
Abstract
Aims
Abdominal aortic aneurysm is a life-threatening condition due to the risk of aneurysm growth and rupture. There are no approved diagnostic or prognostic biomarkers for abdominal aortic aneurysm. We aimed to identify diagnostic and prognostic biomarkers for abdominal aortic aneurysm and to investigate their relationship with abdominal aortic aneurysm diameter and growth.
Methods
In this case-control study, patients were included from an abdominal aortic aneurysm screening study on men aged ≥65 years. Of 24,589 examined men, 415 had abdominal aortic aneurysm, out of whom 134 consented to participate in the present study. One hundred and thirty-six screened men with aortic diameter <30 mm, matched for comorbidities and time of sampling were included as non-abdominal aortic aneurysm patients. Ninety-one cardiovascular specific proteins in plasma samples were measured by the Proseek Multiplex CVD III96x96 panel.
Results
After Bonferroni correction, plasma levels of 21 proteins associated with proteolysis, oxidative-stress, lipid metabolism, and inflammation were significantly increased, whereas levels of paraoxonase 3, associated with high-density lipoprotein metabolism, were decreased in abdominal aortic aneurysm patients. Combination of growth/differentiation factor 15 and cystatin B had the best ability to discriminate abdominal aortic aneurysm from non-abdominal aortic aneurysm (area under the curve, 0.76; sensitivity, 80% and specificity, 52%). Myeloperoxidase showed the best prognostic value (area under the curve, 0.71; sensitivity, 80% and specificity, 59%) and higher baseline levels of myeloperoxidase were significantly associated with faster abdominal aortic aneurysm growth compared with lower levels, independent of baseline diameter.
Conclusions
We have identified multiple proteins associated with abdominal aortic aneurysm diameter and growth with a potential to become novel diagnostic and prognostic biomarkers for abdominal aortic aneurysm.
Introduction
Abdominal aortic aneurysm (AAA) is defined as weakening and dilatation of the abdominal aorta, most commonly affecting the infrarenal part. AAA is a potentially lethal disease that is more common in men; the prevalence is between 1.5–7.6% over the age of 65 years. 1 The pathological hallmarks of AAA are defined as a permanent, focal widening of the abdominal aortic diameter of ≥30 mm on ultrasonography or computed tomography (CT) scanning. 2 The main complication of AAA is continuing growth leading to risk of rupture, which is associated with approximately 150,000–200,000 deaths/year worldwide. 3 The risk of AAA rupture is correlated to aortic diameter and is often the first symptom of an AAA. 2 Therefore, in many countries including Sweden, 65-year-old men are invited to ultrasound screening for AAA. 4 Current guidelines recommend that small and medium asymptomatic AAA (<55 mm in men) are managed by monitoring AAA diameter under ultrasound surveillance at regular intervals chosen with regard to actual aortic diameter. 2 If a large (≥55 mm) AAA shows extensive growth or is symptomatic, the patient is referred to surgical intervention. 2
There has been no effective pharmacotherapy so far available for treating AAAs, 5 which implies that patients who are unfit for surgery or with small and medium AAAs have no active treatment options. AAA aetiology is multifactorial with known risk markers (smoking, male sex, increased age, white European ancestry, atherosclerosis and hyperlipidaemia) that contribute towards aneurysm development. 6 However, the exact underlying pathophysiology of AAA is still not well understood, making it difficult to develop therapeutic agents for AAA treatment.
Despite the proven efficacy of surveillance programmes, the associated cost can incur significant monetary burdens to the healthcare systems, so alternative methods are continuously being researched. 4
Identification of biomarkers related to aortic diameter and AAA growth may help identify patients in need of extra surveillance. In addition, biomarkers linked to AAA can be a potential target for future therapeutic interventions. However, at present, no biomarkers have sufficient sensitivity and specificity to be used in clinical praxis. 7
Recent research advances allow us to perform high throughput detection of potential protein biomarkers. For example, a new technology, the proximity extension assay, has enabled the screening of 92 proteins simultaneously with high sensitivity and specificity in small biological sample volumes. 8 In this exploratory study, we used this robust immunoassay to investigate the potential role of circulating proteins with proposed involvement in various processes associated with the pathophysiology of CVDs with the aim to identify new diagnostic biomarkers for AAA. In addition, we also aimed to examine the associations between newly identified AAA biomarkers with AAA diameter and growth. To our knowledge, this is the first study in which a wide range of potential protein biomarkers has been screened in a relatively large population-based screening cohort of AAA.
Material and methods
All subjects gave written consent to participation and the study was approved by the Ethics Committee of Lund University (2010/239) and the procedures were in accordance with the Declaration of Helsinki.
Study population
All 65-year-old men from the city of Malmö and 15 neighboring municipalities are invited to AAA screening with ultrasound at the Department of Vascular Diseases, Skåne University Hospital, Malmö. During 2010–2017, 415 (1.7%) of 24,589 examined men were found to have AAA, which is in accordance with a recent study on AAA prevalence in Sweden. 4 Out of these, 134 (32%) men accepted an invitation to undergo physical examination, blood sampling, and collection of medical history in the present study. 9 As a control group, we selected 136 screened men with aortic diameter <30 mm, matched for comorbidities and date of examination/blood sampling. Follow-up data concerning aneurysm diameter were available for 108/134 (81%) men with AAA. Ultrasound follow-up was performed at regular intervals determined by the aneurysm size according to the European recommendation and in practice with the screening programme.2,4 Therefore, follow-up data concerning aneurysm diameter were available for 108/134 (81%) men with AAA. Ultrasound examinations were performed by biomedical scientists or registered nurses using the LOGICe (General Electric Healthcare Inc., Chalfont St Giles, UK). All nurses completed a special course on ultrasound measurement of the aorta. The maximal infrarenal anteroposterior diameter of the aorta was evaluated, and AAA was defined as an aortic diameter of ≥30 mm, using the leading-edge to leading-edge (LELE) technique. In cases where the ultrasound was not conclusive, subjects were referred to conventional CT scan without contrast.
