
Abstract
Aims
Obesity carries significant risk for unfavorable ventricular remodeling and subsequent heart failure (HF) development, although the association between abdominal fat distribution and subclinical ventricular dysfunction is unclear. This study aimed to compare the subcutaneous and visceral abdominal adiposity with the risk of decreased ventricular strain.
Methods
We included 340 participants without overt cardiac disease who underwent laboratory testing, abdominal computed tomographic examination, and speckle-tracking echocardiography. Abdominal adiposity was quantitatively assessed as visceral fat area (VFA) and subcutaneous fat area (SFA) at the level of the umbilicus. Speckle-tracking echocardiography was performed to assess left ventricular global longitudinal strain (LVGLS) and right ventricular free-wall longitudinal strain (RVLS).
Results
Mean age was 56 ± 9 years, and 244 of the participants (72%) were male. The mean LVGLS and RVLS were −19.1 ± 3.0% and −25.0 ± 4.1%, respectively. Both VFA and SFA correlated with LVGLS (r = 0.46 and r = 0.15, both p < 0.01) and RVLS (r = 0.38 and r = 0.12, both p < 0.05), demonstrating a stronger correlation between VFA and ventricular strain. Multivariable analysis showed that VFA was significantly associated with LVGLS and RVLS, independent of traditional cardiovascular risk factors as well as pertinent laboratory and echocardiographic parameters (both p < 0.05), whereas SFA was not. Serum adiponectin level was correlated with LVGLS (r = –0.34, p < 0.001) and RVLS (r = –0.25, p < 0.001), although it lost statistical significance following multivariable adjustment.
Conclusion
In a sample of the general population, VFA, but not SFA, accumulation was significantly associated with decreased LV and RV strain, an association that may be involved in the increased risk of HF in obese individuals.
Introduction
The prevalence of obesity and overweight has increased worldwide over the past few decades, now affecting nearly three-fourths of US adults. 1 These conditions are associated with an excess of cardiovascular risk factors and carry significantly increased risk for almost all cardiovascular diseases, particularly heart failure (HF) development.2–4 Although body mass index (BMI) has been a convenient and simple index for obesity and overweight, it is difficult to define these conditions by BMI alone since they are remarkably heterogeneous, with varying cardiovascular manifestations across individuals. Recently, particular attention has been given to patterns of body fat distribution and their impact on left ventricular (LV) morphology and functional alteration, and incidence of HF. Increased visceral fat was significantly associated with concentric LV remodeling, 5 diastolic dysfunction, 6 and subsequent HF development, 7 independent of traditional cardiovascular risk factors.
Although survival after the onset of HF has improved due to the development of various medications and device therapies, the mortality remains high. 1 These observations underscore the need for earlier detection of individuals at higher risk for HF. Furthermore, recent studies have demonstrated the independent prognostic value of right ventricular (RV) function in various HF settings.8–10 However, due to the anatomic complexity of the RV, it is difficult to accurately assess chamber function utilizing conventional two-dimensional echocardiography. Longitudinal strain with speckle-tracking echocardiography, a measure of the myocardial systolic deformation over the longitudinal axis, is emerging as an important tool to detect early RV as well as LV dysfunction, and is more sensitive than conventional echocardiographic parameters.11–13
The possible association between abdominal fat distribution and subclinical ventricular dysfunction has not been evaluated in the general population. The aim of the present study was to investigate whether increased visceral adiposity is associated with decreased LV and RV strain in a community-based cohort without overt cardiac disease, also taking into consideration pertinent laboratory parameters, including adipokines.
Methods
Study population
We initially enrolled 383 consecutive participants who voluntarily underwent extensive cardiovascular health check-up, including laboratory test, abdominal computed tomography (CT), and two-dimensional echocardiography. Our clinic provides an extensive health check-up for the promotion of health and prevention of cardiovascular disease; these systems, called “Kenshin”, are common in Japan. All tests were performed on the same day in the University of Tokyo Hospital between June 2018 and February 2019. Among all, participants who met the following criteria were excluded: 1) history of coronary artery disease (N = 8), 2) atrial fibrillation (N = 4), 3) LV ejection fraction <50% (N = 5) and 4) inadequate image quality or incomplete assessment of echocardiographic examination (N = 26). None of the participants had significant valvular diseases. The final population for this study consisted of 340 participants (244 men, mean age 56 years). This study was approved by the institutional ethics committee of the University of Tokyo. Written informed consent was obtained from all study participants.
Risk factor assessment and laboratory examination
Hypertension was defined as systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or the use of antihypertensive drugs. Diabetes mellitus was defined as fasting glucose ≥126 mg/dl or the use of insulin or hypoglycemic agents. Hypercholesterolemia was defined as total serum cholesterol >240 mg/dl or the use of lipid-lowering medications. BMI was calculated as body weight (kg) divided by height squared (m2).
