
Abstract

Previous studies suggested that increased platelet levels played an important role in the development of adverse outcomes following percutaneous coronary intervention (PCI). 1 Recent studies2,3 also suggested that low baseline hemoglobin is a simple and powerful predictor of poor outcomes in patients who undergo PCI. Therefore, the platelet–hemoglobin ratio (PHR) may be a more powerful predictor of clinical outcomes. However, the relationship between PHR and outcomes after PCI has not been investigated.
The present study enrolled 6046 coronary artery disease (CAD) patients who underwent PCI. All of the patients were from the Clinical Outcomes and Risk Factors of Patients with Coronary Heart Disease after the PCI (CORFCHD-PCI; identifier: ChiCTR-ORC-16010153) study described previously. 4 To investigate the relationship between PHR and outcomes after PCI, 6050 patients were evaluated initially. Four patients were excluded due to unavailable blood routine examination data. A total of 6046 patients were enrolled in the present study. We collected and recorded demographic data, cardiovascular risk factors and laboratory data, including blood and biochemical parameters, for all patients. Cardiovascular risk factors included smoking status, alcohol consumption, previous diagnosis of diabetes, history of hypertension, familial history of CAD, history of medication and surgical disease. Fasting blood samples for routine blood tests were collected via direct venipuncture before coronary angiography after at least 12 h of fasting.
The primary endpoint was long-term mortality, including all-cause mortality (ACM) and cardiac mortality, during the up to 10-year follow-up. The secondary endpoints were stroke, bleeding events, readmission, major adverse cardiac events (MACEs) and major adverse cardiac and cerebrovascular events (MACCEs), which were described previously. 5 An adjudication committee who were blinded to the patient group determined all incidents. An event adjudication committee who were blinded to patient group adjudicated all events. All of the patients were followed up for at least two years. The median follow-up time was 32 months, and the longest follow-up time was 10 years. The investigators followed the patients via office visits or telephone contact as necessary.
All patients in the present study were divided into four groups according to PHR quartile: first quartile (PHR < 1.22, n = 1505); second quartile (PHR ≤ 1.49 to 1.22, n = 1520); third quartile (PHR ≤ 1.49 to 1.85, n = 1574) and fourth quartile (PHR ≥ 1.85, n = 1447). A number of variables were significantly different between these four groups, including age, gender, smoking, alcohol drinking, hypertension, systolic blood pressure (SBP), heart rate, creatinine and uric acid (all ps < 0.05). We did not find significant difference between groups in calcium channel blocker, angiotensin converting enzyme inhibitor or angiotensin II receptor blocker, clopidogrel, aspirin, or statin use, diabetes, body mass index, diastolic blood pressure, blood urea nitrogen, glucose, total cholesterol, triglycerides, high-density lipoprotein (HDL-C), low-density lipoprotein, apolipoprotein A1, apolipoprotein B or lipoprotein (a) (all ps > 0.05).
