
Abstract
Aims
Due to improving cancer treatment results, non-cancer mortality is an important issue for cancer survivors. Cardiovascular diseases are the leading causes of death in Korea and globally. In addition to lowering the risk of cardiovascular disease, the use of statins has led to an overall reduction in cancer mortality in recent observational studies. We investigated the status of current dyslipidemia management in cancer survivors with reference to 2018 guidelines.
Methods
The study is a cross-sectional analysis of 1460 cancer survivors aged from 40 to 75 years who participated in the Korean National Health and Nutrition Examination Survey from 2007 to 2016. Dyslipidemia management status among cancer survivors was assessed according to 2018 American College of Cardiology/American Heart Association guidelines and Korean Coronary Heart Disease Risk Score guidelines.
Results
The rate of treatment for dyslipidemia was 8.5% for males, 13.8% for females, and 11.9% overall. Among cancer survivors who were not receiving treatment for dyslipidemia, 59.6% of males, 34.2% of females and 43.9% of total cancer survivors would have been eligible for statin therapy under the 2018 American College of Cardiology/American Heart Association guidelines and Korean Coronary Heart Disease Risk Score guidelines. The rate of undertreatment of dyslipidemia increased with age and length of time since cancer diagnosis.
Conclusion
Nearly 50% of cancer survivors remain untreated although they are eligible for statin therapy. This emphasizes the need for more attention to prevent atherosclerotic cardiovascular disease among cancer survivors.
Introduction
Due to improvements in cancer treatment results, non-cancer mortality has emerged as an important issue for cancer survivors. In Korea, the 1.74 million cancer patients who are currently being treated represent 3.4% of the total Korean population. The overall five-year relative survival rate of cancer patients diagnosed in the last five years (2011–2015) has increased continuously to 70%, which is 1.7 times higher than the previous 20 years’ survival rate (1993–1995). 1 As a result, increasing attention is being paid to general health management after cancer treatment, especially for cardiovascular disease (CVD). CVD, including ischemic heart disease and stroke, is the most common cause of death in the world and second in Korea after cancer.2,3 Compared with time after cancer diagnosis, CVD accounts for 50% of non-cancer deaths, 4 while nearly 50% of non-cancer deaths in Korean prostate cancer patients were due to CVD. 5
Management of dyslipidemia is key for prevention of cardiovascular events. Because dyslipidemia is an important risk factor for CVD, many other guidelines recommend lipid screening over 40 years of age for primary prevention of future CVD events.6–8 Also, the American College of Cardiology/American Heart Association (ACC/AHA) 2018 revision of their Guideline on the Management of Blood Cholesterol recommends statin use for primary prevention of CVD in adults with absolute baseline risk of a future CVD event. Statins are also recommended for those between 40 and 75 years of age with more than 7.5% risk of 10-year atherosclerotic CVD (ASCVD).9,10 In addition, the anti-cancer effects of statin have been suggested by in vitro studies,11,12 population-based cohort studies13–16 and studies of cancer survivors.11,17–19 Use of statins can therefore be important in comprehensive care of cancer survivors, especially those at high risk for ASCVD.
In this study using Korea National Health and Nutrition Survey (KNHANES) data, we investigated the status of dyslipidemia management and statin undertreatment among Korean cancer survivors by applying Korean dyslipidemia management20–22 and 2018 ACC/AHA cholesterol treatment guidelines.
Materials and methods
Study design and participants
Our study is a cross-sectional analysis of data derived from the KNHANES between 2007 and 2016. KNHANES has been conducted annually since 2007 by the Korea Centers for Disease Control and Prevention. Detailed explanations on the KNHANES are available elsewhere.23–25
Among an initial dataset comprising 78,113 subjects, we selected 36,984 subjects between the ages of 40 and 75 years, a range determined by the 2018 ACC/AHA cholesterol treatment guideline. 10 Of those subjects, 1460 were cancer survivors who responded to a self-reported questionnaire that they had been diagnosed with some type of cancer. Another 35,524 subjects were members of the general population who did not have a history of any type of cancer diagnosis.
The Institutional Review Board (IRB) of Samsung Medical Center (IRB file no. 2019-06-048) approved the study. Participants gave their written informed consent.
