centres were included in the study.
Eligibility criteria
All patients were unselected and consecutively included. Patients under 18 years of age, patients without a Danish civil registration number and patients who did not understand Danish were excluded from the study. For ethical reasons, patients who were unconscious when transferred were also excluded.
Recruitment
Patients were asked to complete and return a questionnaire before they left the hospital or to do so at home within three days of discharge and return it by mail.
Patients were recruited by a ward nurse or by a research assistant nurse. The questionnaire was distributed with a postage prepaid envelope for the return of the questionnaire.
Ethics approval
The study complies with the Declaration of Helsinki. According to Danish legislation, surveys are not approved by an ethics committee system (H-4-2013-FSP) but rather by the Danish Data Protection Agency (2007-58-0015/30-0937). Use of register data was permitted by the Danish National Board of Health (FSEID-0001131). DenHeart is registered at ClinicalTrials.gov (NCT01926145) and approved by the institutional boards of the heart centres. Patients signed an informed consent. All authors had full access to all of the data in the study.
Variables
The DenHeart questionnaire consisted of five validated questionnaires and a number of ancillary questions, a total of 80 questions:
The short form-12 (SF-12), a brief measure of overall health status that generates a physical and a mental component score ranging from 0 to 100, with higher scores indicating better health status; 11 the hospital anxiety and depression scale (HADS), a 14-item questionnaire that assesses levels of anxiety and depression in medically ill patients, HADS-anxiety (HADS-A) and HADS-depression (HADS-D), scores of 8–10 suggest the presence of a mood disorder, scores of 11 or greater indicate the probable presence of a mood disorder; 12 EQ-5D, a standardised instrument for use as a measure of current health status that provides a simple descriptive profile and a single index value that can be used in the clinical and economic evaluation of healthcare and in population health surveys, higher scores indicate better health status; 13 HeartQoL, a disease-specific questionnaire that measures quality of life in cardiac patients and produces a global score and two subscales, a physical scale and an emotional scale ranging from 0 to 3, with higher scores indicating better quality of life status;14–16 and the Edmonton symptom assessment scale (ESAS), a 10-item questionnaire that allows patients to rate their symptoms on a visual numerical scale, higher scores indicate the presence and intensity of the symptoms, 17 a total score of 25 or above indicates moderate distress, scores of 33 or above indicate severe distress. 18 The survey also included nine questions about health and health behaviour from the Danish National Health Survey.19,20
Data from the following Danish national registers were collected on all identified patients at baseline: the Danish Civil Registration System, 21 the Danish National Patient Register, 22 Danish education registers 23 and Danish registers on personal income and transfer payments. 24
To combine questionnaire data with data from the registers all questionnaires were matched with a hospital discharge from the National Patient Register. Patients without a relevant cardiac diagnosis or cardiac observation diagnosis were not counted among possible respondents.
Respondents were divided into seven diagnostic groups based on their primary International Classification of Disease, version 10, action diagnosis obtained from the Danish National Patient Register. The diagnostic groups were defined as presented in Supplementary File 1.
Information on comorbidity was obtained for all patients from the National Patient Register going back 10 years, not including the index discharge. Both primary and secondary diagnoses were included. We calculated the Tu comorbidity index 25 utilising information on primary and secondary diagnoses from all in and outpatient contacts 10 years back. The following diseases are included in the Tu score: congestive heart failure; cardiogenic shock; arrhythmia; pulmonary oedema; malignancy; diabetes; cerebrovascular disease; acute/chronic renal failure; chronic obstructive pulmonary disease. All diagnoses are weighted equal.
Follow-up data were collected from the Danish Civil Registration System and the Danish National Patient Register.
Cardiac events were defined as presented in Supplementary File 1.
Study size
The study consisted of the total population of patients discharged from the five heart centres during one year in order to secure as high a level of specificity as possible. Patients admitted with lung disease and other non-cardiac diseases were excluded.
Statistical methods
The incidence rates of mortality and cardiac events, respectively, were calculated per 1000 person-years.
A total of 23 respondents was lost to follow-up in the registers as they did not have an address in Denmark. These were excluded from the analyses.
The associations between the PROs and the risk of one-year all-cause mortality within one year of hospital discharge were assessed using Cox proportional hazards models. Furthermore, the associations between the PROs and risk of a (non-fatal) cardiac event within one year of hospital discharge were also assessed using Cox proportional hazards models. Follow-up was continued until the first relevant event (death or a cardiac event), emigration or end of follow-up. In the analyses, age was used as the underlying time scale, thus treating age at discharge as the time of delayed entry. All analyses were adjusted for sex, marital status, educational level, Tu co-morbidity score, smoking, body mass index and alcohol intake. The proportional hazards assumption was checked graphically. Results are reported as hazard ratios (HRs) with 95% confidence intervals (CIs). As missing data were more frequent for the SF-12 outcomes than the other PROs, the following diagnostic groups were pooled with the combined group when analysing the SF-12 outcomes: patients with heart valve disease and patients under observation for heart disease.
