
Abstract
Background
The Comparison of Sacubitril–Valsartan versus Enalapril on Effect on NT-proBNP in Patients Stabilised from an Acute Heart Failure Episode (PIONEER-HF) trial demonstrated significant reductions in N-terminal pro-B-type natriuretic peptide. Our study explored the cost-effectiveness of the use of sacubitril-valsartan versus enalapril in acute decompensated heart failure from the Australian healthcare perspective.
Methods
A Markov model was designed using data from the PIONEER-HF trial to model the clinical progress and costs of patients over a lifetime time horizon. The model consisted of three health states: ‘alive and event-free’, ‘alive after non-fatal hospitalisation for acute decompensated heart failure’ or ‘dead’. Costs and utilities were estimated from published sources. The cost of sacubitril-valsartan (per the Australian pharmaceutical benefits schedule) was AU$7.08/day. Outcomes of interest were the incremental cost-effectiveness ratios in terms of cost per quality-adjusted life year gained and cost per year of life saved. Cost and benefits were discounted at 5.0% per annum.
Results
Compared to enalapril, sacubitril-valsartan was estimated to cost an additional AU$7464 (discounted) per person, but lead to 0.127 years of life saved (discounted) and 0.096 quality-adjusted life years gained (discounted) over a lifetime analysis. These equated to incremental cost-effectiveness ratios of AU$58,629/year of life saved (US$41,795, EU€58,629, GBP£32,001) and AU$77,889/quality-adjusted life year gained (US$55,526, EU€49,202, GBP£42,504). We have assumed a threshold of AU$50,000/quality-adjusted life year gained to suggest cost-effectiveness.
Conclusions
At its current acquisition price, sacubitril-valsartan in comparison to enalapril is not likely to be cost-effective in the management of acute decompensated heart failure in Australia. A price reduction of more than 25% would confer cost-effectiveness.
Introduction
In Australia, there were 173,000 hospitalisations due to heart failure (HF) in 2016, and every year, HF accounts for 1.6% of all hospitalisations. 1 Furthermore, the risks of one-year rehospitalisation and mortality following acute decompensated heart failure (ADHF) are significant, at 56% and 24%, respectively. 2 Therapeutic guidelines for the management of ADHF include the use of supplemental oxygen for desaturation, intravenous loop diuretics for cardiac decongestion and vasodilator/inotropic agents for haemodynamic compromise. 3
Sacubitril-valsartan is a first-in-class angiotensin receptor neprilysin inhibitor which simultaneously inhibits neprilysin and the renin angiotensin aldosterone system. Its efficacy in the context of symptomatic heart failure with reduced ejection fraction (HFrEF) compared to enalapril was demonstrated in the PARADIGM-HF (Prospective Comparison of ARNI with ACEi to Determine Impact on Global Mortality and Morbidity in Heart Failure) trial, in which benefits were observed for all-cause and cardiovascular mortality, risk of HF hospitalisation and reduction in symptoms and physical limitations from HF. 4 In addition, studies have shown that sacubitril-valsartan is cost-effective compared to enalapril for the treatment of chronic HF.5–7 In June 2017, the Australian pharmaceutical benefits scheme (PBS) listed sacubitril-valsartan for the treatment of patients with New York Heart Association (NYHA) class II–IV chronic HF. 8
The PIONEER-HF (Comparison of Sacubitril-Valsartan versus Enalapril on Effect on NT-proBNP in Patients Stabilised from an Acute Heart Failure Episode) trial assessed the efficacy and safety of sacubitril-valsartan compared to enalapril, after haemodynamic stabilisation, among patients who were hospitalised for ADHF. 9 In this study, 881 patients were randomly assigned to receive sacubitril-valsartan (target dose 97 mg sacubitril and 103 mg valsartan, twice daily) or enalapril (target dose 10 mg, twice daily). Participants were followed up for 8 weeks, and the primary outcome was the time-averaged proportional change in N-terminal pro-B-type natriuretic peptide (NT-proBNP) concentration from baseline, to weeks 4 and 8. The ratio of the geometric mean of values of NT-proBNP levels obtained at weeks 4 and 8 to the baseline value was 0.53 in the sacubitril-valsartan group compared to 0.75 in the enalapril group (percentage change −46.7% vs. −25.3%). 9
The aim of our study was to assess the cost-effectiveness of sacubitril-valsartan compared to enalapril, for the management of ADHF, from an Australian healthcare perspective.