Measurement and data collection
Self-reported questionnaire
The survey questionnaire included questions on age, sex and socioeconomic status. We collected a self-reported history of comorbidity diseases, current medication, smoking history and family medical history of CVD, which are considered risk factors for CVD according to the ACC/AHA cholesterol treatment guideline. 10 Cancer survivors were also asked about site of cancer and age of diagnosis. 24
Anthropometric measurements
Participants underwent blood collection after fasting for 12 h, and their samples were tested with a Hitachi Automatic Analyzer 7600-210 (Hitachi, Japan) and Tosoh G8 (Tosoh, Japan). We used blood pressure, fasting serum glucose, total serum cholesterol, triglycerides, high-density lipoprotein cholesterol (HDL-C), 26 low-density lipoprotein cholesterol (LDL-C) and body measurements (height, weight, waist circumference). The LDL-C was calculated using the Friedewald formula if the triglycerides level was <200 mg/dL, as follows: LDL-C = total cholesterol – HDL-C – (triglycerides/5), and the LDL-C was directly measured if the triglycerides level was ≥200 mg/dL.
Risk group categorization
To analyze dyslipidemia management status, we divided the risk groups into four subgroups and described statin use criteria in each group according to the Korean guidelines (Supplementary Material Table 1 online). 20 And for analysis of subjects who are indicated for statin therapy, we categorized the participants into four risk groups according to the ACC/AHA cholesterol treatment guideline (Supplementary Table 2). 10
As the pooled cohort equation and similar risk assessment tools 10 were developed for Western patients, Asians can overestimate their 10-year ASCVD risk. We therefore calculated 10-year ASCVD risk based on: 1) the Korean Coronary Heart Disease Risk Score (KRS) from the Korean Heart Study population 21 and 2) a recalibrated Framingham risk equation developed from CVD incidence rates in the non-Chinese Asian population. 22
Definition of variables
Ever diagnosed, receiving treatment, control, and prevalence of dyslipidemia
Ever diagnosed, receiving treatment, and control of dyslipidemia were defined using the health interview and the health examination survey results from KNHANES. Ever diagnosed with dyslipidemia was defined as subjects who responded positively to the question: ‘Have you ever been diagnosed with dyslipidemia by a doctor?’ Receiving treatment for dyslipidemia was defined as those with dyslipidemia for which they are currently using a lipid-lowering medication. Control of dyslipidemia was defined based on LDL-C level as four subgroups (Supplementary Table 1). 20 Prevalence of dyslipidemia was defined in subjects who were ever diagnosed or treated with dyslipidemia or who met the diagnostic criteria. In addition, two different factors were used to define controlled dyslipidemia: (a) all subjects with prevalent dyslipidemia and (b) subjects receiving dyslipidemia treatment.
Definition of cardiovascular risk factor status
Ever diagnosed and treatment of hypertension and diabetes were defined in the same way as dyslipidemia. Poorly controlled hypertension was defined as systolic blood pressure (SBP) ≥140 mmHg or diastolic blood pressure (DBP) ≥90 mmHg, and undiagnosed hypertension was defined as SBP ≥140 mmHg or DBP ≥90 mmHg without a self-reported hypertension diagnosis. Poorly controlled diabetes was defined as glycated hemoglobin (HbA1c) ≥7.0%, and undiagnosed diabetes was defined as fasting blood sugar ≥126 mg/dL or HbA1c ≥6.5% without a self-reported diagnosis of diabetes. In addition, three different factors were used to define poorly controlled and undiagnosed hypertension and diabetes: (a) all subjects with prevalent hypertension and diabetes; (b) subjects receiving hypertension and diabetes treatment; and (c) subjects with never diagnosed hypertension and diabetes. Body mass index (BMI) was calculated as the ratio of weight to square of height (kg/m2). We divided BMI data into two categories according to Korean obesity standards (obesity 25–29.9, and severe obesity ≥30.0). In addition, men and women with a waist circumference ≥90 cm and ≥85 cm, respectively, were defined as abdominally obese. 27
Statistical analyses
Demographic characteristics along with dyslipidemia and other cardiovascular risk-factor management status values were tabulated and proportionally weighted by applying integrated weights using the svy command to reflect the complex sampling design. 24
Undertreatment of dyslipidemia was examined based on the 10-year ASCVD risk using the three formulas described earlier: KRS was used for the main analysis, and recalibration of the Framingham risk equation and the pooled cohort equation were used for sensitivity analysis. Cancer survivors were divided into subgroups by age at examination, survey year (KNHANES IV 2007–2009, V 2010–2012, VI–VII 2013–2016) and period after cancer diagnosis. To compare the level of undertreatment with that of non-cancer subjects, we matched at a 1:4 ratio each case of cancer survival by age and sex. All statistical analyses were performed using STATA software (version 14.0).