Venous blood samples were collected between 8:00 a.m. and 10:00 a.m., following a 12-hour overnight fast. All blood samples were collected in the sitting position and measurements included serum fasting glucose, total cholesterol, low-density lipoprotein cholesterol, and high-density lipoprotein cholesterol. Serum C-reactive protein (CRP) was measured using the slide latex agglutination test and enzyme-linked immunosorbent assay. Serum adiponectin was measured using the Human Adiponectin Latex Kit (Eiken Chemical Co., Ltd, Tokyo, Japan) and the values were analyzed using an automatic clinical chemistry analyzer, LABOSPECT 008 (Hitachi High-Tech Co., Tokyo, Japan).
Assessment of abdominal adiposity
Abdominal adiposity was assessed as visceral fat area (VFA) and subcutaneous fat area (SFA), both of which were quantitatively measured by CT conducted at the level of the umbilicus, as previously reported. 14 The CT examination was performed using a 128-slice dual-layer spectral-detector CT scanner (IQon Spectral CT, Phillips Healthcare, The Netherlands) with a thickness of 1.25 mm, and tube voltage of 120 kV. The area of abdominal fat was defined as the sum of the intraperitoneal fat area with CT density ranging from −190 to −30 Hounsfield units, 15 and abdominal adipose tissue was separated into visceral and subcutaneous compartments.
Echocardiographic examination
Two-dimensional echocardiography
Transthoracic echocardiography was performed using a commercially available system (Toshiba Aplio, Toshiba Medical System Corp, Japan). All images were acquired according to a standardized protocol by trained and registered cardiac sonographers who were blinded to all other clinical information. The dimensions of the cardiac chambers were measured in the standard manner. 16 LV mass was calculated by a validated Devereux’s formula 17 : LV mass = 0.8 (1.04 [(SWT + LVEDD + PWT) 3 – LVEDD 3 ]) + 0.6, where SWT = LV end-diastolic septal wall thickness, LVEDD = LV end-diastolic diameter, and PWT = LV end-diastolic posterior wall thickness. Left atrial (LA) volume was measured from the apical two- and four-chamber views using the biplane Simpson’s rule. 18 LV mass and LA volume were indexed for body surface area.
LV diastolic parameters were assessed in accordance with current guidelines. 18 Briefly, the peak velocities of the early (E-wave) and late (A-wave) phases of the mitral inflow pattern from Doppler recordings were measured in the apical four-chamber view and their ratio (E/A) was calculated. The peak early diastolic velocity of the mitral annulus (e’) was calculated by averaging septal and lateral measurements obtained using tissue Doppler imaging in the apical four-chamber view. The ratio of E to e’ (E/e’) was then calculated.
Standard echocardiographic measurements of RV size and contractility were also performed according to current guidelines. 16 RV end-diastolic area and end-systolic area were obtained from the apical four-chamber view, and RV fractional area change (RVFAC) was calculated utilizing the following formula: (RV end-diastolic area − RV end-systolic area)/RV end-diastolic area × 100. The tricuspid annular plane systolic excursion (TAPSE) was also recorded with M-mode echocardiography through the lateral tricuspid annulus by calculating the amount of longitudinal motion of the annulus at peak systole.
Speckle-tracking echocardiography
Speckle-tracking analysis was performed off-line using vendor-independent and commercially available software (2D Cardiac Performance Analysis, Tomtec Imaging Systems, Germany). Semi-automated border detection was performed, and LV and RV borders were tracked throughout the cardiac cycle. Manual correction was performed in case of inadequate endocardial detection. LV global longitudinal strain (LVGLS) was obtained by averaging all segmental strain values from all three apical views, including the four-chamber, two-chamber, and long-axis views. 12 RV free-wall longitudinal strain (RVLS) was evaluated by longitudinal peak systolic strain on the RV free wall acquired from the apical four-chamber view. 13 According to the definition of strain, negative strain denotes shortening for LV and RV, which indicates that increasing absolute values represent a better ventricular function. Excellent correlations were observed in the inter- and intra-observer variabilities of LVGLS and RVLS in 15 randomly selected participants; r = 0.93 and r = 0.94 for LVGLS, and r = 0.94 and r = 0.93 for RVLS. In the Bland–Altman analysis, the inter- and intra-observer variabilities were −0.6 ± 1.3% and 0.2 ± 1.4% for LVGLS, and −1.0 ± 2.5% and −0.3 ± 2.6% for RVLS (mean ± 1.96 standard deviation, respectively).
Statistical analysis
Categorical variables are presented as numbers and frequencies (%), and continuous variables are presented as means ± standard deviations or median and interquartile range, as appropriate. Univariable correlations between variables were evaluated by Pearson’s correlation coefficients (r). Univariable and multivariable linear regression analyses were conducted to evaluate the association of abdominal adiposity (SFA and VFA) with conventional echocardiographic parameters, including E/e’, RVFAC, and TAPSE, and ventricular strain in four sequential models, respectively, as follows: Model 1: adjustment for age and sex; Model 2: adjustment for age, sex, systolic blood pressure, antihypertensive medication use, diabetes mellitus, hypercholesterolemia, and smoking status; Model 3: adjustment as in Model 2 plus pertinent echocardiographic parameters including LV mass index and E/e’; Model 4: adjustment as in Model 3 plus serum CRP and adiponectin levels. For the RV parameters, additional adjustment for LVGLS was performed (Model 5). A value of p < 0.05 was considered significant. Statistical analyses were performed using JMP 14 software (SAS Institute, Cary, NC, USA).