Methods
Model structure and population
A decision analytic Markov model was developed to simulate and compare the downstream consequences of sacubitril-valsartan versus enalapril. The model consisted of three health states: ‘alive and event-free (no re-hospitalisation for ADHF)’, ‘alive after non-fatal hospitalisation for ADHF’ or ‘dead’ (Figure 1). The first health state was the residual of the other two health states. The model population comprised 1000 subjects profiled on the baseline characteristics of patients in PIONEER-HF. Thus, they had a starting median age of 61 years, signs and symptoms that led to a primary diagnosis of ADHF but were haemodynamically stable. Detailed characteristics are outlined elsewhere.
9
The first cycle length was 8 weeks to concur with the follow-up period of PIONEER-HF. This initial cycle allowed the model to account for latency in treatment effects over the 8-week period in lowering NT-proBNP levels. Subsequent cycles were one year in duration. The model time horizon was a lifetime (15 years), in line with the International Society for Pharmacoeconomics and Research Outcomes recommendations.
10
The outcomes of interest were net direct healthcare costs, quality adjusted life years (QALYs) saved, years of life saved (YoLS) and the incremental cost-effectiveness ratios (ICERs) in terms of cost per QALY gained and cost per YoLS. A discount rate of 5% per annum was applied to all outcomes in accordance with Australian guidelines.
11
A willingness to pay threshold of AU$50,000 per QALY gained was assumed to determine cost-effectiveness.
12
Markov model of the possible health states. Non-fatal hospitalisation (NHF) pertains to those who had a first non-fatal hospitalisation, but no subsequent hospitalisations. Once a second hospitalisation occurred, patients moved to the ‘rehospitalisation’ health state and were at risk of further hospitalisations and death.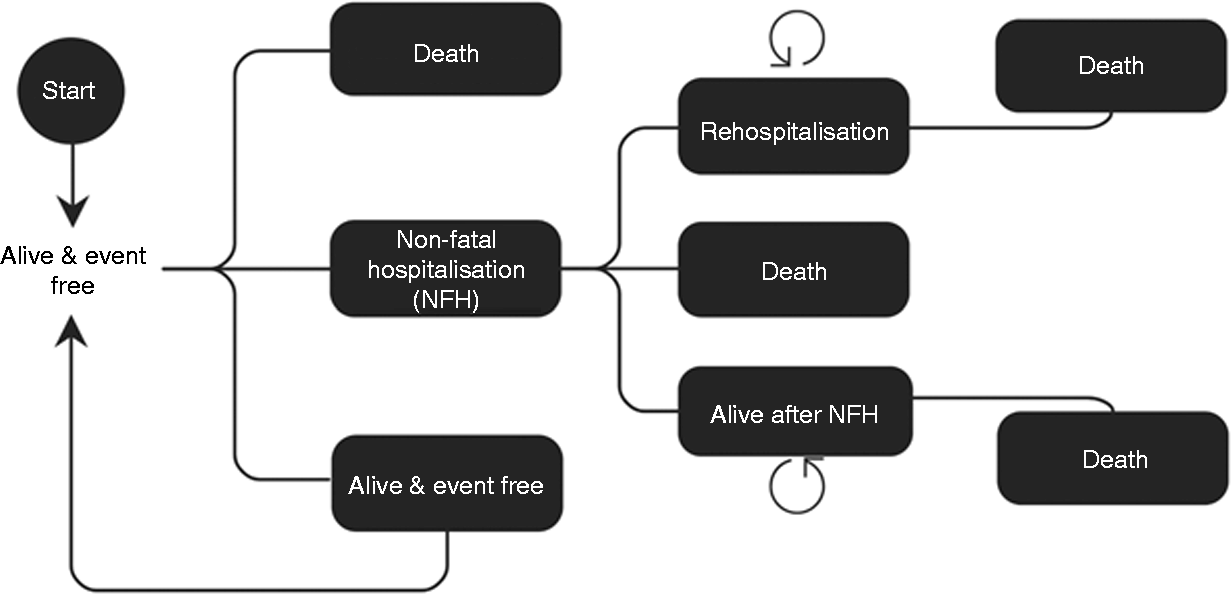
Correlating NT-proBNP with clinical outcomes
The primary outcome of PIONEER-HF was a change in the concentration of NT-proBNP over 8 weeks. To estimate the clinical impact of these changes, correlations between NT-proBNP levels and risks of rehospitalisation and mortality were derived from a study by Linssen et al., who assessed the prognostic value of NT-proBNP and BNP after HF hospitalisation. 13 The baseline characteristics of participants in PIONEER-HF and the study by Linssen et al. were similar. In particular, the median age of patients was 61 years (interquartile range (IQR) 51–71) and 71 years (standard deviation (SD) 11), respectively, and 28% and 39% were women, respectively. Baseline NT-proBNP levels were 2883 pg/ml (IQR 1610–5403) and 2536 pg/ml (IQR 1363–4917) in the enalapril and sacubitril-valsartan group, respectively, in PIONEER-HF and 2528 pg/ml (IQR 1289–5615) in Linssen et al. 9 The use of HF medications at baseline was higher in Linssen et al. compared to PIONEER-HF (angiotensin-converting enzyme inhibitors (ACEis) and/or angiotensin receptor blockers (ARBs), 82% vs. 48%; β-blockers, 67% vs. 60%; diuretics, 96% vs. 60%, respectively). Medication use in PIONEER-HF referred to previous use prior to study entry while patients included in Linssen had to be stable on standard HF medication prior to hospital discharge, thus accounting for the differences in medication use. Due to similarities in other baseline demographics, the multivariable adjusted probabilities reported by Linssen et al. were considered appropriate to correlate a given patient’s NT-proBNP concentration in PIONEER-HF with their probability of death and hospitalisation for HF.
