
Abstract
Background
There is increasing evidence of an association between social relationships and morbidity in general, and cardiovascular disease in particular. However, recent syntheses of the evidence raise two important questions: is it the perceived quality or the more objective quantity of relationships that matters most; and what are the implications of changes in relationships over time? In this study, we investigate the cumulative effects of loneliness and social isolation on incident cardiovascular disease.
Design
A secondary analysis of prospective follow-up data from the English Longitudinal Study of Ageing (ELSA).
Methods
To assess the association between social isolation or loneliness and incident cardiovascular disease, lagged values of exposure to loneliness and isolation were treated as time-varying variables in discrete time survival models controlling for potential confounders and established cardiovascular disease risk factors.
Results
A total of 5397 men and women aged over 50 years were followed up for new fatal and non-fatal diagnoses of heart disease and stroke between 2004 and 2010. Over a mean follow-up period of 5.4 years, 571 new cardiovascular events were recorded. We found that loneliness was associated with an increased risk of cardiovascular disease (odds ratio 1.27, 95% confidence interval 1.01–1.57). Social isolation, meanwhile, was not associated with disease incidence. There was no evidence of a cumulative effect over time of social relationships on cardiovascular disease risk.
Conclusions
Loneliness is associated with an increased risk of developing coronary heart disease and stroke, independently of traditional cardiovascular disease risk factors. Our findings suggest that primary prevention strategies targeting loneliness could help to prevent cardiovascular disease.
Introduction
There is growing evidence that adults who are socially isolated (i.e. who have few social contacts) or who feel lonely (i.e. are unhappy about their social relationships) are at greater risk of cardiovascular disease (CVD). A recent meta-analysis of observational studies found that weaker social relationships were associated with a 29% increase in the risk of incident heart disease and a 32% increase in the risk of stroke. 1 Primary studies have highlighted three pathways through which social relationships can influence CVD risk: behavioural (e.g. smoking, physical inactivity); psychological (e.g. low self-esteem and self-efficacy); and biological (e.g. response to stress, allostatic load and cardiovascular reactivity). 2
Social relationships change over time. Loneliness and social isolation may for example increase following widowhood, migration or a decline in functional capacity. 3 Conversely, changes such as the birth of grandchildren can bring increased contact with children in later life, and research indicates that people continue to acquire new acquaintances and rekindle weakened ties in old age. 4 Analyses that take into account the dynamic and multidimensional nature of social relationships are needed to inform the design of effective interventions. We therefore took advantage of the availability of repeated measures of loneliness and social isolation in a large-scale prospective cohort, the English Longitudinal Study of Ageing (ELSA), 5 to investigate whether they were independently associated with an increased risk of incident CVD.
Methods
Participants
ELSA is a population-based cohort study of adults aged 50 years and over living in England, for which ethical approval was granted by the National Research Ethics Service. It began in 2002, with a sample of 11,391 individuals who in 1998, 1999 or 2000 took part in the Health Survey for England (HSE), an annual cross-sectional survey designed to monitor the population's general health.
6
For the HSE, participants were selected using a multistage stratified probability sampling design. First, UK postcode sectors stratified by health authority and the proportion of households in non-manual socioeconomic groups were selected with probability proportional to their size. In a second stage, a fixed number of addresses was identified systematically from each postcode sector and households were selected for each address.
7
A total of 31,051 households were sampled, of which 11,578 were eligible for ELSA (see Figure 1 for a summary of the sample definition process).