Results
Participants
A total of 34,564 patients were discharged from the heart centres during the study period. Most, 33,060, were eligible and 16,712 patients completed the questionnaire, and one-year register follow-up was possible for 16,689 patients, Figure 1. The response rate was 51%.
Flow chart.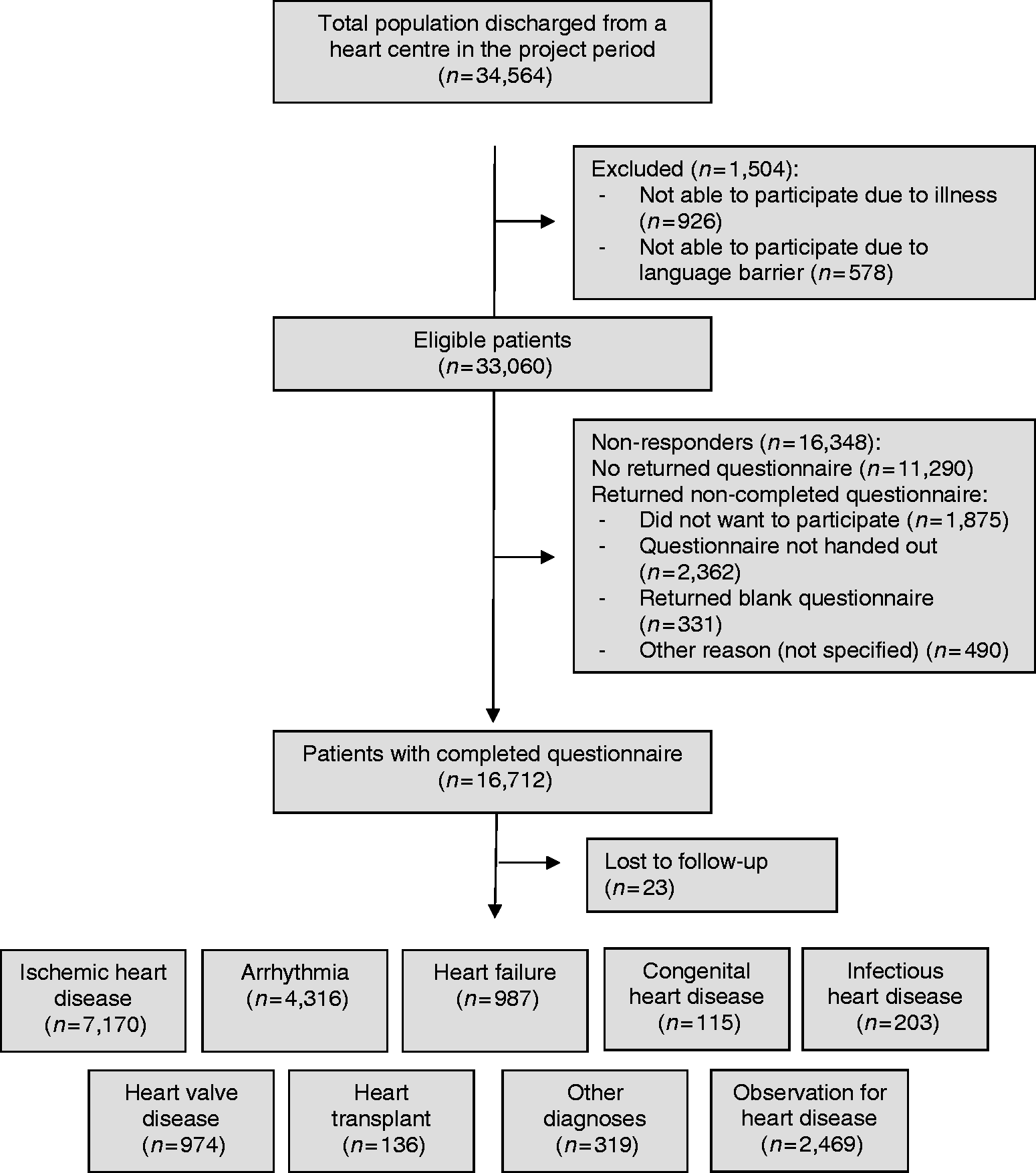
Demographic profile
Demographic and clinical data for all patients treated, responders and according to diagnostic group.