As formulae for this correlation were unavailable and the data presented by Linssen et al. were in a graphical format, 174 data points were estimated using Plot Digitiser Ver. 2.6.8, 2015.
14
These data points were used to fit a logarithmic function to estimate the probability of death, or being ‘alive and event free’ for a given NT-proBNP level (see Supplementary Appendix 1). ‘Hospitalisation for HF’ reported by Linssen et al. did not distinguish between ‘fatal’ and ‘non-fatal’ hospitalisations. To determine transitions to our model health state ‘alive after non-fatal hospitalisation for ADHF’, the probability was estimated using the formulae below:
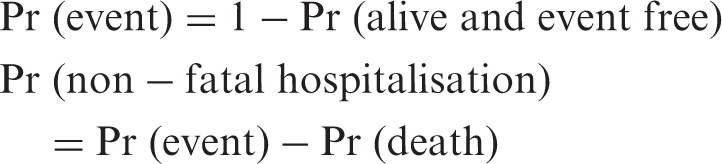
Linssen et al. measured NT-proBNP levels at the time of discharge and estimated the probability of these outcomes (‘alive and event free’ and ‘death’) over an 18-month follow-up period. The probabilities of non-fatal hospitalisation and death were converted to one-year estimates, in line with our model cycle length, using the formulae of Briggs et al. 15
Transition probabilities
‘Alive and event free’
All subjects began the model in the ‘alive and event free’ health state. From here, they were at risk of having a non-fatal HF hospitalisation or dying, extrapolated from data from PIONEER-HF (discussed above). To account for any latency in treatment effects, transition probabilities for non-fatal hospitalisation and death in cycle 1 were assumed to be the same as patients’ baseline risk in PIONEER-HF estimated from their baseline NT-proBNP values. 9 For cycle 2, transition probabilities were estimated using the derived 8-week values of NT-proBNP from PIONEER-HF. 9 In all subsequent cycles, transition probabilities were modelled on expected age-related increases in risk derived from Australian mortality data. 16 In particular, the risk of death was increased using all-cause mortality data. Due to lack of data on the age-related trends of non-fatal hospitalisation for ADHF, we assumed these changes were the same as the age-related trends for mortality from HF. 16
‘Alive after non-fatal hospitalisation’
Subjects could only occupy this health state from cycle 2 onwards (Figure 1). Having survived the initial non-fatal hospitalisation, subjects were at risk of rehospitalisation (from any cause) or death. Subjects continued to be at risk of rehospitalisation until death. Transition probabilities were increased to reflect the greater risk of a secondary event as per the findings from a systematic review and meta-analysis by Al-Omary et al. assessing mortality and readmission following HF hospitalisation in Australia. 2 The one-year risk of rehospitalisation for any cause after an ADHF hospitalisation was 0.56 (95% confidence interval (CI) 0.39–0.72) and the one-year probability of mortality was 0.25 (95% CI 0.22–0.29). 2 As described above, after cycle 2, risks were increased according to age-related trends with each subsequent cycle.