Results
Baseline characteristics of the study population
Characteristics of the study population.
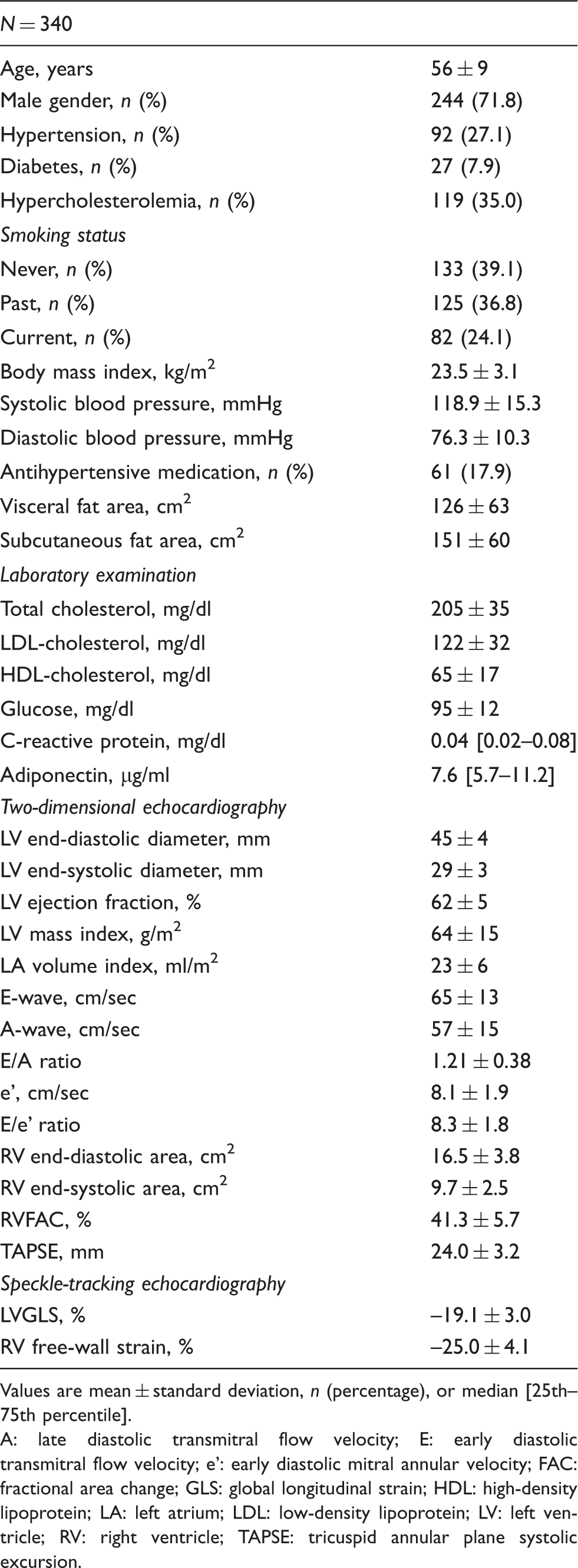
Values are mean ± standard deviation, n (percentage), or median [25th–75th percentile].
A: late diastolic transmitral flow velocity; E: early diastolic transmitral flow velocity; e’: early diastolic mitral annular velocity; FAC: fractional area change; GLS: global longitudinal strain; HDL: high-density lipoprotein; LA: left atrium; LDL: low-density lipoprotein; LV: left ventricle; RV: right ventricle; TAPSE: tricuspid annular plane systolic excursion.
