
Abstract

Physical activity is consistently associated with reduced risk of vascular and non-vascular outcomes as well as mortality. 1 Vigorous or high-intensity physical activity (HIPA) (defined as energy expenditure of >6.0 metabolic equivalents of task (METs)) is associated with substantial improvements in cardiovascular risk factors such as cardiorespiratory fitness (CRF) and larger reductions in the risk of vascular outcomes. 2 Cross-country skiing is a seasonal HIPA which is undertaken as a leisure-time physical activity or long-term endurance sport; it is recognized as one of the most demanding aerobic endurance activities requiring good CRF. Emerging data suggests that cross-country skiing, undertaken as either a leisure-time or endurance training and competitive activity, is associated with reduced risk of vascular diseases, as well as mortality.3–5 There are suggestions that HIPA might be associated with potential toxic effects such as abnormalities in biochemical markers and cardiac dysfunction and arrhythmias, especially in endurance running and cycling. 6 However, it has been reported that this evidence is not consistent or strong enough to recommend avoiding heavy endurance exercise or sports. 6 Some reports suggest that cross-country skiing may be associated with an increased risk of acute cardiac events as well as common cardiac arrhythmias such as atrial fibrillation.7,8 Similarly these findings have been inconsistent; whereas some studies have shown an increased risk of atrial fibrillation with cross-country skiing,7,8 others have shown decreased or no difference in risk.3,9 In this context, our primary objective was to evaluate the associations of total volume and duration of leisure-time cross-country skiing with the risk of incident atrial fibrillation in a large general population-based sample of middle-aged Finnish men aged 42–61 years at baseline. Secondary objectives included (i) assessing the associations of leisure-time cross-country skiing habits with the risk of incident stroke and (ii) assessing the joint associations of leisure-time cross-country skiing habits and CRF with the risk of incident atrial fibrillation and stroke.
Data employed for this analysis came from the Kuopio Ischaemic Heart Disease Risk Factor (KIHD) study, a prospective population-based cohort study designed to investigate potential risk factors for atherosclerotic cardiovascular disease and other related chronic disease outcomes. Methods for participant recruitment, baseline examinations and measurements have been described previously. 4 Baseline measurements were performed between 20 March 1984 and 5 December 1989. Leisure-time cross-country skiing activity habits were assessed using a 12-month physical activity questionnaire modified from the Minnesota Leisure-Time Physical Activity Questionnaire. 4 All incident cases of atrial fibrillation and stroke from study entry through to 2017 were included and no losses to follow-up were recorded. The diagnostic classification of atrial fibrillation cases was conducted according to ICD-10 codes (I48.0–I48.9). A stroke event was classified according to ICD-10 codes I60–I68 and G45–G46]. The protocol was approved by the Research Ethics Committee of the University of Eastern Finland in line with the Helsinki Declaration and every participant provided written informed consent. Hazard ratios with their 95% confidence intervals (CIs) for outcomes were calculated using Cox proportional hazard models. All statistical analyses were conducted using Stata version MP 16 (Stata Corp, College Station, Texas, USA).
Associations of total volume and duration of leisure-time cross-country skiing with atrial fibrillation and stroke.
