
Abstract
Background and design
There are limited data on the effects of blood pressure and cholesterol lowering in Asians at intermediate risk and no cardiovascular disease. We report an analysis of the effects of blood pressure and cholesterol lowering in Asians enrolled in the Heart Outcomes Prevention Evaluation 3 (HOPE 3) trial.
Methods
We randomly assigned 6241 Asians and 6464 non-Asians at intermediate risk without cardiovascular disease to candesartan 16 mg/hydrochlorothiazide 12.5 mg or placebo and rosuvastatin 10 mg or placebo. The first co-primary outcome was a composite of cardiovascular disease death, myocardial infarction and stroke. The second co-primary outcome additionally included heart failure, cardiac arrest and revascularisation. Median follow-up was 5.6 years.
Results
Reduction in systolic blood pressure was less among Asians (4.3 vs. 7.7 mmHg for non-Asians, P < 0.0001) mainly due to a lesser effect in Chinese (2.1 mmHg) than in other Asians (7.3 mmHg), reduction in the latter being similar to non-Asians. The effect on the composite outcomes was similar, with no significant benefits from blood pressure lowering for either Asians (Chinese or non-Chinese) or non-Asians. Rosuvastatin reduced low-density lipoprotein cholesterol to a lesser degree in Asians (0.49 mmol/L (–19.1 mg/dL) compared with non-Asians 0.95 mmol/L (−36.7 mg/dL), Pinteraction < 0.0004). Yet both groups had similar reductions in the two co-primary outcomes. There was no increase in permanent medication discontinuation due to muscle-related symptoms in either group. There was an excess in new diabetes in non-Asians (4.70% rosuvastatin, 3.52% placebo, P = 0.025) but not in Asians (3.02% rosuvastatin, 4.04% placebo, P = 0.0342), Pinteraction = 0021.
Conclusions
Candesartan/hydrochlorothiazide had fewer effects in reducing blood pressure in Chinese and rosuvastatin reduced low-density lipoprotein cholesterol to a lesser extent in Asians compared with non-Asians. There was no overall reduction in clinical events with lowering blood pressure in either Asians or non-Asians, whereas there were clear and consistent benefits with lipid lowering in both. Despite extensive analyses, we have no obvious explanation for the observed findings. Future studies need to include larger numbers of individuals from different regions of the world to ensure that the results of trials are applicable globally.
Introduction
Eighty per cent of the global burden of cardiovascular disease (CVD) occurs in low and middle income countries.
1
The recommended strategy for primary prevention2,3 – identifying people at risk and titrating medications individually to target levels of risk factors – requires multiple visits to a healthcare facility, carries a high burden on staff and patients, increases costs and may reduce adherence. In 2003 Wald and Law
4
proposed that, if all people older than 55 years or with CVD were to be given a fixed-dose multicomponent pill (with medications to lower blood pressure (BP), low-density lipoprotein (LDL) cholesterol, aspirin and folic acid) myocardial infarction (MI) and stroke could be reduced by 80%, regardless of specific risk factor levels. Although the efficacy and safety of these combination therapies have been studied,5,6 until recently there have been few data on reduction in clinical events. The Heart Outcomes Prevention Evaluation 3 (HOPE 3) trial7–9 demonstrated significant reductions in CVD events with rosuvastatin irrespective of base line LDL-cholesterol or other characteristics. However, BP lowering with the combination of candesartan and hydrochlorothiazide did not reduce CVD in the overall population, except in those in the highest third of systolic blood pressure (SBP) (
Although about half the world’s population lives in Asia, there are limited data on cholesterol or BP lowering in Asians. Furthermore, there have been concerns that statin use may be associated with more adverse effects in Asians.10,11 We report here a prespecified analysis from the HOPE 3 trial comparing the efficacy and safety of both study treatments in Asians and non-Asians.
Methods
Central LDL-cholesterol measurement.
LDL: low-density lipoprotein.
The trial had two co-primary outcomes. Co-primary outcome 1 was the composite of death from cardiovascular causes, non-fatal MI or non-fatal stroke; co-primary outcome 2 included the first composite outcome plus resuscitated cardiac arrest, heart failure or revascularisation. Secondary outcomes included individual components of the co-primary outcomes, and the second co-primary outcome plus angina with evidence of ischaemia. The main safety outcomes included myopathy, rhabdomyolysis and any hospitalisation. All cardiovascular events and cases of new diabetes were adjudicated.
Distribution of subjects (Asian or non-Asian) by country of recruitment or by declared ethnicity.
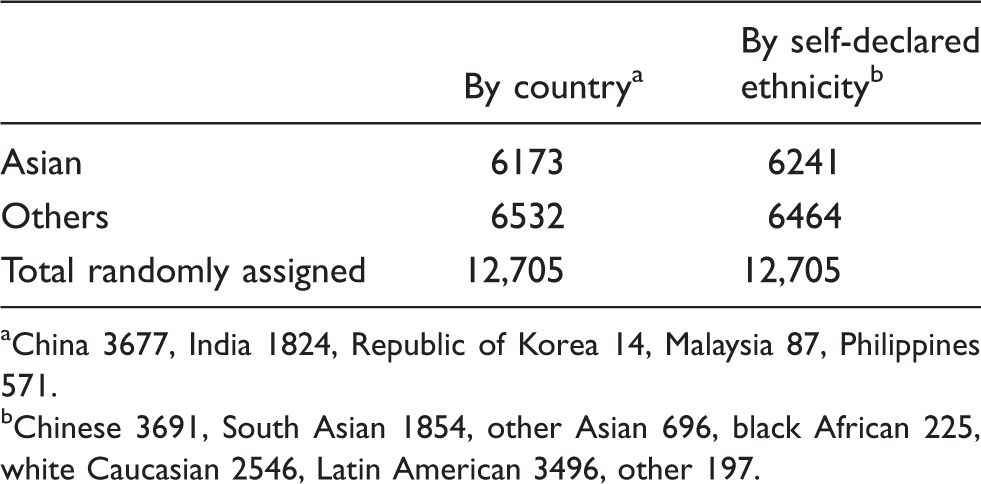
China 3677, India 1824, Republic of Korea 14, Malaysia 87, Philippines 571.
Chinese 3691, South Asian 1854, other Asian 696, black African 225, white Caucasian 2546, Latin American 3496, other 197.
Statistical analysis
Comparisons of the effects on BP, lipids and the clinical events of each treatment versus its respective placebo and of the combination versus double placebo were calculated among Asians and non-Asians using Cox proportional hazards models stratified according to the factorial allocation. The hazard ratio (HR) for each treatment versus its placebo was calculated among Asians and non-Asians and was compared using tests of interaction. Analyses were performed in all randomly assigned subjects and also in those in the upper third of SBP. Analyses were done using SAS version 9.4 (SAS Institute Inc., NC, USA) and figures were generated using S-PLUS 8.2 (TIBCO Software Inc., CA, USA).
Results
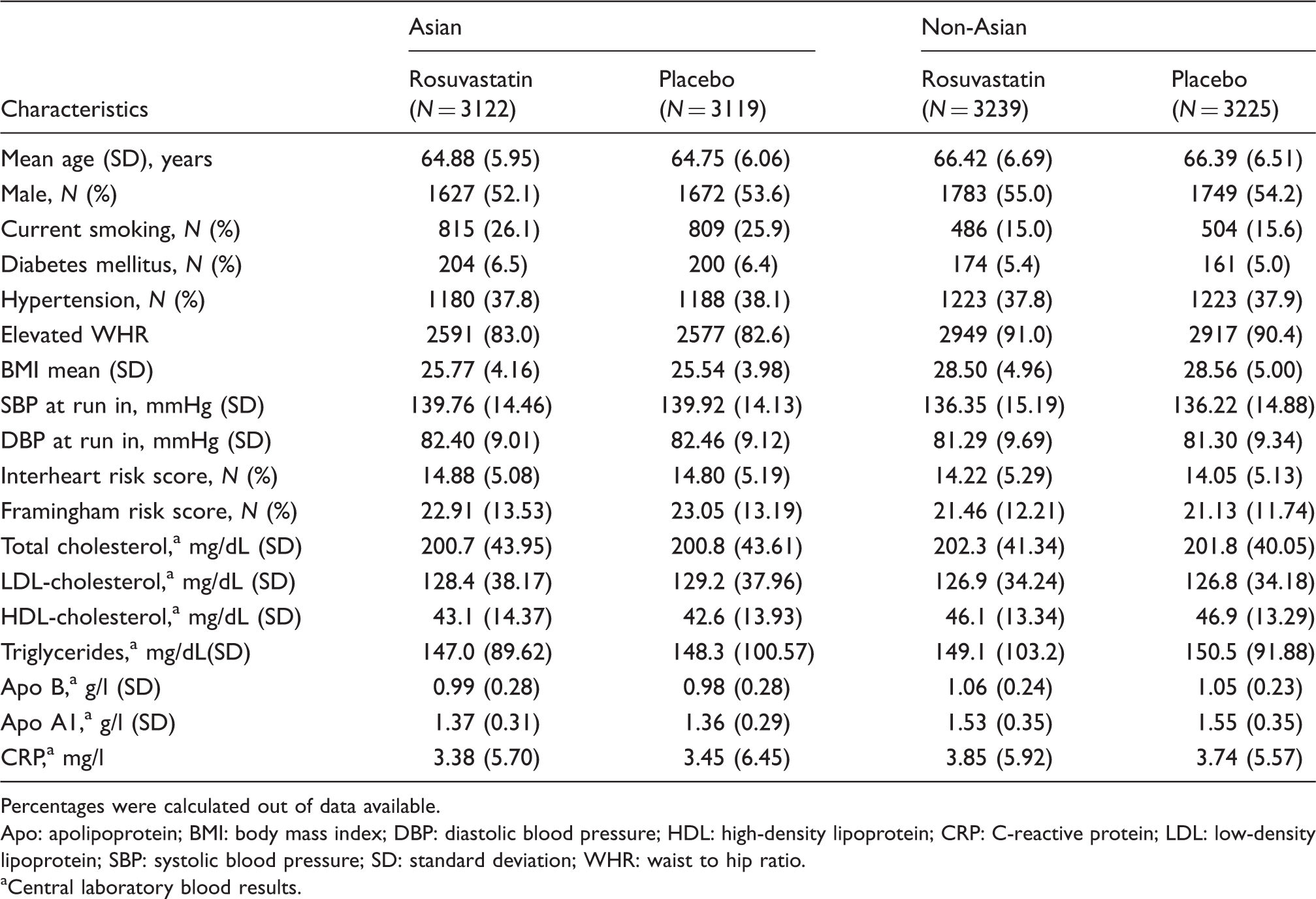
Baseline characteristics in Asians and non-Asians.