Abdominal adiposity and LV performance
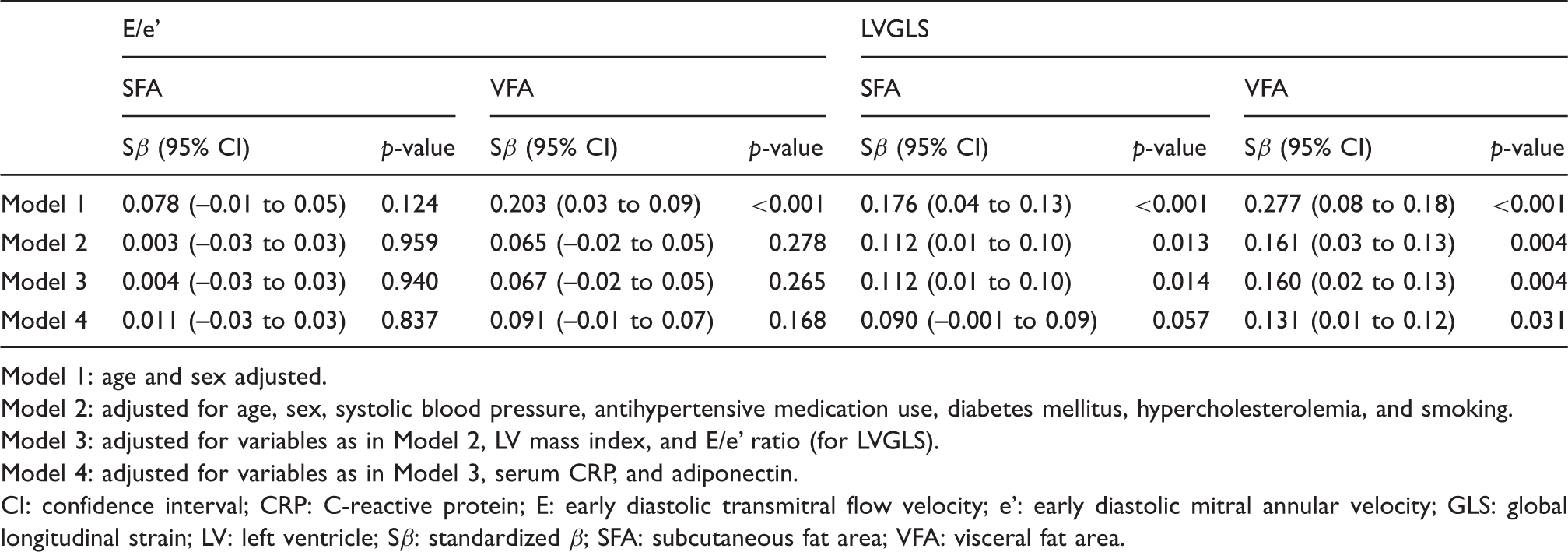
The association between abdominal adiposity and LVGLS is shown in Figure 1(a) and (b). Although both VFA (r = 0.46, p < 0.001) and SFA (r = 0.15, p = 0.006) were correlated with LVGLS, a stronger association was observed in VFA. VFA was associated with LVGLS in the age- and sex-adjusted model (Table 2, Model 1). Following multivariable linear regression analyses adjusted for age, sex, and traditional cardiovascular risk factors, the association between VFA and LVGLS persisted (Table 2, Model 2). Adjustment for echocardiographic parameters (LV mass index and E/e’ ratio) did not change the independent association between VFA and LVGLS (Table 2, Model 3). Even after adjustment for laboratory parameters, including CRP and adiponectin, VFA remained significantly associated with LVGLS (standardized β = 0.131, p = 0.031; Table 2, Model 4). On the other hand, SFA was no longer significantly associated with LVGLS following a full adjustment (standardized β = 0.090, p = 0.057). As for the diastolic parameter, VFA, but not SFA, was associated with E/e’ in the age- and sex-adjusted model (also Table 2, Model 1). However, both VFA and SFA were not associated with E/e’ following adjustment for traditional cardiovascular risk factors (Table 2, Model 2).
Scatter plot between abdominal adiposity and ventricular strain. (a) VFA and LVGLS, (b) SFA and LVGLS, (c) VFA and RVLS and (d) SFA and RVLS. Association of abdominal adiposity with E/e’ and LVGLS. Model 1: age and sex adjusted. Model 2: adjusted for age, sex, systolic blood pressure, antihypertensive medication use, diabetes mellitus, hypercholesterolemia, and smoking. Model 3: adjusted for variables as in Model 2, LV mass index, and E/e’ ratio (for