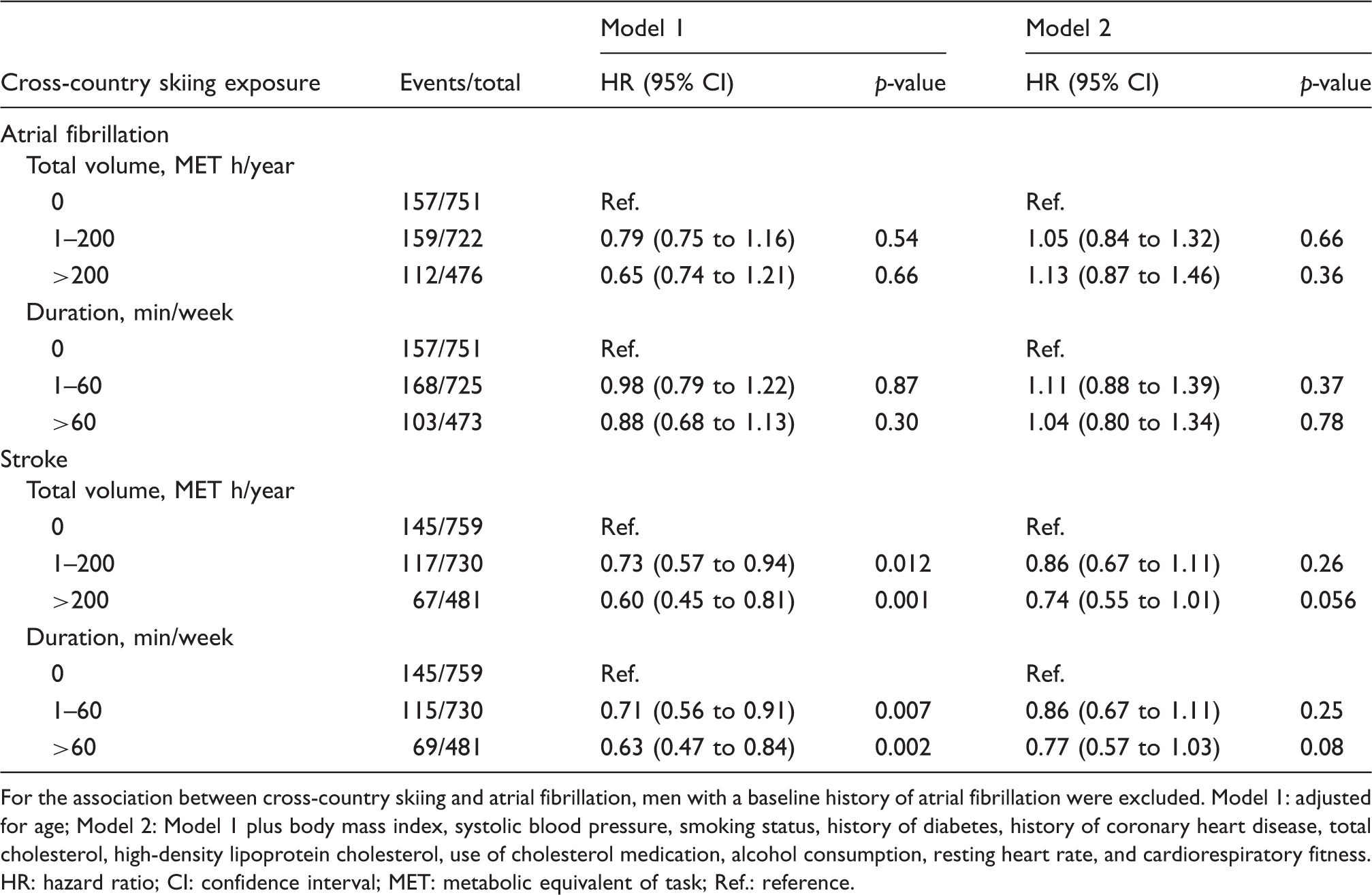
For the association between cross-country skiing and atrial fibrillation, men with a baseline history of atrial fibrillation were excluded. Model 1: adjusted for age; Model 2: Model 1 plus body mass index, systolic blood pressure, smoking status, history of diabetes, history of coronary heart disease, total cholesterol, high-density lipoprotein cholesterol, use of cholesterol medication, alcohol consumption, resting heart rate, and cardiorespiratory fitness.
HR: hazard ratio; CI: confidence interval; MET: metabolic equivalent of task; Ref.: reference.
Joint associations of leisure-time cross-country skiing and cardiorespiratory fitness with atrial fibrillation and stroke.