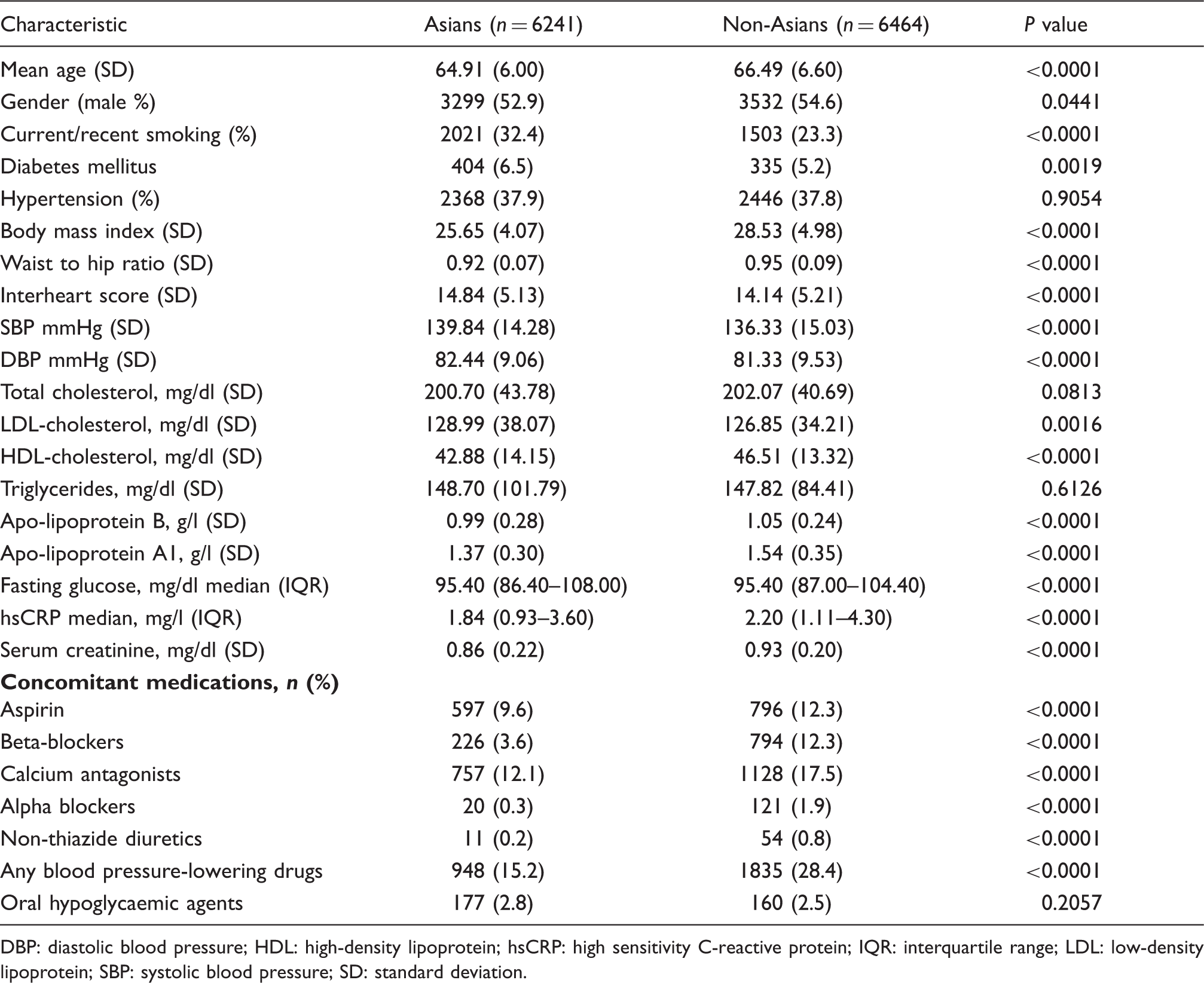
DBP: diastolic blood pressure; HDL: high-density lipoprotein; hsCRP: high sensitivity C-reactive protein; IQR: interquartile range; LDL: low-density lipoprotein; SBP: systolic blood pressure; SD: standard deviation.
Baseline characteristics at run in visit by study arm: candesartan.
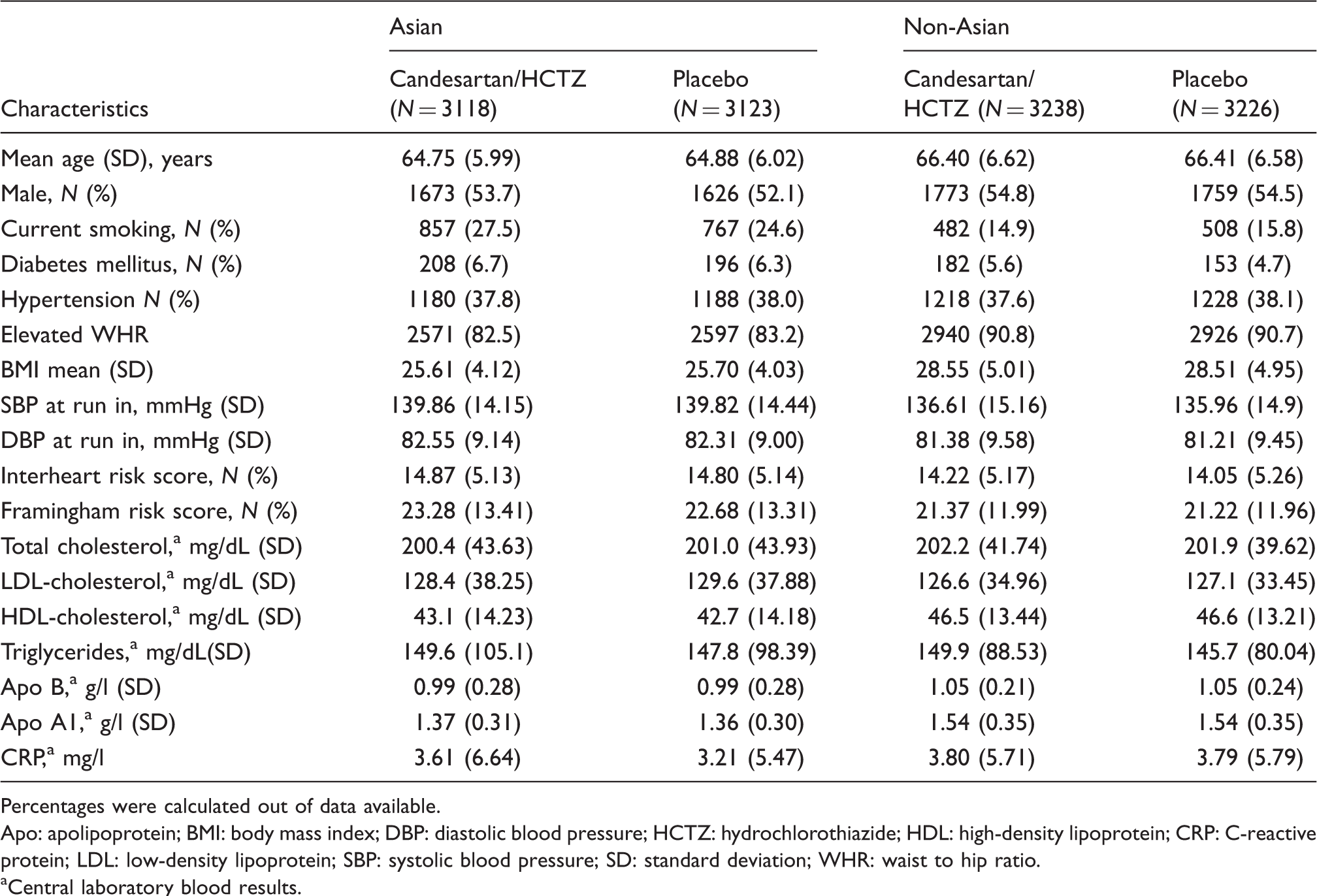
Percentages were calculated out of data available.
Apo: apolipoprotein; BMI: body mass index; DBP: diastolic blood pressure; HCTZ: hydrochlorothiazide; HDL: high-density lipoprotein; CRP: C-reactive protein; LDL: low-density lipoprotein; SBP: systolic blood pressure; SD: standard deviation; WHR: waist to hip ratio.
Central laboratory blood results.
Baseline characteristics at run in visit by study arm: rosuvastatin.
Percentages were calculated out of data available.
Apo: apolipoprotein; BMI: body mass index; DBP: diastolic blood pressure; HDL: high-density lipoprotein; CRP: C-reactive protein; LDL: low-density lipoprotein; SBP: systolic blood pressure; SD: standard deviation; WHR: waist to hip ratio.
Central laboratory blood results.
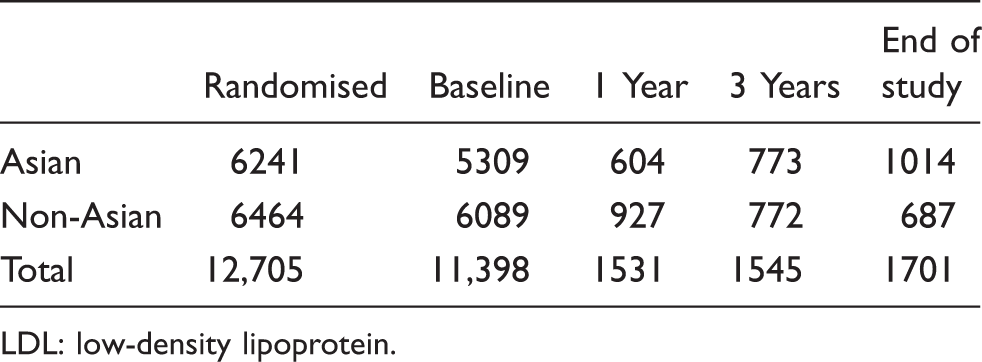
Adherence to study medications.
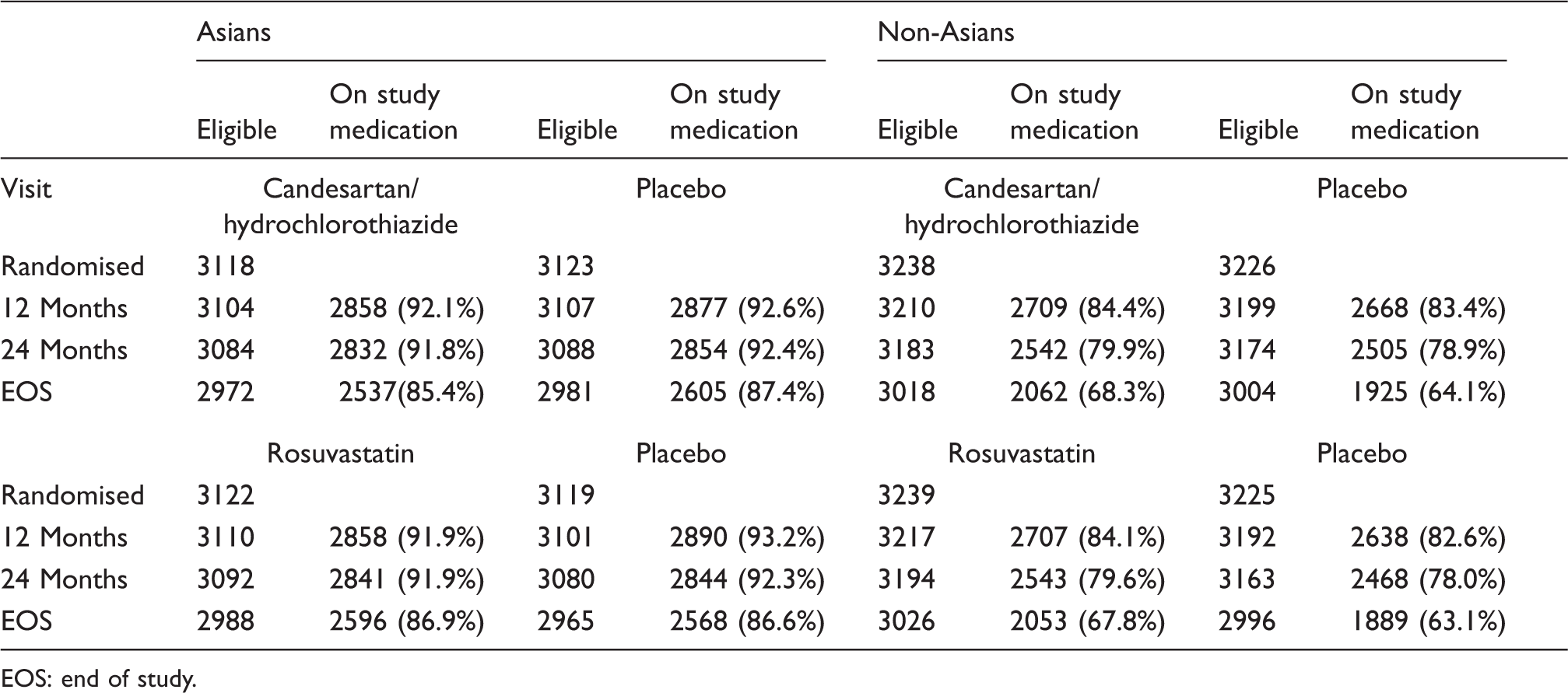
EOS: end of study.