Results
Study participants
The overall study sample comprised 1460 cancer survivors (519 males and 941 females). The average age of all cancer survivors was 63.8 (±8.5) years in men and 58.4 (±9.3) years in women. Gastric (17.3%), thyroid (16.0%), cervical (13.2%) and breast cancer (13.0%) were the most common types of cancer. A history of coronary heart disease was reported by 3.8% of subjects, while 2.4% reported a prior stroke (Supplementary Table 3).
Ever diagnosed, receiving treatment, and control of dyslipidemia by Korean guidelines
Diagnosis, treatment and control of dyslipidemia in different risk groups of cancer survivors.
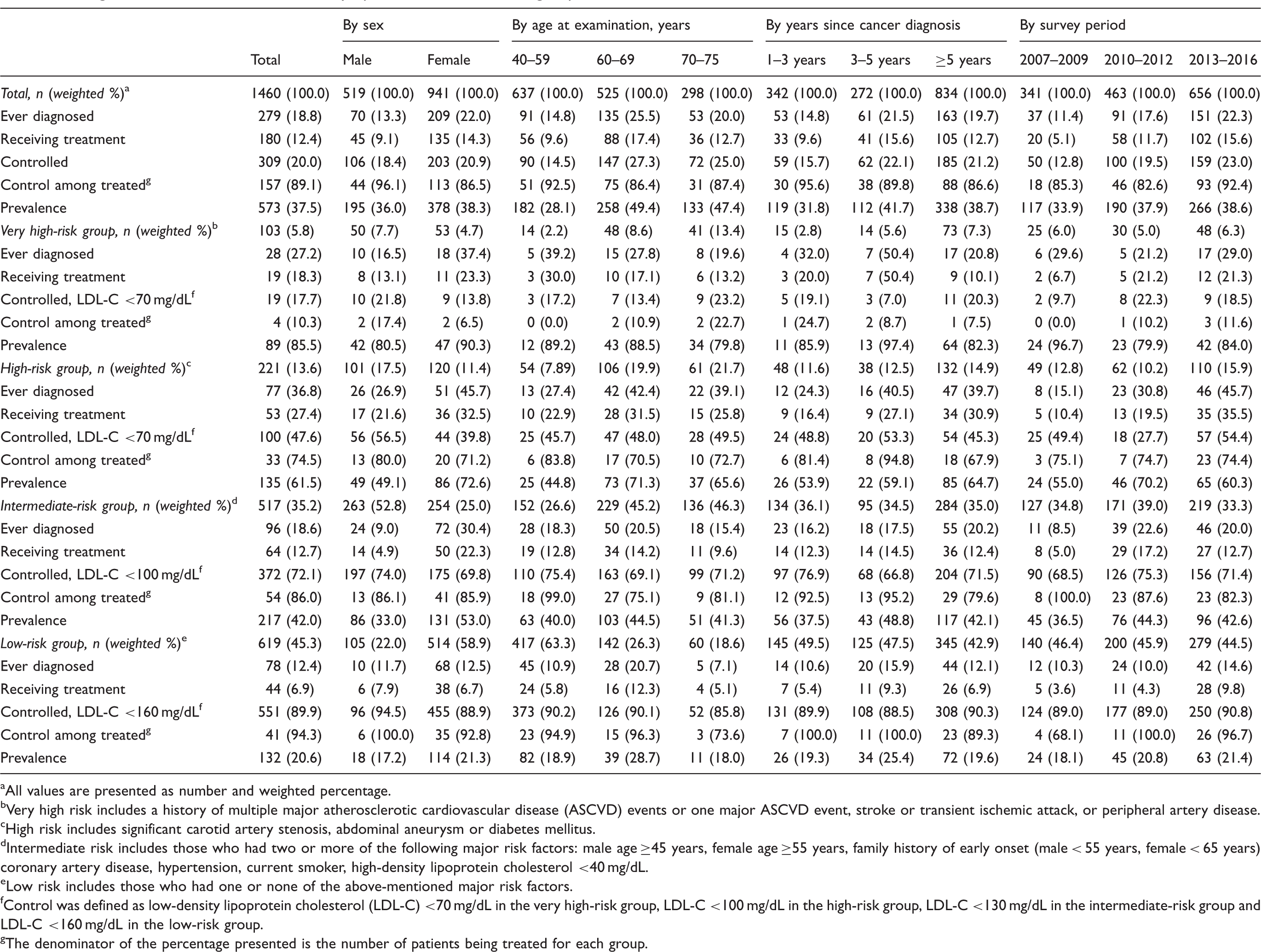
All values are presented as number and weighted percentage.
