
Abstract

Obesity has been associated with arterial stiffness (AS) and increased risk of cardiovascular disease.1,2 Although aerobic exercise (AE) promotes positive effects on AS,3,4 obese individuals have presented an increase of AS after both acute maximal exercise and moderate-intensity continuous training (MICT).5,6 Higher AS following exercise, even if transitory, may contribute to sudden cardiovascular events by increasing left ventricular afterload and depressing coronary perfusion. 5 High-intensity interval training (HIIT) has shown superior results in cardiorespiratory fitness 7 and endothelial function. 8 However, the acute impact of HIIT on AS in obese individuals is not known. Considering that both moderate and vigorous AE are recommended for health maintenance, and that HIIT was recently stated as an alternative to MICT for cardiometabolic disease prevention, 9 it becomes pivotal to test the effects of HIIT on AS in the obese. Therefore, we investigated the acute effects of HIIT and MICT on AS in young obese women.
Fifteen young obese women, with a body mass index (BMI) range from 30–39.9 kg/m2 (Supplementary Material Table 1), with no history of chronic diseases or continuous medication use participated in the present crossover design study. They were randomly assigned to HIIT (4×4 min at 85–95% of heart rate (HR)max, interspersed with three minutes active recovery periods at 65–75% of HRmax), MICT (41 minutes at 65–75% of HRmax) and control condition (CO) (30 min at rest in the sitting position). The exercise protocols were performed on a treadmill, and were standardized to guarantee that they were isocaloric. 10 Central systolic blood pressure (cSBP), carotid-femoral pulse wave velocity (cfPWV) and augmentation index (AIx) were measured by SphygmoCor (AtCor Medical, Sydney, Australia) 2 at baseline, and one, 30 and 60 min after all experimental conditions. This study was approved by the local ethics committee, and registered as a clinical trial.