BP-lowering arm
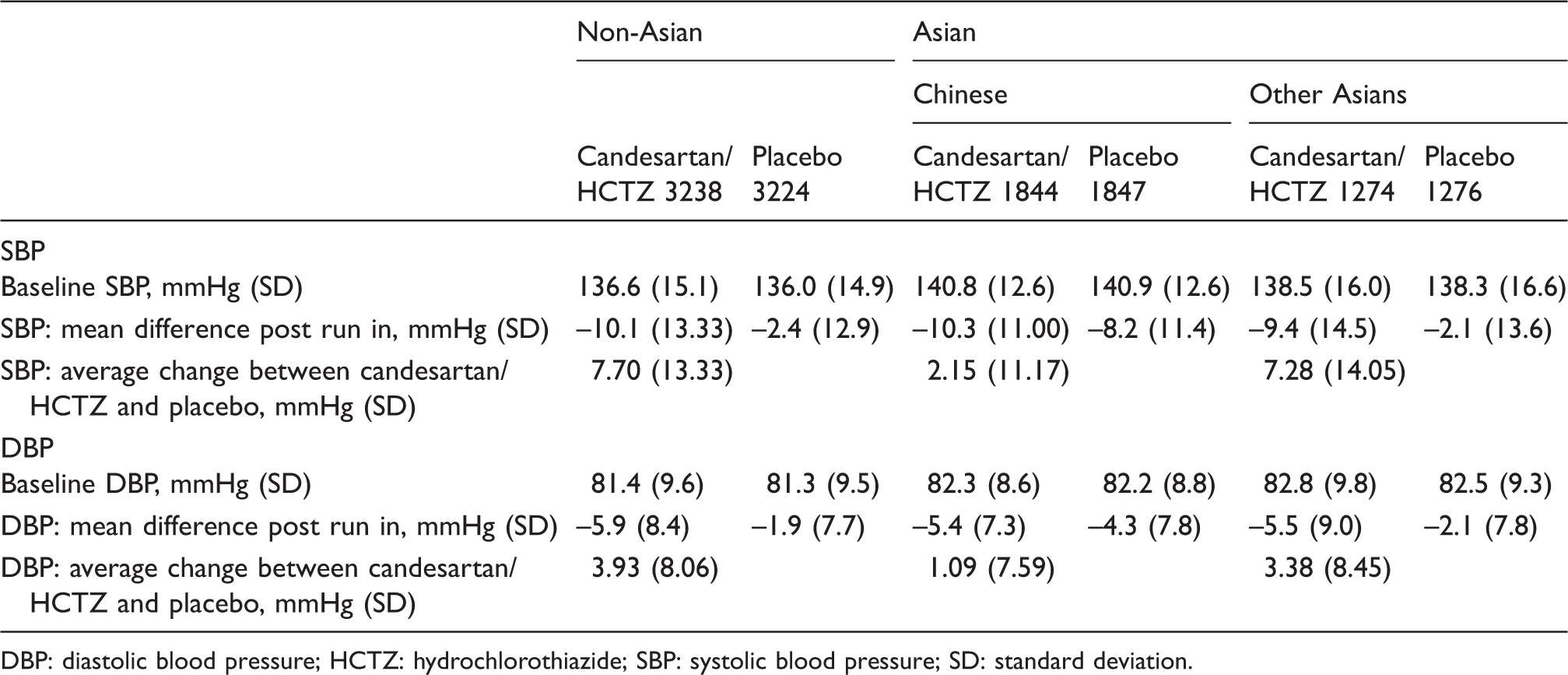
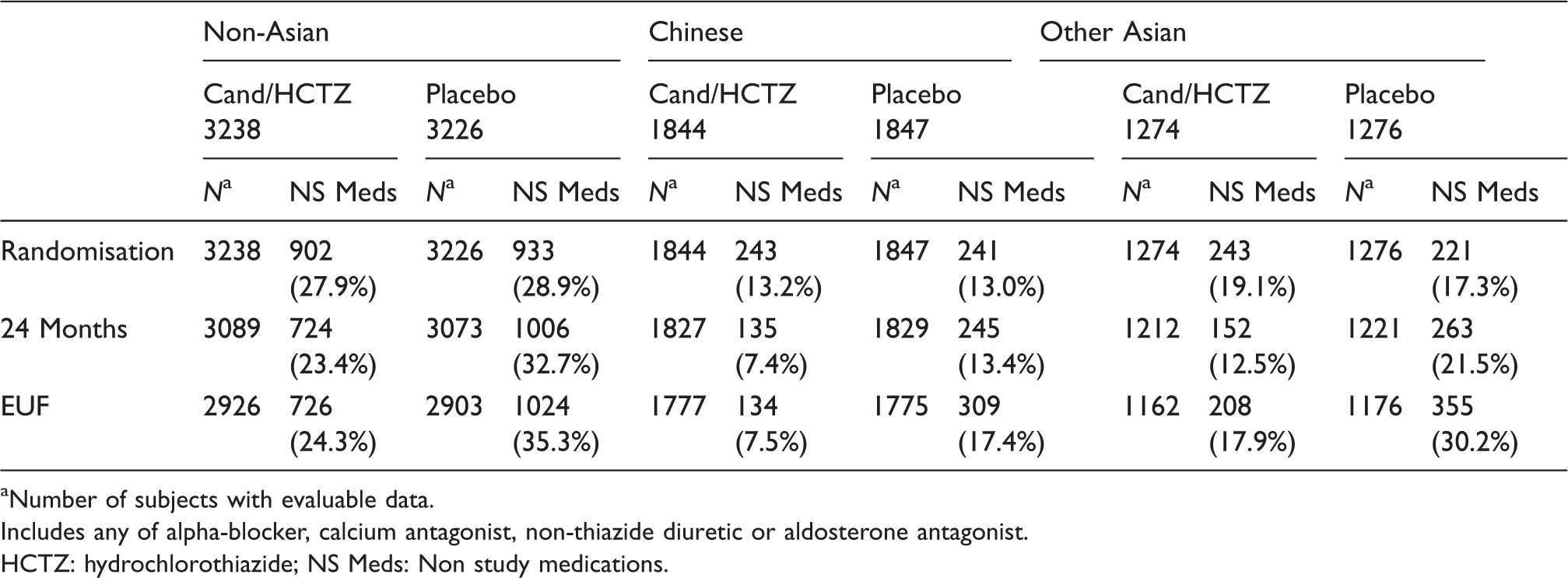
Asians had less reduction in SBP in the active BP-lowering arm (4.3 ± 12.62 mmHg) compared to non-Asians (7.7 ± 13.33 mmHg), Pinteraction < 0.0001) (Figure 1 and Table 7). Among Asians the SBP lowering was significantly more modest among Chinese (difference in SBP of –2.1 ± 11.17 and DBP of –1.1 ± 7.59 between active and control) compared with non-Chinese Asians (difference of SBP –7.3 ± 14.08 and DBP of –3.4 ± 8.45 between active and control (Table 8). This lower reduction in BP among Chinese was not due either to the increased use of open label BP-lowering medications or drug discontinuation (Tables 9 and 10).
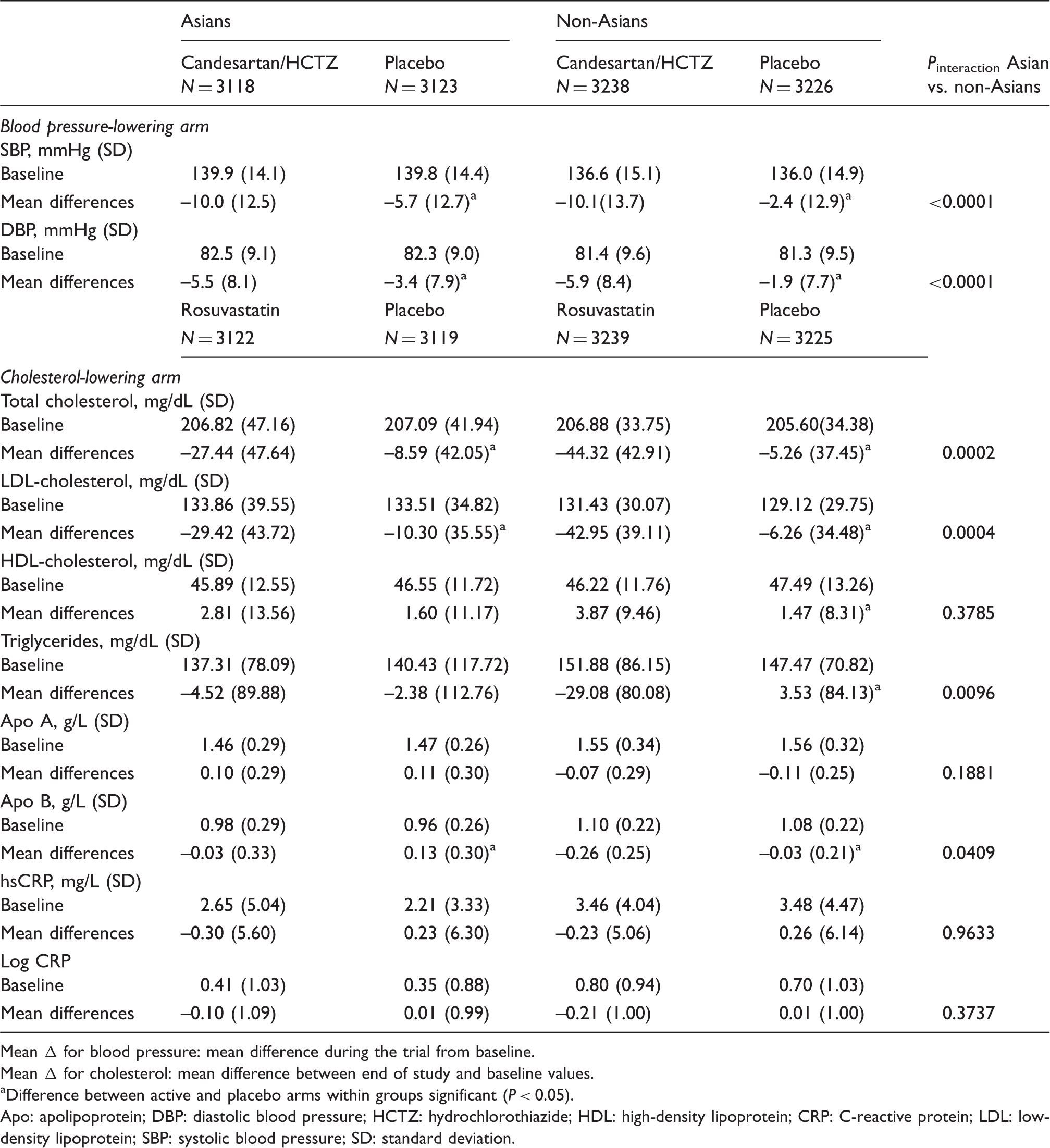
Systolic and diastolic blood pressure by candesartan/hydrochlorothiazide and placebo in Asians and non-Asians. Reductions in blood pressure, lipids and hs-CRP in Asians and non-Asians. Mean Δ for blood pressure: mean difference during the trial from baseline. Mean