
Abstract
Aim
Cardiac rehabilitation promotes functional recovery after cardiac events. Our study aimed at evaluating whether, compared to usual care, a home-based exercise programme with monthly reinforcement sessions adds long-term functional benefits to those obtained with cardiac rehabilitation in the elderly.
Methods
After a 4-week outpatient cardiac rehabilitation, 160 of 197 patients aged 75 years and older screened for eligibility with different indications for cardiac rehabilitation, were randomly assigned to a control (C) or an active treatment (T) group. During a 12-month follow-up, C patients received usual care, while T patients were prescribed a standardised set of home-based exercises with centre-based monthly reinforcements for the first 6 months. The main (peak oxygen consumption) and three secondary outcome measures (distance walked in 6 minutes, inferior limbs peak 90° Torque strength, health-related quality of life) were assessed at baseline, at random assignment and at 6 and 12-month follow-ups with the cardiopulmonary exercise test, 6-minute walking test, isokinetic dynamometer and the Short Form-36 questionnaire, respectively.
Results
Both C and T groups obtained a significant and similar improvement from baseline to the end of the 4-week cardiac rehabilitation programme in the three functional outcome measures. However, at univariable and age and gender-adjusted analysis of variance for repeated measures, changes from random assignment to 6 or 12-month follow-up in any outcome measure were similar in the C and T groups.
Conclusion
Results from this randomised study suggest that a home-based exercise programme with monthly reinforcements does not add any long-term functional benefit beyond those offered by a conventional, 4-week outpatient cardiac rehabilitation programme.
Trial registration
ClinicalTrial.gov Identifier: NCT00641134.
Introduction
Guidelines recommend cardiac rehabilitation (CR) as a routine component of the clinical management, and an essential measure in secondary prevention, for patients with coronary artery disease1–4 or chronic heart failure,5,6 defining its key elements and outcome measures. The strength (IA level) of such a recommendation is supported by numbers of randomised clinical trials, meta-analyses and observational studies, demonstrating that CR reduces cardiovascular morbidity/mortality 7 and improves exercise capacity, health-related quality of life and adherence to therapies8,9 in both middle-aged 10 and elderly patients.11,12 It is hypothesised that the long-term (4–10 years of follow-up)13,14 beneficial effects of CR, independent of age and type of diagnosis, result at least in part from patients' empowerment, which favours the control of risk factors through improved adherence to evidence-based treatments.15,16 Therefore, any effort should be put into maximising the participation in CR and planning tailored educational interventions, in a perspective of long-term comprehensive cardiac care. In this view, GOSPEL 17 was the first trial to demonstrate that multidimensional, continuously reinforced interventions up to 3 years after myocardial infarction may reduce some adverse outcomes. Unfortunately, this trial, like others,10,12,18–20 enrolled small proportions of older patients. In a previous randomised trial, 21 we found that the functional improvement from baseline to the end of a 2-month CR programme was similar across three age groups but, in patients older than 65 years and, most remarkably, in those older than 75 years, exercise capacity returned towards baseline after 6 and 12 months of follow-up. These observations generate the research hypothesis that continuously reinforced interventions, aimed at maintaining long-term the benefits achieved with CR, might be particularly useful in older patients.
Therefore, we conducted a prospective, randomised, single-centre trial (Cardiac Rehabilitation in Advanced aGE: EXercise TRaining and Active follow-up, CR-AGE EXTRA; ClinicalTrials.gov identifier: NCT00641134), to assess whether a home-based, 6-month exercise programme with monthly follow-up and exercise sessions, provides any functional advantage over usual care after a 4-week outpatient CR programme in patients older than 75 years.