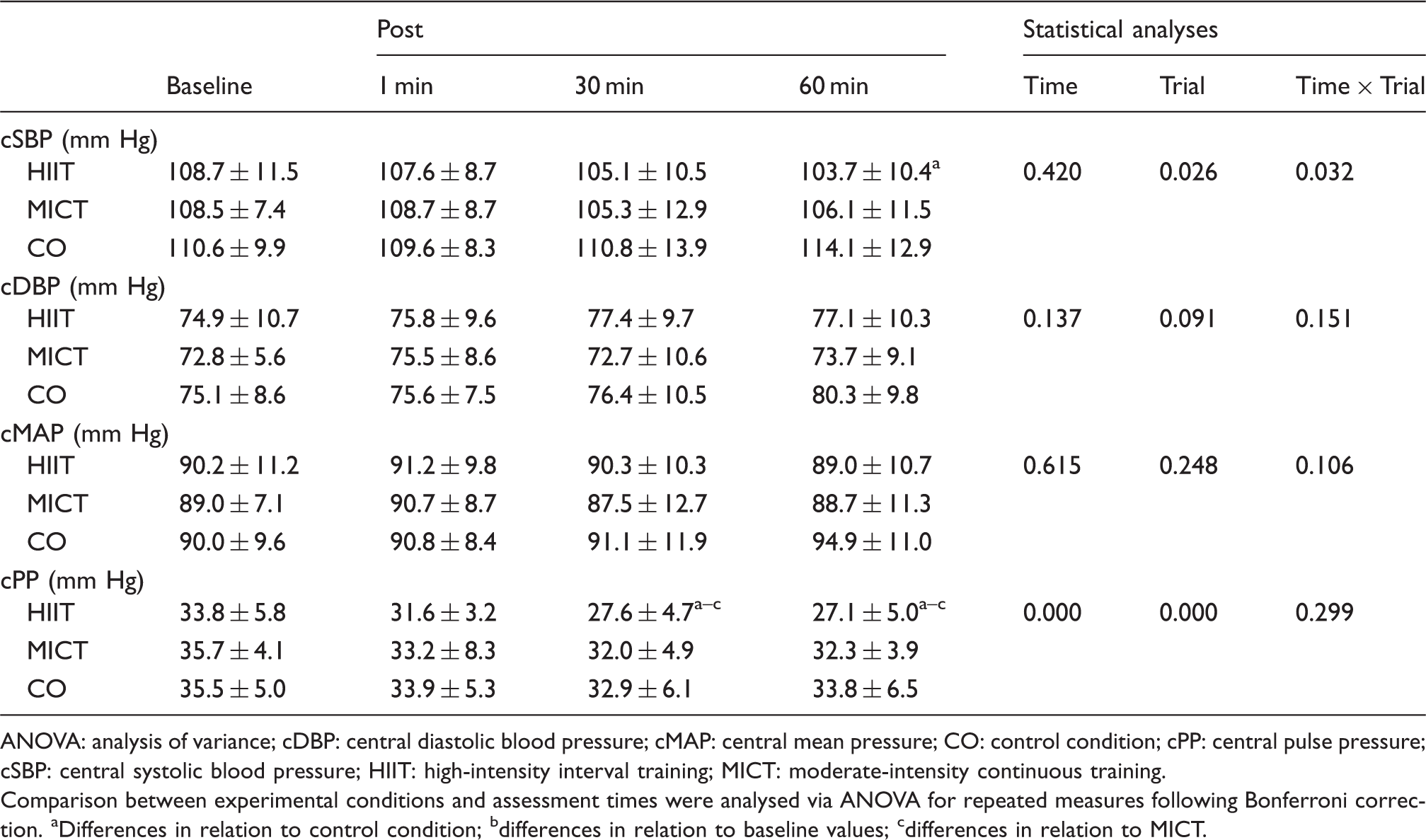
HR (179.7 ± 10.5 vs 137.3 ± 8.3 bpm, p < 0.001) was higher and the covered distance was lower (3.2 ± 0.3 vs 3.9 ± 0.5 km, p < 0.001) for HIIT when compared to MICT. However, the energy expenditure were similar between them (386 ± 38.5 vs 379.9 ± 35.2 kcal, p = 0.631, respectively). The effects of the experimental conditions on AS are presented in Table 1 and Figure 1. No intervention-time interactions were observed for cfPWV (p = 0.811) (Figure 1(a)). Significant intervention-time interactions were found for AIx (p < 0.001) and AIx adjusted for 75 beats per minute (AIx@75) (p = 0.049) (Figure 1(b) and (c)). A significant decline on AIx was observed after HIIT in comparison to CO at 30 and 60 min, and at 60 min when compared to MICT. Yet, the AIx presented a significant reduction following HIIT throughout the entire post-exercise recovery period, while the MICT decreased only at 60 min in comparison to baseline. Significant differences were observed in the AIx@75 after HIIT. The values were greater than CO at 60 min (p = 0.003), showing also a reduction in comparison to baseline at this time. The intervention-time interactions revealed a significantly higher HR after HIIT in comparison to MICT (p < 0.001) and CO (p < 0.001) at all post exercise moments. HR was higher for MICT than CO only at one minute, being also significant when compared to baseline (Figure 1(d)). Significant intervention-time interaction was verified for cSBP (p = 0.032). cSBP was significantly lower at 60 min following HIIT when compared to CO (p < 0.001).