Δ for cholesterol: mean difference between end of study and baseline values. Difference between active and placebo arms within groups significant (P < 0.05). Apo: apolipoprotein; DBP: diastolic blood pressure; HCTZ: hydrochlorothiazide; HDL: high-density lipoprotein; CRP: C-reactive protein; LDL: low-density lipoprotein; SBP: systolic blood pressure; SD: standard deviation. Blood pressure response to candesartan/HCTZ. DBP: diastolic blood pressure; HCTZ: hydrochlorothiazide; SBP: systolic blood pressure; SD: standard deviation. Use of non-study blood pressure-lowering medication by random assignment to candesartan/HCTZ and placebo. Number of subjects with evaluable data. Includes any of alpha-blocker, calcium antagonist, non-thiazide diuretic or aldosterone antagonist. HCTZ: hydrochlorothiazide; NS Meds: Non study medications. Permanent discontinuation of candesartan/HCTZ and placebo by ethnicity. HCTZ: hydrochlorothiazide.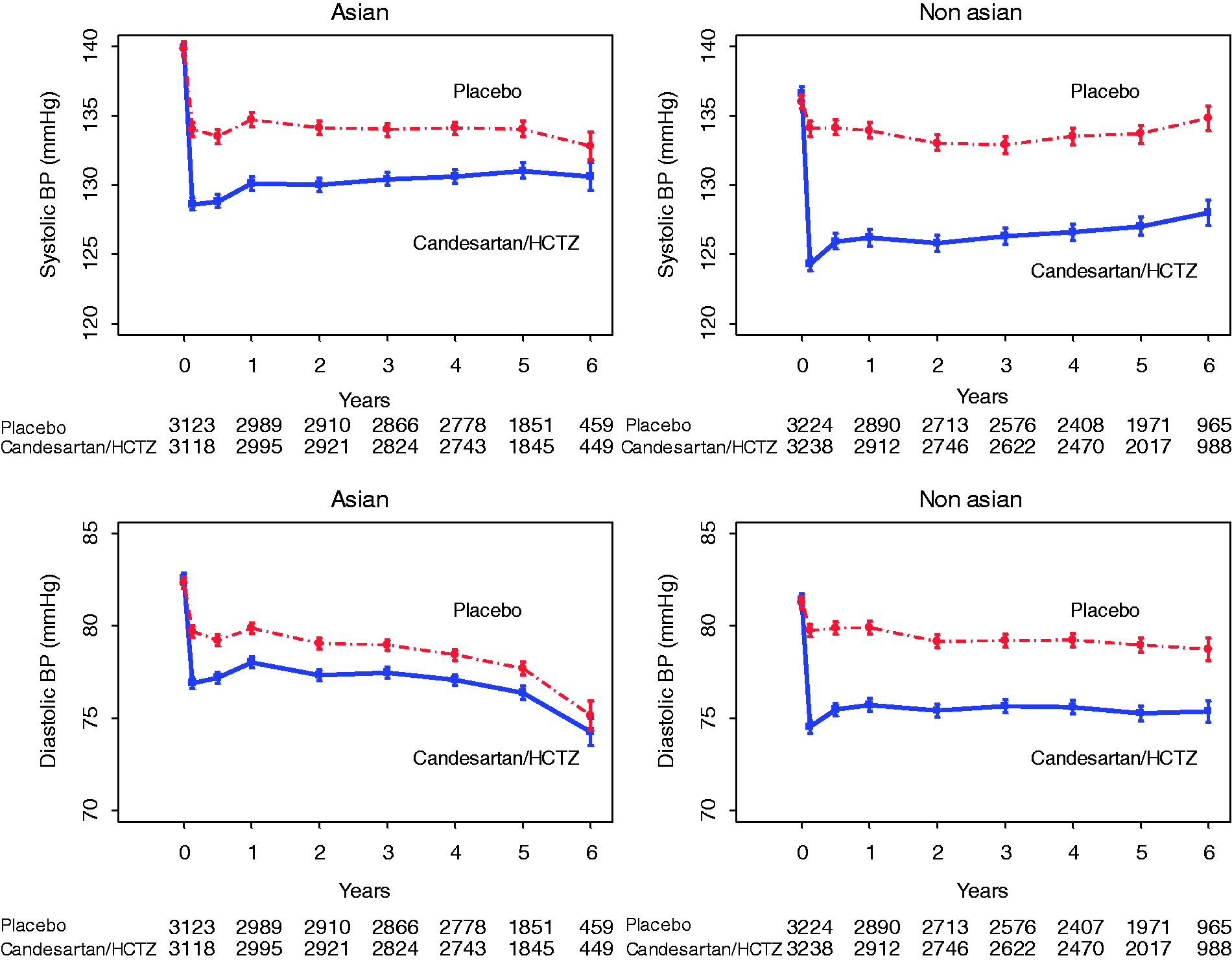

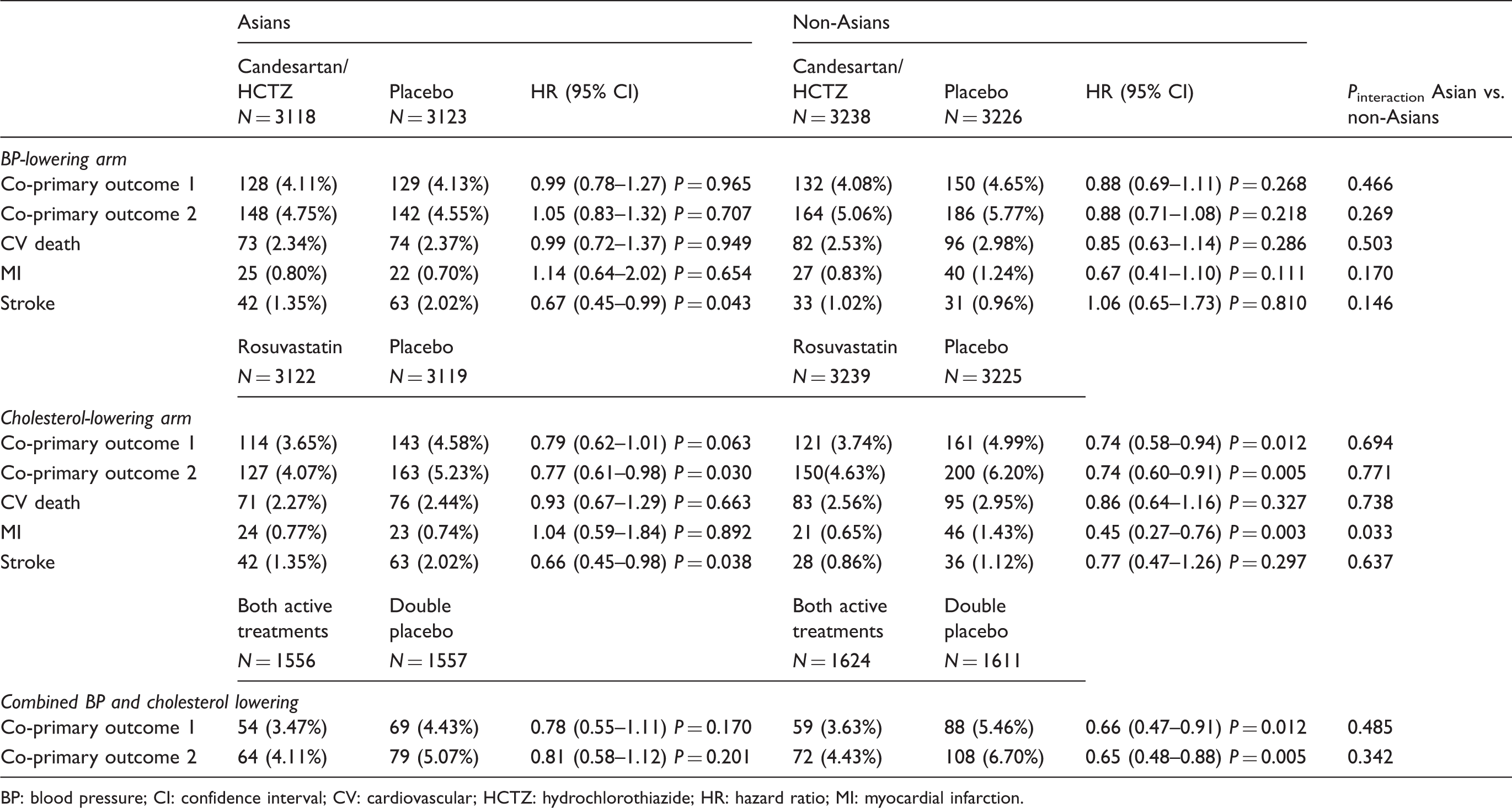