Methods
The CR-AGE EXTRA trial has been approved by the local ethics committee and was conducted in accordance with the Declaration of Helsinki. We screened for eligibility all the consecutive patients aged 75 years and older referred to the CR unit of Careggi University Hospital over a 46-month period, after an acute coronary syndrome or coronary artery bypass grafting (CABG) and/or cardiac valve surgery. In addi-tion to the usual cardiological assessment, including recording of medical history and drug therapy, 12-lead ECG, echocardiogram and cardiopulmonary exercise test, patients underwent comprehensive geriatric assessment (CGA), to evaluate their chronic comorbidity burden as well as their functional (including physical exercise habits), psycho-emotional and socioeconomic profile. Because of the prescription of home-based exercise in a study arm (see below), moderate to severe cognitive impairment (Mini Mental State Examination (MMSE) score < 18), 22 disability in two or more basic activities of daily living (BADL), 23 severe lower limb musculoskeletal disease or other contraindication to exercise, expected survival less than 6 months, heart failure 24 or left ventricular ejection fraction of 35% or less, were all taken as exclusion criteria.
Study design and patient allocation
Over the study period, 197 patients (mean age 81 ± 4 years, 66.5% men) were consecutively screened for eligibility. Of these, 37 were excluded for heart failure or left ventricular ejection fraction of 35% or less (n = 23), cognitive impairment (n = 9), severe musculoskeletal disease (n = 5). The remaining 160 were randomly assigned to a control (C) or a treatment (T) group in a 1:1 ratio, using a computer-generated list (Figure 1), after they had completed a 4-week CR programme as detailed elsewhere.
25
The median interval between hospital discharge and admission to outpatient CR was 9 days. C group patients were instructed to carry out self-managing sessions of walking and/or biking and/or calisthenics. The intensity of home-based training was prescribed as to attain a 70–85% of peak heart rate achieved in a symptom-limited cardiopulmonary exercise test carried out at the end of the 4-week CR. Patients were also instructed appropriately to perform the training sessions (rest, load shedding, etc.) and to recognise alert symptoms that suggested the need to reduce the load or to stop exercising. T group patients were assigned to a home-based exercise programme, consisting of standardised exercises of intensity prescribed following the same method used for C patients. This prescription could be modified at subsequent monthly visits scheduled over the first 6 months, or in the case of clinical need. Patients were also instructed to record in a logbook the beginning and termination of exercise sessions, the type of exercise (walking, biking, calisthenics) and the heart rate at rest and at mid-session. The need to reduce the workload or to stop the exercise session, and the main reason for doing it, also had to be reported in the logbook. During the monthly follow-up visits, these patients also underwent reinforcement sessions at the rehabilitation centre, where they were asked to bring the logbook that was taken as a check of their adherence to exercise prescription. In order to reinforce their adherence to the exercise programme, during the monthly visit patients were asked to repeat the home exercise programme under the supervision of a member of the rehabilitation staff who checked the correctness of exercise procedures, the compliance with exercise times and resting and exercise heart rate. The physical training programme was interrupted in the case of cardiovascular or non-cardiovascular relevant clinical events (i.e. relapse of acute coronary syndrome, pneumonia, fracture, urinary tract infections), requiring or not hospitalisation and limiting the possibility to exercise safely; the programme was continued soon after clinical stabilisation. In the case of interruptions longer than 2 weeks, which did not occur during the study, the patients would have been switched to the C group. At 6 (F6) and 12-month (F12) follow-up visits, functional capacity, health-related quality of life and clinical events including re-hospitalisations for cardiovascular and non-cardiovascular reasons were re-assessed in all patients.