Very high risk includes a history of multiple major atherosclerotic cardiovascular disease (ASCVD) events or one major ASCVD event, stroke or transient ischemic attack, or peripheral artery disease.
High risk includes significant carotid artery stenosis, abdominal aneurysm or diabetes mellitus.
Intermediate risk includes those who had two or more of the following major risk factors: male age ≥45 years, female age ≥55 years, family history of early onset (male < 55 years, female < 65 years) coronary artery disease, hypertension, current smoker, high-density lipoprotein cholesterol <40 mg/dL.
Low risk includes those who had one or none of the above-mentioned major risk factors.
Control was defined as low-density lipoprotein cholesterol (LDL-C) <70 mg/dL in the very high-risk group, LDL-C <100 mg/dL in the high-risk group, LDL-C <130 mg/dL in the intermediate-risk group and LDL-C <160 mg/dL in the low-risk group.
The denominator of the percentage presented is the number of patients being treated for each group.
Treatment status of dyslipidemia by ASCVD risk score
Treatment status of dyslipidemia in Korean cancer survivors aged 40 to 75 years: application of the 2018 American College of Cardiology/American Heart Association guideline with calculation of atherosclerotic cardiovascular disease risk by Korean Coronary Heart Disease Risk Score.
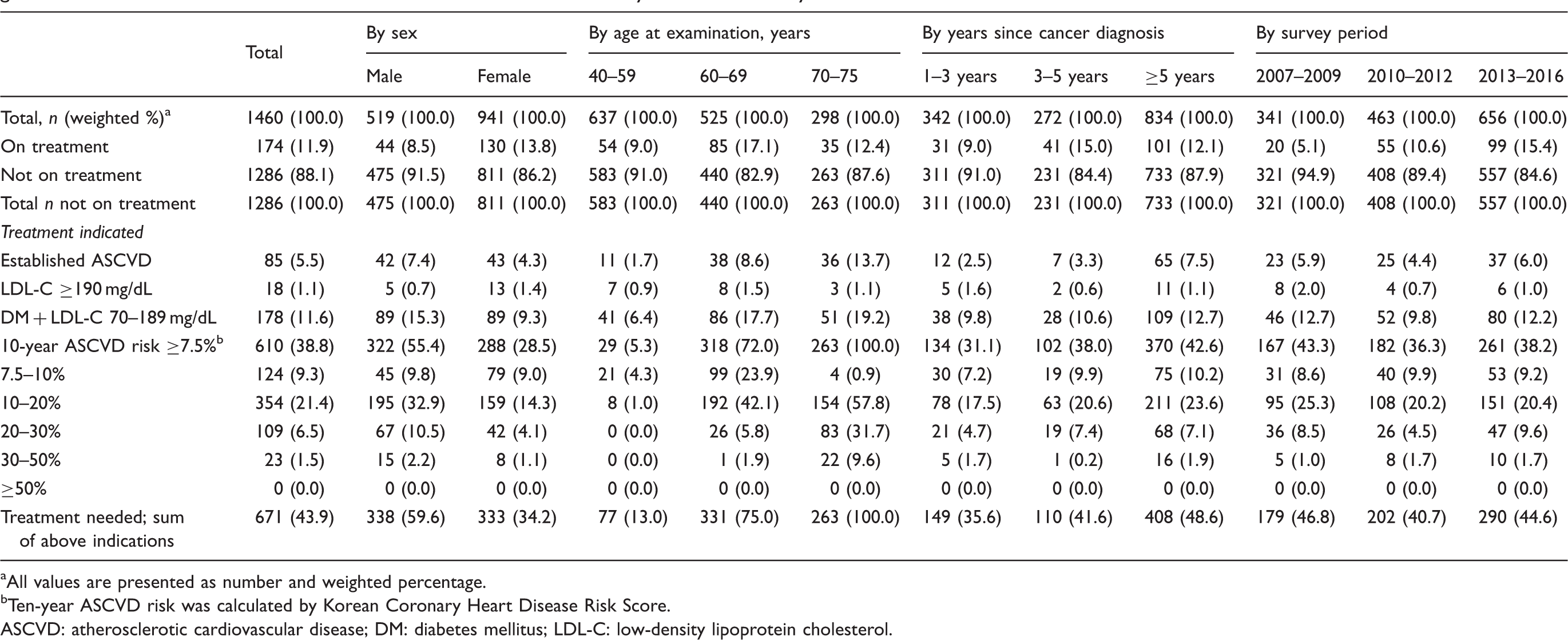
All values are presented as number and weighted percentage.