Sample selection process. *Note that household numbers only were available for these stages.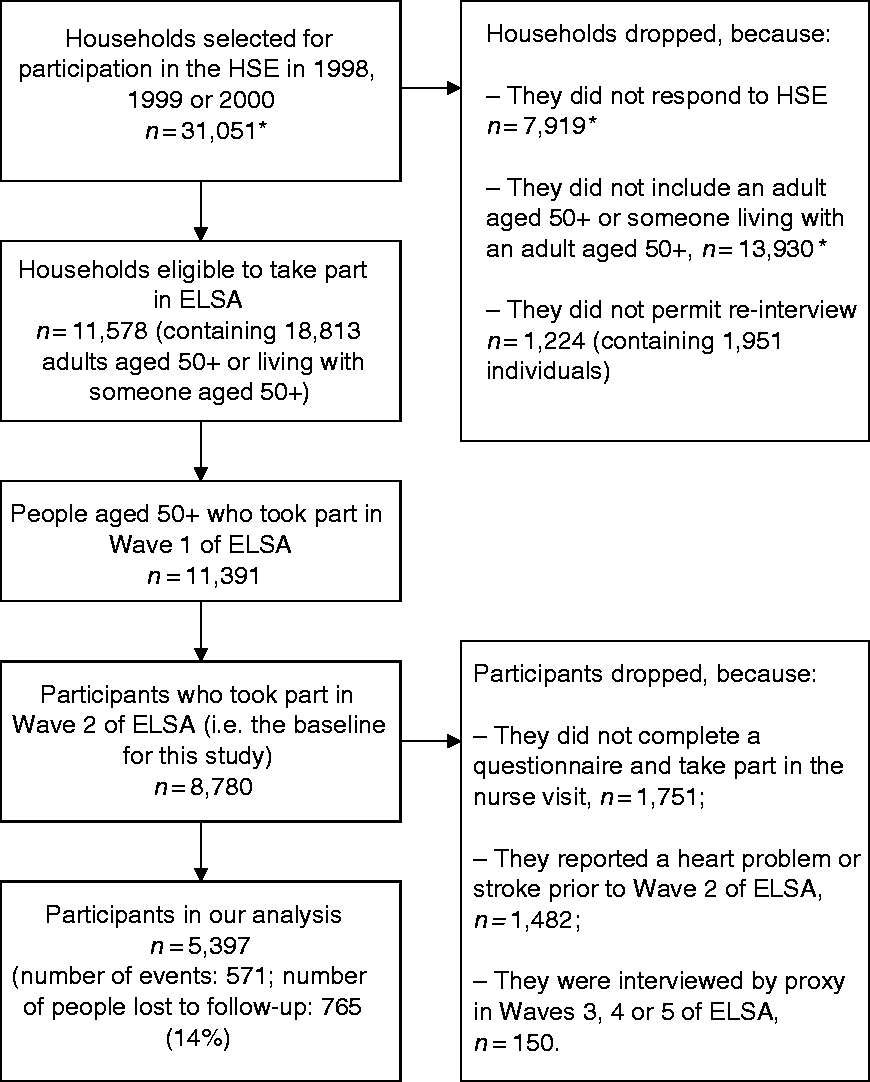
Comparison of the sociodemographic characteristics of the 11,391 people who eventually took part in ELSA's first wave with national census data indicate that this sample was representative of the English population. 5 Thereafter, members were surveyed every 2 years using computer-assisted personal interviews and self-completion questionnaires. Wave 5 was the last wave for which data on both fatal and non-fatal CVD events were available at the time of our analyses. We used wave 2 as the baseline for our study because this was the first wave at which core ELSA participants (i.e. excluding partners aged under 50 years) took part in a nurse visit when biomarkers pertinent to CVD risk – blood pressure and cholesterol – were measured. We excluded: participants diagnosed with a heart condition or stroke prior to wave 2, as we wanted to investigate first events; and individuals interviewed by proxy due to poor health or disability, because proxy questionnaires did not assess loneliness or isolation.
Exposure: loneliness and social isolation
Loneliness
We selected two instruments used in ELSA to capture loneliness feelings in waves 2, 3 and 4 of ELSA: a direct single-item question, in which participants were asked in person whether they agreed or not with the statement ‘Much of the time during the past week, you felt lonely’; 8 and the University of California, Los Angeles (UCLA) three-item loneliness scale, which covers the frequency and intensity of loneliness feelings and was administered by means of a self-completion questionnaire. Its three items are: How often do you feel you lack companionship? How often do you feel left out? How often do you feel isolated from others? For each question, participants could answer ‘hardly ever or never’ (score of 1), ‘some of the time’ (score of 2) or ‘often’ (score of 3). Total scores ranged from 3 to 9, with a higher score indicating greater levels of loneliness. This scale has been validated and shown to be reliable among older adults. 9
Because we were specifically interested in whether the frequency (rather than the intensity) of loneliness was associated with the risk of CVD, we chose the direct single-item question for our main analyses. We coded loneliness to reflect cumulative exposure up until the event or censoring – i.e. reporting feeling frequently lonely at none, one or two waves was coded as 0, 1 and 2. The three-item UCLA scale was used in sensitivity analyses. In line with previous studies, we used a score of 6 as the cut-off to distinguish between more and less lonely participants.10,11
Social isolation
We adapted the index of social isolation developed by Shankar et al., 10 assigning one point for each of the following six items: living alone; less than monthly face-to-face, telephone or written/e-mail contact with children outside the household; less than monthly contact with other relatives outside the household; less than monthly contact with friends; not participating in any organisations, religious groups, or committees; and not currently employed. Our rationale for adapting the Shankar index was that the former does not capture contact with relatives other than partners or spouse living at home, and nor does it tap into the potential network of colleagues one might access when in employment. Scores on our index ranged from 0 to 6, with higher scores indicating greater social isolation. Because we were specifically interested in whether the most isolated individuals were at increased risk of CVD, we dichotomised the index using 5 as the cut-off score (i.e. those scoring 5 or 6 were classed as socially isolated). In our main analyses, we compared those who were classed as isolated in one or more waves (i.e. in waves 2, 3 or 4 of ELSA), with those who were never isolated. In sensitivity analyses, we first checked our findings against those obtained based on the measure developed by Shankar and colleagues; we then used the tool selected by Elovainio et al. for analyses of the UK Biobank dataset. 12
Incident CVD
Fatal CVD events were derived from the UK National Health Service Central Register, using ICD-9 codes 390–459 and ICD-10 codes I00–I99. Non-fatal events were reported by participants, according to whether they had been diagnosed with a heart condition or stroke since their last interview. New heart problem diagnoses included angina, heart attack, congestive heart failure, a heart murmur, an abnormal heart rhythm or any other heart trouble. Studies have found that respondents may be prone to misclassify specific diagnoses of heart conditions and that self-reports have more validity when heart disease is defined more broadly.13,14 Comparisons of estimates from clinically verified studies with self-reported incident stroke in ELSA's sister study, the Health and Retirement Study, suggest that misreporting is non-systematic and that participant-reported events can be used to study stroke incidence and risk factors. 15