Flowchart of study participants through the study.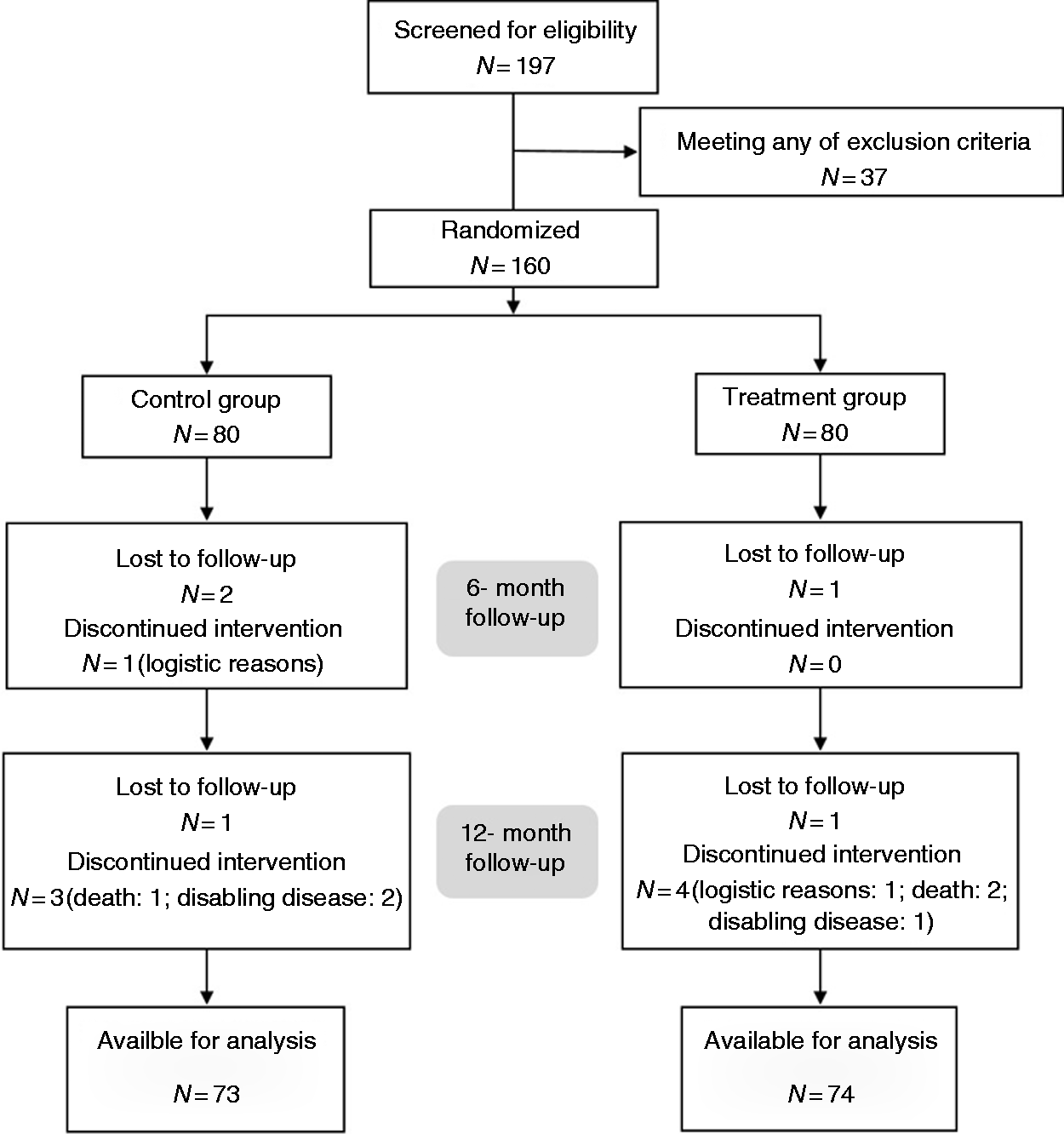
Functional capacity and outcomes measures
Changes in aerobic capacity during the follow-up in the T as compared to the C group was the main study outcome measure. Aerobic capacity was expressed as the maximal oxygen consumption (VO2-peak, ml/kg/min) resulting from breath-to-breath analysis (CPX Medical Graphics system) during a symptom-limited cardiopulmonary exercise test at cycle ergometer (Formula ESAOTE Biomedica instrument), conducted following a 10 Watt/minute incremental workload protocol, which was considered to be the most appropriate to evaluate post-acute elderly, as reported in the 2002 American Thoracic Society/American College of Chest Physicians statement on cardiopulmonary exercise testing. 26 Endurance, lower limb muscle strength, and health related-quality of life were secondary study outcome measures. Endurance was defined as the total distance walked during a 6-minute walk test (6MWT) 27 in a 30-metre corridor with telemetric ECG and oxygen saturation monitoring, without previous familiarisation test. Lower limb muscle strength was measured with an isokinetic dynamometer (BIODEX Medical System) at three progressive angular speeds (5, 8 and 10 repeats at 90, 120 and 180°/second), evaluating the bilateral quadriceps and hamstring muscles strength in flexion extension. The outcome measure was the averaged 90° Torque peak (Newton for metre). 28 Health-related quality of life was measured with the Short Form-36 (SF-36) questionnaire. 29 Adherence to the rehabilitation programme in the T group was evaluated at each of the five recall visits, according to four predefined items: appointment attendance; execution of all exercises; correct execution of exercises; completion of exercises within the expected time. Adherence was scored on a 0.0–1.0 scale, in which only patients with an excellent level of adherence (from 1 to 0.85) were considered as adherent. For more details, see Appendix 1.