Clinical variables
The following variables were analysed: aortic diameter, systolic (S), and diastolic (D) blood pressure (BP), ankle-brachial index (ABI) in both legs, use of antihypertensive, metformin and lipid-lowering drugs, plasma (p)-creatinine, p-cholesterol, high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol, p-triglycerides (TG), p-haemoglobin (Hb), p-glucose, p-homocysteine and smoking habits. Furthermore, smoking habits were categorised into three groups; current, previous, and never smokers.
Blood sampling and biomarker quantification
Fasting venous blood (6 ml) was collected in vacuum tubes (Becton-Dickinson, Franklin Lakes, USA) containing ethylenediaminetetraacetic acid (EDTA). Blood samples were centrifuged at 1800 g for 15 min at 4℃ and the plasma was then aliquoted and stored at −80℃ for later analyses for protein biomarkers. Routine laboratory markers were analysed immediately at the Department of Clinical Chemistry, Skåne University Hospital, Malmö (SWEDAC approved according to European norm 45001).
Protein profiling of cardiovascular-associated proteins was performed using Proseek Multiplex CVD III96x96 (Olink Biosciences) panel; a full list of biomarkers with UniProt ID are presented in Supplementary Material Table S1. This protein panel was selected because it consists of a comprehensive array of proteins which have direct or indirect role in the development of cardiovascular diseases. The panel is a high-throughput, multiplex immunoassay enabling simultaneous quantification of 92 CVD-related proteins by Proximity Extension Assay (PEA) technology. 8 However, due to technical issues, C-C motif chemokine 22 (CCL22) could not be analysed and has been excluded from the panel by the vendor. The current Multiplex CVD III96x96 panel used in this study, therefore, consists of 91 proteins associated with various biological processes such as inflammation, angiogenesis, coagulation, platelet activation, cell adhesion, wound healing, chemotaxis, metabolism, etc. PEA was performed according to the Proseek Multiplex CVD III96x96 user manual at SciLifeLab located at the Clinical Biomarker Facility, Uppsala University, Sweden. 10 Briefly, 91 oligonucleotide-labelled antibody probe pairs that upon simultaneous binding to the target analyte creates a real-time PCR amplicon by a proximity-dependent DNA polymerization event and the resulting sequence is subsequently detected and quantified using standard real-time PCR. The raw data were normalised and are presented as Normalised Protein Expression (NPX). NPX-values are obtained by normalising cq-values against extension control, interplate control, and a correction factor. NPX values are on a log2 scale where a high NPX value corresponds to a high protein concentration and can be linearised by using the formula 2^NPX. The limit of detection (LOD) is determined for each biomarker based on the negative controls analysed in each run.
Statistical analyses
The Mann–Whitney U test was used for quantitative variables and the Fisher's exact test (two-sided) was used for nominal variables. The Bonferroni method was employed for multiple testing. Quantitative variables were expressed as the median and interquartile range (IQR). Nominal variables were stated as frequencies and percentages. Variables with a significant difference were included in a multivariate analysis. Logistic regression analysis adjusted for smoking, use of metformin, antihypertensive and lipid-lowering medication to test the association between biomarkers and AAA. Spearman's rank correlation coefficient test was used to evaluate correlations between aortic diameter and biomarkers. Linear regression analysis was used to test the associations between biomarkers and log transformed AAA growth (mm/year). We used receiver-operating characteristic (ROC) curves to analyse the diagnostic and prognostic potential of the protein biomarkers. This curve plot represents the true positive rate (also known as sensitivity) against the false positive rate (1-specificity) and the accuracy is measured by the area under the curve (AUC). An AUC value = 1 represents a perfect test while an AUC = 0.5 indicates no prognostic power of the test. To obtain the optimal cut-off point to discriminate the AAA patients from non-AAA subjects, we used Youden Index method. Statistical analyses were done in SPSS (SPSS Inc., IBM, New York, USA) version 20. Values of p < 0.05 were considered significant.
Results
Baseline clinical characteristics of 65-year-old men without abdominal aortic aneurysm (non-AAA) and with AAA.
