
Abstract

Cardiovascular disease (CVD) is a leading cause of death in women. Women who suffer an acute coronary event are more likely to be less physically active than men. 1 Participation in exercise-based cardiac rehabilitation (CR) has been shown to improve exercise capacity, enhance quality of life and reduce cardiovascular mortality. 2 Although women are in need of the secondary prevention advantages provided by CR, they are, ironically, less likely than men to adhere to CR. 3 Traditional CR may not meet the needs of women; innovative programmes which target women’s motivation and interests are in dire need. 4 Women-only CR is becoming more common, but developing new, women-only programmes can be challenging and costly particularly when adherence rates are low. 5 Introducing different exercise modalities in existing CR programmes may be a more feasible option for programme directors and benefit the women they serve.
Aerobic interval training (AIT) has been shown to produce similar or greater improvements in physical and psychosocial health outcomes in a time-efficient manner when compared to traditional moderate-to-vigorous intensity continuous exercise (MICE) in patients with CVD. 6 Such studies have, however, predominantly involved men, and rarely addressed mental health. 6 The purpose of this matched case–control study was to examine the impact of AIT when compared to MICE on mental and physical health outcomes in women with CVD participating in CR, with the hypothesis that AIT would produce similar or greater improvements in mental and physical health outcomes when compared to MICE.
Women who engaged in MICE served as the controls; they were matched for age (±2 years, on average) and cardiovascular diagnosis. Approval for the study was obtained from the Ottawa Health Sciences Network Research Ethics Board (protocol no. 20170721-01H). All exercise training sessions were performed in our prevention and rehabilitation centre. AIT participants exercised twice weekly for 10 weeks. The initial 2 weeks of the 10-week programme served as a familiarisation period during which participants learned a dance-based routine for the AIT protocol. Each session was 45 minutes in duration and followed a modified Norwegian AIT protocol which consisted of: (a) 10-minute warm-up at 60–70% peak heart rate (HR); (b) 4 × 4 minutes of high-intensity intervals at 85–95% peak HR interspersed with 3 minutes of low-intensity intervals at 60–70% peak HR; and (c) 10-minute cool-down at 60–70% peak HR. MICE participants exercised twice weekly for 8 weeks. Each session was 60 minutes in duration and followed CR guidelines which consisted of: (a) 10-minute warm-up; (b) 35 minutes of aerobic conditioning at 70–85% peak HR (i.e. moderate-to-vigorous intensity); and (c) 15-minute cool-down. 7 Peak HRs were estimated using the formula: 220 – age (–30 bpm for those taking β-blockers). 