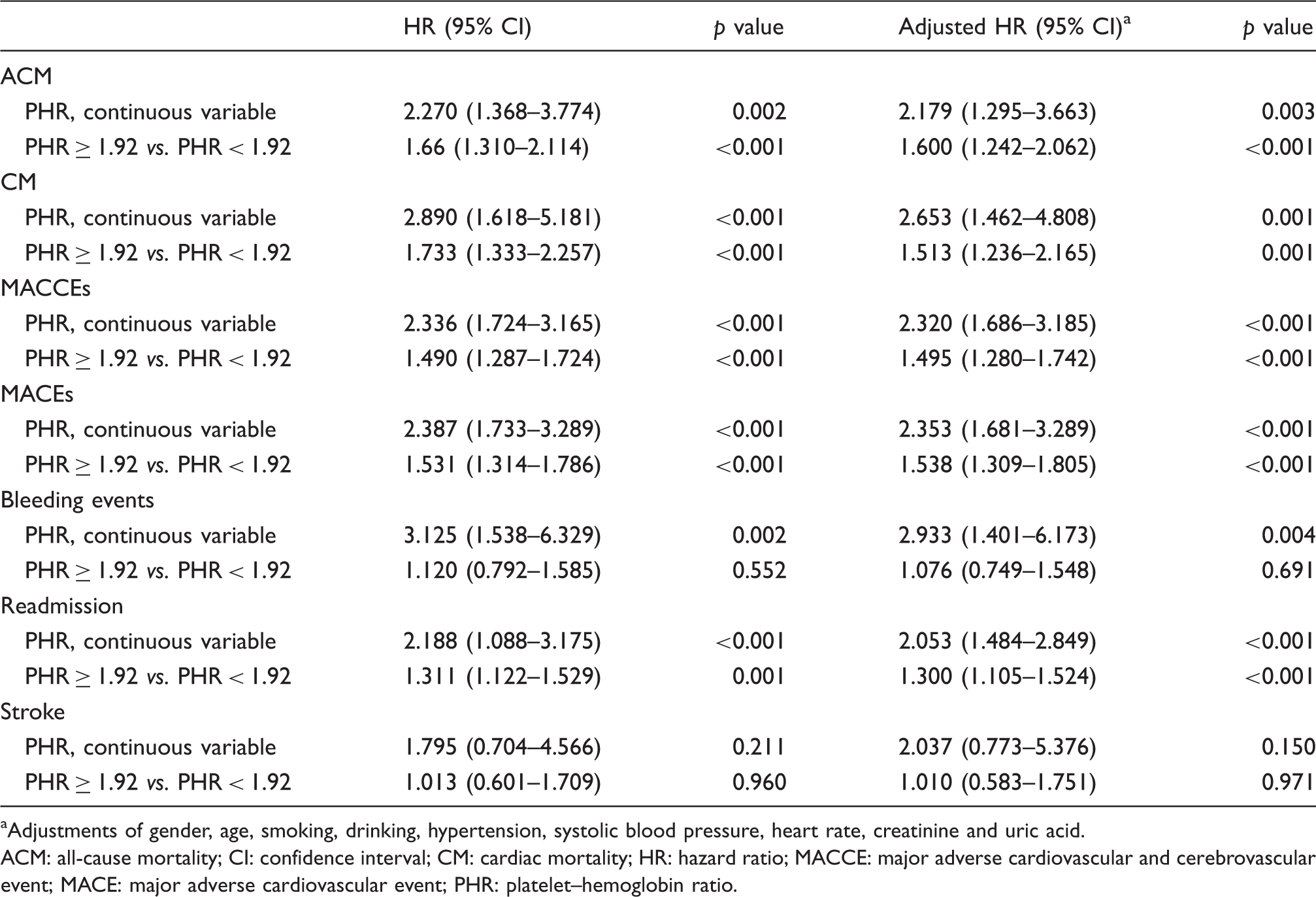
Kaplan–Meier curves for PHR divided by quartile and adverse outcomes (ACM, cardiac mortality, MACCE, MACE, bleeding events, and readmission) are shown in Figure 1. Patients in the fourth quartile with a PHR ≥ 1.85 showed significantly higher accumulated risk of ACM, cardiac mortality, MACCEs, MACEs and readmission compared with patients in the other three quartiles. Bleeding risk was highest in the second quartile and lowest in the first quartile. Multivariable analysis was performed to assess the prognostic value of PHR and adverse outcome after adjusting for gender, age, smoking, drinking, hypertension, SBP, heart rate, creatinine and uric acid. Table 1 shows the analyses with PHR as a continuous variable, and every increase of 1 in PHR was associated with 2.27, 2.89, 2.336, 2.387, 3.125 and 2.188 times increased risk of ACM, cardiac mortality, MACCEs, MACEs, bleeding events and readmission at 10-year follow-up, respectively. Although we used multivariable analysis models to account for the impact of confounders, it may not necessarily account for all differences. Therefore, we also performed a propensity matched (PSM) analysis to further clarify the predictive effect of PHR on adverse outcomes. The results showed that the predictive effect of PHR remained strong and independent after PSM analysis.