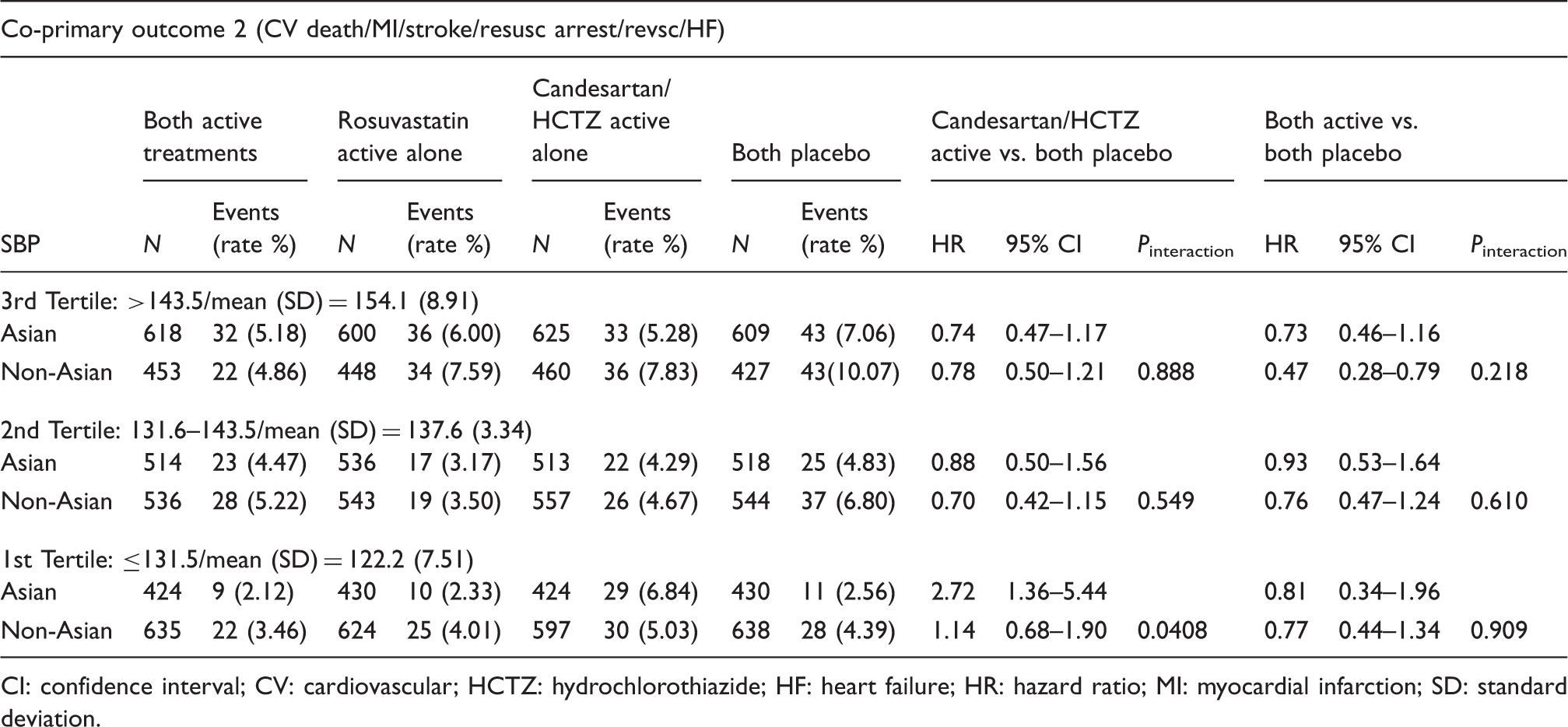
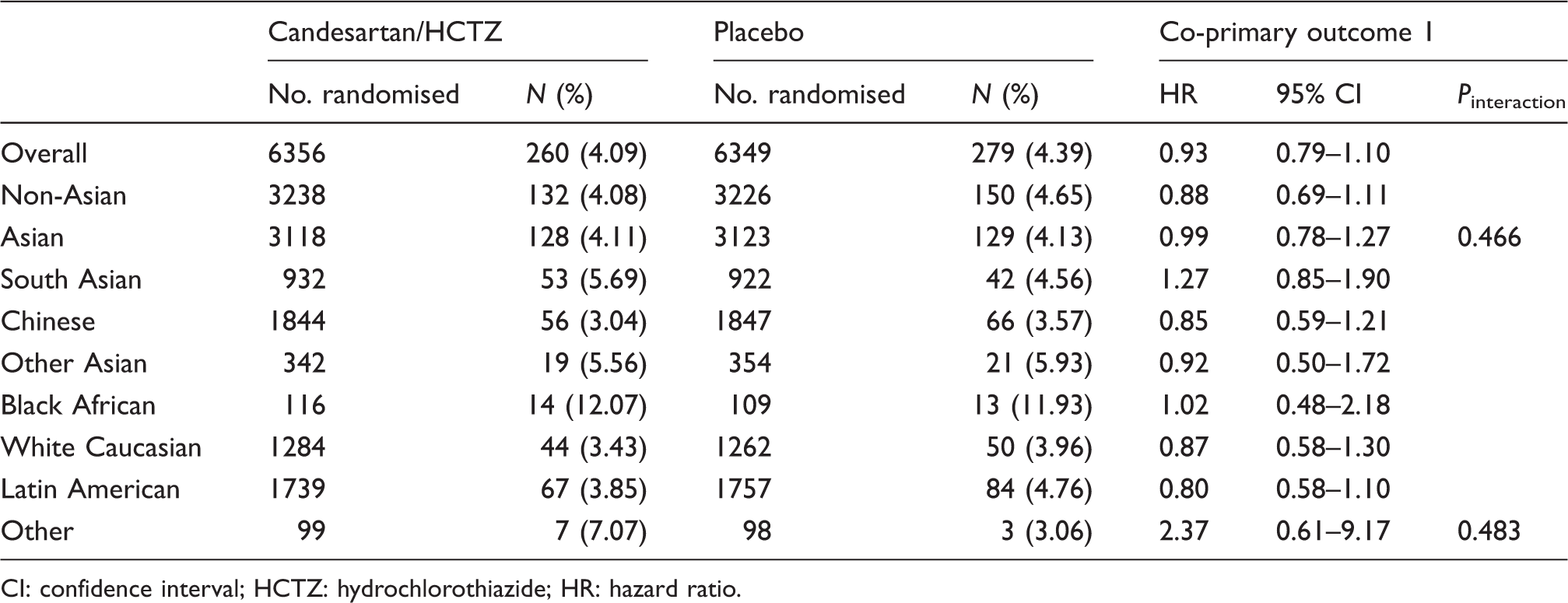
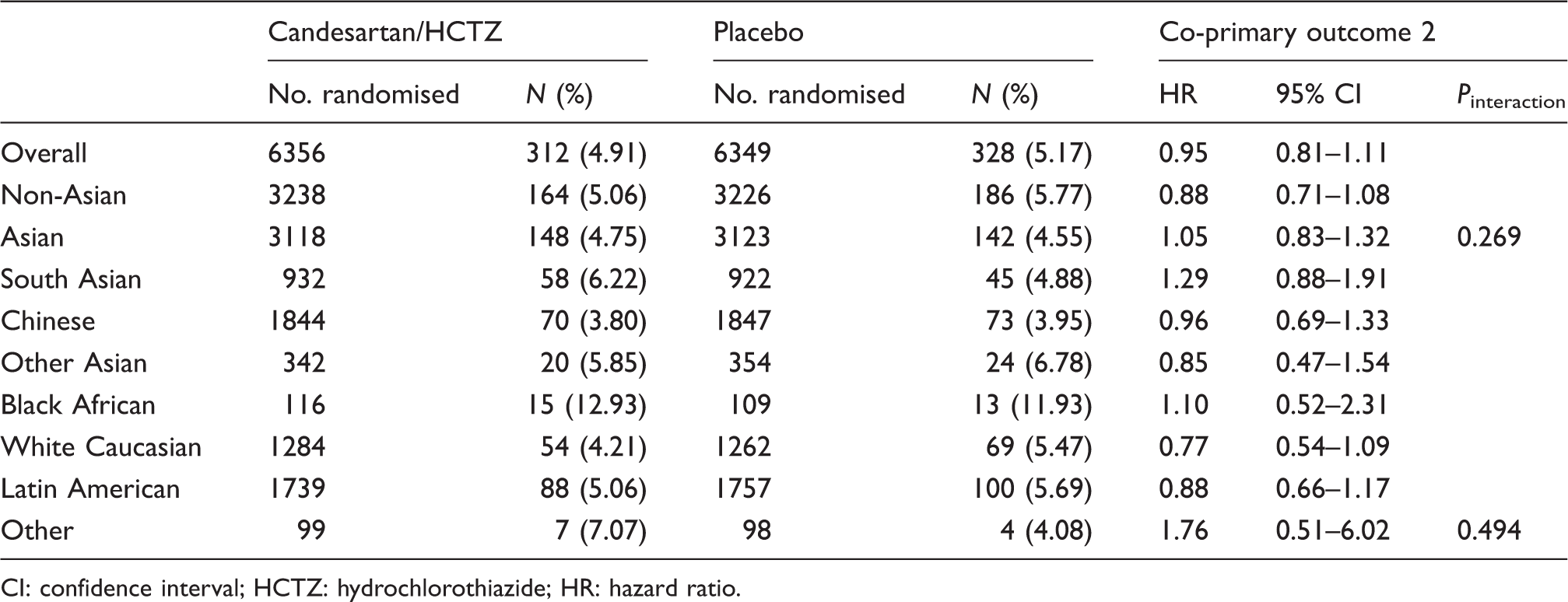
The placebo event rates were similar in Asians and non-Asians (Figure 2, Table 11). There were no significant differences between groups in treatment effects in either of the composite primary outcomes, cardiovascular death or MI. A nominally significant reduction in stroke was observed in Asians in the BP-lowering arm (HR 0.67, 95% confidence interval (CI) 0.45–0.99) but not in non-Asians (HR 1.06, 95% CI 0.65–1.73). However, the test for interaction was not significant (P = 0.146). In an analysis by tertiles of SBP, apparent harm was observed in the lowest tertile (SBP ≤131.5 mm), HR 2.72, 95% CI 1.36–5.44) among Asians which was not observed in non-Asians (HR 1.14, 95% CI 0.68–1.90). The P for interaction was significant at 0.0408 (Table 12). Despite the lower reduction in BP in Chinese, the impact on clinical events was similar in Chinese compared with others (Tables 13 and 14).
