
Abstract

Introduction
Prevention, both primary and secondary, was in the spotlight of this years American Heart Association (AHA) Scientific Sessions held in freezing Chicago in early November. Two late-breaking clinical trials sessions were dedicated to the field of prevention, covering several fields including inflammation reduction as a therapeutic means in atherosclerotic cardiovascular disease (ASCVD) prevention, the presentation of the third sodium-dependent glucose transporter-2 (SGLT-2) inhibitor phase III outcome trial and most importantly, the vast field of lipidology, from low-density lipoprotein (LDL)-lowering agents, somewhat surprising results in the omega-3 field to the new North American guideline on the management of blood cholesterol.
Lipid lowering: new guidelines, VITAL, REDUCE-IT, alirocumab cost effectiveness analysis, EWTOPIA-75 and AKCEA-APO(a)-LRX
After the heavily discussed, criticised and praised 2013 North American lipid guidelines, which largely abandoned LDL-cholesterol (LDL-C) targets and introduced a score for 10-year ASCVD risk guiding initiation of lipid-lowering therapy for primary prevention, the new guidelines were awaited eagerly. The 2018 American Heart Association / American College of Cardiology (AHA/ACC) guideline on the management of blood cholesterol brought back target values and now gives caregivers and patients a little more space and flexibility regarding initiation of primary prevention statin treatment according to ASCVD risk. 1 For secondary prevention, the guidelines differentiate between patients at very high risk – those are patients with several ASCVD events or one major event and multiple high risk conditions like hypertension, smoking, diabetes, chronic kidney disease or age > 65 years – and patients with stable ASCVD. For the latter condition < 75 years of age, high-intensity statins are recommended and if LDL-C < 70 mg/dl cannot be achieved, ezetimibe should be added. In those patients considered at very high risk that miss the LDL-C threshold (<70 mg/dl) with high-intensity statin treatment, first ezetimibe should be added and if the goal is still missed, a proprotein convertase subtilisin/kexin-9 (PCSK-9) inhibitor should be considered.
Overview of some of the important prevention studies presented at AHA Scientific Sessions 2018.
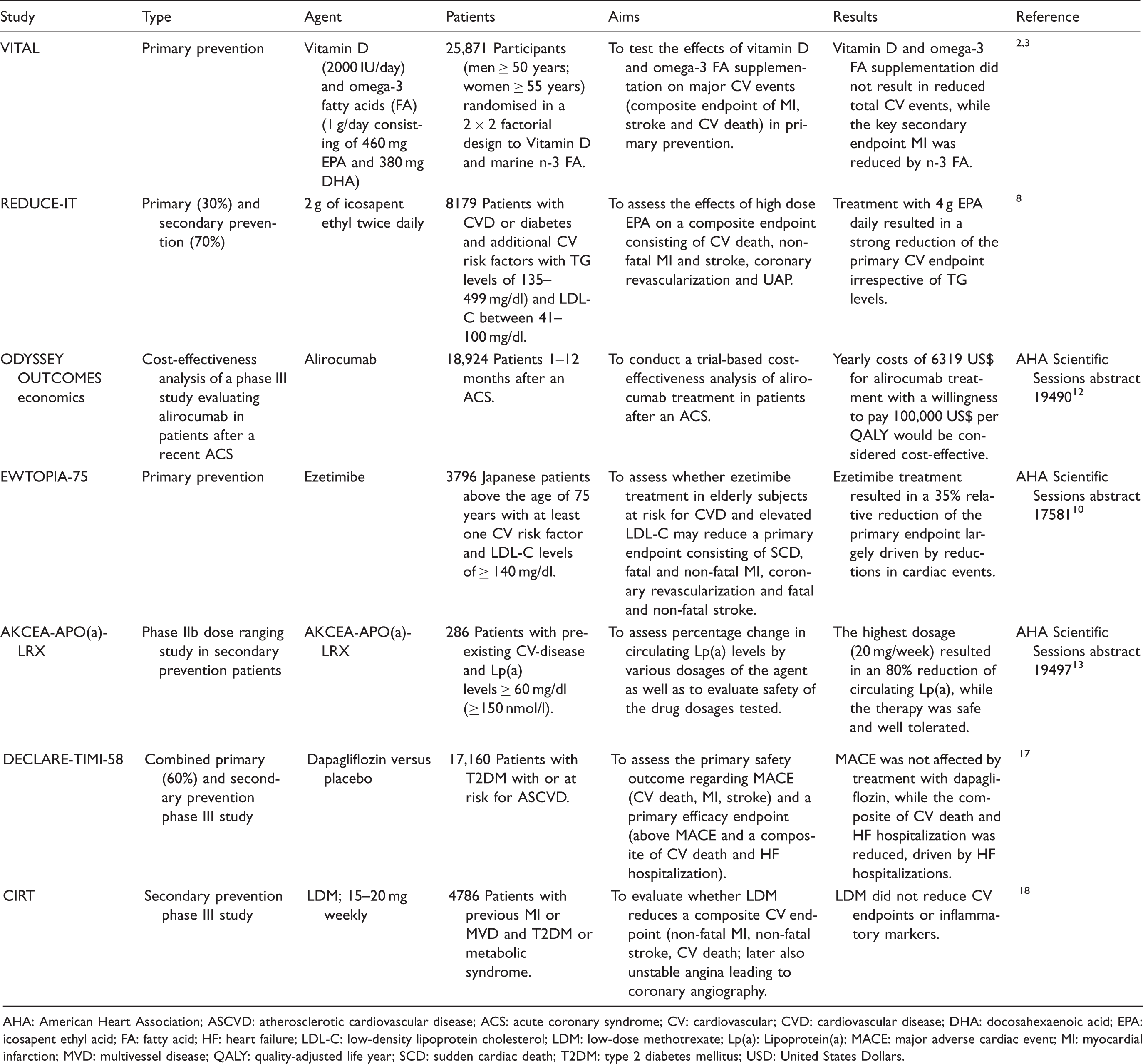
AHA: American Heart Association; ASCVD: atherosclerotic cardiovascular disease; ACS: acute coronary syndrome; CV: cardiovascular; CVD: cardiovascular disease; DHA: docosahexaenoic acid; EPA: icosapent ethyl acid; FA: fatty acid; HF: heart failure; LDL-C: low-density lipoprotein cholesterol; LDM: low-dose methotrexate; Lp(a): Lipoprotein(a); MACE: major adverse cardiac event; MI: myocardial infarction; MVD: multivessel disease; QALY: quality-adjusted life year; SCD: sudden cardiac death; T2DM: type 2 diabetes mellitus; USD: United States Dollars.