LVGLS). Model 4: adjusted for variables as in Model 3, serum CRP, and adiponectin. CI: confidence interval; CRP: C-reactive protein; E: early diastolic transmitral flow velocity; e’: early diastolic mitral annular velocity; GLS: global longitudinal strain; LV: left ventricle; Sβ: standardized β; SFA: subcutaneous fat area; VFA: visceral fat area.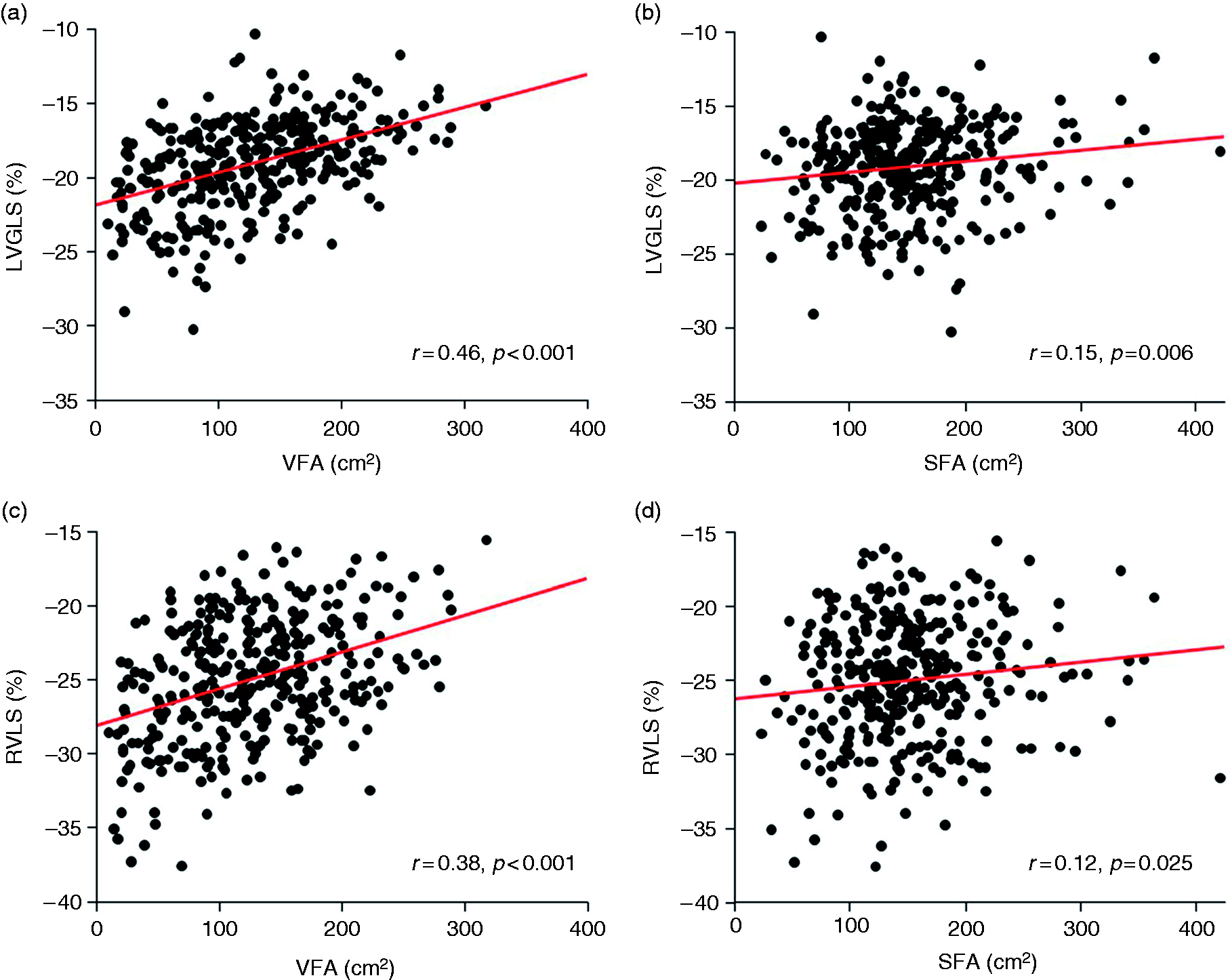
Abdominal adiposity and RV performance
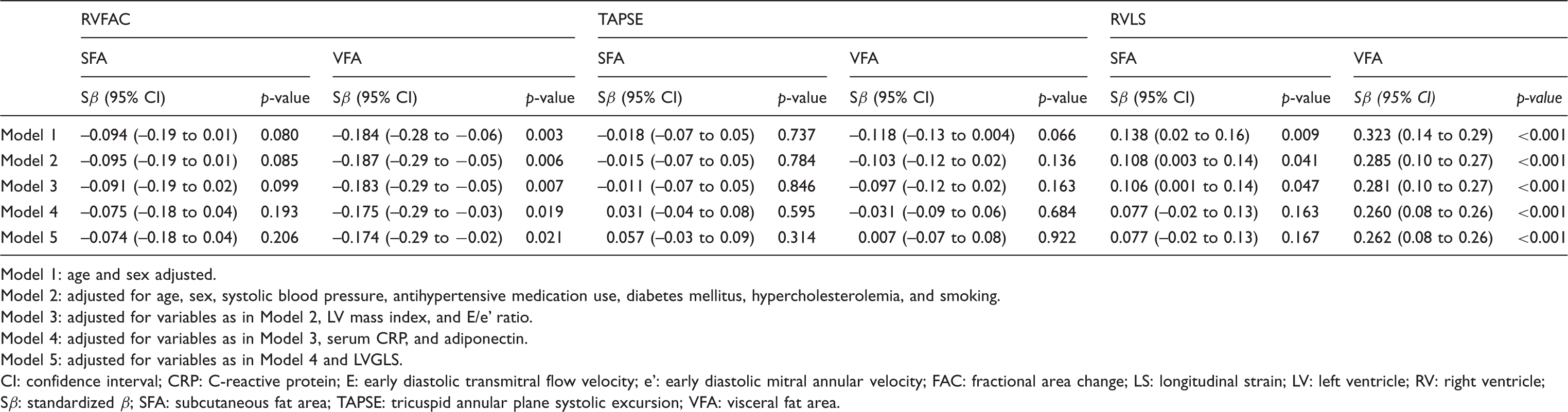
VFA was correlated with RVLS (r = 0.38, p < 0.001; Figure 1(c)), whereas a weaker, yet significant, correlation existed between SFA and RVLS (r = 0.12, p = 0.025; Figure 1(d)). VFA was associated with RVLS in the age- and sex-adjusted model (Table 3, Model 1). This association was not altered after adjustment for traditional cardiovascular risk factors (Table 3, Model 2). When adjusted for echocardiographic parameters (LV mass index and E/e’ ratio), VFA remained significantly associated with RVLS (Table 3, Model 3). This finding persisted after adjustment for CRP and adiponectin (Table 3, Model 4). Finally, even after controlling LVGLS, VFA was still independently associated with RVLS (standardized β = 0.262, p < 0.001; Table 3, Model 5). A similar trend was observed between SFA and RVLS, but was not statistically significant after adjustment for pertinent laboratory parameters (also Table 3). Two case examples with the same BMI of 23.5 kg/m2 are presented in Figure 2. The bottom case with a larger VFA had decreased LVGLS and RVLS compared with the top case with a smaller VFA. The associations between abdominal adiposity and standard RV parameters are also shown in Table 3. VFA was independently associated with RVFAC, but not TAPSE, whereas SFA was not significantly associated with either RVFAC or TAPSE.