Kaplan–Meir curves for co-primary outcome 2, stroke and myocardial infarction for blood pressure lowering in Asians and non-Asians. Clinical outcomes. BP: blood pressure; CI: confidence interval; CV: cardiovascular; HCTZ: hydrochlorothiazide; HR: hazard ratio; MI: myocardial infarction. Co-primary outcome 2 by tertiles of baseline systolic blood pressure. CI: confidence interval; CV: cardiovascular; HCTZ: hydrochlorothiazide; HF: heart failure; HR: hazard ratio; MI: myocardial infarction; SD: standard deviation. Co-primary outcome 1 by ethnicity. CI: confidence interval; HCTZ: hydrochlorothiazide; HR: hazard ratio. Co-primary outcome 2 by ethnicity. CI: confidence interval; HCTZ: hydrochlorothiazide; HR: hazard ratio.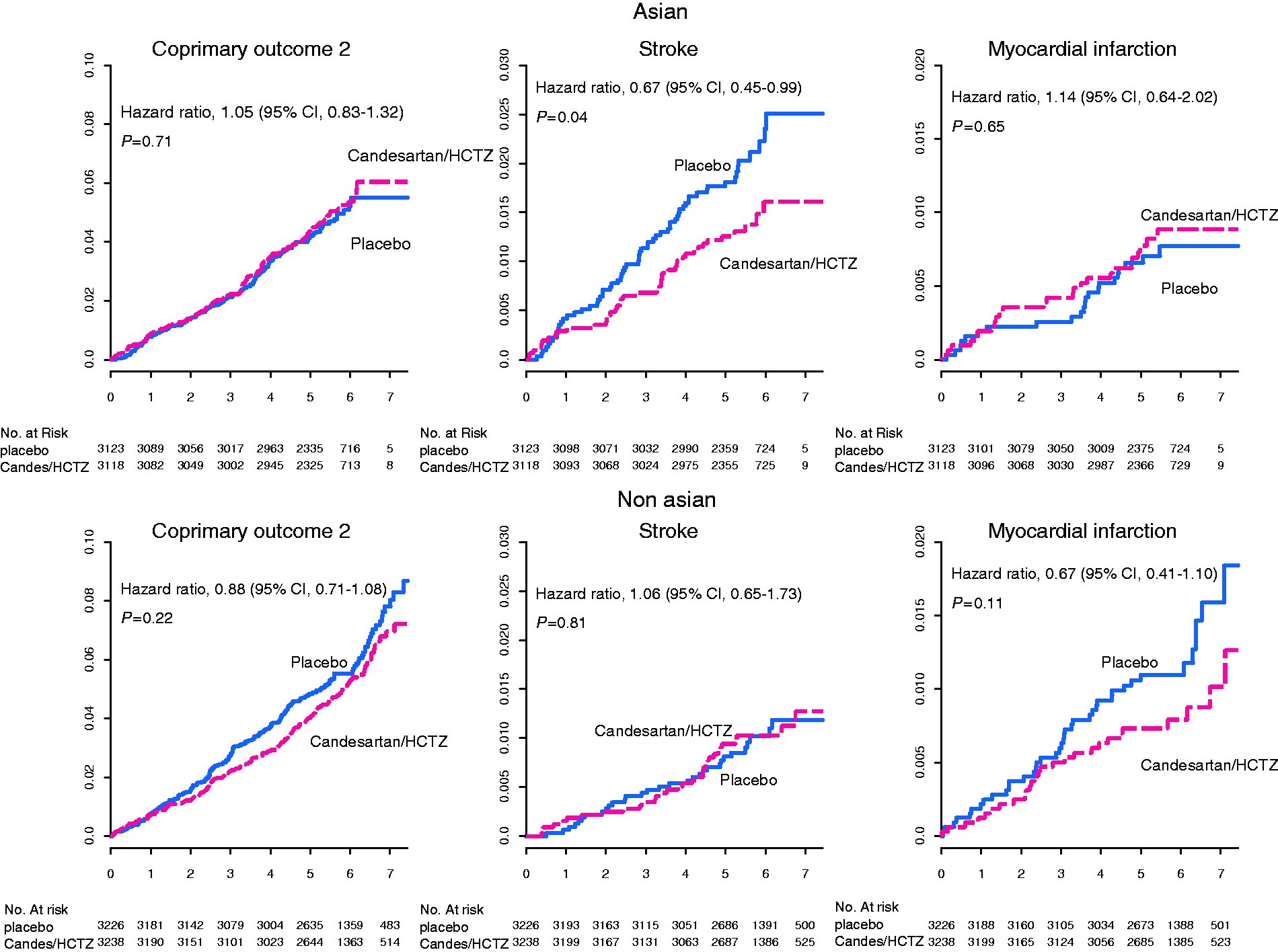
Cholesterol lowering
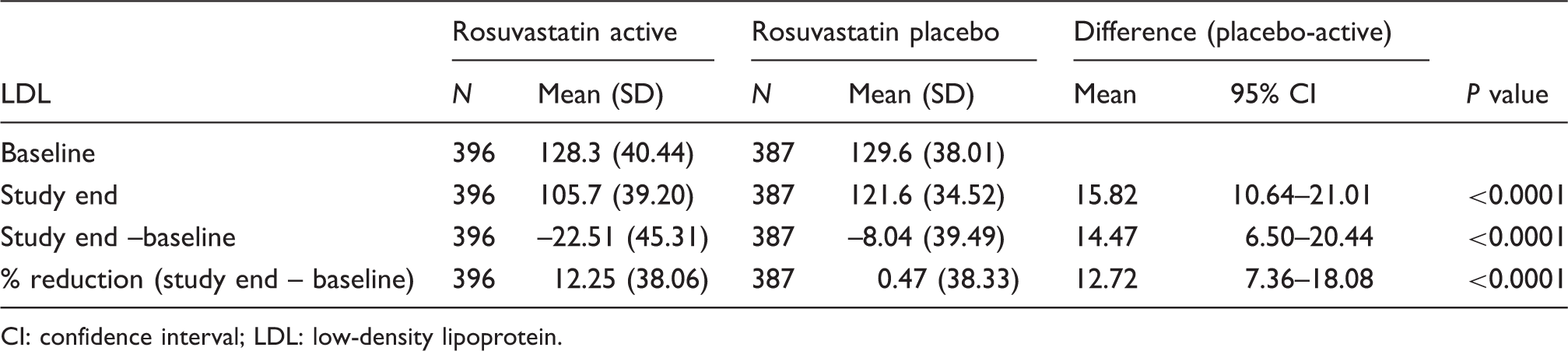
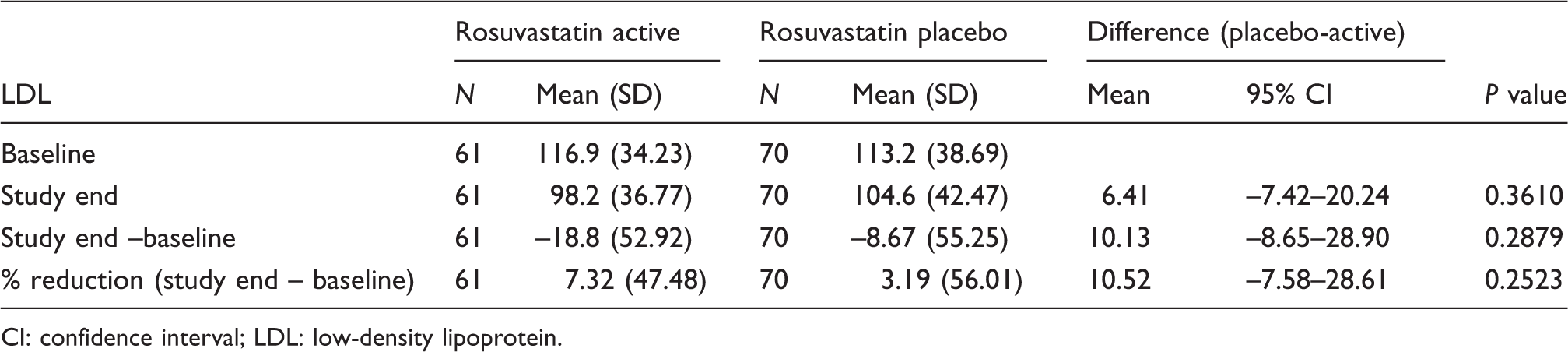
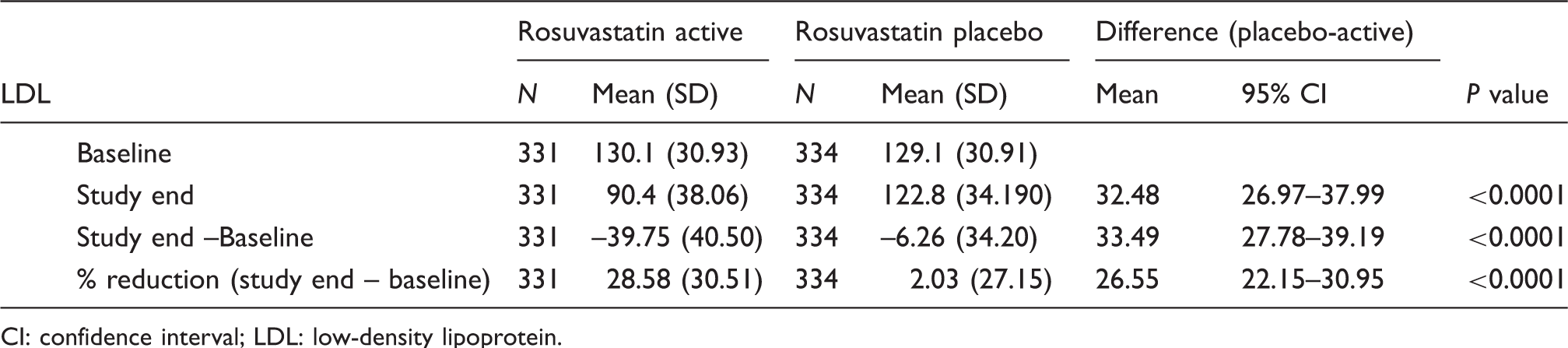
Rosuvastatin lowered LDL-cholesterol significantly in both non-Asians and Asians but the reduction was less in Asians than in non-Asians (0.49 mmol/L (19.1 mg/dL) vs. 0.95 mmol/L (36.7 mg/dL), respectively, Pinteraction < 0.0004, Table 7 and Figure 3). This reduced effect was observed in both Chinese and non-Chinese Asians although the number of evaluable samples in the latter was small (Tables 15, 16 and 17). There was a significant reduction in triglycerides in non-Asians which was not seen in Asians (–0.29 mmol/L (−25.6 mg/dL) non-Asians vs. –0.02 mmol/L (−2.14 mg/dL) Asians, respectively, Pinteraction = 0.0096). Rosuvastatin lowered high sensitivity C-reactive protein in non-Asians and Asians to the same extent (–4.67 nmol/L (–0.49 mg/L) and –5.05 nmol/L (−0.53 mg/L), respectively).
Levels of low-density lipoprotein cholesterol, apo-lipoprotein B and C-reactive protein by rosuvastatin and placebo in Asians and non-Asians. LDL-cholesterol changes from baseline to study end rosuvastatin versus placebo Chinese. CI: confidence interval; LDL: low-density lipoprotein. LDL-cholesterol changes from baseline to study end rosuvastatin versus placebo non-Chinese Asians. CI: confidence interval; LDL: low-density lipoprotein. LDL-cholesterol changes from baseline to study end rosuvastatin versus placebo non-Asians. CI: confidence interval; LDL: low-density lipoprotein.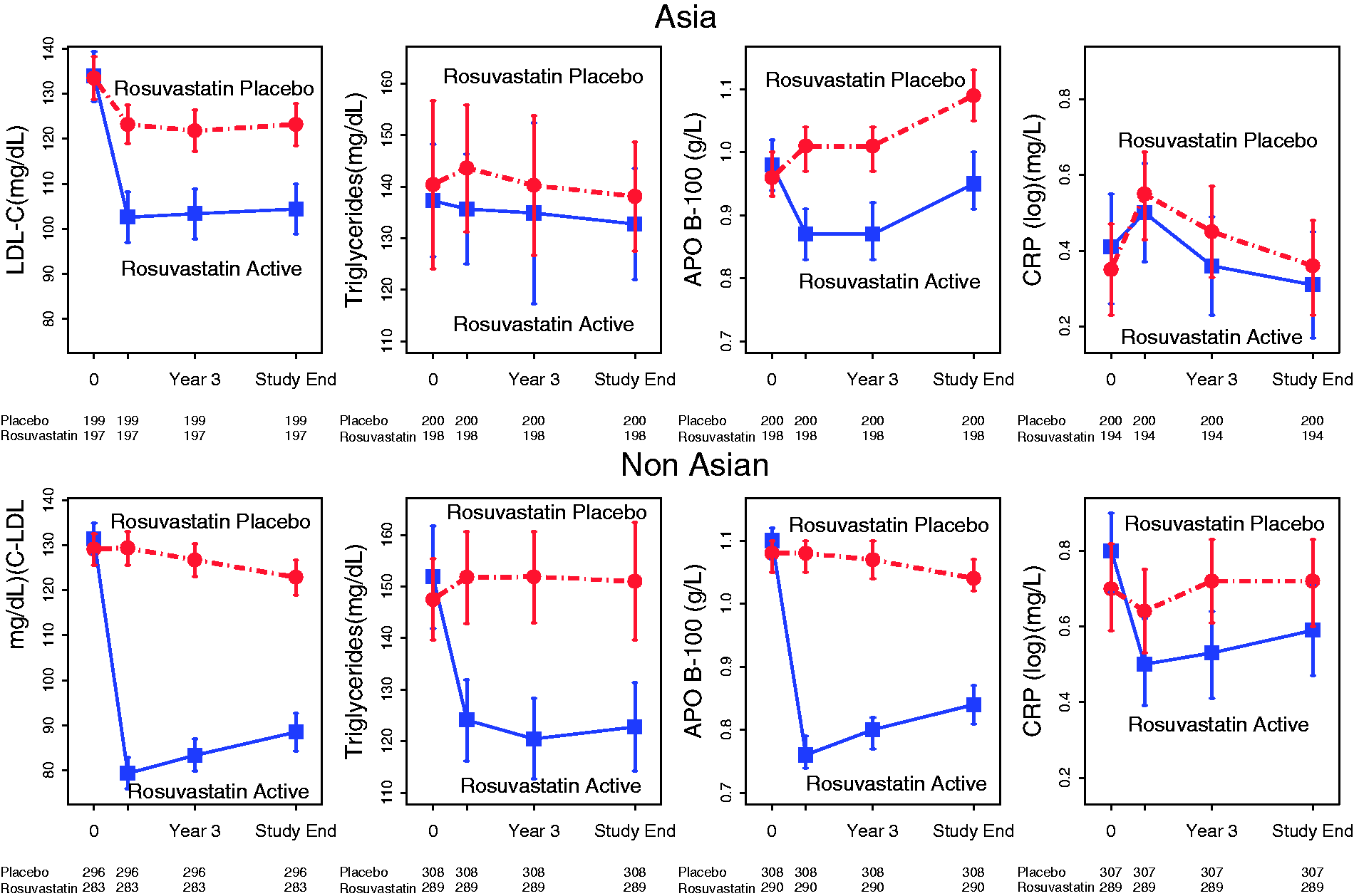
Among Asians there was a significant 21% and 23% reduction in co-primary outcomes 1 and 2, respectively (Table 11 and Figure 4). This was similar to reductions seen in non-Asians (26% reduction for both primary outcomes). Both Asians and non-Asians had a significant reduction in stroke – by 34% and by 23%, respectively (Pinteraction = 0.637). A significant 55% reduction in MI was seen only in non-Asians (Pinteraction = 0.033) but not in Asians.