Ten-year ASCVD risk was calculated by Korean Coronary Heart Disease Risk Score.
ASCVD: atherosclerotic cardiovascular disease; DM: diabetes mellitus; LDL-C: low-density lipoprotein cholesterol.
Similar results were obtained from a sensitivity analyses using the recalibrated Framingham risk and pooled cohort equations. The undertreatment rate of dyslipidemia showed similar results among matched non-cancer subjects (Supplementary Tables 4 and 5).
Cardiovascular risk-factor management status among cancer survivors
Risk factors for cardio-cerebrovascular disease in cancer survivors.
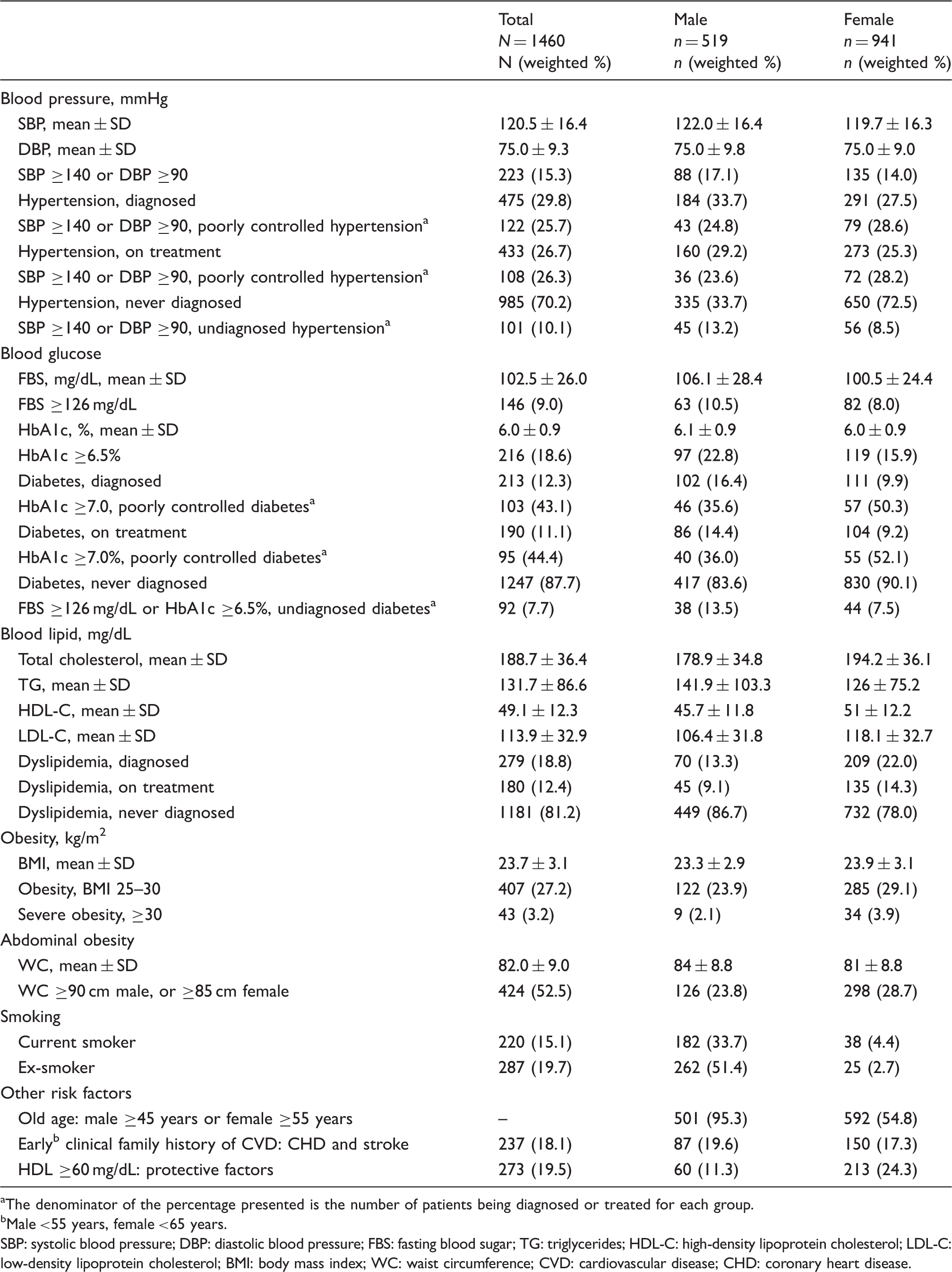
The denominator of the percentage presented is the number of patients being diagnosed or treated for each group.
