
Abstract

Lyme disease (LD), caused by the spirochete Borrelia burgdorferi, is one of the most prevalent tick-borne diseases worldwide. The acquisition of the infection occurs 7–28 days after experiencing a bite from an Ixodes scapularis tick, 1 with the classic of erythema migrans (EM) or “bull’s eye rash.” When diagnosis fails during the early course of the disease, B. burgdorferi may invade other organ tissues such as the heart and joints, causing carditis and arthritis, respectively.1,2 Of all LD syndromes, one of particular concern is carditis because of its association with morbidity and mortality. Lyme carditis (LC) was first reported in 1980. 3 LC is caused by direct invasion of myocardial tissue by spirochetes and an immunological host response causing lymphocyte inflammation. B. burgdorferi has a predisposition to cause inflammation of the atrioventricular (AV) node resulting in variable conduction abnormalities which can be seen in electrocardiograms (ECGs/EKGs), 4 such as atrioventricular conduction abnormalities (most common), right bundle branch block (RBBB), and left bundle branch block (LBBB). 3 Furthermore, cases of LC with widening of the QRS complex, AV dissociation, atrial fibrillation, ventricular dysfunction, fulminant myocarditis, and even cardiac arrest have been described.3–5 While LC is not commonly present during early LD, disseminated EM and LC may present concurrently within two weeks of tick attachment. 6 Furthermore, single EM concomitantly with an AV block has been also reported. 7 LC is reported to occur in 4–10% of untreated LD cases and is usually present 2–5 weeks after EM rash or onset of infection. 8 The aim of this study is to determine the frequency of abnormal ECG changes in patients with early LD seen in Stony Brook University Hospital (SBUH) which is the only major tertiary care medical center in Suffolk County, the area with the highest absolute number of LD cases reported in New York State.
A retrospective study was designed to identify cases of LD at SBUH between 2010–2016. SBUH is a 603-bed academic, tertiary medical center located in Suffolk County, Long Island, New York, USA. All patients with a discharge diagnosis of LD were identified by a search in the Electronic Medical Records (EMR) database of SBUH using International Classification of Diseases (ICD)-9 and ICD-10 codes. LD was defined either by the presence of EM rash, or two-tier serological confirmation by Western blot according to Center for Disease Control (CDC) criteria (at least two Immunoglobulin M [IgM] or five Immunoglobulin G [IgG] bands) and having being admitted to the hospital due to new diagnosis of LD. LC was defined as a case of LD with an abnormal ECG (AV block, right or left bundle branch abnormalities, new onset atrial fibrillation, T wave inversion, ST elevation and prolonged QT). Determination of LC was confirmed by either an infectious diseases specialist or a cardiologist. Demographics, past medical history, ECG and laboratory results were extracted from each patient’s chart. To identify risk factors, controls were included defined as LD with a normal ECG. Data were analyzed with STATA 12.1 (StataCorp, College Station, Texas, USA). This study was reviewed and approved by the Institutional Review Board (IRB# 834409) at SBUH.