Kaplan–Meir curves for co-primary outcome 2, stroke and myocardial infarction for cholesterol lowering in Asians and non-Asians.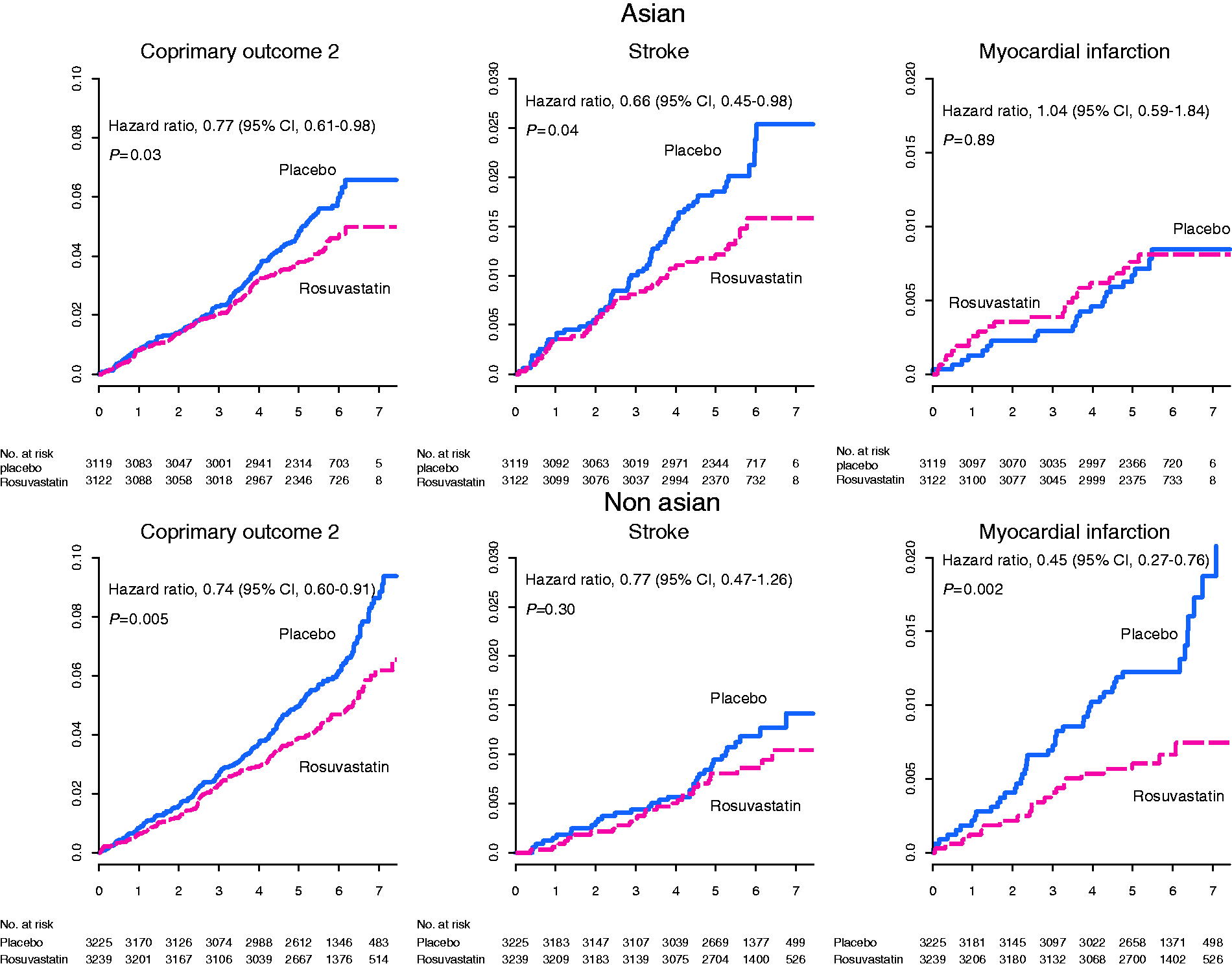
Combined BP and cholesterol lowering
Asians and non-Asians receiving both active BP and cholesterol-lowering medication had similar and significant reductions in CVD events compared with those receiving double placebo (Table 11 and Figure 5).
Kaplan–Meir curves for co-primary outcome 2, stroke and myocardial infarction for combined cholesterol and blood pressure lowering in Asians and non-Asians.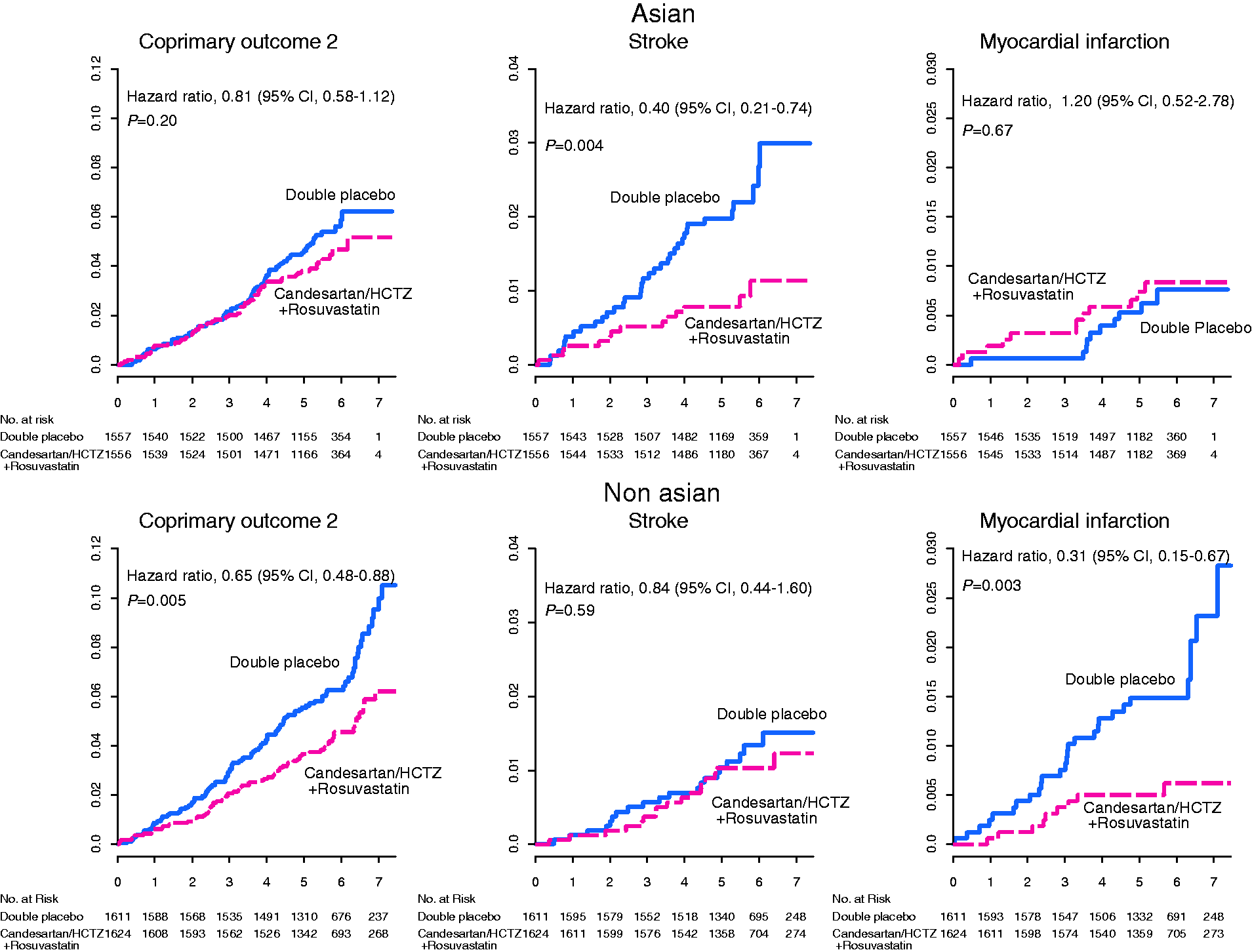
Safety
Permanent discontinuation of medication and adverse effects.
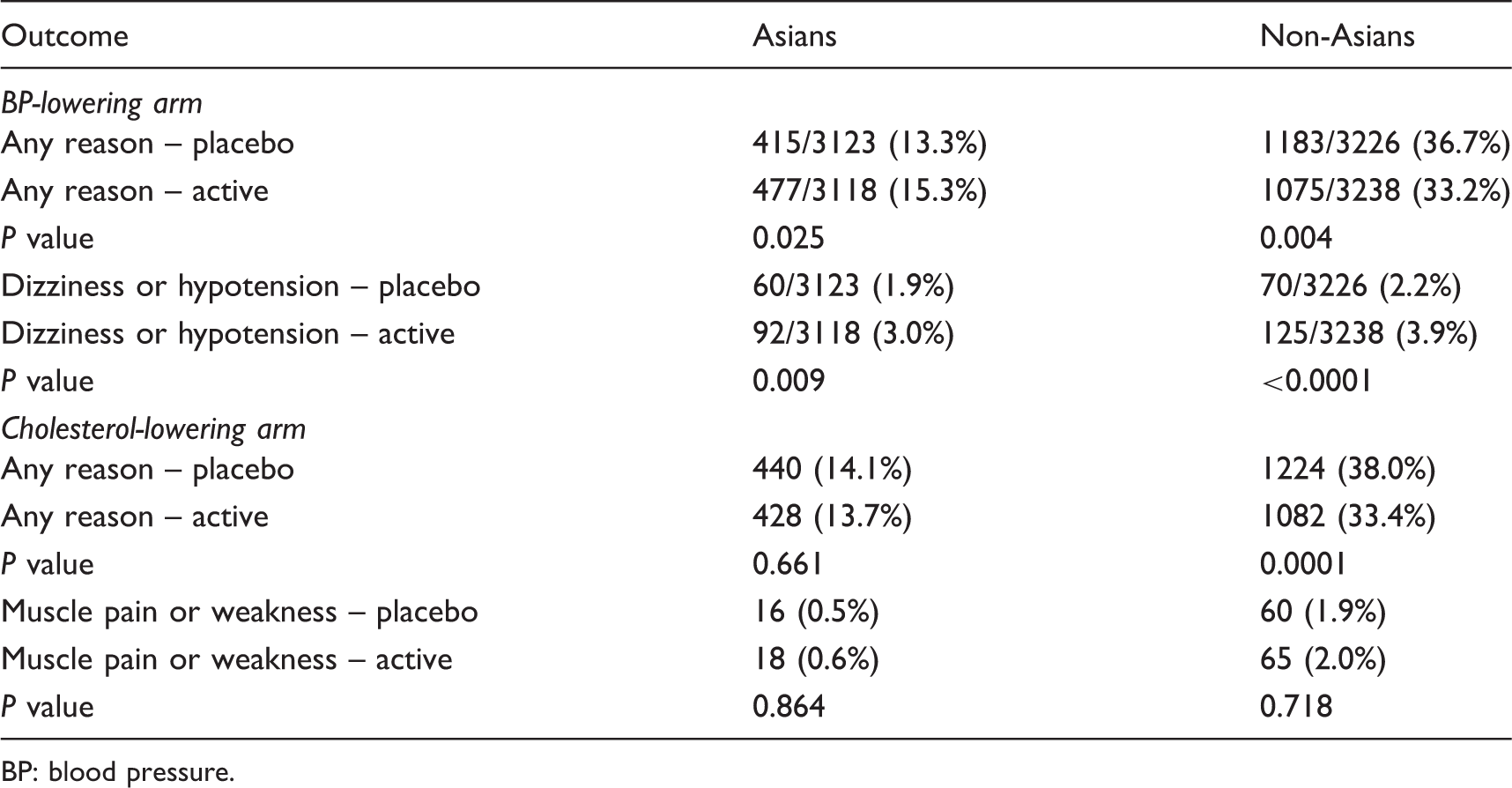
BP: blood pressure.