Utilities
The baseline utility value ascribed to the health state ‘alive and event free’ was 0.752. 17 Griffin et al. employed this value to reflect the utility of those with ADHF and chronic HF patients. 17 Such an assumption was reasonable in the context of PIONEER-HF, as patients in that study had HFrEF. Utility decrements for ADHF hospitalisations were also sourced from Griffin et al. and specified for 3 months. As cycle lengths were one year in duration, for every acute hospitalisation event, a utility decrement of 0.064 was applied for 3 months before returning to the baseline utility value of 0.752 for the remaining 9 months – giving a weighted average utility of 0.736 for the cycle. 17 The utility value was assumed to have been restored back to the baseline value of 0.752 in the following cycle.
Costs
Cost of treatment
The cost of sacubitril-valsartan combination therapy and enalapril was obtained from the Australian PBS, which subsidises medications for Australians. Assuming the dosing regimen employed in PIONEER-HF, the acquisition price of sacubitril-valsartan was AU$198.10 for 56 units. 18 If administered twice daily, as per PIONEER-HF, 9 sacubitril-valsartan was assumed to cost AU$7.08 per day or AU$2584 per year. The cost of enalapril is listed at AU$14.42 for 30 units on the PBS. 19 This equated to a cost of AU$0.96 per day or AU$351 per year, assuming enalapril was taken twice daily, as per PIONEER-HF. 9 Treatment costs were applied in the model as long as subjects remained alive.
Cost of disease
The acute costs of hospitalisation for ADHF and death were obtained from the Australian refined diagnosis related groups (AR-DRGs) data. 20 Costs were listed for the year 2015–2016, and were updated to 2018–2019 values using the Australian total health price index (HPI). 21 For HF hospitalisations, the weighted average cost was AU$9245. For deaths, the weighted-average cost was AU$3817 (for cardiovascular-related death). The ongoing chronic costs of HF management were as per Ford et al., who listed the ongoing cost of HF without hospitalisation for each NYHA class. 22 Using the distribution of NYHA class patients in PIONEER-HF at baseline, this cost was adjusted to an annual weighted average value and updated for inflation from the source year of 2012 to 2018–2019 using the HPI, to yield a value of AU$220. 21 It was conservatively assumed that 50% of deaths occurred in hospital, and therefore only 50% of deaths incurred hospitalisation costs. 20 All costs are reported in Australian dollars for 2018–2019.
Sensitivity analyses
To quantify the level of confidence in the ICERs and test uncertainty in key model input parameters, univariate and probabilistic sensitivity analyses (PSA) were performed. Key parameters in univariate analysis were varied as per Supplementary Appendix 2. The PSA consisted of a second order Monte Carlo simulation with 10,000 iterations. Input parameters, ranges and distributions are included in Supplementary Appendix 2. In the primary PSA, all input parameters were varied except for baseline NT-proBNP levels, which remained static. In a secondary PSA, the baseline NT-proBNP level for enalapril was varied according to the IQR reported by PIONEER-HF 9 using a uniform distribution. The baseline NT-proBNP level for sacubitril-valsartan was adjusted according to the baseline NT-proBNP level for enalapril and a proportional reduction of 12% estimated from the baseline median values for each treatment arm. Scenario analyses were performed to test model assumptions and identify key input parameters. Scenario analyses included reducing the discount rate to 0% and 3.5% in line with the National Institute for Health and Care Excellence (NICE) recommendations, 23 omitting age-related increases in risks, altering the model time horizon (to 5 and 10 years), varying the baseline NT-proBNP levels, assuming sacubitril-valsartan and enalapril decreased NT-proBNP levels over one year, and reducing the acquisition cost of sacubitril-valsartan.
Results
Base case
Base case results for 1000 patients with ADHF treated with sacubitril-valsartan compared to enalapril, followed-up over their lifetime.