Statistical analysis
It was estimated (G-Power 3.118 software) that a sample size of at least 144 patients was needed to detect a difference of at least 2.0 ml/kg/minute in VO2-peak at 12-month follow-up between the T and C groups at a significance level of less than 0.05 with a power (1-b) of 0.85. Statistical analyses were performed using the SPSS v.23 package. Continuous and categorical variables are expressed as mean ± standard deviation or percentages, respectively. Student's t-test and or the chi-square test were used for between-group comparison of continuous or categorical variables at baseline. Analysis of variance (ANOVA) for repeated measurements was used to compare the time and treatment-related changes. The Greenhouse–Geisser correction was adopted when statistical significance of Mauchly's test for sphericity was violated. A two-sided P < 0.05 was considered statistically significant.
Results
Study population
Demographic and clinical characteristics of control (C) and treatment (T) groups at random assignment.
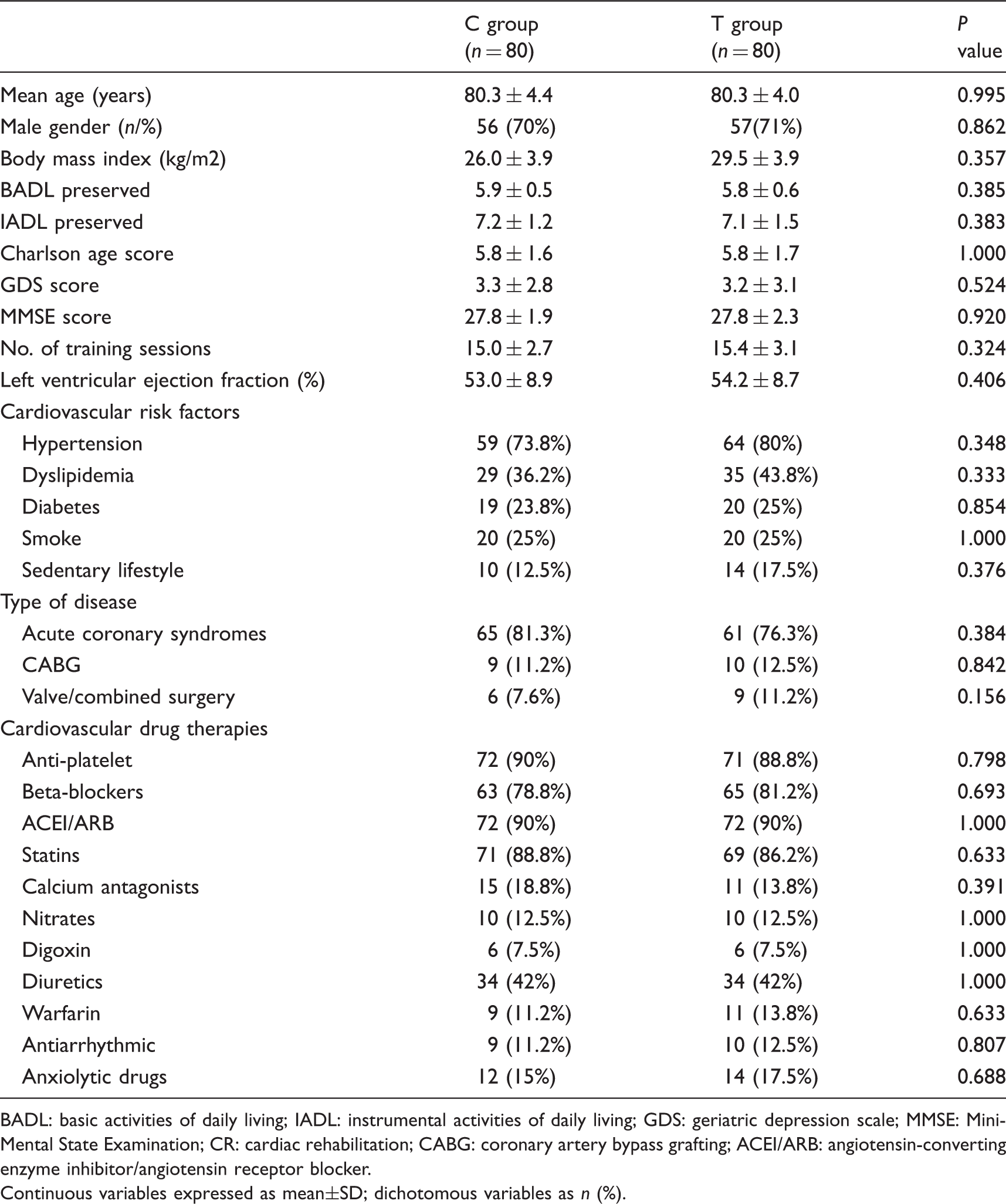
BADL: basic activities of daily living; IADL: instrumental activities of daily living; GDS: geriatric depression scale; MMSE: Mini-Mental State Examination; CR: cardiac rehabilitation; CABG: coronary artery bypass grafting; ACEI/ARB: angiotensin-converting enzyme inhibitor/angiotensin receptor blocker.