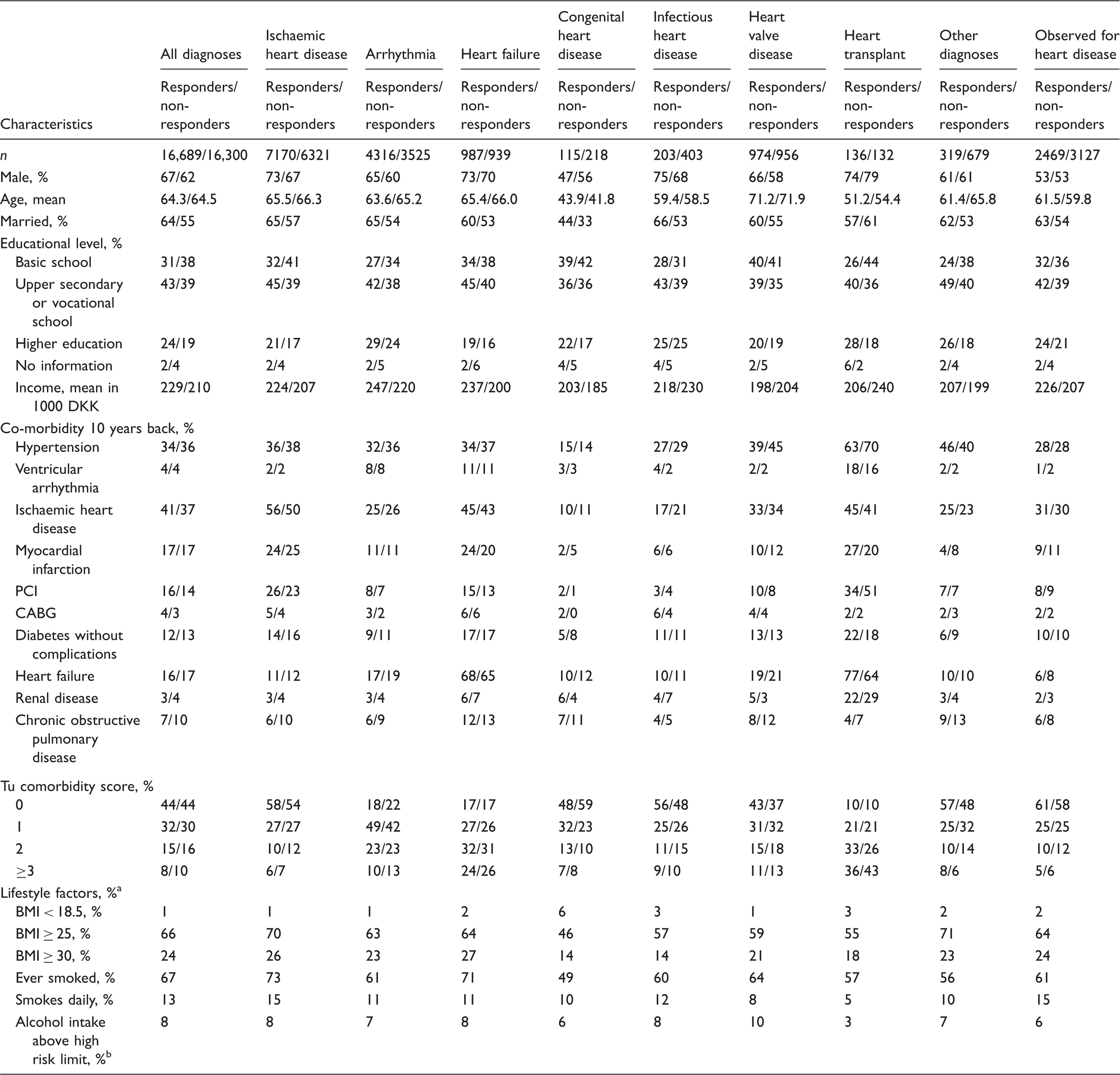
SE: standard error; PCI: percutaneous coronary intervention; CABG: coronary artery bypass grafting; BMI: body mass index.
Information about BMI, smoking and alcohol consumption was included in the DenHeart questionnaire. Therefore, these parameters are only presented for the responders.
The Danish National Board of Health defines the high-risk limit for alcohol consumption as a weekly intake of more than 21 standard drinks for men and more than 14 standard drinks for women.
Mortality and cardiac events
Mortality and cardiac events one year after hospital discharge.