Cumulative Kaplan–Meier estimates of the time to the first adjudicated occurrence of the primary endpoint and secondary endpoints. Univariate and multivariable analyses of PHR and outcomes. Adjustments of gender, age, smoking, drinking, hypertension, systolic blood pressure, heart rate, creatinine and uric acid. ACM: all-cause mortality; CI: confidence interval; CM: cardiac mortality; HR: hazard ratio; MACCE: major adverse cardiovascular and cerebrovascular event; MACE: major adverse cardiovascular event; PHR: platelet–hemoglobin ratio.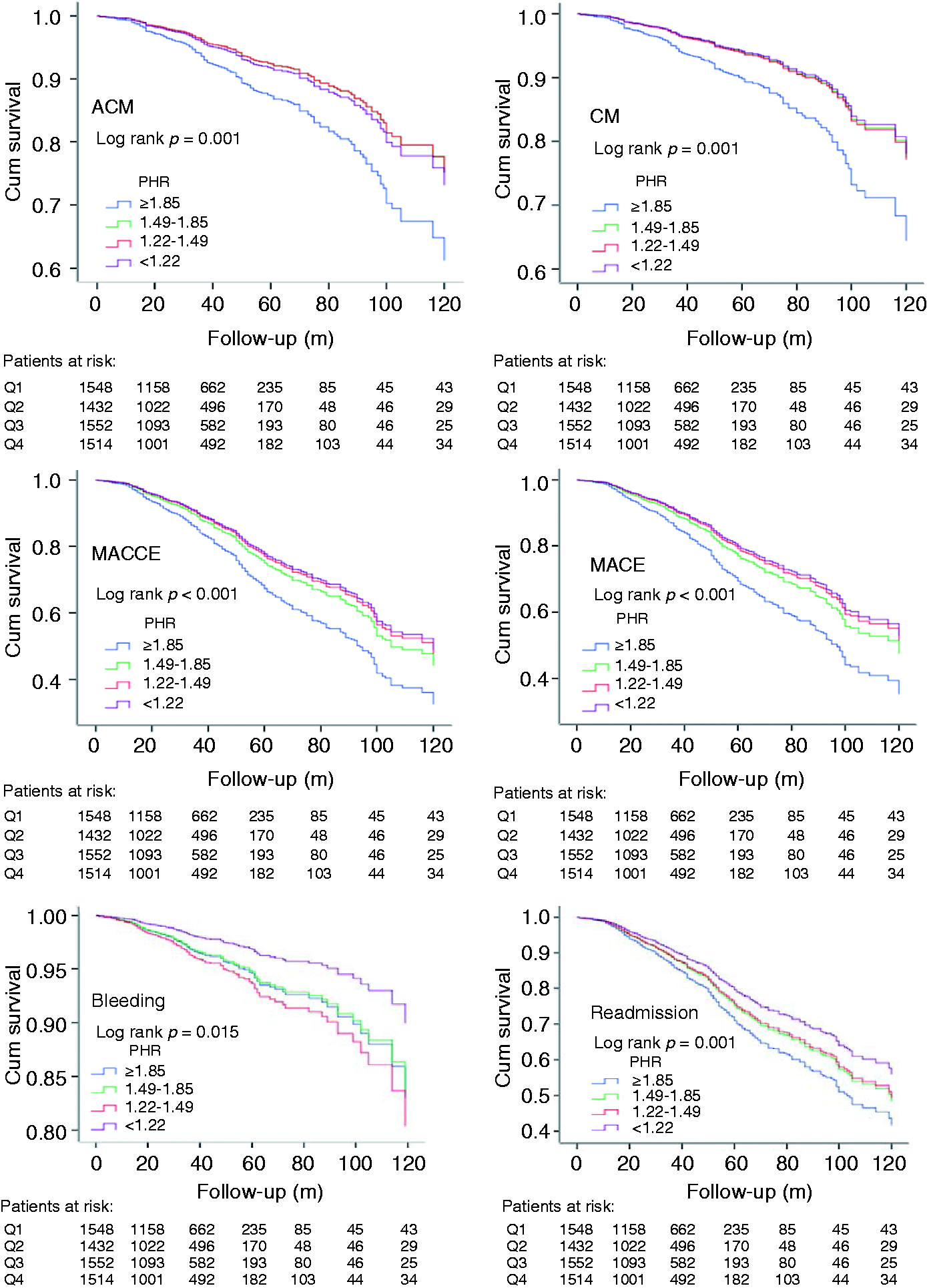
A receiver operating characteristic (ROC) curve showed that the area under the curve (AUC) of PHR for ACM was the largest (AUC = 0.708, 95% confidence interval: 0.671–0.745, p < 0.001) compared with platelet count (0.708 vs. 0.614, p = 0.017) and hemoglobin (0.708 vs. 0.663, p = 0.025), which suggests that PHR was a stronger predictor of adverse outcomes in CAD patients who underwent PCI than platelet count or hemoglobin alone. To further clarify the predictive effect of PHR, we used the Hosmer–Lemeshow goodness of fit test to evaluate the calibration of the predictive model and found that the model prediction curve was very close to the actual observation curve, which suggests that the calibration ability of the model is good (χ2 = 4.246, p = 0.834).
The ROC curve revealed 1.92 as the optimal cut-off value of PHR. Patients with a PHR ≥ 1.92 had a significantly increased risk of ACM, cardiac mortality, MACCEs, MACEs and readmission compared with patients with a PHR < 1.92. However, we did not find a significant difference in bleeding events with a cut-off value of 1.92 (data not shown). To further clarify the relationship between PHR and bleeding events, we divided the 6049 patients into eight groups according to an eight-digit method and found an inverted U-shaped curve relationship between PHR and bleeding events (data not shown).