Representative images of LVGLS and RVLS in two cases with the same BMI of 23.5 kg/m2. The lower case with larger VFA (b) had decreased LVGLS and RVLS compared with the upper case with smaller VFA (a). Association of abdominal adiposity with RVFAC, TAPSE, and RVLS. Model 1: age and sex adjusted. Model 2: adjusted for age, sex, systolic blood pressure, antihypertensive medication use, diabetes mellitus, hypercholesterolemia, and smoking. Model 3: adjusted for variables as in Model 2, LV mass index, and E/e’ ratio. Model 4: adjusted for variables as in Model 3, serum CRP, and adiponectin. Model 5: adjusted for variables as in Model 4 and LVGLS. CI: confidence interval; CRP: C-reactive protein; E: early diastolic transmitral flow velocity; e’: early diastolic mitral annular velocity; FAC: fractional area change; LS: longitudinal strain; LV: left ventricle; RV: right ventricle; Sβ: standardized β; SFA: subcutaneous fat area; TAPSE: tricuspid annular plane systolic excursion; VFA: visceral fat area.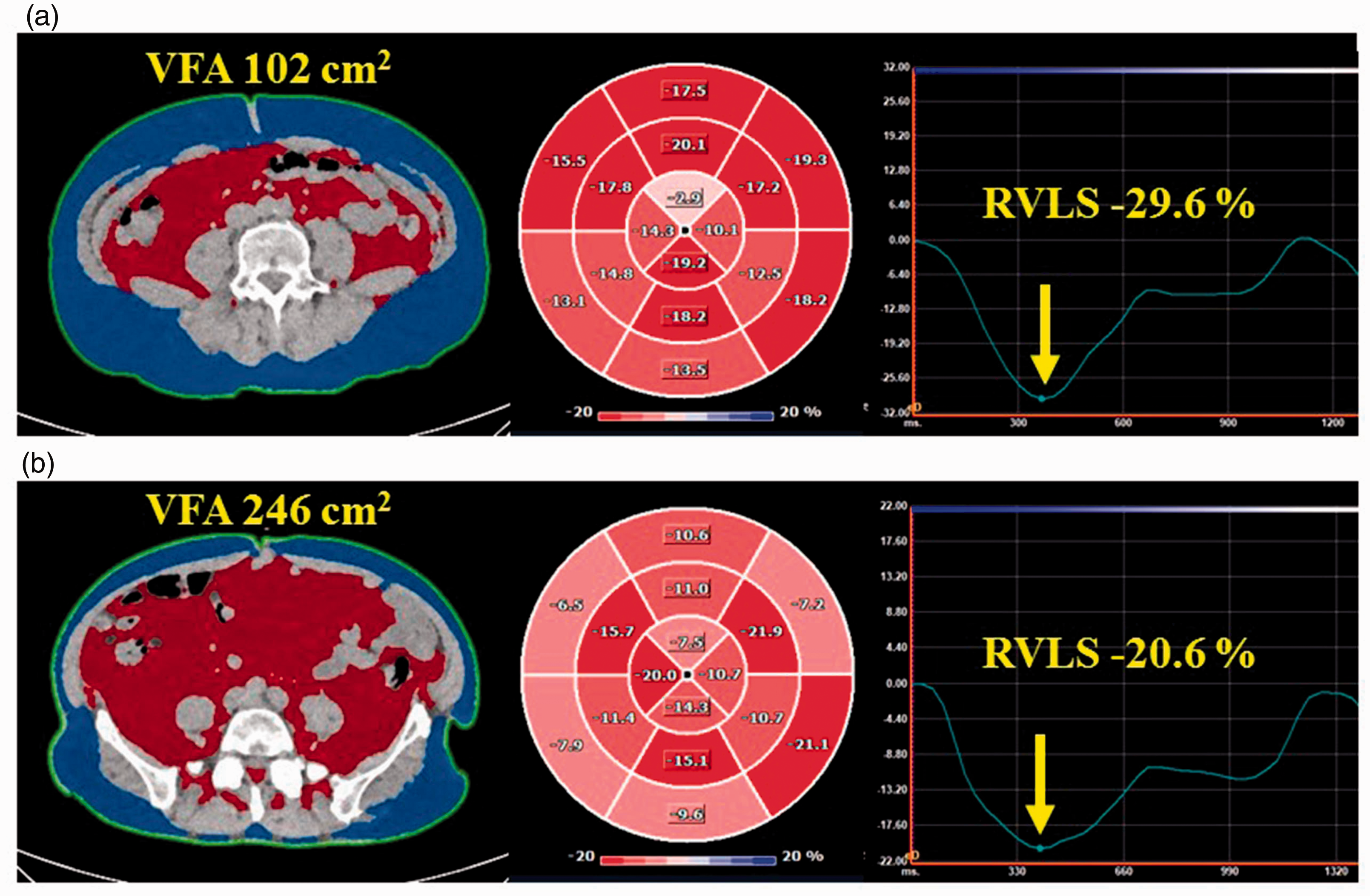
Adiponectin and ventricular strain
Although plasma adiponectin level was negatively correlated with LVGLS (r = –0.34, p < 0.001) and RVLS (r = –0.25, p < 0.001; Figure 3), no independent association was observed between serum adiponectin level and LVGLS (standardized β = –0.046, 95% confidence interval (CI) −0.079 to 0.031, p = 0.396) and RVLS (standardized β = –0.062, 95% CI −0.132 to 0.043, p = 0.319) in the multivariable analyses.