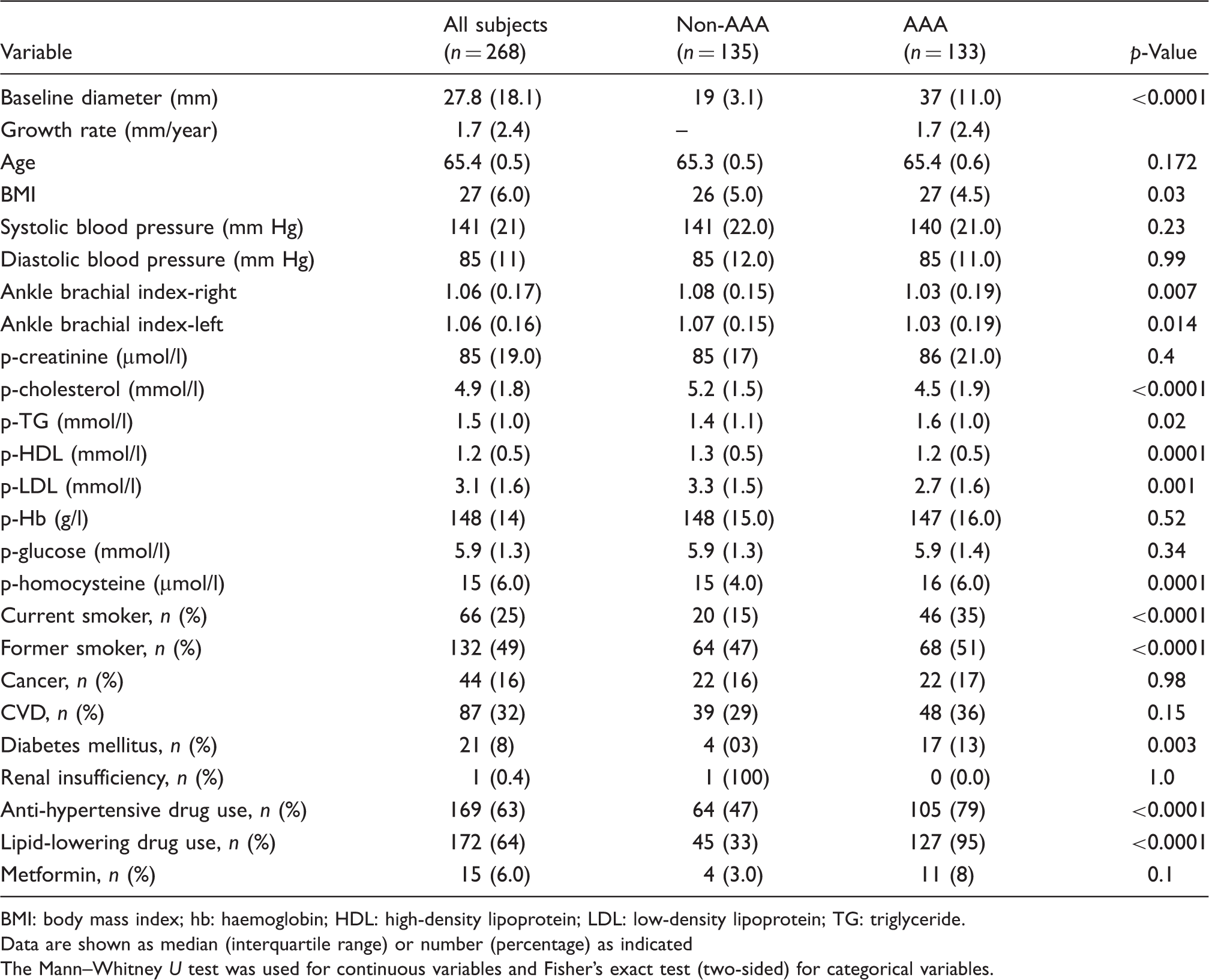
BMI: body mass index; hb: haemoglobin; HDL: high-density lipoprotein; LDL: low-density lipoprotein; TG: triglyceride.
Data are shown as median (interquartile range) or number (percentage) as indicated
The Mann–Whitney U test was used for continuous variables and Fisher's exact test (two-sided) for categorical variables.
ABI in both right and left legs, BMI, cholesterol, TG, HDL, LDL, homocysteine were significantly different between the AAA and non-AAA groups. Smoking, use of metformin, antihypertensive and lipid-lowering medication was more common in the AAA group (Table 1)
Levels of biomarkers in AAA and non-AAA patients
Levels of protein biomarkers (mean ± standard deviation (SD)) in non-abdominal aortic aneurysm (AAA) and AAA before and after multiple testing corrections (Bonferroni test), and their association with AAA risk (odds ratio (OR)) and diagnostic potential (area under curve (AUC)).
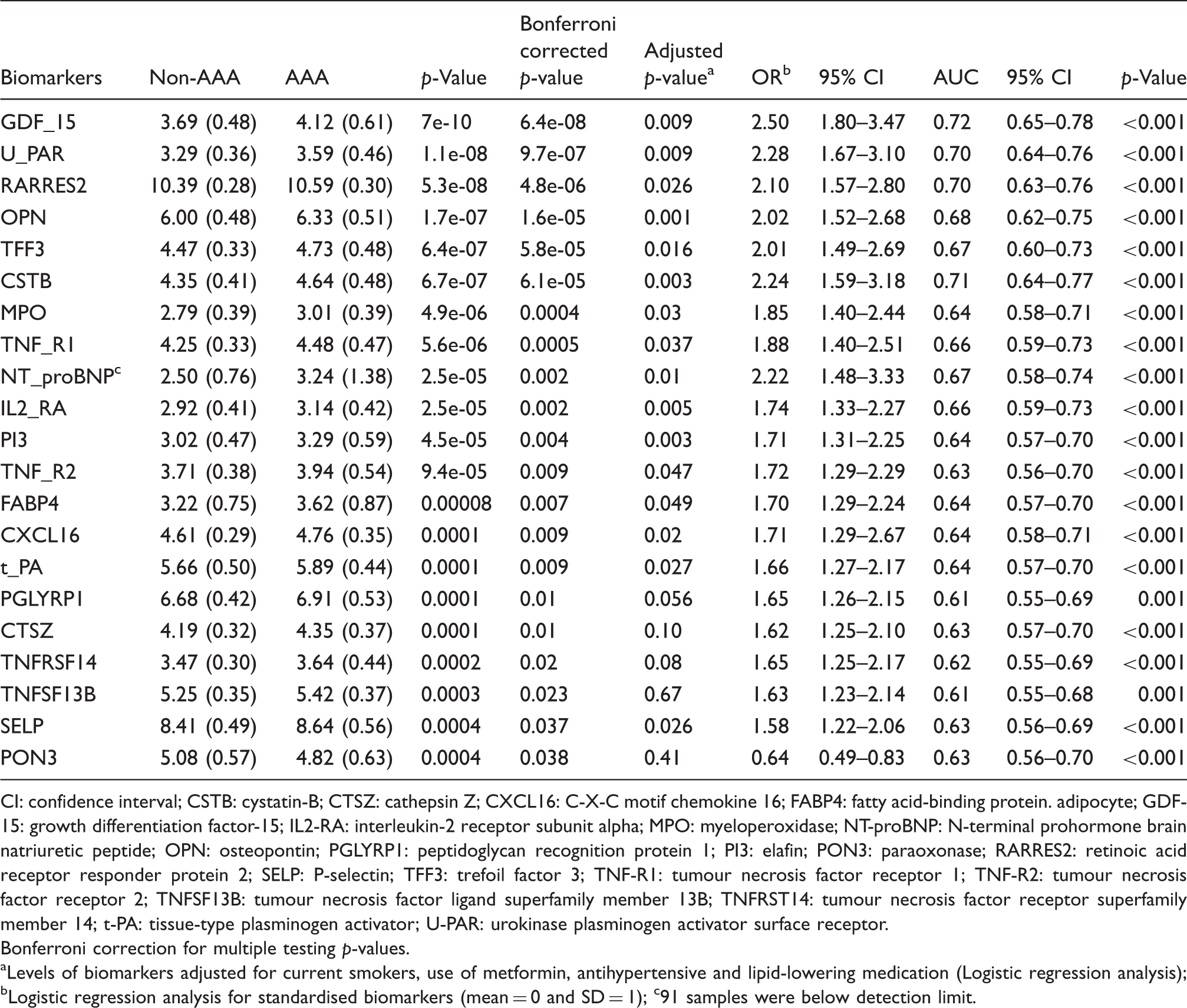
CI: confidence interval; CSTB: cystatin-B; CTSZ: cathepsin Z; CXCL16: C-X-C motif chemokine 16; FABP4: fatty acid-binding protein. adipocyte; GDF-15: growth differentiation factor-15; IL2-RA: interleukin-2 receptor subunit alpha; MPO: myeloperoxidase; NT-proBNP: N-terminal prohormone brain natriuretic peptide; OPN: osteopontin; PGLYRP1: peptidoglycan recognition protein 1; PI3: elafin; PON3: paraoxonase; RARRES2: retinoic acid receptor responder protein 2; SELP: P-selectin; TFF3: trefoil factor 3; TNF-R1: tumour necrosis factor receptor 1; TNF-R2: tumour necrosis factor receptor 2; TNFSF13B: tumour necrosis factor ligand superfamily member 13B; TNFRST14: tumour necrosis factor receptor superfamily member 14; t-PA: tissue-type plasminogen activator; U-PAR: urokinase plasminogen activator surface receptor.
Bonferroni correction for multiple testing p-values.
aLevels of biomarkers adjusted for current smokers, use of metformin, antihypertensive and lipid-lowering medication (Logistic regression analysis); bLogistic regression analysis for standardised biomarkers (mean = 0 and SD = 1); c91 samples were below detection limit.
Protein biomarkers and risk of AAA