Covariates
Items of the Framingham 10-year CVD risk score
To investigate whether loneliness and social isolation predicted CVD independently from the factors traditionally taken into account when assessing disease risk, we included the components of the Framingham score in our analyses. These include age, high-density lipoprotein (HDL) and total cholesterol, systolic blood pressure, treatment for hypertension, smoking and diabetes. 16 At wave 2 of ELSA (the baseline wave for our study), blood samples were taken from participants with written consent who did not have a clotting or bleeding disorder and were not taking anticoagulant drugs. Samples were assayed for total and HDL cholesterol, haemoglobin A1C and for fibrinogen and C-reactive protein at the Royal Victoria Infirmary in Newcastle-upon-Tyne, UK. Systolic blood pressure was measured three times using an Omron blood pressure monitor with the participant seated; the mean of the last two readings was used in our analysis. Participants were asked about their smoking status and whether they were taking any medication for high blood pressure. We defined prevalent diabetes mellitus based on reported doctor-diagnosed diabetes and/or the use of diabetes medication, or a haemoglobin A1C level of 6.5% or greater. 17 Each variable was entered separately into our analytical models; in a sensitivity analysis, we checked whether our results changed when we substituted the individual items with the overall Framingham score predicting 10-year CVD risk, as used in clinical practice.
Total household wealth
In addition to the factors included in the Framingham score, we identified socioeconomic status as a potential confounder.18,19 We used total household wealth quintiles, a robust indicator of socioeconomic circumstances and standard of living in ELSA, which includes financial wealth, the value of any home and other property, the value of business assets, physical wealth such as artwork and jewellery and debt.20,21
Statistical analysis
Associations between social relationship measures and CVD incidence were estimated with odds ratios (ORs) and 95% confidence intervals (CIs) computed in discrete time survival analyses. Discrete time models were chosen because the exact time at which events occurred was unknown, and because such models easily accommodate time-varying variables that have not been measured continuously over time. Multinomial logit models allowed us to model non-CVD death as a competing risk. 22 After running separate models for loneliness and isolation only (models A and B), we adjusted for potential confounders (model C, adjusting for household wealth quintile, age and gender), before adding in the rest of the Framingham score items (model D). All models satisfied the minimum requirement of 10 events per parameter. The proportional hazards assumption was checked by testing whether an interaction term between time and the independent variables was significant. In all models, the values used for loneliness and isolation were lagged values – i.e. the models sought to investigate whether the number of times a person reported feeling lonely or being isolated in the waves prior to CVD event assessment predicted the likelihood of an event. Sensitivity analyses were run to gauge whether results changed when the Framingham score, UCLA loneliness scale, Shankar or Elovainio indices of social isolation were used.
Participants lost to follow-up (n = 765, 14% of the study sample) – i.e. who were not known to have died during the study but who dropped out before it ended) – were treated as censored in our survival analyses. We assessed missing data for all the variables in our models and used multiple imputation by chained equations with 25 replications, under the assumption that values were missing at random.23,24 The imputation model included the event indicator, the Nelson–Aalen estimator, age, gender, total household wealth, HDL cholesterol, total cholesterol, systolic blood pressure, treatment for hypertension, smoking, diabetes, and loneliness and social isolation at each wave. We used Rubin's rules (1987) to pool the imputation estimates. 23
All statistical analyses were conducted using Stata SE 14.2 25 and the significance level used was 5%.
Results
Study population
Of the 18,813 people eligible to take part in the first wave of ELSA, 8780 (47%) completed the main interview in wave 2. Eighty-one per cent (7029) of those who were interviewed in person completed a questionnaire and took part in the nurse visit. After excluding the 1482 people who reported a heart problem or stroke diagnosis prior to wave 2, and the 150 people who went on to be interviewed by proxy, a total of 5397 individuals were eligible for our analyses (see Figure 1 for a summary of the sample selection process).