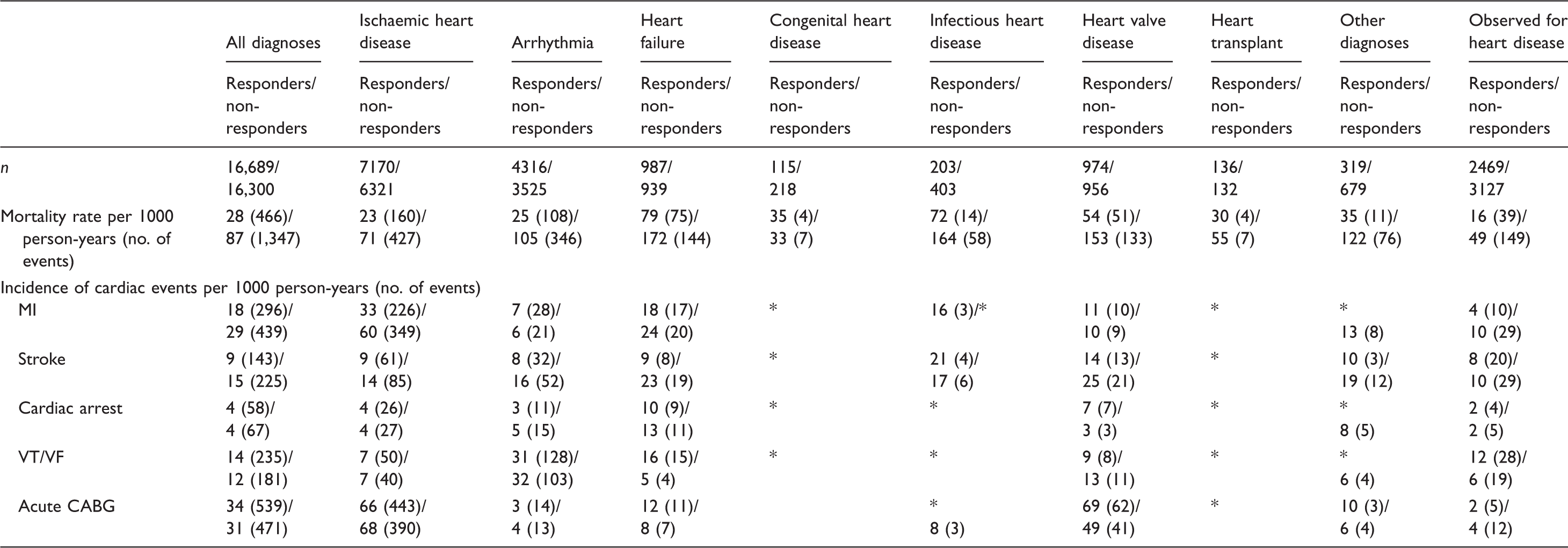
CABG: coronary artery bypass grafting; MI: myocardial infarction; VF: ventricular fibrillation; VT: ventricular tachycardia.
Fewer than three cases.
Predictors of mortality
Anxiety measured by HADS seemed to be a strong predictor of mortality across diagnostic groups (Figure 2), as patients with a HADS-A score of 8 or greater had almost double the mortality risk (HR 1.92, 95% CI 1.52–2.42) of patients with a HADS-A score less than 8, Table 3. Depression measured by HADS was also a strong predictor of mortality. Patients with a HADS-D score of 8 or greater had a HR of 2.29 (95% CI 1.81–2.90) compared to patients with a HADS-D score less than 8. The estimates varied across the diagnostic groups, Table 3. For the physical component scale SF-12 the estimates indicate that as patients’ self-reported health increased by one point on the scale their mortality risk decreased by 5% (HR 0.95, 95% CI 0.94–0.96). Similarly, a one point increase on the mental component scale meant a 3% decrease in mortality risk (HR 0.97, 95% CI 0.95–0.98), Table 3. In the three groups, heart valve disease, combined group and observation for heart disease there were not enough events to comply with the statistical model. However, when combining the groups, the estimate for the physical component scale was HR of 0.95 (95% CI 0.92–0.97) and for the mental component scale HR of 0.97 (95% CI 0.95–0.99) indicating a similar association between scores and mortality across the three groups.
Patient-reported health outcomes as predictors of mortality and cardiac events including all cardiac diagnoses in the DenHeart study. Predictors of mortality one year after hospital discharge. HADS-A: hospital anxiety and depression scale – anxiety; HADS-D: hospital anxiety and depression scale – depression; HR: hazard ratio; CI: 95% confidence interval; MCS: mental component scale; PCS: physical component scale. This group consists of patients with congenital heart disease, infectious heart disease, heart transplant and other small diagnostic groups. Cox regression adjusted for age, sex, marital status, educational level, TU co-morbidity score, smoking, body mass index and alcohol intake. Significance level set at 0.05. In the diagnostic groups marked NA there were not enough deaths to conduct the statistical analyses.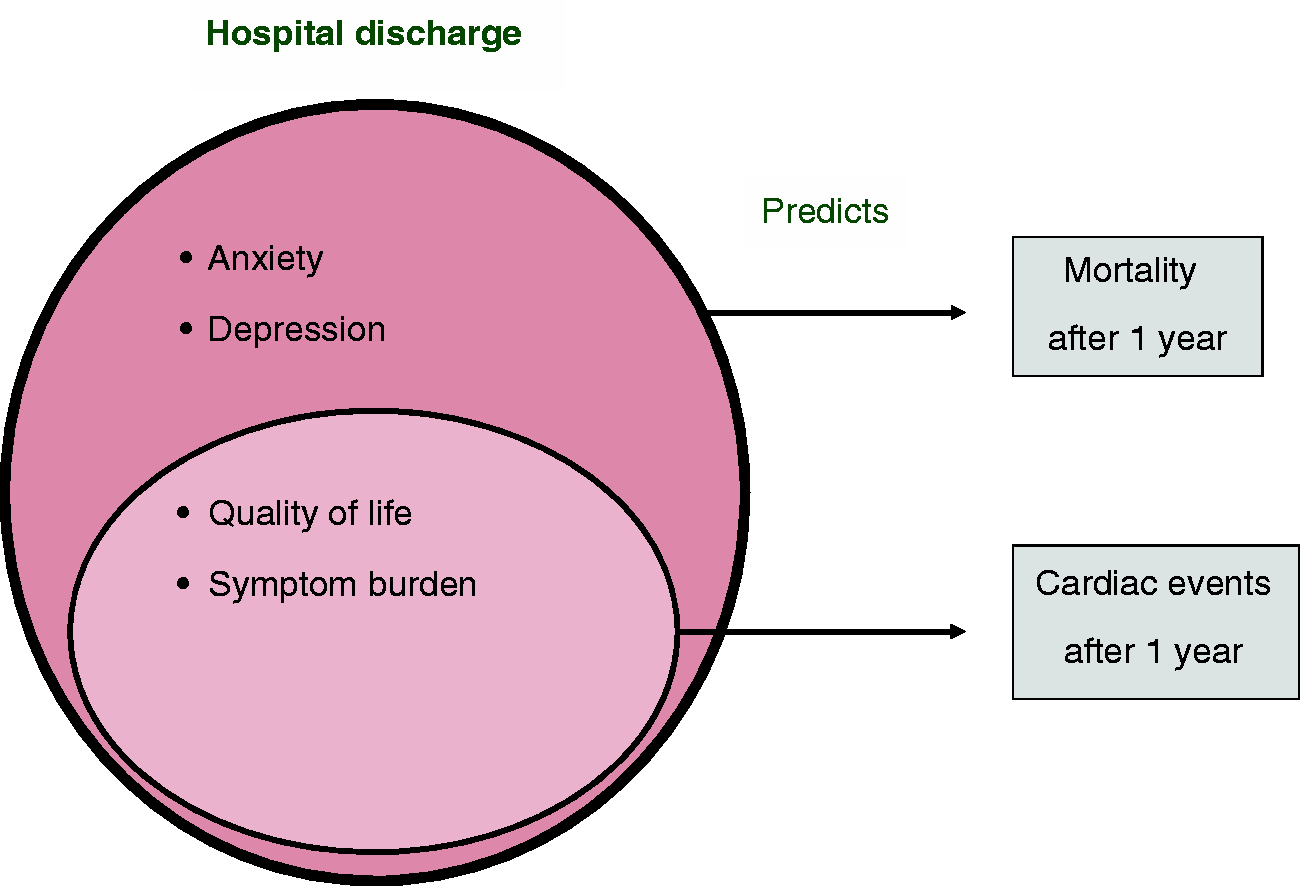