Correlation between serum adiponectin level and LVGLS (a), and RVLS (b).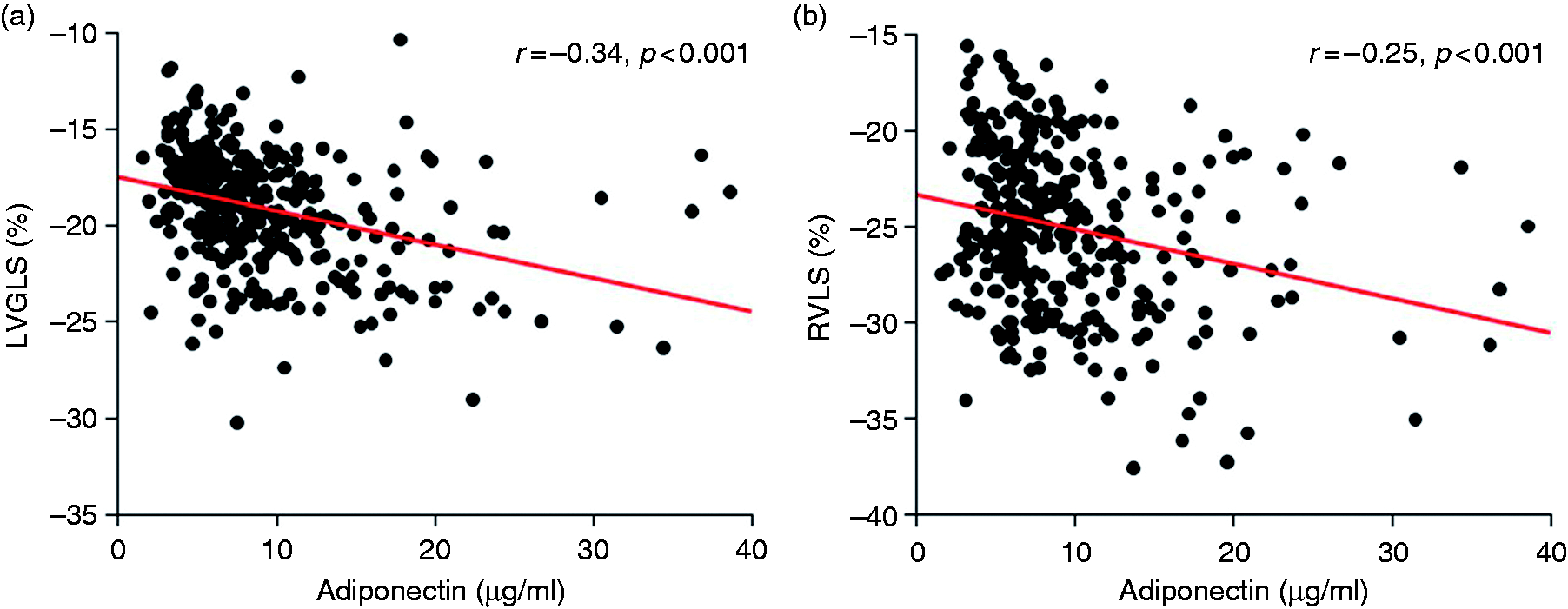
Discussion
We demonstrated for the first time that increased VFA, but not SFA, was associated with decreased LVGLS and RVLS, assessed by speckle-tracking echocardiography in a sample of the general population without overt cardiac disease. This association was independent of traditional cardiovascular risk factors and pertinent laboratory parameters. Furthermore, the association between VFA and RVLS was also independent of LV geometry and function, including LVGLS. Serum adiponectin level was correlated with LVGLS and RVLS, but it lost statistical significance after multivariable adjustment.
Visceral adiposity and ventricular strain
Concern has been raised regarding the growing prevalence of obesity and its deleterious impact on the incidence of cardiovascular disease, especially HF development.2–4 Due to unfavorable outcomes and the vast medical costs that result from HF, early identification of individuals at higher risk of HF is of clinical importance. 1 Longitudinal strain, a measure of the myocardial systolic deformation over the longitudinal axis, is emerging as an important tool to detect subclinical ventricular dysfunction, and is more sensitive than conventional echocardiographic parameters.11–13 We found that VFA was significantly associated with LVGLS, and that the observed association was independent of traditional cardiovascular risk factors and pertinent laboratory parameters. Our observations are consistent with current epidemiological studies showing an independent association of increased visceral fat with concentric LV remodeling, 5 diastolic dysfunction, 6 and incident HF, 7 and extend those observations to the study of subclinical LV dysfunction. Furthermore, our findings may shed light on the underlying mechanism involved in obesity-related HF.