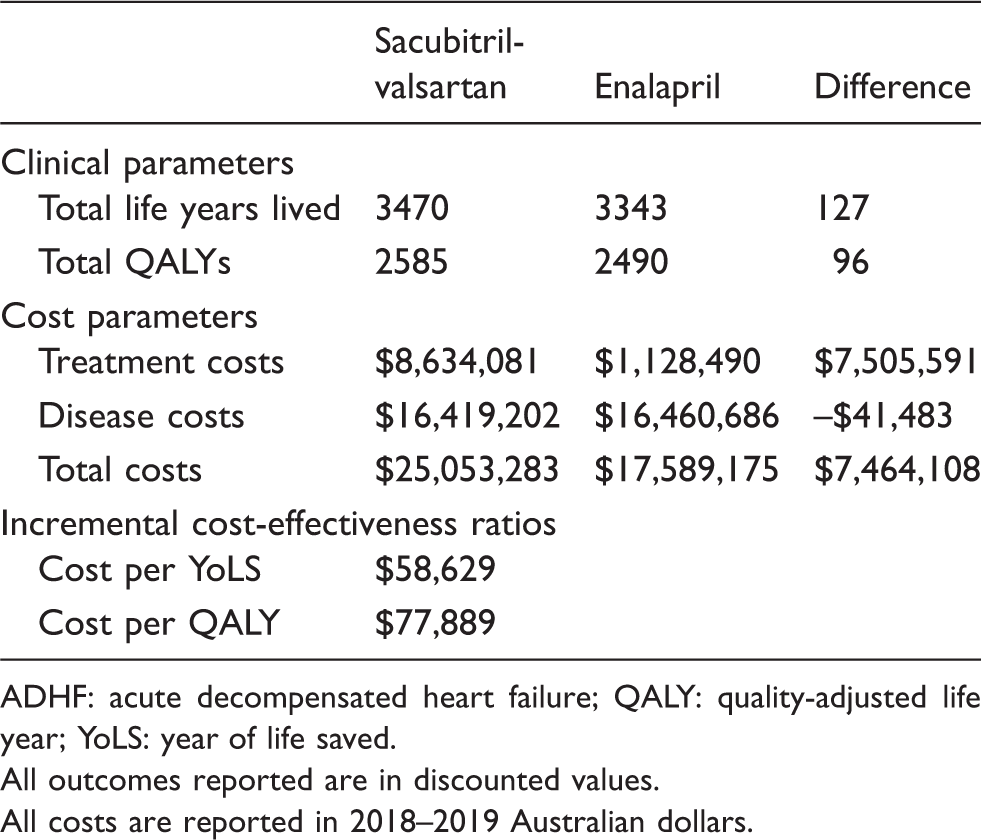
ADHF: acute decompensated heart failure; QALY: quality-adjusted life year; YoLS: year of life saved.
All outcomes reported are in discounted values.
All costs are reported in 2018–2019 Australian dollars.
Univariate sensitivity analyses
The univariate sensitivity analyses results are shown in Supplementary Appendix 3, which demonstrates the ICER in terms of cost per QALY. The analysis was most sensitive to the cost of sacubitril-valsartan as well as the percentage change in NT-proBNP in the sacubitril-valsartan treatment arm. When the percentage change in NT-proBNP was varied by ± 15% of the base case (to –39.7% and –53.7%), to mimic variable drug efficacy, the cost per QALY was AU$105,634 and AU$59,770, respectively. The treatment effect and change in NT-proBNP was more influential on the ICER than the median NT-proBNP level at random assignment. This indicates that the severity of ADHF, which PIONEER-HF approximates with NT-proBNP at random assignment, 9 is less important than the treatment effect to lower NT-proBNP levels, for achieving cost-effectiveness.
Scenario analyses
Scenario analyses.
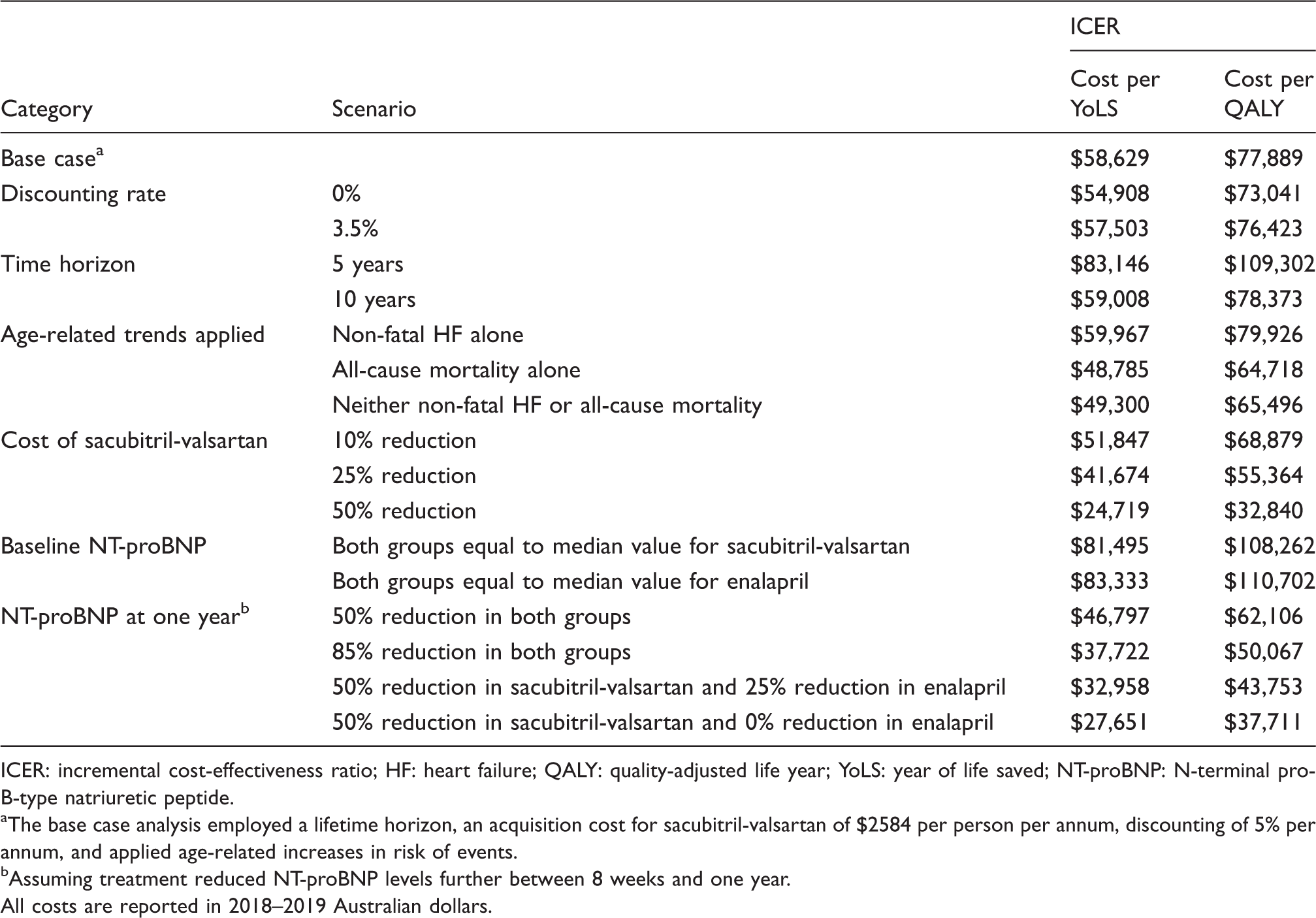
ICER: incremental cost-effectiveness ratio; HF: heart failure; QALY: quality-adjusted life year; YoLS: year of life saved; NT-proBNP: N-terminal pro-B-type natriuretic peptide.
The base case analysis employed a lifetime horizon, an acquisition cost for sacubitril-valsartan of $2584 per person per annum, discounting of 5% per annum, and applied age-related increases in risk of events.
Assuming treatment reduced NT-proBNP levels further between 8 weeks and one year.
All costs are reported in 2018–2019 Australian dollars.
Probabilistic sensitivity analyses