The first of the two late-breaking clinical trial sessions covering prevention started with two studies evaluating omega-3 fatty acids in primary and secondary prevention. In VITAL, an NIH-sponsored primary prevention study including more than 25,000 participants (men > 50 years; women > 55 years), the effects of vitamin D3 and marine omega-3 fatty acid supplementation on a composite endpoint of myocardial infarction (MI), stroke or death from cardiovascular disease (CVD) were evaluated using a two-by-two factorial design. Interestingly, neither vitamin D3 (at a dose of 2000 IU per day) nor omega-3 fatty acids (1 g per day as a fish oil capsule containing 840 mg of n-3 fatty acids, including 460 mg of icosapent ethyl acid (EPA) and 380 mg of docosahexaenoic acid (DHA)) prevented major CV events or cancer compared to placebo. It has to be noted that incidence of MI, a key secondary endpoint, was significantly reduced using n-3 fatty acids, particularly in African-American participants.2,3
Those findings are in line with findings from other trials, testing 1 g of n-3 fatty acids including EPA and DHA for CVD reduction, such as ASCEND, ORIGIN and the ALPHA OMEGA study.4–6However, the JELIS study which randomised 18,000 Japanese participants with high total cholesterol (>250 mg/dl) to either statin therapy alone or statin therapy and 2 g EPA for both primary and secondary prevention, showed a 19% reduction in incident coronary events. 7 Those beneficial effects for high-dose EPA shown in 2007 were probably the inspiration for the REDUCE-IT trial, the second late-breaking omega-3 fatty acids trial, which randomised more than 8000 patients with established CVD (70%) or diabetes and additional risk factors as well as fasting triglycerides (TGs) between 135 and 499 mg/dL to either 4 g of EPA daily, a n-3 fatty acid or placebo (mineral oil). 8 After nearly five years of follow-up, treatment with EPA, which was based on much higher doses than most trials so far besides JELIS, strongly reduced the primary endpoint (CV death, non-fatal MI, non-fatal stroke, coronary revascularization or unstable angina) by an impressive 25% with a number needed to treat (NNT) of 21. The key secondary endpoint consisting of CV death, non-fatal MI and non-fatal stroke, was relatively reduced by 26%. Of interest also, CV death and sudden cardiac death (SCD) rates went down while bleeding was increased numerically and hospitalization for atrial fibrillation or flutter was significantly increased. The study was strongly praised but also criticised for using mineral oil as a placebo, and the fact that high sensitive C-reactive protein (hs-CRP) and LDL-C levels increased in the placebo group. Still, most participants in the discussion agreed that this alone could not explain these dramatically positive results. The exact mechanisms remain unclear, as the beneficial effects were independent from starting TG levels as well as independent from reaching desirable levels of < 150 mg/dl or not. The prevention world now looks at the STRENGTH trial, evaluating another high dose n-3 fatty acid formula using a different placebo treatment. 9
Further studies from the lipid field include EWTOPIA-75, that tested ezetimibe and diet counselling in > 3000 Japanese individuals > 75 years of age with an LDL-C of > 140 mg/dl with one or more CVD risk factors but without a history of CAD against diet counselling alone. 10 Ezetimibe treatment lowered mean LDL-C levels from 160 mg/dl to 126 mg/dl and the primary combined endpoint of SCD, MI, PCI or CABG was reduced by 34%, which was largely driven by reductions in cardiac events. These surprisingly strong and pleasant results probably need validation in a non-Japanese cohort before being ready for prime-time.
