
Abstract

Perioperative myocardial infarction (PMI) is a serious complication after cardiac surgery with an estimated incidence of 1–10%. It is associated with increased in-hospital morbidity and mortality. 1 The subtle and challenging presentation of PMI often requires rapid and effective diagnostic and therapeutic interventions, to salvage the ischaemic myocardium, protect from endothelial dysfunction and preserve cardiac function. 2 Emergency coronary angiography (ECA) has emerged as a safe and effective tool to identify PMI in post coronary artery bypass graft (CABG) patients with haemodynamic instability.1,3,4 However, its role in other cardiac surgeries is unclear. 5 It should be emphasized that ECA after cardiac surgery procedure is performed in patients in a critical condition, which increases the risk of cardiac and non-cardiac complications, including sudden cardiac arrest, bleeding, acute kidney injury and others. 6
We report our institutional experience of performing ECA in patients with haemodynamic instability or suspected myocardial ischaemia within 24 h after cardiac surgery. Out of 11,537 consecutive cardiac surgeries performed at our institution over a five year period, 115 patients (1.19%) underwent ECA during the early postoperative period of 24 h after cardiac surgery. Cardiac surgeries were performed using standard operative techniques. ECA was performed during the early post operative period if the patient had any of the following criteria: new unexplained haemodynamic collapse, malignant ventricular arrhythmias, sudden cardiac arrest, persistent ST-segment changes on electrocardiogram (ECG), elevation in high-sensitivity cardiac troponin T, ck-MB levels or new regional wall motion abnormalities on 2D-transthoracic echocardiogram or any other clinical findings suggestive of myocardial ischaemia. ECA was deferred if acceptable haemodynamic stability could not be maintained despite maximal medical therapy. ECAs were performed in a standardized way by a cardiologist. After the ECA patients were transferred to the cardiothoracic surgery intensive care unit. The decision to pursue percutaneous versus surgical revascularization was left to the discretion of physicians based on the results of ECA.
The chi-square test was used for categorical variables. Associations between non-parametric and parametric variables were assessed by Spearman’s and Pearson’s tests, respectively. Multiple logistic regression was used to identify the predictors of in-hospital mortality in the ECA cohort. A two sided alpha (p value) of less than 0.05 was considered statistically significant. In-hospital mortality was defined as any death that occurred during the same hospital admission corresponding to cardiac surgery.
The ECA cohort was composed of 66.2% males and a mean ± (SD) age of 65.9 ± 11.4 years. Coronary artery disease (CAD) (80.1%) and hypertension (78.8%) were the most common comorbidities. Sixty per cent had prior myocardial infarction and 31.2% had prior percutaneous coronary intervention (PCI). The most common indication for ECA was haemodynamic instability (35%) followed by ECG changes (25%), cardiac arrest (23%), troponins elevation (8%) and miscellaneous causes (9%).
The most common finding on ECA was graft failure (31.3%) followed by coronary artery occlusion (7.8%), coronary artery embolism (7.0%), coronary artery spasm (4.3%), extrinsic compression (2.6%), diffuse atherosclerosis (1.7%) and subclavian artery stenosis (0.9%). No significant pathology was identified in 50/115 (43.5%) patients. Cardiac surgeries with CABG are more likely to yield a positive finding on ECA compared with non-CABG only surgeries (43/77 (55.8%) vs. 10/38 (26.3%); p value < 0.001). We did not observe statistically significant differences in the ECA finding based on indication for ECA. Table 1 summarizes the ECA results and outcomes in the entire cohort and cohorts stratified by type of surgery. Overall in-hospital mortality was 36.5% with no significant difference between the groups (p = 0.94). Significant predictors of mortality were age, diabetes mellitus and hyperlipidaemia, which are also main risk factors for morbidity and mortality in cardiovascular disease, including heart failure and ischaemic heart disease7–9 (Figure 1).