Continuous variables expressed as mean±SD; dichotomous variables as n (%).
Overall, 13 patients (8.1%), similarly distributed in the two groups (P = 0.754), did not complete the follow-up: three died of non-cardiovascular reasons between 6 and 12 months (two newly diagnosed lung or gastric cancer, one1 septic shock); three developed non-cardiovascular disabling diseases; two could not attend the visit for logistic reasons; and five (3.1%) were lost to follow-up (Figure 1). Therefore, 147 (91.9%) completed the programme and were analysed.
Functional outcomes
Both the C and T groups obtained a significant and similar improvement from baseline to the end of the 4-week CR programme in all outcome variables (Figure 2). However, no significant difference was found between their further trajectories, adjusted for age and gender, over the 12-month follow-up (Figure 2). These results were confirmed when analysing the trajectories, for age, gender and baseline VO2-peak (data not shown).
Effect of active versus control treatment on physical performance measures over time. B: baseline; R: randomisation; F6: 9-month follow-up; F12: 12-month follow-up.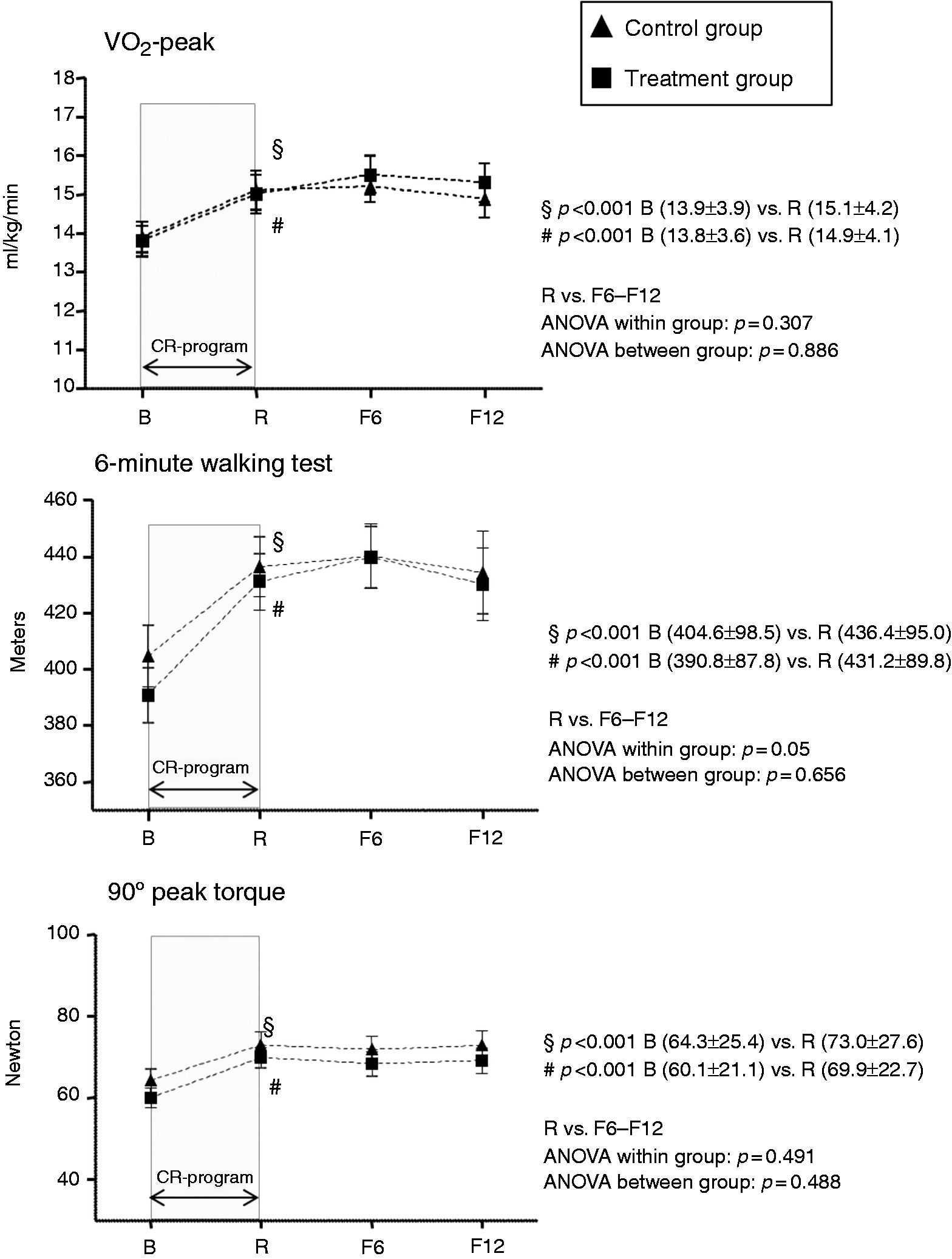
Health-related quality of life
SF-36 total score and its two subscores (physical functioning and mental health) were similar in the C and T groups both at baseline and over the whole follow-up, and failed to show any change within each group (data not shown).
Adherence
The average score in T group was 0.76, suggesting overall good adherence. In particular, adherence was scored as excellent in 40.3%, good in 28.6%, sufficient in 11.7% and poor in 12.9% of patients, while 6.5% only were non-adherent. We further analysed the results by comparing adherent, non-adherent and C group patients. Adherence to the treatment did not affect VO2-peak at either F6 (P = 0.950) or F12 (P = 0.955). However, at F12 adherent patients had better, although not significantly, values of 6MWT (P = 0.805), 90°Torque peak (P = 0.667) and total SF-36 (P = 0.188), when compared to both non-adherent and C group patients.
Hospitalisation rate
Over the follow-up, there were 51 re-hospitalisations, with no difference between the C and T groups neither for the absolute numbers (23 and 28, respectively; P = 0.208) nor for the subtypes of re-hospitalisation due to cardiovascular (F6 P = 0.416 and F12 P = 0.568) or non-cardiovascular reasons (F6 P = 0.363 and F12 P = 0.574).