Recently, particular attention has been directed to RV dysfunction in HF patients due to its deleterious impact on prognosis.8–10 Despite the significant impact of obesity on incident HF and the relevance of assessing RV function in patients with HF, limited data are available regarding the impact of obesity on RV function. Wong et al. demonstrated that obesity was strongly associated with impaired RV function using tissue Doppler imaging in 148 subjects without overt cardiac disease. 19 Another study by Tadic et al. showed that BMI was inversely associated with RVLS in 127 untreated hypertensive patients. 20 However, no studies have investigated the direct association between visceral fat accumulation and RV performance. We demonstrated that increased VFA was significantly associated with decreased RV strain independent of LV morphology and function, including LVGLS.
The underlying mechanisms involved in decreased ventricular strain as a result of increased VFA are not entirely clear; however, we hypothesize several potential explanations. First, increased visceral fat may induce a chronic inflammatory state, leading to worsened ventricular function. 21 Second, accumulation of visceral fat contributes to the development of insulin resistance 22 and the activation of the renin angiotensin system, 23 resulting in subclinical ventricular dysfunction. Indeed, recent studies showed that increased insulin resistance 24 and conditions leading to the activation of the renin angiotensin system, 25 such as chronic kidney disease, are associated with impaired ventricular strain via cardiomyocyte hypertrophy, perivascular fibrosis, and increased collagen deposition. Furthermore, alterations in lipid metabolism accompanied by visceral fat accumulation can cause increased arterial stiffness, also possibly leading to ventricular dysfunction. 26 Third, the presence of sleep disorders, which are closely associated with excess adiposity, can cause hypoxia and activation of the sympathetic nervous system, resulting in ventricular dysfunction. 27 Finally, an excess of visceral fat causes impaired coronary microcirculation, 28 which might be involved in the association between visceral adiposity and ventricular strain.
Serum adiponectin, LVGLS, and RVLS
Adiponectin, one of the adipokines produced by adipose tissue, has cardioprotective effects and is inversely correlated with visceral fat accumulation. 29 In this study, serum adiponectin level was not independently associated with LVGLS and RVLS; however, there was an inverse correlation between them when utilizing the univariable model. Other adipokines such as leptin, resistin, or adipsin may play a more important role in the association between visceral adiposity accumulation and impaired ventricular function. 30 An experimental study revealed that endothelial leptin signaling contributes to cardiac fibrosis and functional deterioration in a murine model. 31 Furthermore, Fontes-Carvalho et al. demonstrated that serum leptin level was more strongly associated with LV dysfunction than adiponectin level in 556 individuals from a community-based cohort. 32 On the other hand, adiponectin circulates as high-, middle-, and low-molecular weight isoforms in human plasma, each of which plays a different role in the cardiovascular system.33,34 However, we did not independently assess the different isoforms, which may underestimate the impact of adiponectin on the observed association.
Study limitations
Our study has several limitations. First, due to the cross-sectional design of our study, we cannot establish a cause–effect relationship between visceral adiposity and ventricular strain. Second, obese subjects typically have expanded plasma volumes, which might affect our observations; we did not assess plasma volume in this study. Third, we only measured total serum adiponectin level, which may be not enough to understand the role of adipokines on the observed association, although previous population-based studies demonstrated that low adiponectin level was associated with LV hypertrophy and diastolic dysfunction.35,36 Future studies are warranted to explore the role of other adipokines and adiponectin isoforms in the association between visceral fat accumulation and subclinical ventricular dysfunction. Finally, although we accounted for several potential confounders and performed multivariable analyses adjusting for cardiovascular risk factors, laboratory parameters, and echocardiographic measures, we cannot rule out the possibility of unmeasured confounders such as sleep disorders, which could play a role in the observed associations.
Conclusions
This study demonstrated a significant association of visceral adiposity with LVGLS and RVLS in a sample of the general population without overt cardiac disease. This association was independent of traditional cardiovascular risk factors and serum biomarkers, including adiponectin. Furthermore, the association between VFA and RVLS was independent of LV geometry and function, including LVGLS. Our findings suggest that visceral fat plays a central role in obesity-related ventricular dysfunction, and that the assessment of visceral fat may enable us to identify individuals at higher risk of incident HF. BMI might be an insufficient surrogate of VFA (because of its inability to distinguish between different VFA/SFA ratios) and, therefore, an inadequate therapeutic target for affecting subclinical ventricular dysfunction.
Footnotes
Author contribution
NS and KN contributed to the conception and design of the work. NS, KN, MD, HM, and IK contributed to the acquisition, analysis, and interpretation of the data for the current study. NS drafted the manuscript. KN, MD, YY, JI, MH, TN, HM, MRD, SH, and IK critically revised the manuscript. All authors provided final approval and agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was partially supported by the Yamauchi Susumu Scholarship for Cardiovascular Research.