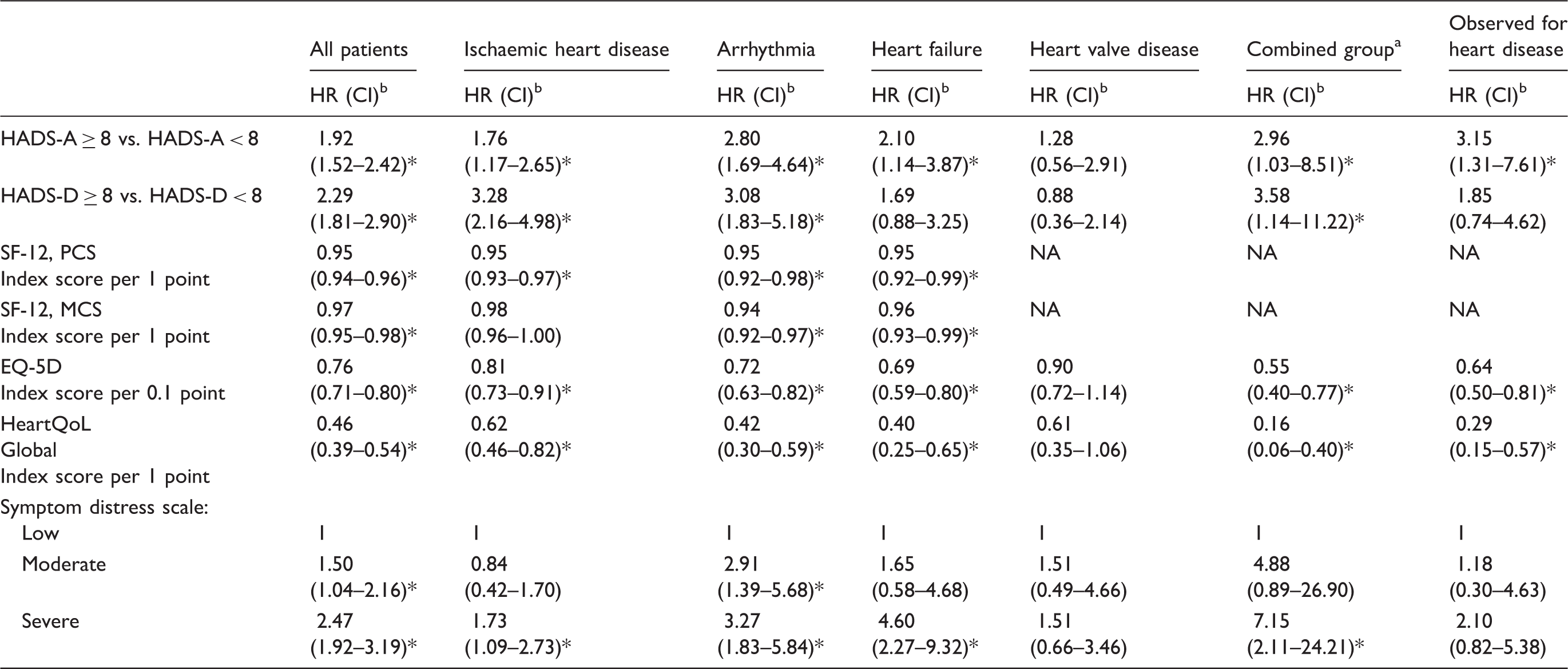
Regarding health-related quality of life measured by EQ-5D, an increase of 0.1 on the scale meant a 24% decrease in mortality risk (HR 0.76, 95% CI 0.71–0.80). Estimates for all diagnostic groups are presented in Table 3. Similarly, disease-specific quality of life measured by the HeartQoL showed a 54% decrease in mortality risk with a one point increase on the scale, Table 3.
Furthermore, the mortality risk seemed to increase with increasing severity of symptoms across the diagnostic groups. Patients with severe symptom distress had almost 2.5 times the mortality risk of patients with low symptom distress (HR 2.47, 95% CI 1.92–3.19), Table 3.
There is almost no difference between the unadjusted and adjusted estimates (Supplementary File 2) indicating that the associations between PROs and mortality cannot be explained by age, sex, marital status, educational level, comorbidity, smoking, BMI and alcohol intake.
Predictors of cardiac events
Both anxiety HADS-A and depression HADS-D seemed to predict cardiac events (MI, stroke, cardiac arrest, VT/VF, acute CABG) (Figure 2) as patients with symptoms of anxiety had a 16% increase in the risk of cardiac events (HR 1.16, 95% CI 1.01–1.34) and patients with symptoms of depression had a 20% increased risk (HR 1.20, 95% CI 1.02–1.42) (Table 4).
Predictors of cardiac events a one year after hospital discharge.
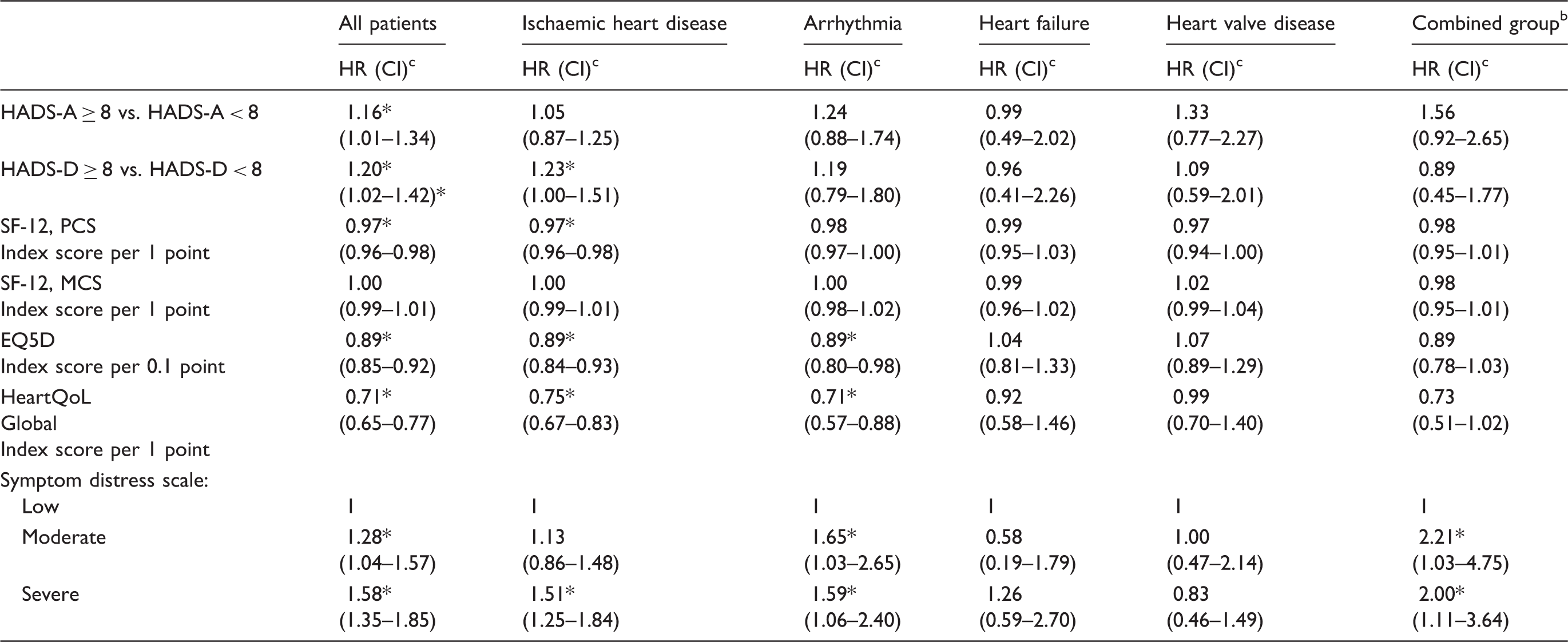
HADS-A: hospital anxiety and depression scale – anxiety; HADS-D: hospital anxiety and depression scale – depression; HR: hazard ratio; CI: 95% confidence interval; MCS: mental component scale; PCS: physical component scale.
Cardiac events are defined as: myocardial infarction, stroke, cardiac arrest, ventricular tachycardia/ventricular fibrillation and acute coronary artery bypass grafting.