Predictors of mortality in the emergency coronary angiography group (N = 115). Outcomes of emergency coronary angiography after cardiac surgery (N = 115). Data are represented as column percentage (absolute counts). CABG: coronary artery bypass graft; ECA: emergency coronary angiography; IABP: intra-aortic balloon pump; LAD: left anterior descending artery; LCx: left circumflex artery; OR: operating room; PCI: percutaneous coronary intervention; RCA: right circumflex artery; RPD: right posterior descending artery.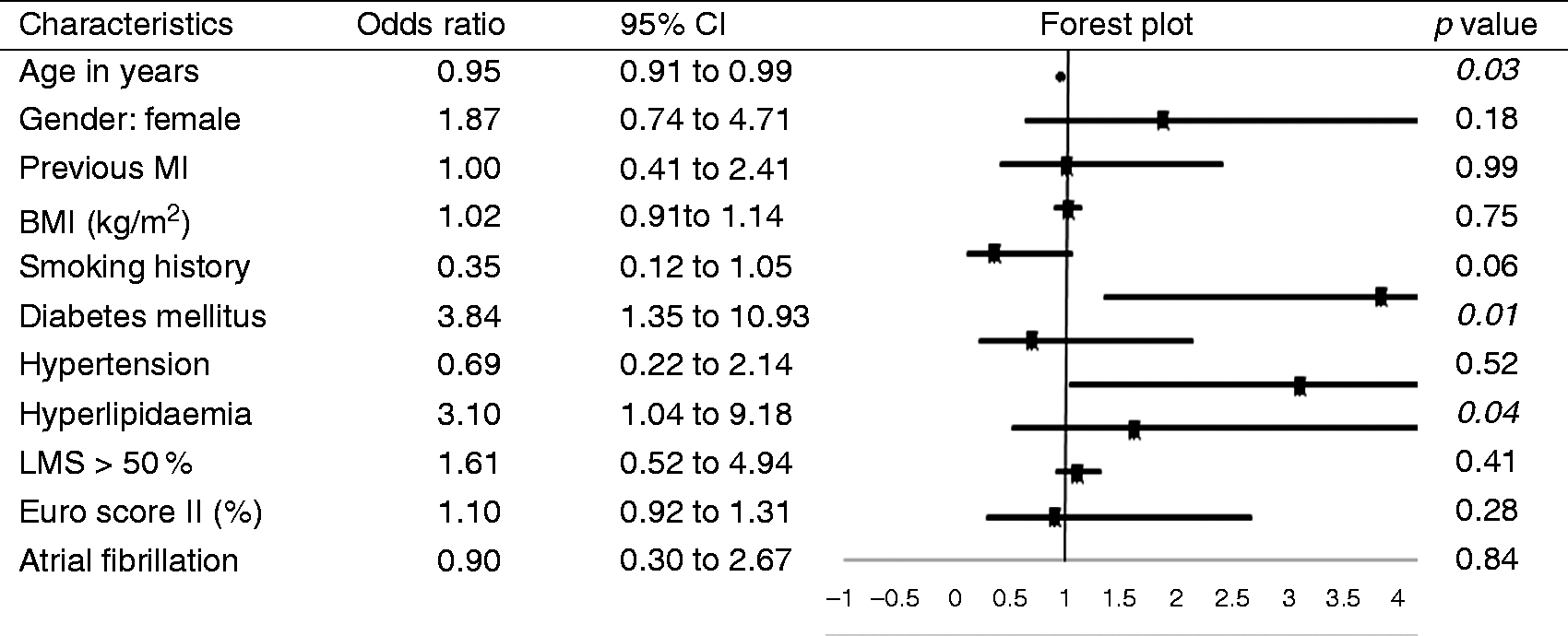
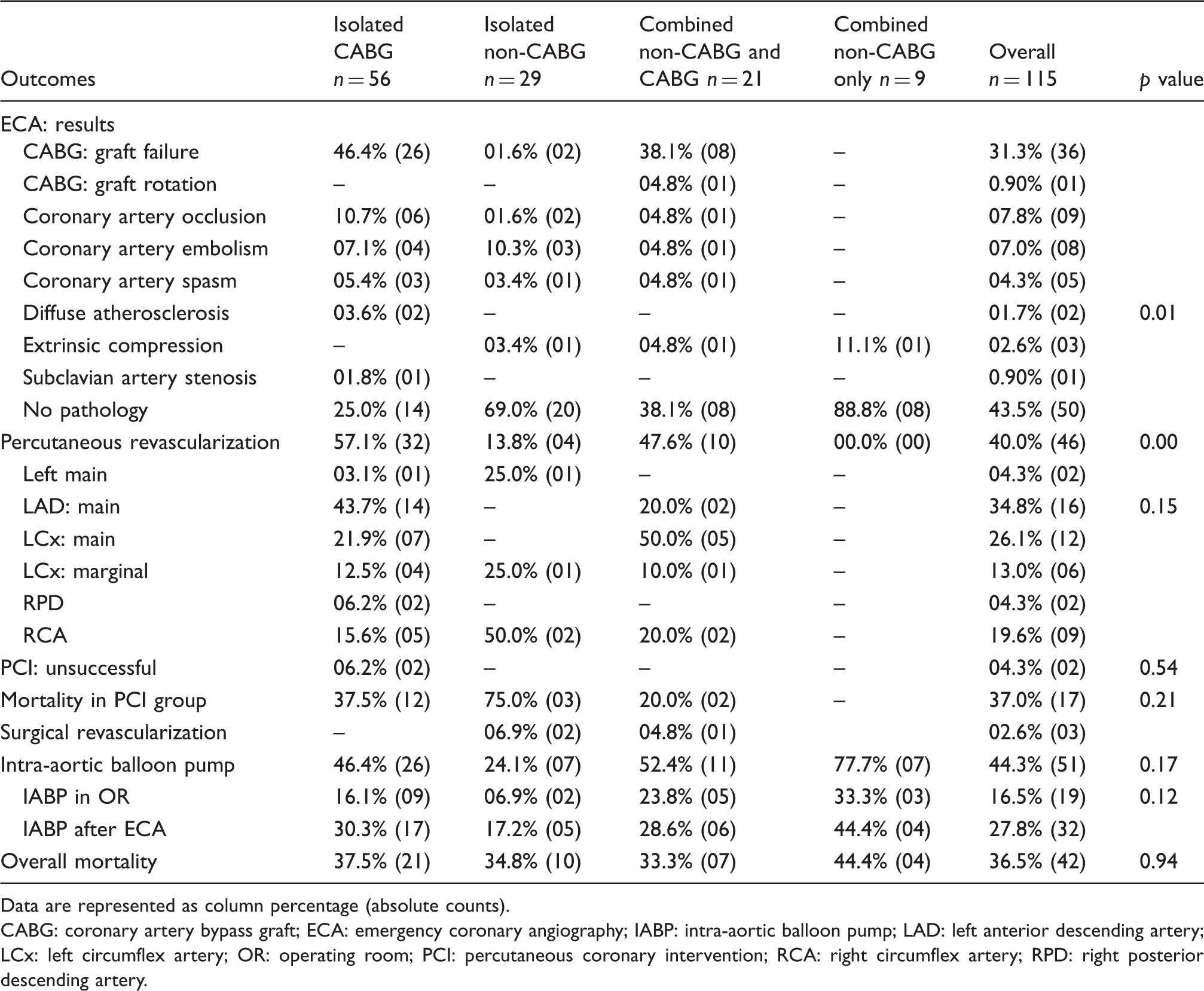
ECA was more frequently performed following combined procedures compared with isolated procedures. PCI was more often performed in CABG groups. However, there was no significant difference in overall mortality rates and mortality after PCI between the four groups. This indicates the safety and feasibility of ECA in other types of cardiac surgeries in addition to CABG.
Graft related complications were significantly higher in CABG groups. There was no statistically significant difference in non-graft related PMI between the CABG and non-CABG procedures. Therefore, ECA can be used to diagnose non-graft related complications such as coronary artery spasm and peripheral coronary artery embolism in any type of cardiac surgery, reducing the need for a reoperation – 5.25% in our study.
CABG groups were more likely to be percutaneously intervened after ECA than non-CABG groups, which is expected due to the higher graft failure rates and pre-existing CAD in this group.
Our study shows that ECA is safe even in those cases who underwent PCI. Only one patient died during angiography (0.9%), which, however, was related to his critical condition rather than the procedure itself.