Logistic regression analysis for standardised biomarkers (mean = 0 and standard deviation (SD) = 1) showed that higher levels of the identified biomarkers were associated with higher risk of AAA (odds ratios ranged from 1.58–2.50), except for PON3 where a higher level was associated with a lower risk of AAA (odds ratio, 0.64; 95% confidence interval (CI) 0.49–0.83). High levels of growth differentiation factor-15 (GDF-15) were associated with the highest risk of AAA (odds ratio, 2.50; 95% CI 1.80–3.47) among all biomarkers analysed in the study, Table 2.
Diagnostic potential of identified biomarkers
To evaluate the diagnostic value of the identified protein biomarkers, we performed ROC curve analysis. The AUC values and 95% CI of the protein biomarkers are shown in Table 2. Among all studied biomarkers, GDF-15 showed the best diagnostic potential based on AUC (AUC, 0.72; 95% CI 0.65–0.78) with a sensitivity of 80% and specificity of 42%, Figure 1(a).
Receiver-operating characteristic (ROC) curve analysis for the diagnostic potential of growth differentiation factor-15 (GDF-15) (a) and for combined GDF-15 and cystatin B (CSTB) (b) as best diagnostic model for distinguishing abdominal aortic aneurysm (AAA) from non-AAA subjects. Prognostic value of myeloperoxidase (MPO) (c) was identified as the best biomarker to distinguish fast growing from slow-growing AAA. Higher baseline levels (≥median) of MPO were associated with faster growth compared with lower (<median) MPO levels (d). Median and interquartile range (error bars), **p-value < 0.005 (Mann–Whitney test). AUC: area under the curve; CI: confidence interval.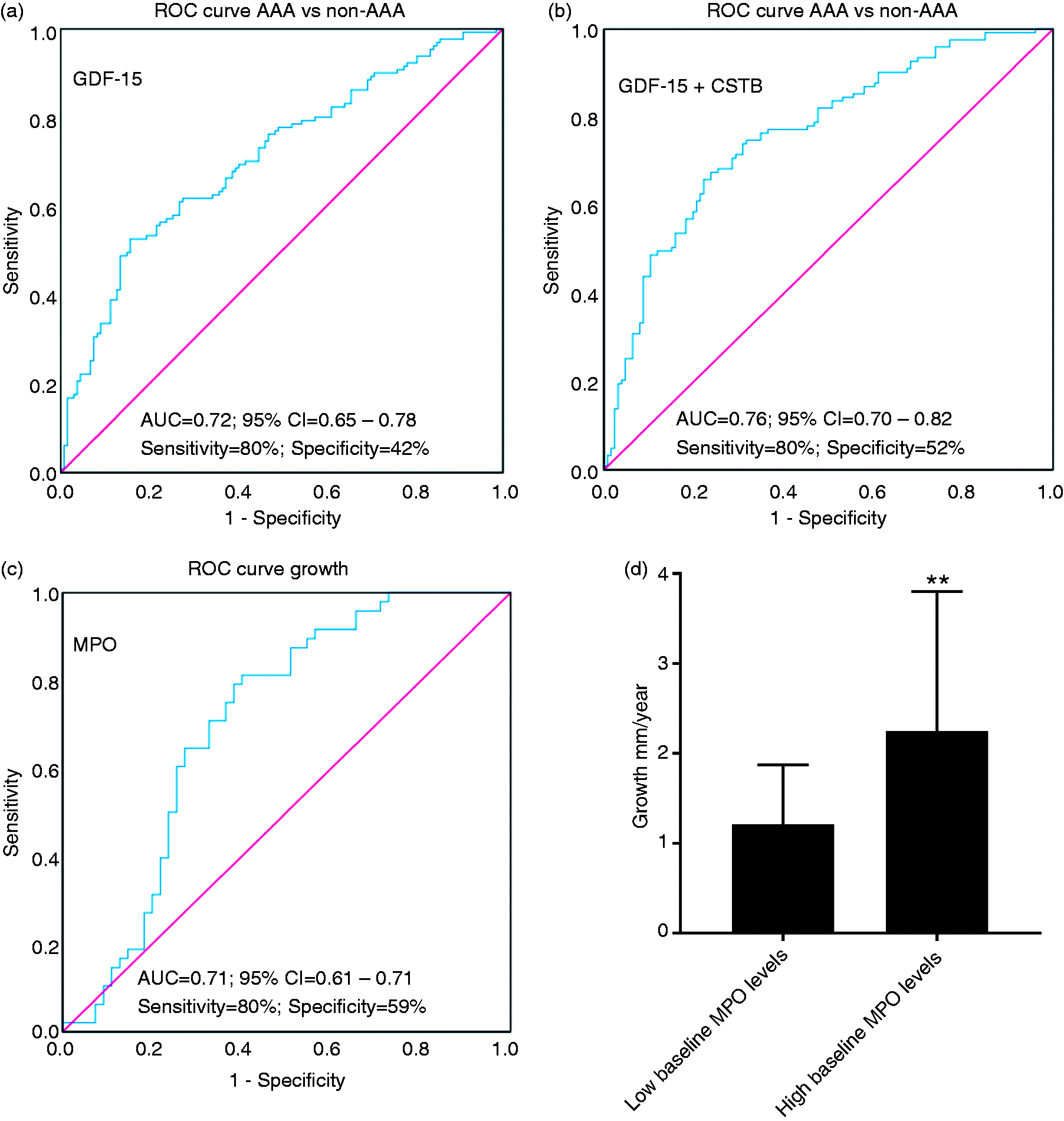
In order to further improve the classification and discrimination ability of these biomarkers we tested various combinations of biomarkers by canonical correlation analysis 11 which focuses on the correlation between a linear combination of the variables. This technique seeks the weighted linear composite for each variate to maximise their correlation by ROC curve. Our results show that the combination of GDF-15 and cystatin-B (CSTB) had the best diagnostic potential (AUC; 0.76, 95% CI 0.70–0.82), with a sensitivity of 80% and specificity of 52%, Figure 1(b)). No other combination of biomarkers showed better diagnostic value (data not shown) than the combination of GDF-15 and CSTB.