Muscle-related symptoms leading to permanent discontinuation of rosuvastatin were similar between the active and placebo groups among Asians and non-Asians (Table 18). However, temporary discontinuation for muscle-related symptoms was more frequent with rosuvastatin in both Asians (1.0% rosuvastatin vs. 0.5% placebo, P = 0.035) and non-Asians (1.7% rosuvastatin vs. 0.8% placebo, P = 0.002). Rhabdomyolysis or myopathy was uncommon in both Asians (zero rosuvastatin, one placebo) and non-Asians (two rosuvastatin, zero placebo).
A significant 33% excess in new diabetes was noted with rosuvastatin in non-Asians (4.70% rosuvastatin vs. 3.52% placebo, P = 0.025), but not in Asians (3.02% rosuvastatin vs. 4.04% placebo, Pinteraction = 0.002). The main study reported a higher incidence of cataract surgery in participants on active rosuvastatin. This was not observed in Asians – 1.66% with rosuvastatin versus 1.49% with placebo. In contrast, there was an increase in cataract surgery among non-Asians – 5.02% rosuvastatin versus 3.79% placebo, P = 0.02. However, the test for interaction was not significant (P = 0.4291).
Discussion
Overall, the impact of both the trial interventions (BP lowering and lipid lowering) on clinical events were similar in Asians and non-Asians. There was a neutral effect with BP lowering but a significant reduction of both primary outcomes of similar magnitude with lowering of LDL-cholesterol. The study medications were well tolerated by both groups, with no excess in muscle-related symptoms in Asians with rosuvastatin. An excess of diabetes and cataract surgery was seen only in non-Asians, but not in Asians. Therefore, contrary to common belief, in HOPE 3, rosuvastatin 10 mg daily was at least as well tolerated in Asians as in non-Asians.
Despite better adherence to medication the degree of BP and LDL lowering was less in Asians, with both interventions compared with placebo. SBP was lowered by 4.24 mmHg in Asians compared with 7.7 mmHg in non-Asians. The reduction in SBP among non-Chinese Asians was similar to that seen in non-Asians (−7.28 mmHg), but the reduction in SBP among Chinese was substantially smaller (–2.15 mmHg). Given that adherence to randomised treatments was higher among Asians (including Chinese participants) compared with non-Asians and the use of non-study medications for lowering BP was similar in Asians and non-Asians, we do not have a coherent explanation for the lesser effect of candesartan plus hydrochlorothiazide in lowering BP among Chinese. While neither group showed significant reductions overall in primary outcomes with BP lowering, Asians in the active BP-lowering arm did have a significant 33% reduction in stroke, which was not evident in non-Asians, although the test for interaction was not nominally significant. This could be due to the higher incidence of stroke among Asians (2.02% in Asians compared with 0.96% in non-Asians in the placebo arm) or the higher initial BP in Asians. The difference in impact on strokes between Asians and non-Asians could also be due to chance. A prespecified analysis of the benefits of BP lowering by thirds of SBP in the main HOPE trial showed a neutral outcome in subjects in the lowest third of SBP. 8 In the present analysis, Asian subjects in the lowest third of SBP (mean SBP 122.2 mmHg) showed apparent harm, while in non-Asians there was a neutral effect (Table 12). This could suggest that in Asians, BP lowering in those with SBP below 130 mmHg should be done with caution, if at all.
The impact of adherence or otherwise to a healthy lifestyle has not been addressed in this analysis. Such an analysis in the entire HOPE 3 study population 12 assessed the effect of drug interactions in subgroups by adherence to two or more of four healthy lifestyle factors – (non-smoking (never smokers and those who had quit more than a year earlier) versus current smoking; moderate or vigorous physical activities versus less activity; optimal waist/hip ratio (≤0.89 for men and ≤0.84 for women) versus a higher ratio and a healthy versus unhealthy diet, assessed using a 9-point Mediterranean diet score) with those with less than two. This analysis reported that those who had two or more of these factors had overall lower rates of cardiovascular events (HR 0.85, 95% CI 0.73–1.00). Rosuvastatin was beneficial to both groups – two or more healthy lifestyle factors (HR 0.85, 95% CI 0.62–0.90) and less than two healthy lifestyle factors (HR 0.79, 95% CI 0.61–1.01). On the other hand, BP reduction with candesartan/hydrochlorothiazide reduced outcomes only in those with less healthy lifestyles – two or more healthy lifestyle factors (HR 1.00, 95% CI 0.83–1.20) and less than two healthy lifestyle factors (HR 0.78, 95% CI 0.61–1.00). This could be due to the lower event rate and lower baseline BP in those with healthier lifestyles.
Previous reports have suggested that Asians have greater cholesterol lowering and higher plasma exposure to rosuvastatin in pharmacokinetic studies compared with other ethnic groups.11,13,14 By contrast, in HOPE 3 while there was a significant reduction in LDL-cholesterol in both Asians and non-Asians, the magnitude of reduction in LDL-cholesterol was less in the Asians despite better adherence to medication. It should be noted that while baseline cholesterol measurements were done in all subjects, repeat measurement was done only in a sample of the population which was selected randomly by the project office (Table 1). This approach minimises the potential for biases in the selection of participants in whom lipid measurements were obtained. Despite the apparent lesser degree of reduction in LDL-cholesterol, the reductions in primary outcome events were surprisingly similar in Asians and non-Asians. In the cholesterol-lowering arm, there was a significant 34% and 23% reduction in stroke among Asians and non-Asians, respectively. While non-Asians showed a significant 55% reduction in MI, this was not apparent in Asians. These differences may be due to chance because of the small number of events in this subgroup analysis or may suggest different benefits for MI versus stroke in Asians compared with non-Asians. This should be systematically examined across all trials comparing the effects of BP lowering and cholesterol lowering in Asians and non-Asians.
Rosuvastatin 10 mg was well tolerated, with no difference between the active and placebo arms either in Asians or non-Asians in permanent discontinuation due to muscle pain or weakness (Table 18). Only three cases of rhabdomyolysis/myopathy were reported in the entire trial. There was no increase in serious muscle-related symptoms among Asians, including 3691Chinese. Pharmacokinetic studies have reported higher plasma levels of statins in Asians,13,14 and although no specific increase in muscle toxicity has been reported there has been an impression that lower doses of statins should be used in Asians. 11 In the HPS-THRIVE study 15 of laropripant and niacin versus placebo on a background treatment of simvastatin 40 mg in 25,672 patients including 10,932 from China, the incidence of any myopathy in the control arm was low but still higher among the Chinese than among Europeans – 0.13%/year in China versus 0.04%/year in Europe, P = 0.001. Most reports of myopathy are associated with higher doses of simvastatin, and possibly the moderate dose of rosuvastatin we used avoided any excess of adverse effects in both Asians and non-Asians. There have been reports of increased rates of new-onset diabetes mellitus associated with the use of statins. In the JUPITER trial 16 a significant 25% increase in new-onset diabetes mellitus was reported in the statin arm among 17,802 randomly assigned patients. However, 20 mg of rosuvastatin was used in JUPITER compared with 10 mg in HOPE 3 and few Asians were included. In HOPE 3 we did not observe any increase in new diabetes mellitus in Asians, but there was a 33% excess in non-Asians (which is consistent with JUPITER). The reasons for this are unclear and could include differences in BMI or genetic differences in the 3-hydroxy-3-methylglutaryl coenzyme A (HMGCoA) reductase enzyme (which has been linked to diabetes). 17 Examining the effects of specific statins at comparable doses on LDL-cholesterol, triglycerides and glucose levels in other studies in Asians and non-Asians is necessary to inform whether the differences we observed in HOPE 3 are real or due to chance.
Conclusion
The results of HOPE 3 indicate that the use of a fixed dose of rosuvastatin 10 mg daily was effective and safe in the primary prevention of CVD in individuals aged over 55 years (women over 60 years) at intermediate risk (Figure 4). Those with SBP over 140 mmHg had incremental benefit with additional BP lowering with fixed dose candesartan 16 mg/hydrochlorothiazide 12.5 mg. With over 6000 Asian participants, the present analysis shows reliably that Asians had similar benefits and at least similar safety with statins and BP lowering compared with non-Asians. However, the lesser degree of BP lowering seen with candesartan plus hydrochlorothiazide among Chinese suggests that future studies should be large enough to explore the consistency of effects in Asians (who constitute a very large part of the world’s population) and in other ethnic groups.
Strategies to address the problem of the surging CVD burden and its risk factors successfully have been hampered by factors such as affordability, access and compliance. 18 The benefit seen in HOPE 3 was achieved using fixed doses of medications without frequent visits for BP, cholesterol measurements or safety blood tests, thereby potentially saving significant costs to the healthcare system and making this strategy easily applicable in various countries and healthcare systems. Such a strategy facilitates large-scale community level interventions with statins and BP-lowering drugs at low or medium doses, to prevent CVD using trained non-physician health workers with a clear protocol and under adequate supervision. Such a model is now being tested in the HOPE 4 trial in Malaysia and in Colombia.18,19 The success of such trials could open the way to the development of polypills for a subset of people such as those with diabetes mellitus. 20
Author contribution
PP and SY drafted and finalised the paper. SY, JB and EL conceptualised and designed the HOPE 3 study. HJ, PP and SY analysed the data for this paper. PP, AD, JZ and LL contributed to the acquisition of data. AD, JZ, LL, DK, JB and EL critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring accuracy and integrity.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The HOPE 3 Study was supported by a grant (IR2-91038) from the Canadian Institutes of Health Research and by an unrestricted grant from AstraZeneca. The authors received no additional financial support for the authorship, analysis or publication of this paper.
Supplemental Material
Supplemental material for Impact of blood pressure lowering, cholesterol lowering and their combination in Asians and non-Asians in those without cardiovascular disease: an analysis of the HOPE 3 study
Supplemental Material for Impact of blood pressure lowering, cholesterol lowering and their combination in Asians and non-Asians in those without cardiovascular disease: an analysis of the HOPE 3 study by Prem Pais, Hyejung Jung, Antonio Dans, Jun Zhu, Lisheng Liu, Deepak Kamath, Jackie Bosch, Eva Lonn and Salim Yusuf in European Journal of Preventive Cardiology
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.