The percentage of missing values at baseline ranged from none for age and gender to 19% for HDL cholesterol. Taking into account patterns of missingness for the two social relationship variables across the 6-year study period, only 62% of the study cohort would have been available for analysis under the traditional listwise deletion method. The distribution of imputed values closely fitted that of observed values, and overall, results using listwise deletion were similar to those using multiple imputation. In this paper, we report imputed results; results from listwise deletion are provided in Supplementary file 1.
Sample characteristics at baseline.
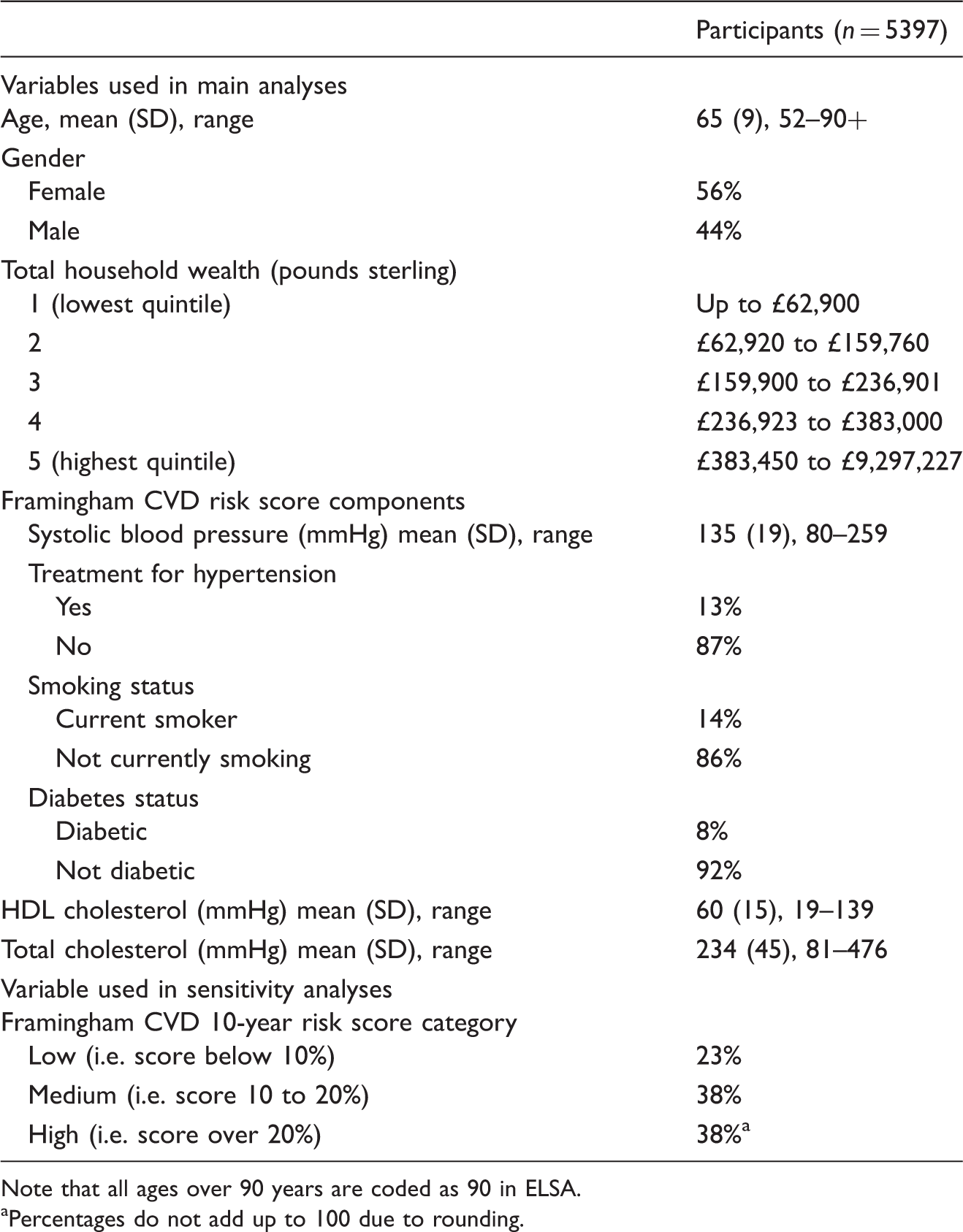
Note that all ages over 90 years are coded as 90 in ELSA.
Percentages do not add up to 100 due to rounding.
Frequency of loneliness and social isolation across waves.