Association between protein biomarkers and AAA diameter
Spearman correlation analysis between biomarkers and abdominal aortic aneurysm (AAA) diameter in whole population (All), cases (AAA) and controls (non-AAA).
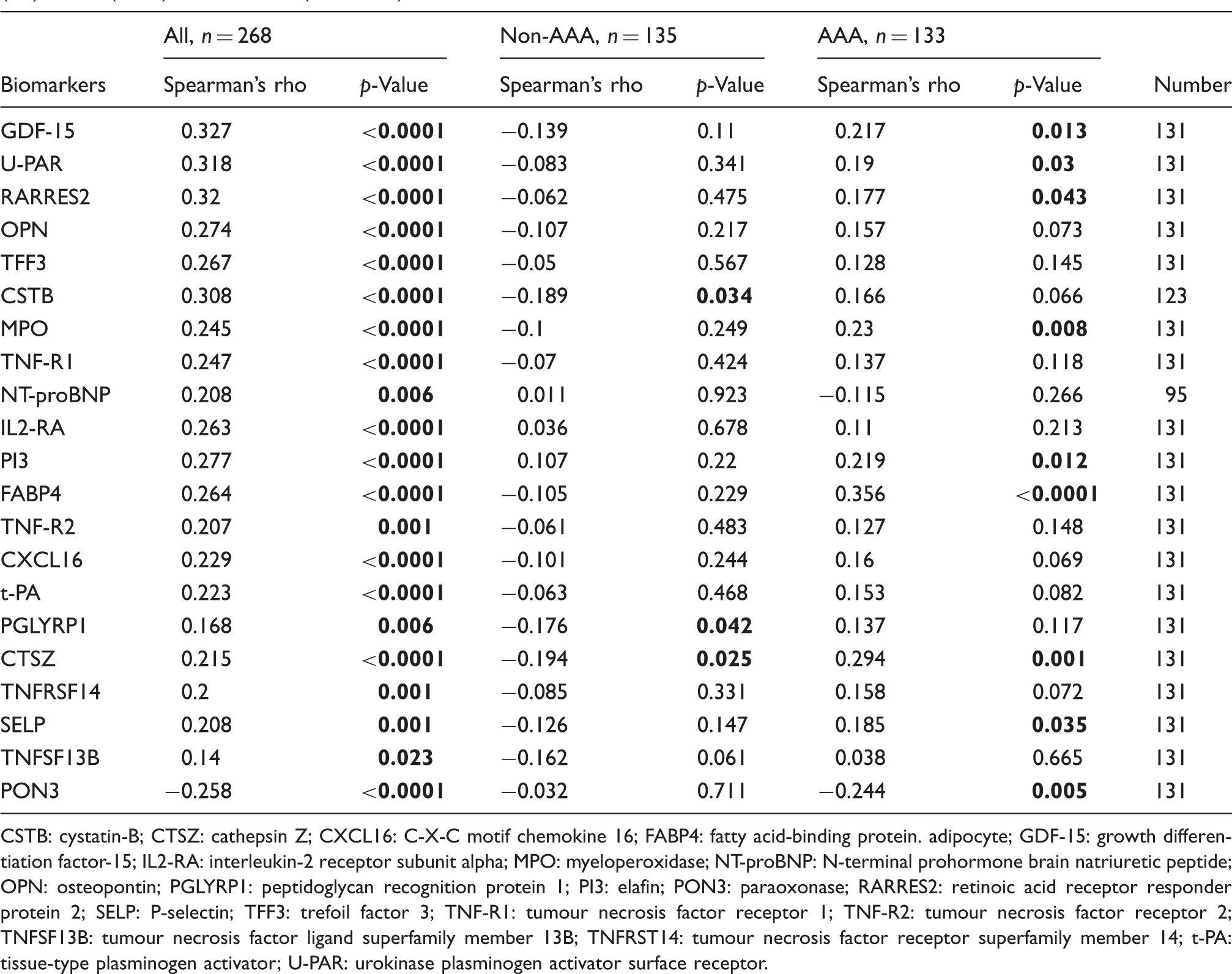
CSTB: cystatin-B; CTSZ: cathepsin Z; CXCL16: C-X-C motif chemokine 16; FABP4: fatty acid-binding protein. adipocyte; GDF-15: growth differentiation factor-15; IL2-RA: interleukin-2 receptor subunit alpha; MPO: myeloperoxidase; NT-proBNP: N-terminal prohormone brain natriuretic peptide; OPN: osteopontin; PGLYRP1: peptidoglycan recognition protein 1; PI3: elafin; PON3: paraoxonase; RARRES2: retinoic acid receptor responder protein 2; SELP: P-selectin; TFF3: trefoil factor 3; TNF-R1: tumour necrosis factor receptor 1; TNF-R2: tumour necrosis factor receptor 2; TNFSF13B: tumour necrosis factor ligand superfamily member 13B; TNFRST14: tumour necrosis factor receptor superfamily member 14; t-PA: tissue-type plasminogen activator; U-PAR: urokinase plasminogen activator surface receptor.
Associations between protein biomarkers and AAA growth and their prognostic
Associations between biomarkers and abdominal aortic aneurysm (AAA) growth as a continuous variable and their predictive value.
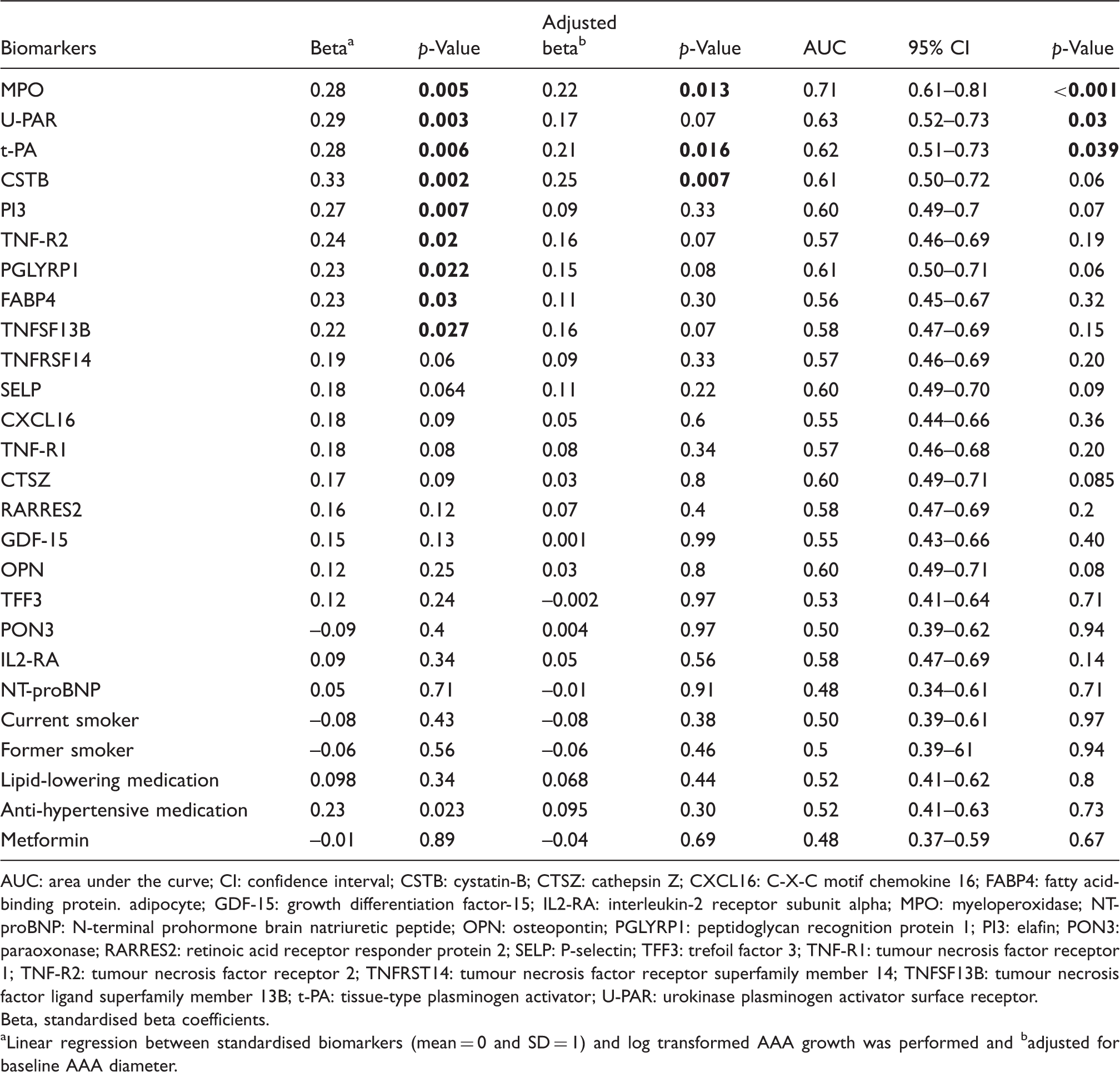
AUC: area under the curve; CI: confidence interval; CSTB: cystatin-B; CTSZ: cathepsin Z; CXCL16: C-X-C motif chemokine 16; FABP4: fatty acid-binding protein. adipocyte; GDF-15: growth differentiation factor-15; IL2-RA: interleukin-2 receptor subunit alpha; MPO: myeloperoxidase; NT-proBNP: N-terminal prohormone brain natriuretic peptide; OPN: osteopontin; PGLYRP1: peptidoglycan recognition protein 1; PI3: elafin; PON3: paraoxonase; RARRES2: retinoic acid receptor responder protein 2; SELP: P-selectin; TFF3: trefoil factor 3; TNF-R1: tumour necrosis factor receptor 1; TNF-R2: tumour necrosis factor receptor 2; TNFRST14: tumour necrosis factor receptor superfamily member 14; TNFSF13B: tumour necrosis factor ligand superfamily member 13B; t-PA: tissue-type plasminogen activator; U-PAR: urokinase plasminogen activator surface receptor.
Beta, standardised beta coefficients.
aLinear regression between standardised biomarkers (mean = 0 and SD = 1) and log transformed AAA growth was performed and badjusted for baseline AAA diameter.