Male <55 years, female <65 years.
SBP: systolic blood pressure; DBP: diastolic blood pressure; FBS: fasting blood sugar; TG: triglycerides; HDL-C: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; BMI: body mass index; WC: waist circumference; CVD: cardiovascular disease; CHD: coronary heart disease.
Discussion
Summary and strengths
To the best of our knowledge, our study is the first to evaluate dyslipidemia management status in Korean cancer survivors. Strengths include a representative sample, application of 2018 Korean and AHA/ACC guidelines, and use of matched non-cancer controls. Our study shows suboptimal dyslipidemia management status in Korean cancer survivors, and approximately half of cancer survivors are currently not receiving indicated lipid-lowering medications, according to current risk-based treatment guidelines.
Management status of dyslipidemia
Our results showed that 37.5% of Korean cancer survivors had dyslipidemia, but only 12.4% of them were taking a lipid-lowering medication. When applying Korean dyslipidemia guidelines, 20.0% were within the goal LDL-C level; among those who were treated for dyslipidemia in the very high-risk group, 10.3% were reaching the goal LDL-C level. This shows poor awareness of dyslipidemia in cancer survivors and suboptimal or poor treatment adherence, even in very high-risk patients. These results suggest that cancer survivors often focus on cancer treatment itself and less on management of chronic diseases. 28
These results also suggest a lack of interest in management of dyslipidemia and ASCVD risk among both cancer survivors and physicians. This is likely because physicians tend to make decisions regarding dyslipidemia treatment according to LDL-C level rather than calculated 10-year risk of ASCVD. One of the reasons why Korean physicians are following Korean guidelines rather than ACC/AHA guidelines is that the 10-year risk calculation is not an essential factor in the initiation of dyslipidemia treatment in Korean guidelines. This assumption was also shown when comparing the prevalence of dyslipidemia in subjects not being treated for dyslipidemia with the application of Korean and ACC/AHA guidelines, respectively (Supplementary Figure 1). Comparing the two guidelines shows that the difference in the prevalence of dyslipidemia increases with age, which is statistically significant (p < 0.001).
Undertreatment and suboptimal management of dyslipidemia were higher in male, elderly, and high-risk groups of cancer survivors. Patients at greatest risk of developing CVD were not receiving adequate management of dyslipidemia.
Undertreatment of dyslipidemia
When applying the ACC/AHA guideline, nearly 50% of cancer survivors were not treated for dyslipidemia although they were eligible for statin therapy. These results indicate that ASCVD risk management is not optimal among cancer survivors.
Undertreatment rate of dyslipidemia tended to increase with age. 29 Almost all cancer survivors in the 70–75 year age group needed statin treatment for undiagnosed dyslipidemia. This implies that age has a significant effect on occurrence of ASCVD and shows that statin therapy is essential to reducing mortality from CVD among older cancer survivors. Also, the longer was the survival period after cancer diagnosis, the greater was the need for treatment among cancer survivors, probably because of the effect of increasing age. Over the years of the survey, the proportion of those receiving treatment increased slightly, but cancer survivors who are not treated for dyslipidemia still accounted for 50%.