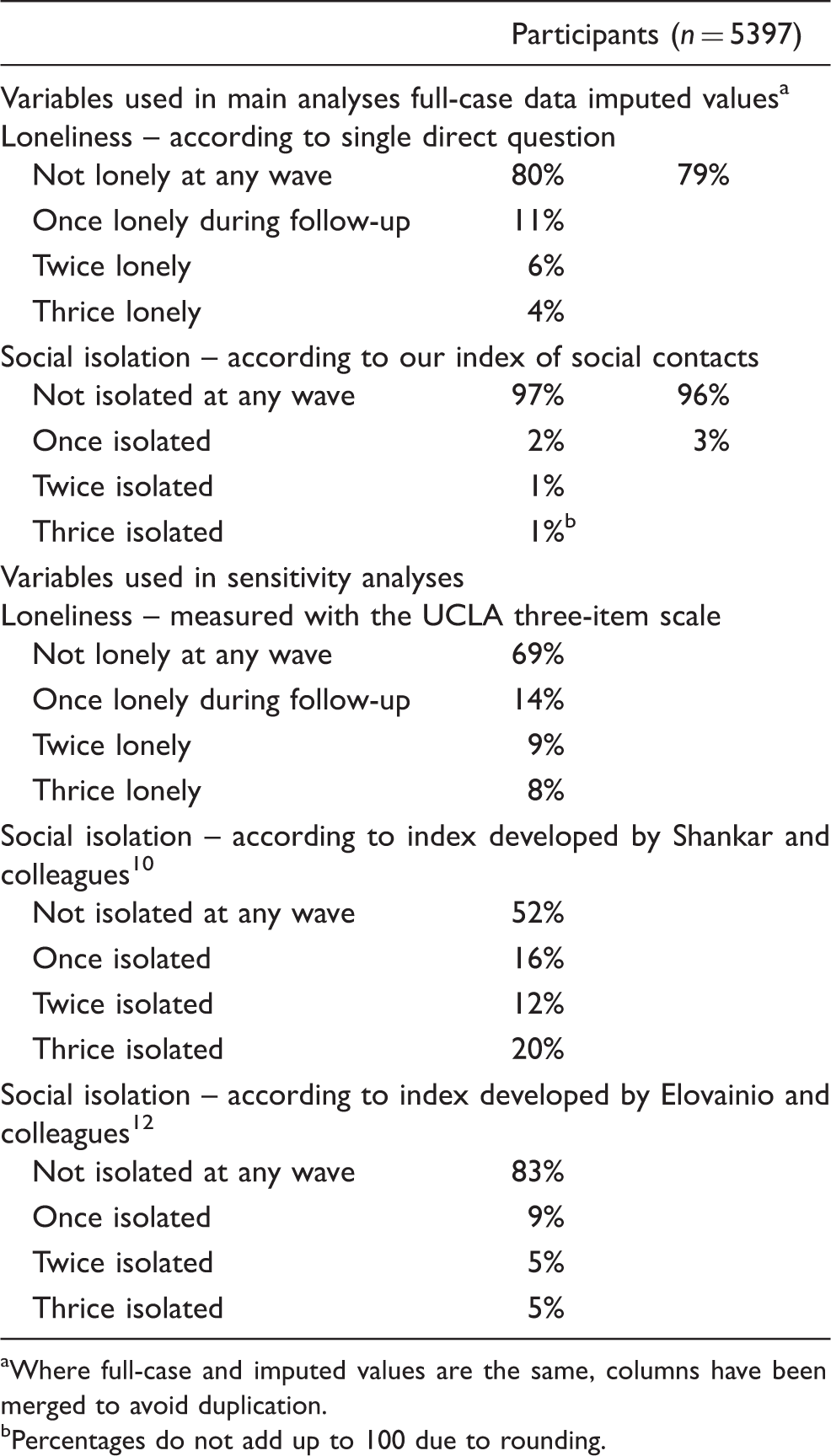
Where full-case and imputed values are the same, columns have been merged to avoid duplication.
Percentages do not add up to 100 due to rounding.
Loneliness, social isolation and incident CVD
Over a mean follow-up period of 5.4 years, 571 first CVD events were recorded. When participants reported a new stroke and heart condition in the same wave (n = 10), these were only counted as one event in our analyses, because we were interested in first events only.
Association between loneliness, social isolation and cardiovascular disease incidence in ELSA in univariable and multivariable discrete time survival analyses.