Discussion
Focusing on the research hypothesis and on the primary and secondary outcomes, the main result of the CR-AGE EXTRA randomised trial was that, compared to a conventional follow-up, an interventional, 6-month re-enforcement programme had a neutral effect on global functional capacity, health-related quality of life and re-hospitalisation rate. Notwithstanding, we guess that a relevant finding of our trial was that an even short (4 weeks) outpatient CR programme is effective in producing, in patients well beyond the age of 75 years who are at increased risk of functional deterioration after hospitalisation, a sustained improvement in functional capacity measures, regardless of the follow-up programme. Following the results of our previous work, 21 we built an outpatient CR programme individually tailored for older patients, through the development of some peculiar aspects of both evaluation and intervention. Baseline evaluation, indeed, was improved with the systematic inclusion of CGA, to capture all the multifaceted aspects of the clinical complexity of older patients. 32 Each clinically relevant issue emerging from CGA was individually discussed and treated by a specialised, multiprofessional team with possible involvement of family members and/or caregivers. An individually tailored health education programme was further enriched with the inclusion of nurse-managed sessions aimed at enhancing adherence to the outpatient and experimental CR programme. In order to improve adherence to the outpatient phase of the programme, which particularly in older patients may be limited by multiple reasons, including logistic ones, we intentionally reduced the number of sessions of physical training, as compared to our previous study. 21 Accordingly, recent observational data confirm that in elderly patients even modest levels of physical activity are able to reduce cardiovascular risk. 33 Indeed, we demonstrated that a well-structured health education programme, even with such a reduced exercise prescription, produced both a high adherence rate and a sustained functional benefit over the follow-up.
We may also hypothesise that this health education programme during the 4-week CR positively influenced the subsequent lifestyle behaviour in all participants in the trial, including their habit of daily exercise, thereby reducing the difference in primary and secondary outcomes between the C and T groups over the follow-up. This might explain the resulting neutral effect of the intensive reinforcement intervention. The effectiveness of a secondary prevention programme on risk factor control, diet adherence and functional capacity in elderly patients after acute coronary syndrome was proved in a recently published randomised clinical trial. 34
An alternative explanation of the neutral results observed during the follow-up might consist of a possible overestimation of adherence to the home-based exercise programme from self-recording sessions in the logbook. Although some studies suggested the possibility of improved assessment of adherence to home-based CR programmes with use of telemedicine technology,35,36 these techniques are not yet validated, particularly in older populations and, hence, logbook recording remains the most commonly used method for the home monitoring of adherence. 37 Therefore, we must recognise that we were unable better to assess objectively the actual adherence to the home-based exercise programme and, therefore, to determine the positive impact of the reinforcement programme on mid-term physical performance.
Despite the neutral effect of our experimental, home-based reinforcement programme, we think that our study reinforces the beneficial impact of CR, which improves mid-term aerobic capacity, endurance and muscle strength with a short (4-week) and early programme, even in patients older than 75 years of age. These results are coherent with the concept that recovery of exercise capacity after an acute event may be clinically valuable to prevent frailty38,39 and disability40–42 in older patients, and with an American Heart Association/American College of Cardiology/American Geriatrics Society joint statement, reporting that ‘Studies are needed to refine the utility of CR programmes to optimize functional capacity, reduce disability and fall risk, preserve independence’. 43
We have to acknowledge some study limitations. First, as we compared only patients who received CR without controls allocated to usual care without rehabilitation, we cannot exclude a spontaneous CR-independent, short-term recovery of physical function, has occurred after acute hospitalisation. However, we considered a no-CR arm as ethically unacceptable in view of guidelines recommendations1–6 and of results of our previous CRAGE trial, 21 particularly in a hospital with well-established rehabilitation facilities. Second, because of the home-based nature of our study, we selected a population free of cognitive decline and functional disability, and this might limit the gene-ralisability of our results. We may speculate that if we had applied the same home programme to a frailer and functionally impaired population, we could have obtained a significant difference in the endpoints at 6 and 12 months. Nonetheless, we are convinced that, with this selection, we could demonstrate the feasibility of such a programme and identify patients who can be safely rehabilitated at home, in order to maintain their functional capacity and prevent their possible progression towards functional decline after an acute cardiac event. 42 Finally, we have obtained a good adherence to a home programme, without significant differences between adherent, non-adherent and C group participants. However, given the trend towards better results of adherent patients, it is possible that higher adherence could have led to different results between the C and T groups.
Footnotes
Author contribution
CB and FF contributed to the conception or design of the work. AP contributed to the acquisition, analysis and interpretation of data for the work. CB, RB, MVS and SV contributed to the acquisition of data. SB and FF contributed to analysis and interpretation of data. NM contributed to interpretation of data. AP, SB and FF drafted the manuscript. CB, FO, AU and NM critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.