A cost-effectiveness analysis of the PCSK9-inhibitor alirocumab using data from the phase III outcome study ODYSSEY outcomes, 11 presented at AHA18, suggested that alirocumab treatment may be cost-effective at yearly costs of US$6319 with a willingness to pay US$100,000 per quality-adjusted life year (QALY). 12 High costs are the main reason in many countries for not prescribing these innovative treatments, especially within the USA where PCSK9-inhibitors have been sold at much higher prices so far.
A phase IIb dose-finding study evaluating a novel antisense agent lowering Lp(a) levels was chosen as a ‘late-breaker’ due to its potential future significance. Sotirios Tsimikas from San Diego presented the study which evaluated five different dosing regimens of AKCEA-APO(a)-LRX in comparison with placebo in more than 200 patients with established CVD and Lp(a) levels of 60 mg/dl (approximately 150 nmol/l) and more. 13 They showed a dose-dependent reduction with the strongest effects, an 80% reduction in Lp(a) levels, with the highest dose tested (20 mg/week). A special focus was provided on adverse events, 25% of patients reported injection-site erythema, otherwise the therapy was safe and well tolerated. Currently the CV world is awaiting the initiation of a phase III study with this agent to prove whether Lp(a)-reduction will lead to reduced CV events.
Diabetes: DECLARE-TIMI 58
After concerns regarding the CV safety of older diabetes drugs, the FDA demanded CV outcome trials for newer drugs for type 2 diabetes. Interestingly, and surprisingly for some, so far all of the eight substances tested have proven to be safe, and three of them have actually shown a benefit. This included the injectable glucagon-like protein-1 (GLP-1) agonist liraglutide, tested in the LEADER trial, as well as the novel class of SGLT-2 inhibitors including empagliflozin in the EMPA-REG OUTCOMES study and canagliflozin in the CANVAS study.14–16At the AHA meeting this year, the third SGLT-2 inhibitor outcome study, DECLARE-TIMI-58, was presented. 17 In total > 17,000 patients were enrolled, of whom approximately 60% had no established ASCVD but were at risk due to the presence of multiple risk factors and were randomised to dapagliflozin or placebo on top of standard therapy. Dapagliflozin treatment did not result in higher or lower major adverse cardiac event (MACE) rates, while the composite endpoint of CV death or hospitalization for heart failure (HF) was significantly reduced, a finding that was driven by lower HF hospitalization. Of interest, the benefit on HF hospitalizations was similar in the primary and secondary prevention group, while for MACEs, a trend towards lower MACE rates was seen in patients with existing ASCVD while no effect was seen in those without. Regarding adverse events, there was an increase in diabetic ketoacidosis as well as genital infections, both known class adverse effects, while lower limb amputations were not increased, as surprisingly shown in the CANVAS study. Taken together, we now have robust proof of a class effect of SGLT-2 inhibitors regarding heart failure outcomes, while benefits regarding MACEs may only be achieved in patients with established ASCVD.
Inflammation: CIRT
After the excitement of last year around the CANTOS trial, the first phase III outcome trial that showed that an interleukin-1 b antibody could reduce CV events, inflammation reduction as a possible target for ASCVD risk reduction, finally arrived at a clinical stage after three decades of accumulating evidence regarding the central role of inflammation in atherogenesis.18,19The CIRT trial, a National Heart, Lung and Blood Institute (NHLBI)-supported study, evaluated low-dose methotrexate (LDM) as an add-on therapy to standard care in stable CAD patients with a history of MI or multivessel disease (MVD) who in addition had either type 2 diabetes or a metabolic syndrome. 20 LDM was chosen as a cheap, effective, widely used treatment for chronic inflammatory conditions such as rheumatoid arthritis. However, the trial was stopped early after a median follow-up of 2.3 years including more than 4500 patients. Treatment with LDM did not result in a reduction of CRP interleukin-6 or interleukin-1β and failed to show any reduction in CV events, while elevations in liver enzymes, reductions in leukocyte counts and haematocrit levels as well as a higher incidence of non-basal-cell skin cancers were observed. In contrast to the CANTOS study, patients were not recruited according to elevated hs-CRP levels, and in fact showed median levels of 1.5 mg/l, as compared to the inclusion requisite of > 2 mg/l for the CANTOS trial. The low baseline inflammatory activity in the patients studied, together with the failure in achieving a reduction in key inflammatory circulating markers, may explain the negative results of this study. Further studies should probably again recruit patients with evidence of ongoing inflammation and use testing agents that have shown the ability to reduce inflammation in a phase II study. The negative results of CIRT should definitely not discourage further research in inflammation reduction as a therapeutic strategy in the secondary prevention of ASCVD.
Conclusions
This years’ AHA Scientific Sessions had a strong focus on CVD prevention, both in the primary and secondary prevention field, with exciting findings regarding lipid-lowering therapy, a focus on the high-risk patient within the new North American guidelines including patients with possible familial hypercholesterolaemia and those with repeated ASCVD events, more evidence for SGLT-2 inhibitors, as well as disappointing results for anti-inflammatory treatment, possibly caused by the not-ideal population and drug tested.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.