
Abstract

Current approaches to prevent atrial fibrillation are limited to risk factor control at the individual level. Identifying population-based strategies to reduce atrial fibrillation incidence is also important. Improving the neighborhood environment may represent one such potential strategy. Neighborhood physical environments include walkability, accessibility of physical activity resources, and availability of healthy foods. Neighborhood social environment features include aesthetic quality, safety, social cohesion and violent crime. Better neighborhood environments are associated with lower rates of atrial fibrillation risk factors, including obesity, hypertension, and diabetes mellitus.1–3 These findings suggest that risk of atrial fibrillation may be affected by large-scale efforts to improve the built environment. We examined the association of neighborhood physical and social environments, including walkability, healthy food availability, physical activity resources, and social cohesion and safety levels, with incident atrial fibrillation in a large, multiethnic population over time.
The Multi-Ethnic Study of Atherosclerosis (MESA) recruited 6814 adults across the United States aged 45–84 years and free of clinically recognized cardiovascular disease between 2000 and 2002. 4 Standardized questionnaires were used at baseline to obtain demographic information, level of education, annual household income, physical activity, alcohol consumption, smoking history, and medication usage, including lipid lowering therapy, anti-hypertensive, or anti-diabetic use. The neighborhood environment was characterized using both Geographic Information System (GIS) data and survey-based measures of neighborhood physical and social environments.
The availability of physical activity establishments, popular walking destinations, and healthy food stores within one mile of participants’ homes was characterized using ArcGIS 9.3. 5 Densities are expressed in units per square mile (henceforth, “densities” indicates units/mi 2 ). Relevant classifications and locations of stores and facilities were identified from Dun and Bradstreet data as compiled by Walls and Associates in the National Establishment Time Series database. 6 Cumulative averages for each of these three variables were determined based on densities from each calendar year between 2000 and 2012.
Survey-based neighborhood scales included the availability of healthy food, safety, social cohesion, and walkability where the participant was asked to rate their neighborhood within a mile of their home. Survey data collected from MESA participants was combined with data from participants in an external survey (the Community Survey) administered to other residents of neighborhoods in which MESA participants lived. Each score has a total possible range from 1 to 5, with a higher score representing a more favorable environment. Scores from the survey scales were summarized as the average of all responses from participants who lived within 1 mi of each MESA participant’s home address. These 1-mi crude means were calculated for two time periods: 2000–2005 and 2006–2011.
Incident atrial fibrillation was identified from study electrocardiograms verified for atrial fibrillation at Visit 5, ICD-9 hospital discharge diagnoses consistent with atrial fibrillation (427.31 or 427.32), and, for participants enrolled in fee-for-service Medicare, inpatient and outpatient atrial fibrillation claims data.
Cox proportional hazards models were used to calculate adjusted hazard ratios for the association of each neighborhood exposure, per unit increase, with incident atrial fibrillation. We also repeated the abovementioned analysis using time-dependent models that updated covariates across study visits.
Adjusted hazard ratios of incident atrial fibrillation corresponding to a standard deviation increase in neighborhood exposure measures.
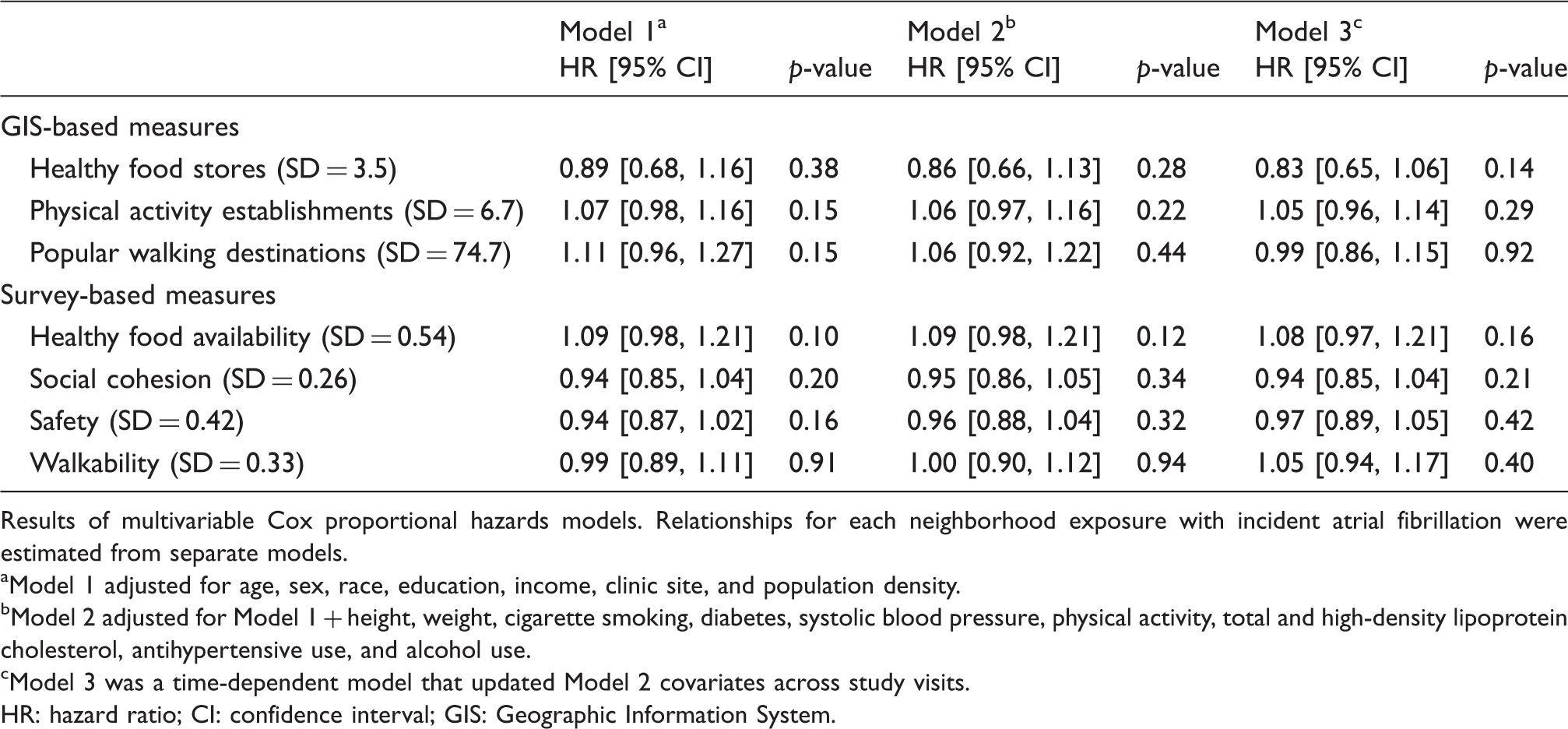
Results of multivariable Cox proportional hazards models. Relationships for each neighborhood exposure with incident atrial fibrillation were estimated from separate models.