ROC curves were plotted to analyse the prognostic value of each biomarker (Table 4) and MPO had the best prognostic value in terms of AUC (AUC, 0.71; 95% CI 0.61–0.81, with a sensitivity of 80% and specificity of 59%) among all biomarkers (Table 4 and Figure 1(c)). Combinations of MPO with other biomarkers did not further improve the prognostic value of MPO (data not shown). Smoking status, metformin, use of lipid-lowering and anti-hypertensive medication was not associated with the risk of AAA growth (Table 4) and had no prognostic value either. To further evaluate the prognostic value of MPO we divided its baseline levels into high and low levels according to median cut-off. Higher levels of MPO (≥median) were associated with significantly faster growth of AAA (median (IQR); 2.3 (2.9) mm/year) compared with lower MPO levels (median (IQR); 1.2 (1.1) mm/year), (Figure 1(d)).
Discussion
In this study, we evaluated the diagnostic and prognostic potential of 91 CVD-related proteins in plasma samples from subjects with and without objectively diagnosed AAA in a population-based study. In total, plasma levels of 21 proteins known to be involved in matrix remodelling, oxidative stress, lipid metabolism, inflammation or immune response were found to be significantly different between AAA and non-AAA subjects after multiple testing correction. Among the identified proteins, the role of GDF-15, elafin (PI3), retinoic acid receptor responder protein 2 or chemerin (RARRES2), tumor necrosis factor receptor superfamily member 1A (TNF-R1), tumour necrosis factor receptor superfamily member 1B (TNF-R2), P-selectin (SELP) and trefoil factor 3 (TFF3), have not previously been shown to be related with AAA in humans and for the first time we show that they may have a role in AAA aetiology.
Diagnostic biomarkers
ROC analysis of the biomarkers yielded AUCs ranging from 0.61–0.72. Furthermore, analysis of various combinations of these biomarkers demonstrated that the combination of GDF-15 and CSTB had the best diagnostic potential with an AUC of 0.76 compared with their individual analysis (GDF-15; AUC = 0.72 and CSTB = 71). GDF-15 is a member of the transforming growth factor beta (TGF-β) family. 