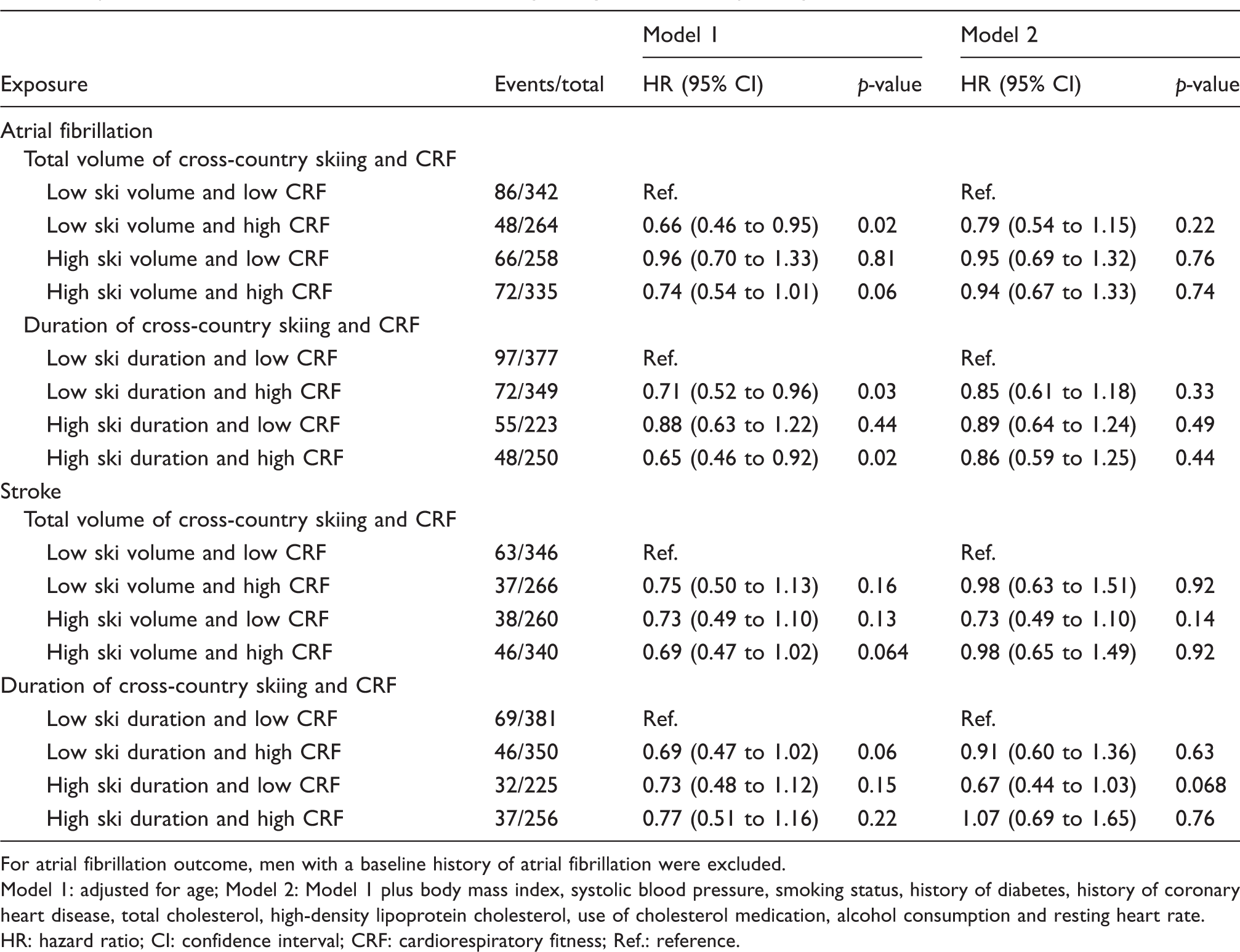
For atrial fibrillation outcome, men with a baseline history of atrial fibrillation were excluded.
Model 1: adjusted for age; Model 2: Model 1 plus body mass index, systolic blood pressure, smoking status, history of diabetes, history of coronary heart disease, total cholesterol, high-density lipoprotein cholesterol, use of cholesterol medication, alcohol consumption and resting heart rate.
HR: hazard ratio; CI: confidence interval; CRF: cardiorespiratory fitness; Ref.: reference.