This group consists of patients with congenital heart disease, infectious heart disease, heart transplant, observation for heart disease and other small diagnostic groups.
Cox regression adjusted for age, sex, marital status, educational level, TU co-morbidity score, smoking, body mass index and alcohol intake.
Significance level set at 0.05.
Furthermore, health-related quality of life measured by EQ-5D predicted cardiac events. A 0.1 point increase in the score meant an 11% decrease in the cardiac event risk (HR 0.89, 95% CI 0.85–0.92), Table 4.
Disease-specific quality of life measured by the HeartQoL questionnaire showed a 29% decrease in cardiac event risk, with a one point increase on the score (HR 0.71, 95% CI 0.65–0.77), Table 4.
Symptom distress also predicted cardiac events, as patients with moderate symptom distress had a 28% greater risk of cardiac events compared to patients with low symptom distress (HR 1.28, (95% CI 1.04–1.57). Similarly, patients with severe symptom distress had an almost 60% greater risk of cardiac events compared to patients with low symptom distress (HR 1.58, 95% CI 1.35–1.85), Table 4.
The above results applied for the combined analyses of all diagnostic groups. Looking at the diagnostic groups separately, the same tendency was found, however, few were significant.
Discussion
This study found that patient-reported anxiety, depression, quality of life and symptom burden were predictors of mortality, and quality of life and symptom burden were predictors of cardiac events across cardiac diagnostic groups.
Strengths and weaknesses
Patients who were too ill or did not speak or understand Danish were excluded. As the most seriously ill patients were not able to participate in the survey the responding patients may not be completely representative of the total target population. The proportions of patients in each diagnostic group are similar among responders and the total population. Furthermore, responders and non-responders have similar demographic and clinical characteristics. 1