(a) Carotid-femoral pulse wave velocity (cfPWV) at baseline and after experimental conditions; (b) augmentation index (AIx) at baseline and after experimental conditions; (c) augmentation index adjusted for 75 beats per minute (AIx@75) at baseline and after experimental conditions; (d) heart rate (HR) at baseline and after experimental conditions. Comparison between experimental conditions and assessment times were analysed via analysis of variance (ANOVA) for repeated measures following Bonferroni correction. *Differences in relation to baseline values; #differences in relation to control condition (interaction group vs time); $differences in relation to moderate-intensity continuous training (MICT) (interaction group vs time). Cardiovascular parameters at baseline and post (1, 30, and 60 min) experimental conditions. ANOVA: analysis of variance; cDBP: central diastolic blood pressure; cMAP: central mean pressure; CO: control condition; cPP: central pulse pressure; cSBP: central systolic blood pressure; HIIT: high-intensity interval training; MICT: moderate-intensity continuous training. Comparison between experimental conditions and assessment times were analysed via ANOVA for repeated measures following Bonferroni correction. aDifferences in relation to control condition; bdifferences in relation to baseline values; cdifferences in relation to MICT.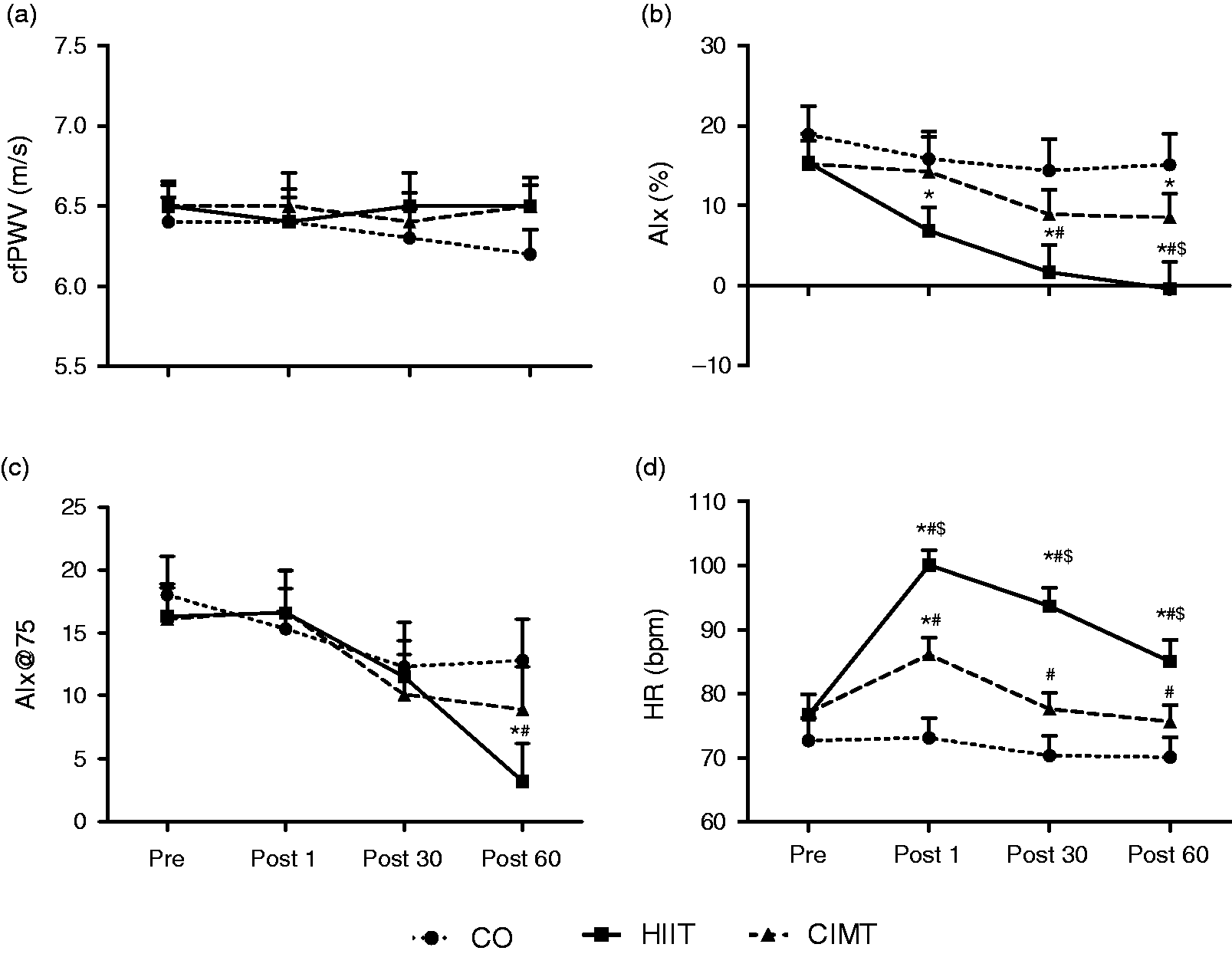
Our main finding are that both HIIT and MICT did not increase cfPWV acutely, and only HIIT was able to reduce AIx and cSBP in obese young women. These findings demonstrate the vascular safety of MICT and HIIT as well as the potential advantage of HIIT over MICT in promoting a transient reduction on AIx and cSBP in this population.