In a cohort of middle-aged Finnish men, male skiers had a similar prevalence of atrial fibrillation to that of non-skiers at study entry. On evaluation of the relationships of leisure-time cross-country skiing habits with the risk of incident atrial fibrillation, no significant associations were observed, and these findings are consistent with some previous reports.3,9 In a large study of 208,654 skiers of the Vasaloppet skiing study matched to 527,448 non-skiers, male cross-country skiers had a similar incidence of atrial fibrillation to that of non-skiers. 9 In another cohort of 399,630 skiers and non-skiers, no differences in the risk of atrial fibrillation were found between the two groups. 3 On the other hand, our null findings on the relation between cross-country skiing habits and risk of stroke are in contrast to findings of previous studies which have shown lower incidence of stroke among skiers.3,9 Given that cross-country skiers have the highest recorded levels of CRF, 10 we hypothesized that there may be an interaction between cross-country skiing activity and objectively measured CRF on the outcomes of atrial fibrillation and stroke. However, our detailed evaluation of the impact of cross-country skiing and CRF on outcomes showed no significant evidence of associations. Since the majority of studies reporting an increased risk of atrial fibrillation with cross-country skiing are based on long-term endurance cross-country skiers, the null association observed between leisure-time cross-country skiing and atrial fibrillation in our study may reflect important pathophysiologic differences between the two types of activities in the pathogenesis of atrial fibrillation. It has been suggested that the dose of endurance exercise plays a role in the pathophysiology of atrial arrhythmias. 11 Indeed, the intensity and volume of endurance cross-country skiing far exceeds those proposed by general population guideline recommendations compared with leisure-time cross-country skiing; these excessive doses may be associated with cardiac injury, increased inflammation, atrial remodelling and autonomic imbalance, which are suggested mechanisms underlying the development of atrial fibrillation. Research evidence also indicates that there is a J-shaped association between atrial fibrillation and the broad range of physical activity and exercise; whereas prolonged endurance exercise increases the prevalence and incidence of atrial fibrillation, modest physical activity is associated with a decreased risk of atrial fibrillation. 12 In a large prospective evaluation of 7018 participants, total and types of physical activity such as walking, cycling, domestic work, gardening and sports, were demonstrated not to be associated with an increased or decreased risk of atrial fibrillation. 13 If there is any association between leisure-time cross-country skiing habits and atrial fibrillation at all, it would more likely be a beneficial one given the overall existing evidence, plausible mechanistic pathways and the direction of effect of our findings. Nevertheless, the null findings could also be due to confounding and differences in factors such as age, sex and genetic background of the population, and study design characteristics such as follow-up duration.
Strengths of the current study include the large sample, which was representative of the general population of middle-aged men, zero loss to follow-up, long-term follow-up and adjustment for a comprehensive panel of confounders. Weaknesses of the study include inability to generalize the findings to women and other age groups, inability to assess associations between skiers with atrial fibrillation and stroke because of the low numbers, the assessment of cross-country skiing habits using self-reported questionnaires, and biases inherent to observational study designs such as residual confounding and reverse causation bias.
In conclusion, leisure-time cross-country skiing is not associated with an increased risk of atrial fibrillation or stroke in middle-aged Caucasian males. These findings extend the evidence on the overall safety of HIPAs.
Footnotes
Author contribution
SKK, JAL, SK, TM and HK contributed to the conception and design of the work. All authors contributed to the acquisition, analysis, or interpretation of data for the work. SKK, JAL, TM, and HK drafted the manuscript. All authors critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Acknowledgements
Our gratitude is extended to the team of the of the Kuopio Research Institute of Exercise Medicine and the Research Institute of Public Health and University of Kuopio, Finland, for the collection and provision of the data for this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the Finnish Foundation for Cardiovascular Research, Helsinki, Finland, for supporting the Kuopio Ischemic Heart Disease Study. SKK acknowledges support from the NIHR Biomedical Research Centre at University Hospitals Bristol NHS Foundation Trust and the University of Bristol. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care. These sources had no role in design and conduct of the study; collection, management, analysis, and interpretation of the data; and preparation, review, or approval of the manuscript.