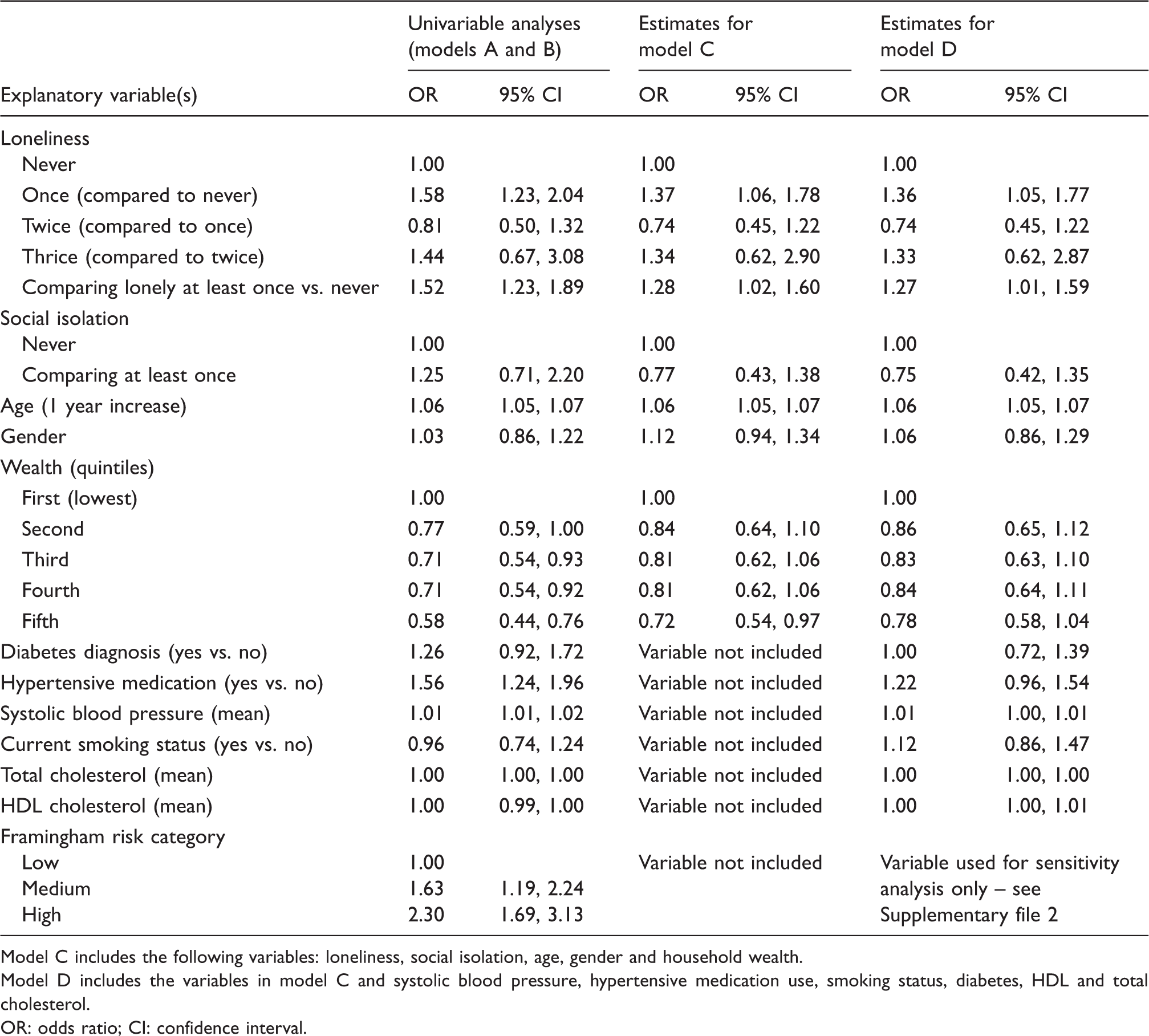
Model C includes the following variables: loneliness, social isolation, age, gender and household wealth.
Model D includes the variables in model C and systolic blood pressure, hypertensive medication use, smoking status, diabetes, HDL and total cholesterol.
OR: odds ratio; CI: confidence interval.
Loneliness
In univariable analyses, reporting one instance of frequent loneliness was associated with an increased risk of incident CVD (OR 1.58, 95% CI 1.23–2.04). There was no evidence of a cumulative association for loneliness over time: those who reported loneliness twice were not at greater risk of disease compared with those who reported loneliness once only (OR 0.81, 95% CI 0.50–1.32). Nor were those who reported loneliness three times at higher risk compared to participants with one report only (OR 1.16, 95% CI 0.59–2.30). In the multivariable model adjusting for age, gender, wealth and social isolation, the association between loneliness and CVD persisted (OR comparing one or more to no report of loneliness 1.28, 95% CI 1.02–1.60). This association did not appear to be mediated by traditional CVD risk factors: when systolic blood pressure, total and HDL cholesterol, diabetes, hypertension medication and smoking status were added to the model, loneliness remained an independent predictor of risk (OR comparing one or more to no report of loneliness 1.27, 95% CI 1.01–1.59). Sensitivity analyses based on the UCLA three-item scale suggested a similar magnitude of association between loneliness and increased risk of an event (OR comparing once or more vs. never lonely in model D 1.21, 95% CI 0.98–1.49), and did not point to a cumulative association (see Supplementary file 2).