Other cardiovascular risk factors
For comprehensive cardiovascular prevention, management of other risk factors is important. 30 However, hypertension and diabetes were prevalent among cancer survivors – 25.7% and 43.1% of hypertension and diabetes patients in cancer survivors had poorly controlled blood pressure (SBP ≥140 mmHg or DBP ≥90 mmHg) and HbA1c level (≥7.0%), respectively. The rates of untreated hypertension and undiagnosed diabetes approached 10% among cancer survivors. These results suggest the need for comprehensive cardiovascular risk management strategies in cancer survivors, not only limited to dyslipidemia management. Also, lifestyle therapy, such as improving dietary habits and achieving exercise recommendations, should be emphasized to prevent CVD. 31
Clinical implications
Comparisons with a matched control in our study showed that statin undertreatment was not significantly different from that in the general population. However, considering that cancer survivors have increased medical contact with health care professionals from regular visits and laboratory tests, it is clear that comprehensive cardiovascular management is not delivered effectively in routine oncologic practice.
Current National Comprehensive Cancer Network guidelines recommend and emphasize the potential benefits for survivorship of care planning, vaccinations, management of chronic disease, healthy behavior, and co-management between oncologists and primary care providers. 32 However, as other studies have demonstrated, cancer survivors have a lower rate of antihypertensive medication adherence than the general population 33 and they tend to neglect management of chronic diseases other than cancer. These results imply that oncologists may have difficulty in paying sufficient attention to primary care needs of cancer survivors, as they generally focus on cancer treatment as their first priority. Since late 2000, it has been suggested that oncologists and primary care physicians exchange opinions and cooperate with one another to manage cancer survivorship programs for cancer survivors. 34 We should therefore emphasize the role of primary and preventive care for cancer survivors and pay more attention to the co-management and shared-care model for ASCVD risk, including dyslipidemia. 35
Limitations
The limitations of this study are related primarily to the use of the KNHANES, which was not designed to evaluate cancer survivorship issues. The study population was relatively small, although we integrated a 10-year (2007–2016) study. Self-reported cancer history and risk factors for co-morbidities may be affected by recall bias, and no self-reporting validation was performed. Also, we were not able to consider the use of non-statin medications (e.g. ezetimibe, bile acid sequestrants or PCSK9-inhibitors) or address the number of patients who had tried but were intolerant to statins because the exact type of dyslipidemia medication or experience with adverse effects of statins and discontinuation was not investigated. Since the cancer stage and treatment status were not examined in this data, it was impossible to rule out the possibility that patients with higher ASCVD risk were more advanced cancer patients and could not receive optimal dyslipidemia treatment.
It was impossible to rule out the possibility that patients with higher ASCVD risk were more advanced cancer patients and could not receive treatment because the data were not available. In addition, detailed information on cancer stage and treatment is unknown. Since the cancer stage and treatment status were not examined in these data, the failure to treat hyperlipidemia among cancer survivors, especially in high-risk cancer survivors, was not considered in relation to cancer treatment and the remaining life.
Conclusion
Nearly 50% of cancer survivors remain untreated although they are eligible for statin therapy. This emphasizes the need for more attention to prevent ASCVD among cancer survivors.
Supplemental Material
CPR905722 Supplemental Material - Supplemental material for Status of dyslipidemia management and statin undertreatment in Korean cancer survivors: A Korean National Health and Nutrition Examination Survey study
Supplemental material, CPR905722 Supplemental Material for Status of dyslipidemia management and statin undertreatment in Korean cancer survivors: A Korean National Health and Nutrition Examination Survey study by Sujeong Shin, Dong Wook Shin, In Young Cho, Su-Min Jeong and Hyein Jung in European Journal of Preventive Cardiology
Footnotes
Author contribution
SS, DWS and SMJ contributed to the conception or design of the work. SS, DWS, IYC, SMJ and HJ contributed to the acquisition, analysis or interpretation of data for the work. SS drafted the manuscript. DWS, IYC and HJ critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work ensuring integrity and accuracy.
Acknowledgement
Some of the results of this study was presented for poster presentation at the 2019 Annual Meeting of the Multinational Association of Supportive Care in Cancer (MASCC) and the International Society of Oral Oncology (ISOO), San Francisco (California, USA), 21 to 23 June 2019.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.