The results of the PSA demonstrated that sacubitril-valsartan therapy compared to enalapril was cost-effective in less than 5% of iterations, assuming a cost-effectiveness threshold of AU$50,000 per QALY gained (see Supplementary Appendix 4). In the primary PSA, when NT-proBNP levels were static, the 2.5th and 97.5th percentiles were AU$47,914 and AU$116,866, respectively. In the secondary PSA, the respective values were AU$48,019 and AU$120,640.
Discussion
To the best of our knowledge, this is the first cost-effectiveness analysis of sacubitril-valsartan versus enalapril in patients with ADHF. Our results indicate that the use of sacubitril-valsartan is not likely to be cost-effective when compared to enalapril in ADHF patients in Australia. The base case results demonstrated an ICER of AU$77,889, which exceeds the commonly accepted willingness to pay threshold of AU$50,000 per QALY. 12 Similar findings were obtained when a variety of scenarios were assessed. However, there is no formally published value for cost-effectiveness in Australia. The choosing interventions that are cost-effective (CHOICE) programme of the World Health Organization (WHO) defines interventions with a cost per QALY less than one gross domestic product (GDP) per capita as very cost-effective, between one and three GDP per capita as cost-effective and over three times the GDP per capita as not cost-effective. 24 Given Australia’s GDP per capita is US$52,003 (or AU$72,965 assuming 1 US$ = 1.40 AU$ on 12 April 2019),25,26 a cost per QALY of less than AU$72,965 would denote a ‘very cost-effective’ intervention. Sacubitril-valsartan would therefore be considered very cost-effective as opposed to enalapril for the management of ADHF.