Study population
The five heart centres treat the most critically ill cardiac patients in Denmark. The chronic and terminally ill cardiac patients were underrepresented in the DenHeart study.
Variables
The majority of the outcome measures included in the questionnaire were validated and standardised instruments used to assess PROs, which enhances the validity of results. However, in the interpretation of the results, it must be taken into account that patients with different cardiac conditions also differ regarding how much their health status and/or health behaviour had changed prior to admission to hospital, and that some of the instruments have long recall, up to four weeks.
Confounding factors
Self-reported outcomes are by nature not objective, and therefore sources of bias may exist. Social desirability bias can be an issue, as respondents answer according to what they believe is socially acceptable.26,27 The National Patient Register is known internationally to be the most comprehensive of its kind and is a very important register for biomedical and public health research. 22
Non-response
Age and socioeconomic position play a significant role for non-response. Also, regional differences of about 15% in response rates have been documented.20,28 The patients treated at the heart centres are often old and severely ill, which may be reflected in the response rate of 51%.
Even though the responders and the non-responders were similar regarding demographic data, a much higher mortality rate was found among non-responders. It is natural that the most severely ill would be overrepresented among non-responders.
Outcomes
The study population is large and attempts to include all patients. Power is sufficient for the total population; however, some of the diagnostic groups were too small and did not have enough events to conduct statistical analyses. The congenital heart disease, infectious heart disease, heart transplant and other small diagnostic groups were gathered together in a new combined group used in the regression analyses.
