
Abstract

Introduction
Atrial fibrillation (AF) is an essential global concern because it could lead to cardiovascular events such as stroke, heart failure, and mortality. However, more than half of the AF cases are reported to be potentially preventable. 1 Although traditional risk factors of AF include hypertension, older age, obesity, diabetes mellitus, and obstructive sleep apnea (OSA), there is emerging evidence that other lifestyle risk factors are also associated with the risk of developing new-onset AF. Recent studies have demonstrated that moderate caffeine or coffee consumption is associated with either increased or decreased risk of cardiovascular diseases such as coronary artery disease and stroke.2–5 This present meta-analysis aimed to explore the association between caffeine/coffee consumption and the risk of developing new-onset AF.
A comprehensive search of articles in several databases from 1966 to June 1, 2019, in any language and conducted on humans was completed. The databases included Ovid MEDLINE, Ovid Embase, Ovid Cochrane Database of Systematic Reviews, Scopus, and Web of Science. The search strategy was designed and conducted by an experienced librarian (AMF) with input from the study’s principle investigator (CK). The search strategies were peer-reviewed by other experienced librarians at Mayo Clinic Libraries. Controlled vocabulary, supplemented with keywords including MeSH and Embase terms, was used to search for studies of “caffeine”, “coffee”, “tea”, “energy drinks”, and “atrial fibrillation”.
Studies with the following outcomes were included: the presence of new-onset AF, and reports by the study investigators of relative risks (RRs), odd ratios (ORs), and/or hazard ratios (HRs) with 95% confidence intervals (CIs). We excluded reviews, editorials, non-human studies, and letters without sufficient data from this study; studies that included a history of AF, chronic AF, or patients with paroxysmal AF were also excluded. In addition, we contacted the authors if further information was needed for testing our hypotheses.
The RRs, ORs, HRs, and 95% CIs were pooled as estimated risk ratios and then logarithmically transformed and weighted for the inverse of the variance. We used the DerSimonian and Laird random-effects models. 6 Exploratory random-effect meta-regression analyses were conducted to assess the influence of study characteristics (i.e. age, country, and follow-up year) on study results. We also conducted subgroup analyses of the included studies stratified by age, follow-up years, geographic location, and risk of bias. The performances of subgroup-specific and statistical tests of interaction among the subgroups were also assessed regarding whether caffeine/coffee consumption effects differ between the subgroups. We used the “leave-one-out” method to evaluate whether any study had a dominant effect on the outcomes. We defined substantial heterogeneity between the studies if I2 > 50%. We performed analyses with OpenMetaAnalyst for 64-bit (Brown University), R version 3.2.3, and Stata version 11 (Stata Corp, College Station, TX, USA), and all tests were two-sided with a significance level of 0.05.
The disposition of studies excluded after the full-text review is shown in Supplementary Figure 1. Overall, 12 observational cohorts were finally selected for this meta-analysis: seven prospective cohorts, including a total of 12,415 new-onset AF cases diagnosed among 219,461 individuals, and five retrospective cohorts, including a total of 5289 new-onset AF cases diagnosed among 141,682 individuals (Supplementary Table 1). The results of a study quality assessment are shown in Supplementary Tables 2 and 3. The caffeine/coffee consumption was not associated with increased or decreased risk of new-onset AF compared with no caffeine/coffee consumption (pooled RR, 0.98; 95% CI: 0.88–1.09; p < 0.001; I2 = 59.21%). The highest category of caffeine/coffee consumption (≥5 cups/day) was not associated with increased or decreased risk of new-onset AF compared with the lowest category (1–2 cups/day) (pooled RR, 0.95; 95% CI: 0.84–1.06; p = 0.004; I2 = 60.25%) (Figure 1). In subgroup analyses using study type (prospective vs retrospective), geography, and follow-up year, we did not find any associations between caffeine/coffee consumption and risk of new-onset AF. Interestingly, after excluding studies with a moderate risk of bias, the highest category of caffeine/coffee consumption was associated with decreased risk of new-onset AF compared with the lowest category (pooled RR, 0.90; 95% CI: 0.82–0.95; p = 0.002; I2 = 0%). There were no significant interactions among the subgroups. There was no study markedly affecting the summary estimate or p-values for heterogeneity in all groups.