12 Under physiological conditions, GDF-15 is expressed in low to moderate levels in most healthy tissues. GDF-15 levels may increase in response to pathological stress associated with inflammation or tissue damage, a hallmark of AAA development. 13 Growing evidence indicates that the GDF-15 level in plasma may be a new biomarker for risk stratification and therapeutic decision-making in cardiovascular diseases. 14 However, its role in AAA pathophysiology is unknown. In our study, we found a strong positive correlation between GDF-15 and aortic diameter and an association between GDF-15 and significantly higher risk of AAA. Furthermore, GDF-15 together with CSTB had the best diagnostic potential among all biomarkers analysed in the study.
CSTB is an inhibitor of cathepsin L, which is suggested to play a role in vascular remodelling and atherogenesis. 15 Clinical studies have shown that the circulating level of cathepsin L, a protease enzyme, is increased in patients with coronary artery stenosis, as well as in AAA. 15 AAA risk factors, such as smoking, hypertension and atherosclerosis, are associated with vascular endothelial cell damage, which increases lysosomal membrane permeability and induces cathepsin secretion. In our study, we found a significant increase of another cathepsin, CTSZ, in AAA patients compared with non-AAA subjects; however, after adjusting for confounding variables, it lost its significance. Interestingly, CTSZ was positively associated with aortic diameter in AAA patients whereas, in non-AAA subjects, it was negatively associated with aortic diameter. In contrast to other cathepsins, 16 the role of CTSZ has not previously been described in AAA, and therefore further investigations on the mechanisms behind the association between CTSZ and AAA are warranted. The cathepsin inhibitor cystatin C (CSTC) is well studied in AAA and its deficiency is associated with both atherosclerosis and AAA. 17 However, little is known about the role of the CSTB in AAA and other CVDs. In contrast to CSTC, a recent and only study on CSTB in AAA shows that higher levels of CSTB are associated with AAA, 18 which is in agreement with the results in the present study. Together these data suggest that CSTB and CSTC may have different roles in AAA pathophysiology.