Interpretation and implications
The study had three key findings. First, PRO scores indicating anxiety, depression, poor quality of life and moderate/severe symptom burden are all independent predictors of mortality, and poor quality of life and moderate/severe symptom burden are also predictors of cardiac events. The second interesting point is that there is very little difference in the predictive value of PROs between diagnostic groups, indicating that this phenomenon could be considered a clinical marker for all cardiac patients. The third key finding is that the unadjusted and adjusted values are almost identical, strengthening the reliability of the associations being real and not just reflections of other known risk factors or morbidity.
Anxiety and depression measured by HADS has previously been linked to mortality in selected cardiac diagnostic groups, e.g. patients undergoing CABG surgery, 29 coronary syndrome and stable angina pectoris.30–33 In heart failure an association with mortality was previously found for depression, 34 which stands in contrast to our study in which anxiety but not depression was associated with mortality in heart failure. In patients with MI depressive symptoms were found to be independent prognostic risk factors for mortality; however, as in our study not for cardiac events. 35 In contrast, an association between anxiety and cardiac events after five-year follow-up was found in patients with MI. 36 Symptoms of anxiety and depression have also been found to be the single biggest driver of healthcare costs three years after index admission in patients with coronary heart disease, 37 indicating an association with comorbidity or potentially preventable hospital admissions caused by mental distress, which could explain why no association with cardiac events was found in our study.
Also, perceived health measured by SF-36 as a predictor of mortality has previously been investigated in selected cardiac groups. An association between PCS, but not MCS, and mortality was found in patients with coronary artery disease 38 and in persons being evaluated for primary cardiac prevention. 39 In our study, we found associations with mortality in both the physical and mental domain; however, not for all diagnostic groups.
For quality of life measured by HeartQoL our findings are confirmed by one study investigating patients with ischaemic heart disease in an outpatient setting, in which a significant linear relationship was found to five-year mortality. 40
The ESAS scale was originally developed for palliative care, but the use is extended to several diagnostic groups. We found symptom distress to be a strong predictor of mortality in several groups. No previous studies investigated this in cardiology; however, the association with mortality was also found in patients with cancer. 41
Our study adds to the body of evidence by including all cardiac diagnostic groups in one study design; PRO at hospital discharge – and mortality and cardiac events at one-year follow-up. The previous studies are smaller with varying adjustments, data collection time points and follow-up time in many selected populations.
The PROs used in this study cover different clinical outcomes. Some, SF-12, EQ-5D, HeartQoL and ESAS reflect physical health, and the connection between perceived physical health and mortality and morbidity may not be surprising. However, it should be noted as a potentially useful screening tool, integrating PROs into individualised medical care in clinical practice. The most noticeable finding is that the mental factors, anxiety and depression are strong independent predictors of mortality across several diagnoses. This adds significant evidence to the autonomic stress–response theory as a likely explanation for the association. 7 Mental factors have proved to be as important as or more important than traditional risk factors such as blood pressure, diabetes, exercise and cholesterol in cardiac disease development. 9 With the present results, the connection to survival and cardiac events is also established across cardiac diagnoses and adds to previous research linking patient-reported psychological outcomes to mortality.
Generalisability
This national study was carried out in Denmark where international guidelines for treatment are followed. The response rate was 51%, which is not unexpected in a population of severely ill patients; however, this may cause concerns regarding representativeness.
Conclusion
Among the 16,689 responders the one-year mortality rate was 28 per 1000 person-years (total of 466). The incidence among responders per 1000 person-years of stroke was nine, cardiac arrest four, VT/VF 14 and acute CABG 34. The incident rate among non-responders was generally higher. Patient-reported anxiety, depression, quality of life and symptom burden were predictors of mortality, and quality of life and symptom burden were predictors of cardiac events across cardiac diagnostic groups.
Author contribution
SKB conceived the idea for the study. All designed the study. KJ, OE and AVC performed the statistical analyses. SKB and AVC wrote the first draft of the manuscript. All revised the manuscript critically. All have given their final approval of the version to be published.
Supplemental Material
Supplemental material for Patient-reported outcomes are independent predictors of one-year mortality and cardiac events across cardiac diagnoses: Findings from the national DenHeart survey
Supplemental material for Patient-reported outcomes are independent predictors of one-year mortality and cardiac events across cardiac diagnoses: Findings from the national DenHeart survey by Selina K Berg, Charlotte B Thorup, Britt Borregaard, Anne V Christensen, Lars Thrysoee, Trine B Rasmussen, Ola Ekholm, Knud Juel and Marianne Vamosi in European Journal of Preventive Cardiology
Footnotes
Acknowledgements
The authors would like to express their gratitude to the patients who took the time to participate in the survey, and also to the 800 cardiac nurses involved in the data collection and the heart centres for prioritising this study in a busy clinic. Furthermore, the authors would like to acknowledge the DenHeart research expert committee.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.