Demographics, clinical features, laboratory and treatment outcomes on patients with Lyme carditis.
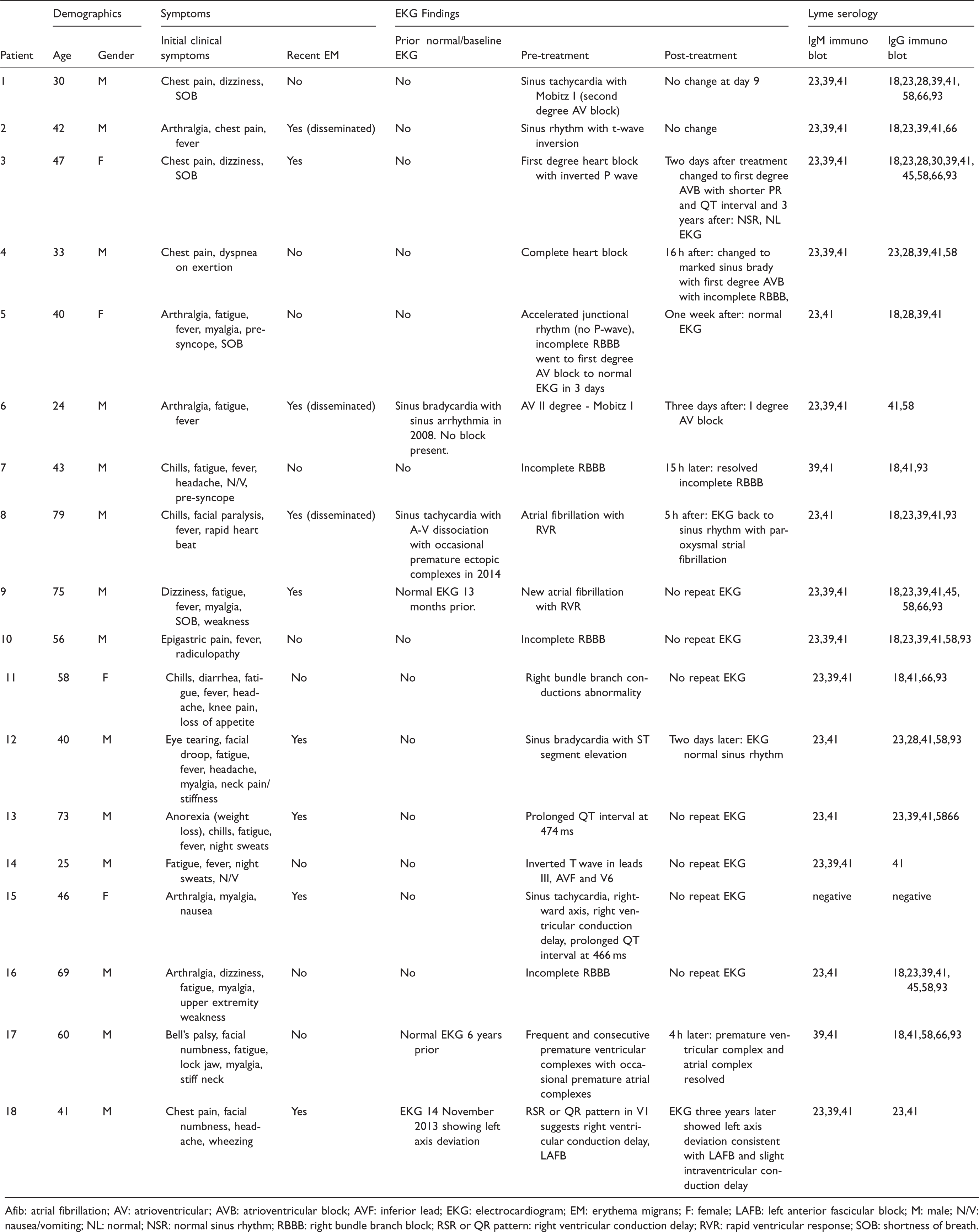
Afib: atrial fibrillation; AV: atrioventricular; AVB: atrioventricular block; AVF: inferior lead; EKG: electrocardiogram; EM: erythema migrans; F: female; LAFB: left anterior fascicular block; M: male; N/V: nausea/vomiting; NL: normal; NSR: normal sinus rhythm; RBBB: right bundle branch block; RSR or QR pattern: right ventricular conduction delay; RVR: rapid ventricular response; SOB: shortness of breath.
In the regression logistic model, antibiotics received prior to admission (odds ratio (OR) = 0.16, 95% confidence interval (CI): 0.02–0.96, p = 0.045) and arthralgia (OR = 4.74, 95% CI: 1.02–22.06; p = 0.047) were found to be statistically significantly associated with LC. The antibiotic regimen received before admission in the control group was a combination of cephalexin/bactrim (n = 3), doxycycline and cephalexin (n = 1), amoxicillin/clavulanic acid (n = 1), cephalexin alone (n = 1), levofloxacin (n = 2), and in the LC group was ciprofloxacin and doxycycline (n = 1), and ceftriaxone intravenously two days prior (n = 1). There was no mortality in either group. Also, the median number of days admitted to the hospital was significantly higher in the LC group compared to the control group (3 vs 0 days, p = 0.04).
Out of the 18 LC cases, nine had a localized or disseminated EM which correlates with the dissemination of the bacteria to other organs including the heart. However, half of them did not have a recent EM and their main complaints on presentation were shortness of breath, chest pain, or fatigue. While the severity of the infection, and the number of spirochetes present in the heart tissue may correlate with the occurrence of ECG abnormalities in humans, a strong correlation between degree of conduction disturbances, severity of cardiac inflammation, and the number of spirochetes in heart tissue was observed in non-human primates infected with B. burgdorferi; 9 which may be the reason why the prior use of antibiotics was less associated with LC in this study.
The findings of our study are important for several reasons. First, the description of ECG abnormalities in well-reported LD cases may help healthcare providers to suspect LD when a patient who lives in a hyperendemic LD area presents with unspecific ECG abnormalities. Second, the spectrum of ECG abnormalities in LC is unknown given the limited number of cases reported in the literature which are mostly complete AV blocks in need of a temporary pacemaker. Mild cases of LC may have not been reported due to several reasons including lack of ECG on presentation or mild symptoms that may not merit an ECG. Our study adds to the literature a greater spectrum of ECG abnormalities in LD which may be present in LC.
The spectrum of ECG abnormalities in LD may be broader than that previously suspected. Clinicians should be aware of these ECG abnormalities that may be a sign of LC in hyperendemic areas.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.