We also identified biomarkers previously known to be associated with AAA such as U-PAR, t-PA, C-X-C motif chemokine 16 (CXCL16), FABP4, interleukin-2 receptor subunit alpha (IL2-RA), N-terminal prohormone brain natriuretic peptide (NT-proBNP), osteopontin (OPN) and MPO. PON3, a member of the paraoxonase family, was the only protein significantly decreased in AAA patients compared with non-AAA; however, its significance was lost when adjusted for lipid-lowering medication. PON3 has been shown to prevent the oxidation of low-density lipoprotein in vitro and protects against atherosclerosis in animal models. 19 In agreement with our results, a recent animal study demonstrated that the PON gene cluster protects against AAA formation. 20 Taken together, our results suggest that PON3 may be a protective molecule against AAA pathogenesis and should be investigated in future human studies.
Prognostic biomarkers
Although AAA growth is exponential, it shows great variability between individuals; for example, smaller AAAs can rupture and large AAAs can remain stable for a long time. 21 At present, a consensus regarding risk factors for AAA growth is lacking. 21 Smoking has been considered as a strong risk factor for initiation of AAA; 22 however, its role in AAA progression remains controversial. Bhak et al. showed that smoking and reduction of diastolic blood pressure reduced the rate of AAA progression. 23 In contrast, Lederle et al. could not find any association between AAA progression and smoking status or commonly used cardiovascular drugs, 24 which is in agreement with the results in this study. The lack of association between AAA progression and smoking is attributed to inconsistent data during follow-up 24 and the reduction in smoking rates after AAA diagnosis. Smoking may therefore not be a consistent risk factor for AAA growth. Therefore, identification of biomarkers for stratification of AAA with a higher risk of expansion is a major priority. Among the biomarkers, MPO had the best prognostic value and was associated with AAA growth, independent of baseline aortic diameter. Higher baseline levels of MPO were associated with significantly faster growth (2.3 mm/year) compared with lower baseline levels (1.2 mm/year). MPO belongs to the heme peroxidase family and is a major oxidative enzyme prominently expressed in neutrophils, which are abundantly found in AAA. 25 Despite its well-known association with inflammation, matrix degradation, and other pathological features of AAA, 26 the role of MPO in AAA is not well studied. We could only find one study showing higher levels of MPO in AAA. 27 Furthermore, a recent animal study demonstrates that MPO gene deletion can prevent AAA formation, 28 which supports a causal association between MPO and AAA. We have, in this study, not only shown that MPO is associated with a higher AAA risk but also with faster growth of AAA in humans. Together, these results suggest that MPO may be an important player in initiation as well as in progression of AAA and its prognostic value warrant further investigation.
One possible limitation of the study is that we have investigated 91 proteins in a matched case-control study; therefore results should be interpreted with caution. However, we adjusted our results for multiple comparisons. Secondly, because of the case-control nature of the study, the temporal relationship between the cause and effect cannot be determined. Nevertheless, this is an exploratory study in which 91 CVD associated proteins have been evaluated in an effort to identify novel AAA biomarkers. Thirdly, as all participants were 65-year-old men; the potential value of the biomarkers in women and in other age groups remains to be tested. Fourthly, it is known that subjects with AAA have higher prevalence of popliteal aneurysms (19%) and thoracic aneurysms (28%); potential impact on biomarkers in subjects with concomitant aneurysms was not evaluated. Finally, volumetric assessment based on CT or MR would have been preferable, however, the national Swedish AAA screening and follow-up programme relies entirely on ultrasound without formal testing for inter-examiner difference. The main strength of the study is that we have identified novel biomarkers which are associated with AAA diameter in a relatively larger study and also confirmed previously known associations with AAA, indicating the robustness of our data.
In conclusion, we have identified multiple novel biomarkers associated with risk and progression of AAA and now present a profile of protein biomarkers, which could help in the development of a powerful multi-marker test for diagnosis and prediction of AAA.
Supplemental Material
Supplemental material for Identification of novel diagnostic and prognostic biomarkers for abdominal aortic aneurysm
Supplemental Material for Identification of novel diagnostic and prognostic biomarkers for abdominal aortic aneurysm by Ashfaque A Memon, Moncef Zarrouk, Sophia Ågren-Witteschus, Jan Sundquist, Anders Gottsäter and Kristina Sundquist in European Journal of Preventive Cardiology
Footnotes
Acknowledgment
The authors would like to acknowledge the support of the Clinical biomarker facility at SciLifeLab Sweden for providing assistance in protein analyses.
Author contribution
AAM, AG, JS, and KS conceived and designed the study; AAM and SW prepared samples and performed the experiments; AG, MZ and SW collected the samples and clinical data. AAM, MZ, JS, AG and KS performed the data analysis and interpretation; AAM wrote the first draft and MZ, SW, JS, AG and KS revised the article, and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from NIH awarded to K Sundquist; ALF funding from Region Skåne awarded to K Sundquist; grants awarded to K Sundquist by the Swedish Research Council and by the National Heart, Lung, And Blood Institute of the National Institutes of Health, Award R01HL116381; grants awarded to J Sundquist by King Gustaf V and Queen Victoria’s Foundation of Freemasons; and The Ernhold Lundström Foundation, Research Funds at Skåne University Hospital and at Region Skåne, the Hulda Ahlmroth Foundation, and the Swedish Government under the LUA/ALF agreement awarded to A Gottsäter.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.