8 Depression and anxiety were assessed using the hospital anxiety and depression scale (HADS), and body mass, body mass index (BMI), waist circumference, resting blood pressure and HR were measured using standardised procedures at the beginning and end of CR.
Participant characteristics at baseline (N = 60).
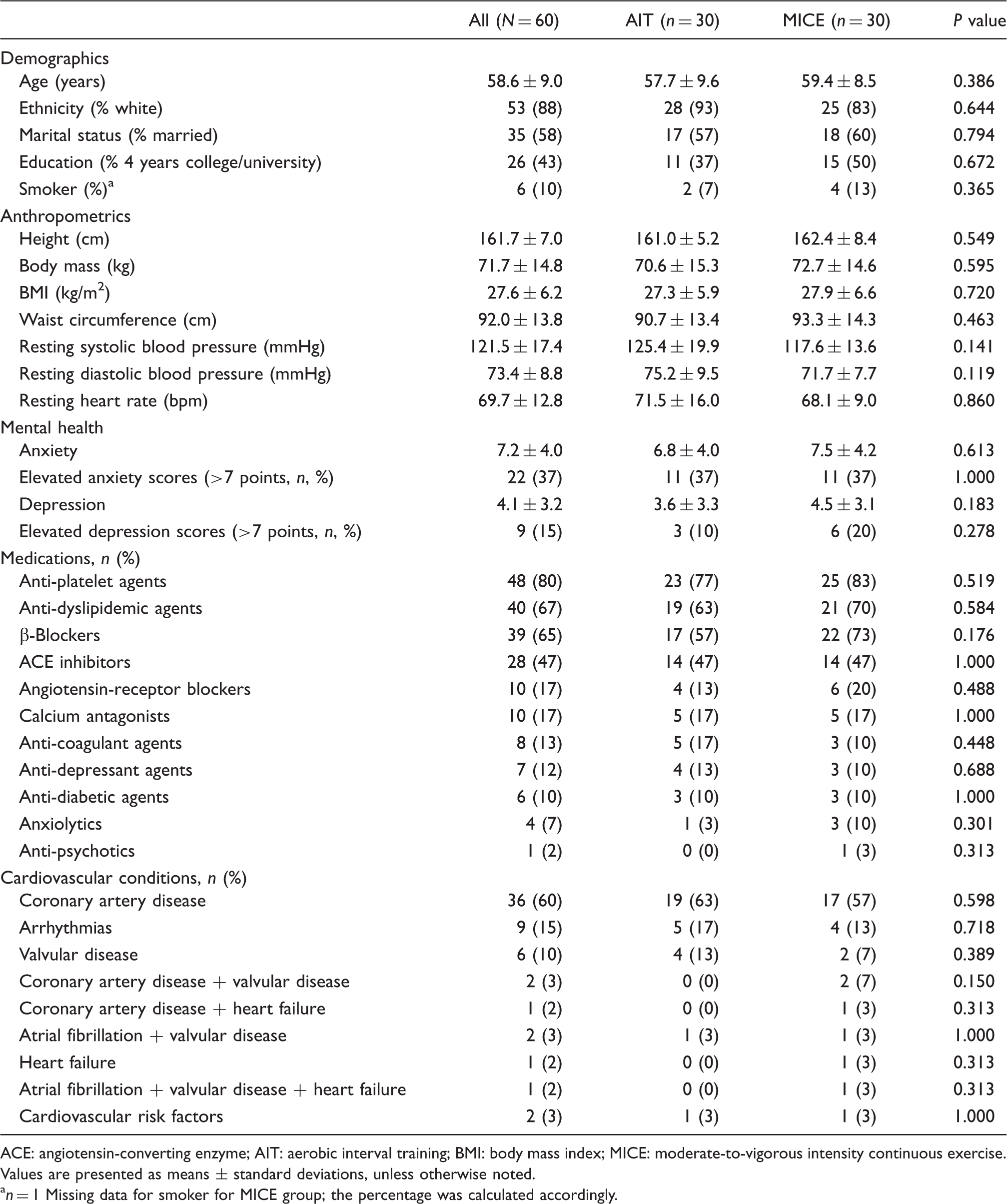
ACE: angiotensin-converting enzyme; AIT: aerobic interval training; BMI: body mass index; MICE: moderate-to-vigorous intensity continuous exercise.
Values are presented as means ± standard deviations, unless otherwise noted.
n = 1 Missing data for smoker for MICE group; the percentage was calculated accordingly.
This study is the first, to our knowledge, to compare the efficacy of AIT and MICE in improving mental and physical health outcomes in women with CVD participating in exercise-based CR. This work is particularly important as few studies have addressed CR in women, and none have examined the impact of varying CR modalities (e.g. AIT vs. MICE) in women, a population that is less likely than men to be referred to, enroll in and adhere to traditional CR offerings.
We observed improvements in the severity of anxiety and depression following AIT and MICE, with no significant differences between these exercise modalities. Our findings are consistent with the previous evidence of improvements in mental health following CR – exercise-based CR involving patients of varying age, sex, diagnosis, comorbidities and mental health status have been shown to produce significant positive mental health outcomes.
7
The improvement in anxiety severity in the AIT group (i.e. −1.8 points) met clinical significance (see Figure 1); the minimal clinically important difference for the HADS among those with CVD completing CR is 1.7 points.
9
It is suggested that those with lower self-efficacy are more likely to believe that they cannot exert control over their environment and experience more distress. It is, therefore, plausible that our AIT, which required women to exercise at a higher intensity, engendered greater confidence in their ability to exercise; this increased self-efficacy may have led to the clinically significant reduction in anxiety levels that was observed.
10
It is unknown if the addition of other exercise training paradigms (i.e. progressive resistance training) to AIT would lead to further improvements in mental health outcomes in women with CVD.