Social isolation
Social isolation was not identified as an independent predictor of CVD risk in our analyses (in model A, OR comparing at least one vs. no instance of isolation 1.25, 95% CI 0.71–2.20; in model D, OR 0.75, 95% CI 0.42–1.35). Sensitivity analyses based on the Shankar index suggested that isolation might predict CVD when no other variables were taken into account (crude OR 1.20, 95% CI 1.00–1.44), but once age, gender, wealth and loneliness were introduced this association disappeared (adjusted OR 0.93, 95% CI 0.88–1.30). Analyses using Elovainio's index produced similar results to our main analyses (crude OR 1.16, 95% CI 0.89–1.52; in the model adjusting for potential confounders and traditional CVD risk factors, OR 0.79, 95% CI 0.59–1.06).
Associations between loneliness, isolation and disease incidence did not change when the items contributing to the Framingham score were replaced by CVD risk category – see Supplementary file 2 for the full set of results from the sensitivity analyses.
Discussion
Main findings and comparison with other work
Our study found that reporting feeling lonely was associated with an increased risk of CVD: the event rate was 27% higher among those who reported feeling lonely at least once over the 6-year study period. The magnitude of this association is comparable to the influence of recognised psychosocial factors, including depression and anxiety.26,27 There was no evidence of a cumulative association: reporting loneliness twice or three times was not associated with a stronger risk of CVD when compared with reporting one instance only.
To our knowledge, this is the first study to examine loneliness and social isolation simultaneously as time-dependent variables in relation to incident fatal and non-fatal cardiovascular risk. A previous Dutch study with multiple measures of loneliness had not reported clear evidence of an association between feeling lonely and cardiovascular mortality in older men (hazard ratio associated with being severely lonely 1.18, 95% CI 0.58–2.39). 28 The absence of a statistically significant effect is likely to have stemmed from the study's relatively small sample size: 719 men in total, only 23 of whom were classed as being ‘severely lonely’. Our study relied on a sample of over 5000 individuals, surveyed every 2 years rather than every 5 years in the Zutphen Elderly Study. Future studies with even shorter periods between data collection points will help to gauge the most appropriate time frame for studying loneliness in relation to CVD incidence.
The association between loneliness and CVD incidence persisted when the main biological and behavioural CVD risk factors were controlled for, suggesting that the mechanisms at play may be more to do with psychological pathways (e.g. depression, anxiety, self-esteem) and/or other behaviours, including alcohol consumption and physical activity. Prospective longitudinal studies have identified loneliness as a risk factor for higher levels of depressive symptoms,29,30 which in turn are associated with a heightened risk of experiencing a CVD event.31,32 Reviews of the literature have also highlighted loneliness as a risk factor for both higher alcohol consumption and lower physical activity.33,34 As health-related behaviours and psychological states can in turn influence loneliness, it is important to bear in mind that the latter may be a marker or ‘symptom’, rather than a cause, of the former. We know that psychosocial risk factors such as depression and anxiety are prevalent among people who have experienced a coronary event, 35 and it may be that loneliness is a manifestation of subclinical symptoms related to CVD. Based on our data and analyses, we cannot assume that loneliness was a causal factor; further analyses will be needed to disentangle potential reverse causality and synergistic effects.
While univariate analyses suggested that social isolation might be linked to a greater risk of CVD (with effect sizes ranging from 1.16 to 1.25 depending on the measure of isolation used), there was no evidence of an effect once loneliness and traditional risk factors were controlled for. This finding, along with our results relating to loneliness, suggests that the quality of relationships may be more important than quantity when assessing disease risk. When people have chosen to have limited interaction with others, they may have developed resilience mechanisms and ways of countering the potentially detrimental consequences of isolation (e.g. by making sure that they continue to drive because they may not be able to rely on anyone else to do so for them, or by making sure that they regularly consult healthcare practitioners to prevent any worsening of their health). We know that interaction with others is not always beneficial, and wider networks may include negative social interactions such as conflict, demands and abuse, which have been linked to physiological processes including allostatic load 36 and elevated hypothalamic–pituitary–adrenal axis responses. 37
Strengths and limitations
Our study drew on the strengths of ELSA, a nationally representative cohort study of adults aged over 50 years who provide robust demographic, social and biological data. This enabled us to incorporate into our analyses the risk factors routinely considered when assessing patients, to ensure that our analyses were relevant to clinical practice. The longitudinal design of the study allowed us to focus on the prospective association between social relationships and CVD, although we acknowledge that reverse causation – in which deficiencies in social relationships are the result of subclinical disease – remains a possibility. Unfortunately, because not all variables were collected at each wave (e.g. the nurse visit was carried out every 4 years, i.e. in alternate waves), it was not possible for us to investigate whether, when treated as time-varying, the relationship between factors such as wealth or CVD risk and social relationships changed.
As there is no consensus on which tools are most appropriate for assessing social relationships, we used multiple measures of loneliness and social isolation to test the robustness of our findings. We found no marked differences in results relating to either loneliness or social isolation, suggesting that a shorter index (as developed by Elovainio and colleagues, for example) 12 could be sufficient to capture the implications of a person's social network for health. Future studies comparing the overlap across measures, and their relationship with different outcomes, will help to clarify which tools might be most appropriate for use in epidemiological studies. Sensitivity analyses were also run using the Framingham score, which captures CVD risk over a 10-year period; the results obtained resembled those based on the baseline measures of cholesterol, diabetes, blood pressure, smoking status and hypertensive medication.