Although it is well established that AE contributes to the reduction of AS, these responses seem to be contrasting in obese.5,6 It has been demonstrated that obese individuals present an increase of AS after maximal exercise 5 and MICT. 6 However, the mechanisms explaining this increase of AS after exercise are unclear. It is speculated that increased sympathetic nerve activity (SNA) at rest and an exaggerated sympathetic response to exercise-induced stress in obese individuals could be related to these responses. 4 This obesity-related sympathetic hyperactivity could also be attributed to oxidative stress, which is increased after exercise. 4 Additionally, oxidative stress could induce an increase in AS in obese individuals by decreasing nitric oxide (NO) bioavailability, leading to endothelial dysfunction. 4
However, our results disagree with previous findings.5,6 This discrepancy could be attributed to sex differences in AS response after exercise. Indeed, Yan and colleagues 11 found a significant effect of sex on changes in AIx, wherein women have two times greater reduction in AIx than men, even when normalized by HR (AIx@75%). It might happen due to the fact that women have greater β-adrenergic receptor sensitivity (β-ARS), which offsets α-adrenergic vasoconstriction resulting in less vasoconstriction for a given amount of SNA (or local norepinephrine). 12 Other mechanisms may be related to the direct effect of estrogen in enhancing β-ARS, or indirectly, by increased NO availability, which may increase β-adrenergic-mediated vasodilation in the peripheral vasculature. 12 Accordingly, considering that AIx is considerably influenced by the peripheral vasculature, a higher dilation could induce a later return of the wave reflection, reducing therefore the AIx. This reduction might also cause a reduction in cSBP, as demonstrated in the present study. Central rather than peripheral BP has been suggested as an important predictor of cardiovascular risk. 13 In contrast to the current findings, Zeigler et al. 6 found an increase of cSBP after an acute bout of MICT in obese men. This outcome has important clinical implications, since minimal reduction in central blood pressure could decrease myocardial work and force imposed on the aorta during the ejection phase, decreasing the chance of ventricular hypertrophy and cardiac remodeling. 13
Despite the acute positive effects of HIIT on AS parameters, HIIT also seems to elicit chronic enhancements on blood pressure, alike other exercise interventions, as well as promote superior improvements on cardiorespiratory fitness. These findings reinforce the pleiotropic effects of exercise on cardiovascular parameters in populations without cardiovascular diseases, 7 and corroborate with the recent findings on the superiority of HIIT rather than MICT on cardiorespiratory fitness in obese and hypertensive individuals. 14
In summary, a single bout of HIIT can reduce AIx and cSBP, without any change in cfPWV in obese young women. Our findings suggest that HIIT is safe and may have cardiac beneficial effect by inducing transient peripheral vascular enhancements after a single bout of exercise. Future studies are required to test the acute effect of HIIT on AS in obese young men, as well as the chronic impact of HIIT on AS in both obese young women and men.
Supplemental Material
CPR909302 Supplemental Material - Supplemental material for Acute effects of high-intensity interval training and moderate-intensity continuous training on arterial stiffness in young obese women
Supplemental material, CPR909302 Supplemental Material for Acute effects of high-intensity interval training and moderate-intensity continuous training on arterial stiffness in young obese women by Karin Hortmann, Pierre Boutouyrie, João C Locatelli, Gustavo H de Oliveira, Caroline F Simões, Victor H de Souza Mendes, Higor B Reck, Rogério TP Okawa and Wendell A Lopes in European Journal of Preventive Cardiology
Footnotes
Author contribution
WAL and RTPO conceived the study design. JCL, WAL, GHO, RTPO, CFS, KH, HBR, and VHSM collected data and performed the assessments. WAL, HBR, RTPO, and CFS analyzed the results. KH, JCL, PB, and WAL drafted the article. PB, WAL, RTPO critically revised the manuscript. All authors have reviewed and made an agreement on this version of the manuscript.
Declaration of conflicting interests
The author(s) declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Fundação Araucária de Apoio ao Desenvolvimento Científico e Tecnológico do Estado do Paraná (FA) e do Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (CP 20/18 PPP).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.