11
Change in HADS scores from baseline to follow-up in women participating in MICE and AIT. Negative change scores indicate an improvement in anxiety and depression severity. The MCID is represented by a black dashed line (i.e. 1.7 points). AIT: aerobic interval training; HADS: hospital anxiety and depression scale; MCID: minimal clinically important difference; MICE: moderate-to-vigorous intensity continuous exercise. Values are presented as means ± standard error of means.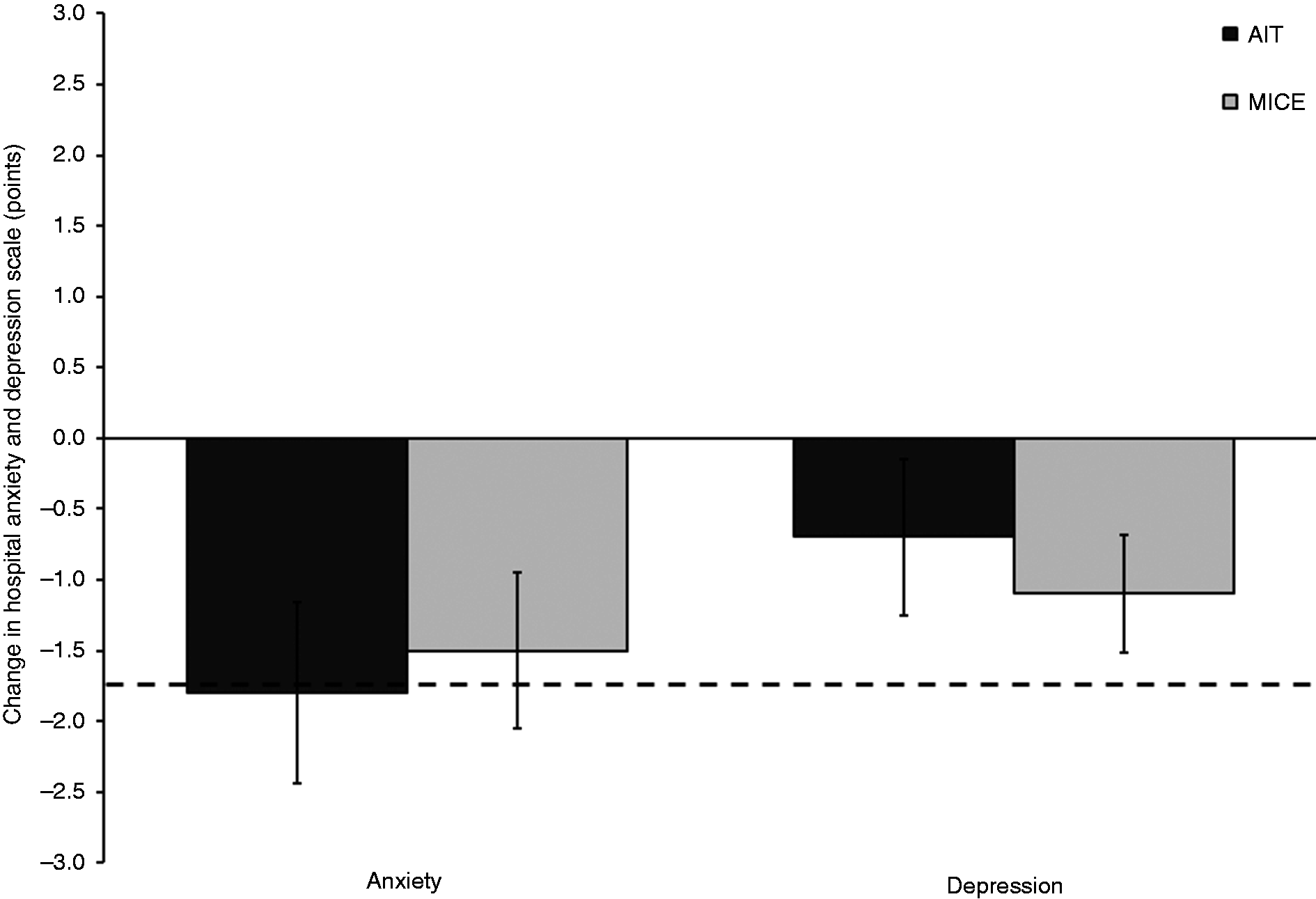
We observed improvements in BMI and waist circumference following AIT and MICE, with no significant differences between these exercise modalities. These findings are unsurprising given CR generally includes weight management as a programmatic component, although weight loss outcomes in CR have been modest at best. The 4 cm reduction in waist circumference following AIT is clinically significant as women decreased from high (90–110 cm) to low (70–89 cm) cardiometabolic health risk. 12 These findings are important; recent research highlights that waist circumference may be a stronger predictor of mortality risk than BMI. 13
Lack of time is a key barrier to routine exercise participation among women with CVD. Innovative, tailored CR for women such as our dance-based AIT that provides mental and physical health benefits with reduced time commitment (i.e. 45 vs. 60 minutes) may address an established barrier to women’s participation in CR. For women who find elements or the style of traditional CR less than inviting, AIT may afford more enjoyable and acceptable opportunities for participation in CR. AIT ensures women exercise at higher intensities which may be more effective in increasing self-efficacy for exercise and decreasing anxiety. It is important that we develop and evaluate innovative and imaginative physical activity programmes to attract, facilitate and increase the participation of women in CR.
Footnotes
Author contribution
JLR conceptualised and designed the study, performed the analyses and interpretation of the data, drafted the initial manuscript, and revised and approved the final manuscript as submitted. MLK, RAB and AZB contributed to conception, design and data acquisition, provided critical revision of the manuscript, and approved the final manuscript as submitted. AEC contributed to data acquisition, provided critical revision of the manuscript, and approved the final manuscript as submitted. ALP and HET contributed to the conception, provided critical revision of the manuscript, and approved the final manuscript as submitted. All authors agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Acknowledgments
This work was presented during the Young Investigator Award (Exercise Basic and Translational Research) session at EuroPrevent in Ljubljana, Slovenia (2018).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported, in part, by a Canadian Institutes of Health Research (CIHR) New Investigator Salary Award in clinical rehabilitation (JLR). No other specific grant from any funding agency in the public, commercial or not-for-profit sectors was received to carry out the work.