The present study found that increased PHR was an independent predictor for adverse outcomes in patients who underwent PCI. To the best of our knowledge, this report is the first study to investigate the relationship between PHR and outcomes in CAD patients. There has been increasing interest in the prognostic role of hematological biomarkers in patients with cardiovascular disease recently. Monocyte-HDL-C ratio, neutrophil-lymphocyte ratio and mean platelet volume were highlighted as efficient biomarkers for the prediction of outcomes in patients with CAD. Several studies suggested that hemoglobin level and platelet count were independent predictors of outcomes in patients after PCI.3,4 Platelets play a key role in the pathogenesis of CAD, and this role is why anti-platelet drugs are essential in the acute phase and for long-term follow-up in preventing recurrent myocardial infarction, stroke and cardiovascular death.6–8 Therefore, a ratio of hemoglobin-to-platelets may be a novel predictor of outcomes after PCI. PHR remained an independent predictor for adverse outcomes for patients after PCI in the present study, after adjustments of confounders. Hemoglobin and platelet counts are well-established predictors of CAD outcomes, and we also observed the predictive effect of these variables alone. However, we found that PHR was the strongest predictor of adverse outcomes in patients after PCI.
There are several strengths of our study. First, the large sample size is one strength of our study, which may improve the statistical power. Second, the long-term follow-up for all patients is another strength of the present study. However, the limitations of our study should also be mentioned. We collected only baseline hemoglobin levels and platelet data during the study duration. Therefore, the effects of dynamic changes in these variables could not be analyzed. Also, the present study was a single retrospective cohort design. Therefore, our results must be further verified in a multicenter, prospective study.
In conclusion, the present study suggests that baseline PHR is an independent predictor of adverse outcome in the CAD patients who underwent PCI.
Footnotes
Acknowledgement
We are grateful to the Department of Cardiology, the First Affiliated Hospital of Xinjiang Medical University for their support and expertise in conducting this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: this research was funded by the National Natural Science Foundation of China (U1603381, 81760043 and 81560070).