Non-fatal CVD events were self-reported by participants at every wave. While this is generally recognised as a relatively robust measure of outcomes such as myocardial infarction or stroke, it may be that participants omitted to, or incorrectly reported, certain events. The possibility that our results were affected by systematic misreporting cannot be excluded, and nor can we be certain that the month and year of diagnosis they provided was accurate.
Similar to many other panel studies, attrition in ELSA is socioeconomically graded and more severe among underprivileged individuals. 5 As lower socioeconomic status is associated with weaker social relationships and CVD incidence, it may be that our analyses underestimate the effect of loneliness and social isolation. Participants lost to follow-up were more likely to report lower levels of education, be less wealthy, be older and report a limiting long-standing illness. 5 As socioeconomic status, age and health are risk factors for loneliness and social isolation as well as CVD,10,11,18,19,38 it is possible that people lost to follow-up were more lonely or isolated, and at greater risk of CVD compared with individuals who remained in the study. We also note that patients with prior events, and patients with otherwise poor health and disability, individuals on anticoagulant drugs, and those reporting clotting or bleeding disorders, were excluded from this study. These subjects could be more prone to isolation and at greater risk of CVD; their exclusion may explain that we found no association between social isolation and CVD incidence, and we cannot generalise our findings to these populations. Nor can we exclude confounding by other causes not included in our models. Many factors, such as depression and health-related behaviours, may be both confounders and on the causal pathway. As survival analyses do not enable us to distinguish between these two effects, we restricted the variables in our models to the factors routinely assessed in practice. Our hypothesis was that loneliness and isolation could be markers of, if not causal factors for, disease risk. In common with other observational studies, we cannot infer causality from our data.
Implications
The finding that lonely individuals are at increased risk of CVD suggests that practitioners ought to take perceptions of social relationships into account when assessing patient risk. Identifying someone as lonely could help to flag up a person who may not be considered at risk of CVD according to traditional factors but whose likelihood of experiencing a CVD event is high nonetheless. More so than objective characteristics such as the size, composition or diversity of a person's social network, subjective perceptions of one's relationships can provide insight into a person's wellbeing; highlighting an individual's loneliness could be the first step in preventing the development and worsening of other risk factors for CVD, including anxiety, depression and health-damaging behaviours such as smoking and drinking. The direct question included in the ELSA interview could be a useful tool for practitioners to identify people who would not otherwise be scored as being at risk of CVD with tools such as the Framingham score. Because individuals may not wish to discuss negative feelings about the people in their lives publicly, it will also be important to consider indirect measures such as the three-item UCLA scale 9 or the de Jong Gierveld loneliness scale. 39
From a public health perspective, our finding that repeated instances of loneliness, compared with only reporting loneliness once, were not associated with a higher risk of CVD suggests that it may be particularly difficult for secondary and tertiary prevention strategies to affect health outcomes positively. If loneliness reflects undiagnosed symptoms, then targeting people who already feel lonely may not reduce CVD risk. In the absence of evidence pointing to the health benefits of improvements in loneliness, primary prevention strategies could be a more promising way of tackling loneliness and its adverse health implications. To date, national initiatives including the Campaign to End Loneliness in the UK, Coalitie Erbij in The Netherlands and MONALISA in France have focused on strengthening the social relationships of people who already experience chronic loneliness. Existing initiatives led by the World Health Organization and European Union (EU) to promote good health and wellbeing in later life, including age-friendly cities and the EU's ‘healthy ageing’ campaign, could in future broaden the agenda to primary prevention and incorporate a ‘loneliness’ component.
Supplemental Material
Supplemental material for Loneliness, social isolation and risk of cardiovascular disease in the English Longitudinal Study of Ageing
Supplemental material for Loneliness, social isolation and risk of cardiovascular disease in the English Longitudinal Study of Ageing by Nicole K Valtorta, Mona Kanaan, Simon Gilbody and Barbara Hanratty in European Journal of Preventive Cardiology
Footnotes
Author contribution
NKV developed the idea for the article and conducted the analyses under the supervision of MK, SG and BH. NKV wrote the first draft, with all authors contributing to critical revision of the manuscript for important intellectual content. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy. NKV is the guarantor.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was funded by the National Institute for Health Research, through a personal doctoral fellowship awarded to NV (NIHR DRF‐2013‐06‐074). The funder had no role in: the study design; in the collection, analysis, and interpretation of data; in the writing of the report; and in the decision to submit the article for publication. The views and opinions expressed in this article are those of the authors and do not necessarily reflect those of the Department of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.