While this is the first evaluation of sacubitril-valsartan versus enalapril in the context of ADHF, cost-effective analyses have been conducted based on findings from the PARADIGM-HF trial, which evaluated the use of sacubitril-valsartan for chronic HFrEF. Benefits were observed for all-cause and cardiovascular mortality, the risk of HF hospitalisation and reduction in symptoms and physical limitations from HF. A recent Australian study found that sacubitril-valsartan is cost-effective compared to enalapril, with an ICER of AU$40,513 per QALY gained. 5 Similar findings have been reported internationally.6,7 Our study employed the primary outcome of PIONEER-HF, a reduction in NT-proBNP concentration, to assess drug efficacy over 8 weeks. In contrast, the PARADIGM-HF trial demonstrated benefits in HF hospitalisation and death over approximately 50 months. Indeed, PARADIGM-HF was terminated early due to the overwhelming benefit for cardiovascular mortality. 4 NT-proBNP concentration is a surrogate biomarker increasingly used in prognostication and risk stratification of HF patients, 27 but not a clinical endpoint, and it was assessed over a short duration in PIONEER-HF. 9
One of the most influential parameters on the ICER was the cost of sacubitril-valsartan. To date, the annual cost of sacubitril-valsartan twice a day, at a dose of 97 mg/103 mg, respectively, as per PIONEER-HF, 9 is AU$2548. A price reduction of more than 25% would be required for sacubitril-valsartan to meet Australia’s cost-effectiveness criteria of AU$50,000 per QALY gained.
Baseline NT-proBNP values for patients with ADHF were also highly influential on the calculated ICERs. The median baseline NT-proBNP was 2883 pg/mL in the enalapril group and 12% lower (2536 pg/mL) in the sacubitril-valsartan group. In the univariate sensitivity analysis, baseline NT-proBNP in the enalapril group was altered according to the lower and upper limits of the IQR reported by PIONEER-HF (1610 and 5403 pg/mL). The NT-proBNP for the sacubitril-valsartan group was assumed to be 12% lower than the corresponding enalapril value. This resulted in a cost per QALY ranging from AU$70,274 to AU$86,345 for the lower and upper limits, respectively. A further scenario analysis was conducted in which both treatment groups were assigned the same NT-proBNP at random assignment. Using the enalapril median value of 2883 pg/mL resulted in a cost per QALY of AU$110,702, while employing the sacubitril-valsartan median value of 2536 pg/mL resulted in a cost per QALY of AU$108,262. Therefore, cost-effectiveness appears more likely to be achieved if the absolute value of NT-proBNP is lower in the sacubitril-valsartan group at random assignment or the relative difference in baseline NT-proBNP levels between the two treatment arms is larger.
The effects of alternative dosing regimens were not assessed in our analyses. Currently, sacubitril-valsartan is also listed on the PBS in 49 mg/51 mg and 24 mg/26 mg formulations. 18 It is therefore unknown whether reduced dosing targets would produce cost-effective results. However, the effects of a dose reduction could be conservatively estimated to have a proportionally lower efficacy in reducing NT-proBNP levels. Our analysis assessed the effects of varying efficacy by altering the percentage change in NT-proBNP by ±15% for the sacubitril-valsartan treatment group. Reductions in efficacy translate to reduced cost-effectiveness (AU$105,634 per QALY gained) while the opposite is seen for improved efficacy (AU$59,770 per QALY gained).