Forest plot of primary outcome (the risk of new-onset atrial fibrillation).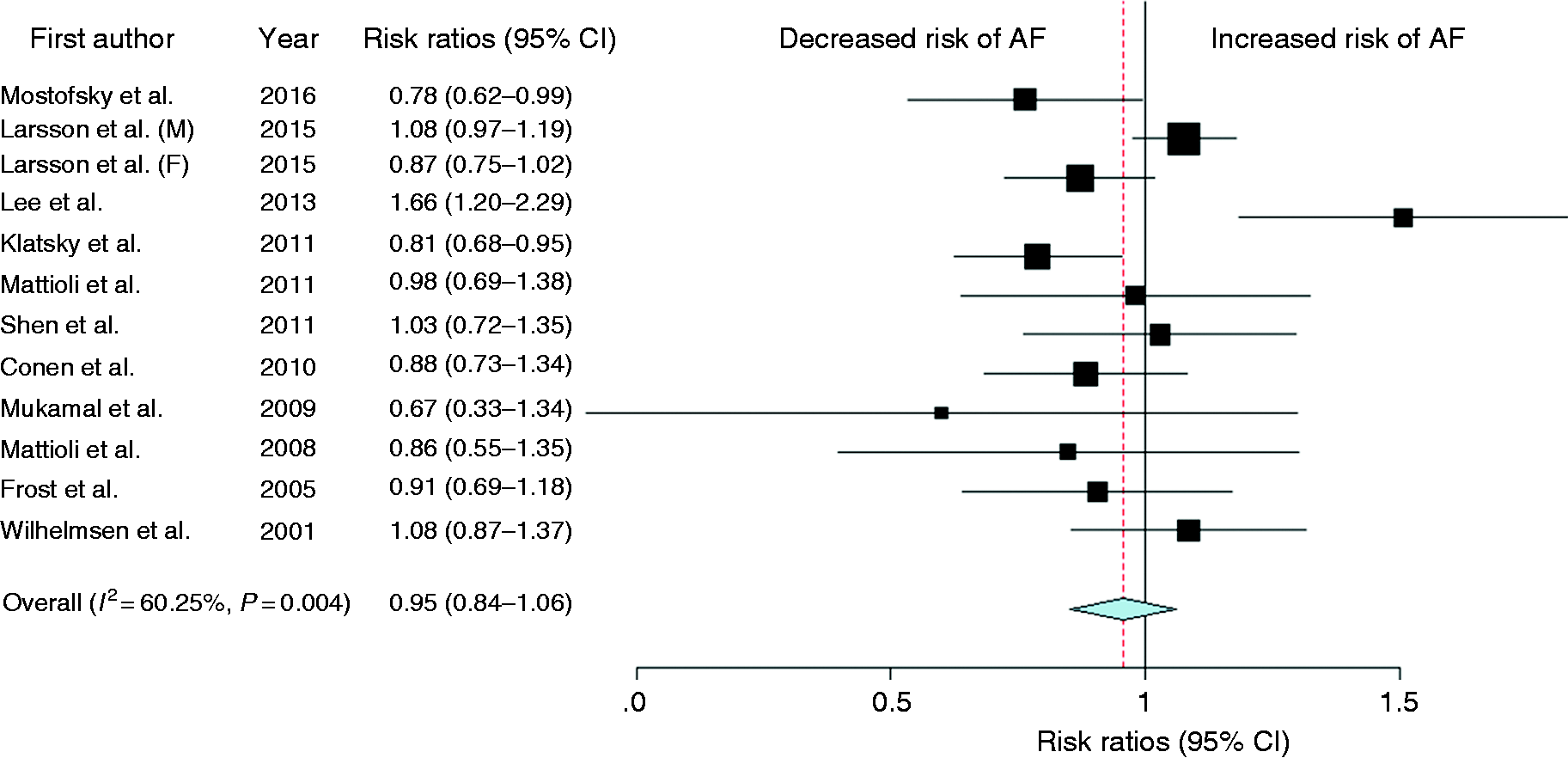
In our meta-analysis including 361,143 subjects, we found no significant association between the highest category of caffeine/coffee consumption and the incidence of AF. The results are consistent with recent meta-analyses.7–9 In addition, in sensitivity analyses, we did not find the association between caffeine/coffee consumption and the incidence of new-onset AF even after adjusting confounders and sensitivity analyses. Our results showed that caffeine consumption is unlikely to be related to the risk of developing new-onset AF and possibly yields a protective effect from AF. In general, caffeine contains several different substances, including lipids, carbohydrates, minerals, vitamins, alkaloids, and phenolic compounds. Although we could not identify the difference in ingredients in caffeine in the included studies, there was no association among the studies in subgroup analyses using geography and type of assessment for caffeine/coffee consumption. To date, biologic mechanisms for protective or causative effects of caffeine remain speculative. However, our study has certain limitations. First, although we performed sensitivity analyses, the pooled estimate is associated with considerable statistical heterogeneity, suggesting confounders. For example, some potential confounders (i.e. undiagnosed OSA, alcohol abuse, hypertension, central stimulant, a social stimulant, and a sleep aid 10 ) might not be excluded or adjusted in the final multivariable analyses. Second, we used only final regression models, which were usually adjusted for all possible variables in each study. However, adjusting for the same variables in all of the included studies is a challenge. Lastly, the lack of genetic information on the etiology of AF is also a limitation.
In conclusion, we found that caffeine or coffee consumption is not associated with the risk of new-onset AF. However, further prospective studies investigating this relationship with a larger sample size are needed.
Supplemental Material
CPR908385 Supplemental Material - Supplemental material for Is caffeine or coffee consumption a risk for new-onset atrial fibrillation? A systematic review and meta-analysis
Supplemental material, CPR908385 Supplemental Material for Is caffeine or coffee consumption a risk for new-onset atrial fibrillation? A systematic review and meta-analysis by Chayakrit Krittanawong, Anusith Tunhasiriwet, Zhen Wang, Ann M Farrell, Sakkarin Chirapongsathorn, HongJu Zhang, Takeshi Kitai and Davendra Mehta in European Journal of Preventive Cardiology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.