Model 1 adjusted for age, sex, race, education, income, clinic site, and population density.
Model 2 adjusted for Model 1 + height, weight, cigarette smoking, diabetes, systolic blood pressure, physical activity, total and high-density lipoprotein cholesterol, antihypertensive use, and alcohol use.
Model 3 was a time-dependent model that updated Model 2 covariates across study visits.
HR: hazard ratio; CI: confidence interval; GIS: Geographic Information System.
In this large multi-ethnic cohort, long-term exposure to more favorable physical or social environments was not associated with a lower incidence of atrial fibrillation. A recent position paper on atrial fibrillation prevention emphasized that particular attention should be paid by policy makers to improving the population’s capability to achieve and maintain a healthy cardiovascular lifestyle through implementation of nutritional interventions and to promote regular exercise. 7 We hypothesized that an improved physical and social environment would be associated with lower incident atrial fibrillation and, therefore, potentially represent one such population-based strategy to reduce the overall atrial fibrillation burden. Better neighborhood environments have already been associated with lower rates of primary atrial fibrillation risk factors, including obesity, hypertension, diabetes mellitus, and coronary artery disease.1–3
We found no association, however, between neighborhood environment measures and atrial fibrillation. Although certain lifestyle factors such as smoking and alcohol intake have been clearly associated with atrial fibrillation risk, the relationships for either physical activity levels or changes in dietary components with risk of atrial fibrillation is not as well-established.8–10 Therefore, while better built environments might favorably impact physical activity levels and food choices, it is not clear that this would translate into a reduced atrial fibrillation risk. Another possibility is that a potential improvement in atrial fibrillation risk due to the neighborhood environment does actually exist but may be indirect and only through improved control of atrial fibrillation risk factors. We found no association, however, between neighborhood environments and incident atrial fibrillation even in a minimally adjusted model.
Our study has limitations. The method of atrial fibrillation detection used is not sensitive for cases of paroxysmal atrial fibrillation that were asymptomatic. Relevant buffer sizes for neighborhood measures may vary based on the specific exposure and different distances may be relevant for different individuals. We did not include other important neighborhood measures such as green space or neighborhood traffic safety. Lastly, we did not characterize the neighborhood environment around workplace environments.
In conclusion, long-term exposure to more favorable physical and social environments was not associated with a lower incidence of atrial fibrillation. Future studies should focus on more completely representing an individual’s neighborhood environment, including both home and work, as well as capturing their use of available resources to determine whether any potential benefit of the neighborhood environment in preventing atrial fibrillation exists.
Footnotes
Acknowledgments
Author contribution
PG, NJ, and SH contributed to the conception or design of the work. All authors contributed to the acquisition, analysis, or interpretation of data for the work. PG and NJ drafted the manuscript. EF critically revised the manuscript. All authors critically revised the paper, gave approval for the final paper, and agree to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this research was supported by contracts HHSN268201500003I, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168 and N01-HC-95169 and by grant R01-HL-127659 from the National Heart, Lung, and Blood Institute, and by grants UL1-RR-024156 and UL1-RR-025005 from the National Center for Research Resources.