Limitations
There is a number of limitations that warrant mention. First, our analysis used data obtained from Linssen et al. to correlate NT-proBNP to a probability of rehospitalisation and mortality. 13 Baseline risk (determined by NT-proBNP level at random assignment in PIONEER-HF) were approximately 4% for non-fatal HF hospitalisation and 2% for mortality, for both treatment groups. A study conducted by Choi et al. demonstrated an inhospital mortality rate (median stay of 10 days) for ADHF admissions for those with a background of HFrEF at 5.7%. 28 Similar results were obtained in an Argentinian study in 2004, which observed an inhospital mortality rate of 4.7%. 29 The lower rates observed in our study are consistent with our study population being haemodynamically stable at discharge, and estimated rates post-discharge. After 8 weeks, the calculated one-year risks of HF hospitalisation and mortality were 21.9% and 12.2% in the enalapril arm and 20.3% and 10.98% in the sacubitril-valsartan group, as per the change in NT-proBNP observed in PIONEER-HF. Literature on the accuracy of these values is scarce. A multicentre cohort study identified the 30-day risk of all-cause hospitalisation and mortality following an admission for ADHF increased to 15.3% and 4.3%, respectively. 30 Nevertheless, the prognostic value of NT-proBNP in ADHF patients has been well established, 31–38 and was highlighted in a scientific statement from the American Heart Association in 2017. 37 The I-Preserve study demonstrated that, after adjustment, a 1000 pg/mL increase in NT-proBNP from baseline to 6 months resulted in a doubling of risk of cardiovascular hospitalisation or cardiovascular death (hazard ratio (HR) 2.01, 95% CI 1.50–2.61). 38 The inverse was seen with a decrease of 1000 pg/mL in NT-proBNP (HR 0.73, 95% CI 0.53–1.02). In addition, a recent study by Salah et al. showed that for every twofold increase in NT-proBNP at discharge, the multivariate adjusted HR for 6-month all-cause mortality was 1.71 for ADHF with preserved ejection fraction and 1.61 for HFrEF. For the composite outcome of cardiovascular readmission/all-cause mortality, the respective values were 1.18 and 1.26. 36 Similarly, the study by Linssen et al. demonstrated that doubling of NT-proBNP at discharge resulted in a multivariate adjusted odds ratio for both outcomes of all-cause mortality and HF hospitalisation/all-cause mortality of 1.45 (over 18 months). 13
Second, our modelled analysis assumed perfect compliance to HF medication over a patient’s lifetime, a feature that is likely not to be true in real-world practice. PIONEER-HF found 20% of patients in each treatment group had discontinued treatment after 8 weeks, mostly as a result of an adverse event. 9 Due to the equal proportion of adverse events reported in each treatment arm, these were not included in our model. However, the efficacy of any neurohormonal agent for ADHF over a lifetime model is affected by compliance, which in turn alters re-admission rates and therefore the ICERs that are obtained.
Finally the model conservatively assumed that the beneficial effects of sacubitril-valsartan in reducing NT-proBNP levels, and possibly the pathological progression of disease in ADHF, ceased after 8 weeks. After this point, the difference in risk was maintained but age-related trends affected the probabilities of mortality and hospitalisation. PARADIGM-HF demonstrated the superiority of sacubitril-valsartan over enalapril in reducing mortality from cardiovascular and all causes, yet poorly evaluated the incremental effects of the non-fatal progression of HF. Another analysis conducted by Packer et al. found that fewer sacubitril-valsartan patients, as compared to enalapril, required follow-up intensive care treatment, cardiac transplantation and 23% fewer hospitalisations for worsening of HF over 50 months. 39 That study was terminated early due to the overwhelming evidence of benefit in cardiovascular mortality. These findings are suggestive of an add-on benefit conferred by continued therapy with sacubitril-valsartan, which is likely to improve cost-effectiveness. In our scenario analyses, reducing NT-proBNP levels in both treatment arms by a further 50% over one year improved the ICER, but sacubitril-valsartan was still not considered cost-effective. However, increasing benefits by applying a 85% reduction in both treatment arms between 8 weeks and one year met cost-effectiveness thresholds. Similarly, cost-effectiveness was achieved if the effects of sacubitril-valsartan on reducing NT-proBNP levels over one year were progressively greater than those elicited by enalapril.
Conclusion
Based on its current acquisition price, sacubitril-valsartan compared to enalapril is unlikely to be cost-effective for the management of ADHF in an Australian healthcare setting. A price reduction of more than 25% would confer cost-effectiveness.
Supplemental Material
CPR878953 Supplemental Material - Supplemental material for Sacubitril-valsartan versus enalapril for acute decompensated heart failure: a cost-effectiveness analysis
Supplemental material, CPR878953 Supplemental Material for Sacubitril-valsartan versus enalapril for acute decompensated heart failure: a cost-effectiveness analysis by Kanila Perera, Zanfina Ademi, Danny Liew and Ella Zomer in European Journal of Preventive Cardiology
Footnotes
Author contribution
DL conceived the idea and DL, EZ and ZA contributed to the design of the work. DL, EZ, KP and ZA contributed to the acquisition, analysis or interpretation of data for the work. KP drafted the manuscript. DL, EZ and ZA critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DL reports grants and personal fees from Abbvie, Astellas, AstraZeneca, Bristol-Myers Squibb, Novartis, Pfizer and Sanofi, grants from Amgen, CSL-Behring and Shire, and personal fees from Bayer, outside the submitted work during the past 36 months prior to submission; EZ reports grants from Amgen, AstraZeneca and Shire, and grants and personal fees from Pfizer, outside the submitted work during the past 36 months prior to submission; KP and ZA have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.