ECA was done in 1% of the patients enrolled in our study, which is comparable to other studies. 3 Overall in-hospital mortality was 36.5%, which was comparable in all groups. Previous studies assessed mortality rate in patients with graft failure on angiography or analysed only a small group with a mortality range of 10–12% which was not comparable among the subgroups.3,10 It should be remembered that these studies were aimed at comparing the therapeutic options after cardiac surgery although this was not the aim of our study and we analysed the largest cohort ever reported in the literature (11,537) in a tertiary care highest referral centre.
The decision to carry out ECA and PCI when indicated was taken by a team consisting of an Intensive Care Unit physician, interventional cardiologist and a cardiac surgeon. It was taken in the first 24 h after cardiac surgery for a rapid diagnosis in order to prevent further complications. In our opinion this is important for two reasons. First, our results are based on the largest cohort of patients in the literature. Second, previous studies were performed when PCI techniques and coronary angiography was not so advanced as nowadays. Therefore we herein present actual results of ECA in actual cardiac surgery.
Footnotes
Author contribution
RL and GF contributed equally to the manuscript and are co-primary authors. RL, GF and BK contributed to the conception and design of the work. MBr and MBa contributed to the acquisition, analysis, or interpretation of data for the work. KB and DL drafted the manuscript. VV, KB, JS and PM critically revised the manuscript. All gave final approval and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.