
Abstract

Dual antiplatelet therapy (DAPT) consisting of aspirin and a P2Y12 inhibitor is the standard treatment in patients undergoing percutaneous coronary intervention (PCI). 1 However, the optimal duration of DAPT continues to be a matter of debate. Current American College of Cardiology (ACC)/American Heart Association (AHA) and European Society of Cardiology (ESC) guidelines recommend at least 12 months of DAPT in patients with acute coronary syndrome (ACS) and 6 months in patients with stable coronary artery disease undergoing PCI with a drug-eluting stent.2,3 Patients who are at high risk of bleeding or develop significant overt bleeding may be considered for a shorter duration of DAPT (≤3 months).2,3 However, with advancement in stent technology and the introduction of newer potent P2Y12 inhibitors, the current recommendations on DAPT duration have been questioned. Recently, a short duration of DAPT (1–3 months) followed by single antiplatelet therapy with a P2Y12 inhibitor (aspirin-free strategy) has been suggested. This strategy was investigated in some studies with disparate results.4–7 We therefore performed a meta-analysis of available randomized controlled trials (RCTs) to compare the aspirin-free strategy with standard term DAPT in patients undergoing PCI.
This study was conducted according to the preferred reporting items for systematic review and meta-analysis (PRISMA) statement. Pubmed, Embase and Cochrane Central databases were searched for RCTs reporting outcomes on short-term DAPT (≤3 months) followed by P2Y12 monotherapy compared to standard term DAPT (12 months) in patients undergoing PCI. Four studies were included in the final meta-analysis.4–7 The primary outcome of interest was major bleeding defined by Bleeding Academic Research Consortium (BARC) type 3 or 5 bleeding. Secondary outcomes of interest were myocardial infarction (MI), stent thrombosis (definite or probable), ischemic stroke, all-cause mortality and cardiovascular mortality. Outcomes were analysed at 12 months follow-up period. Risk ratios (RRs) were calculated for each outcome and a random effects model was used to pool data.
A total of 29,089 patients was included in the analysis in four trials. Of this, 14,530 (≈50%) received aspirin-free strategy and 14,559 (≈50%) received standard term DAPT. Baseline characteristics were comparable between the two groups across the studies (Table 1). A total of 14,990 (51.5%) patients underwent PCI for ACS and 14,095 (48.5%) patients for stable coronary disease. The choice of P2Y12 inhibitor for monotherapy differed among trials. While two trials used ticagrelor,4,7 one trial used clopidogrel 6 and one trial used either ticagrelor or clopidogrel. 5 There was a significant reduction in major bleeding in the aspirin-free strategy group compared to the standard term DAPT group (RR 0.61, 95% confidence interval (CI) 0.38–0.95; P = 0.03) at 12 months’ follow-up. No significant difference was identified for the rest of the outcomes of MI (RR 1.06, 95% CI 0.90–1.25; P = 0.46), ischemic stroke (RR 1.16, 95% CI 0.66–2.04; P = 0.60), stent thrombosis (RR 1.16, 95% CI 0.79–1.70; P = 0.46), all-cause mortality (RR 0.87, 95% CI 0.71–1.06; P = 0.16) and cardiovascular mortality (RR 0.76, 95% CI 0.52–1.11; P = 0.15) between the two groups (Figure 1).
Baseline characteristics of patients of studies included in the analysis.
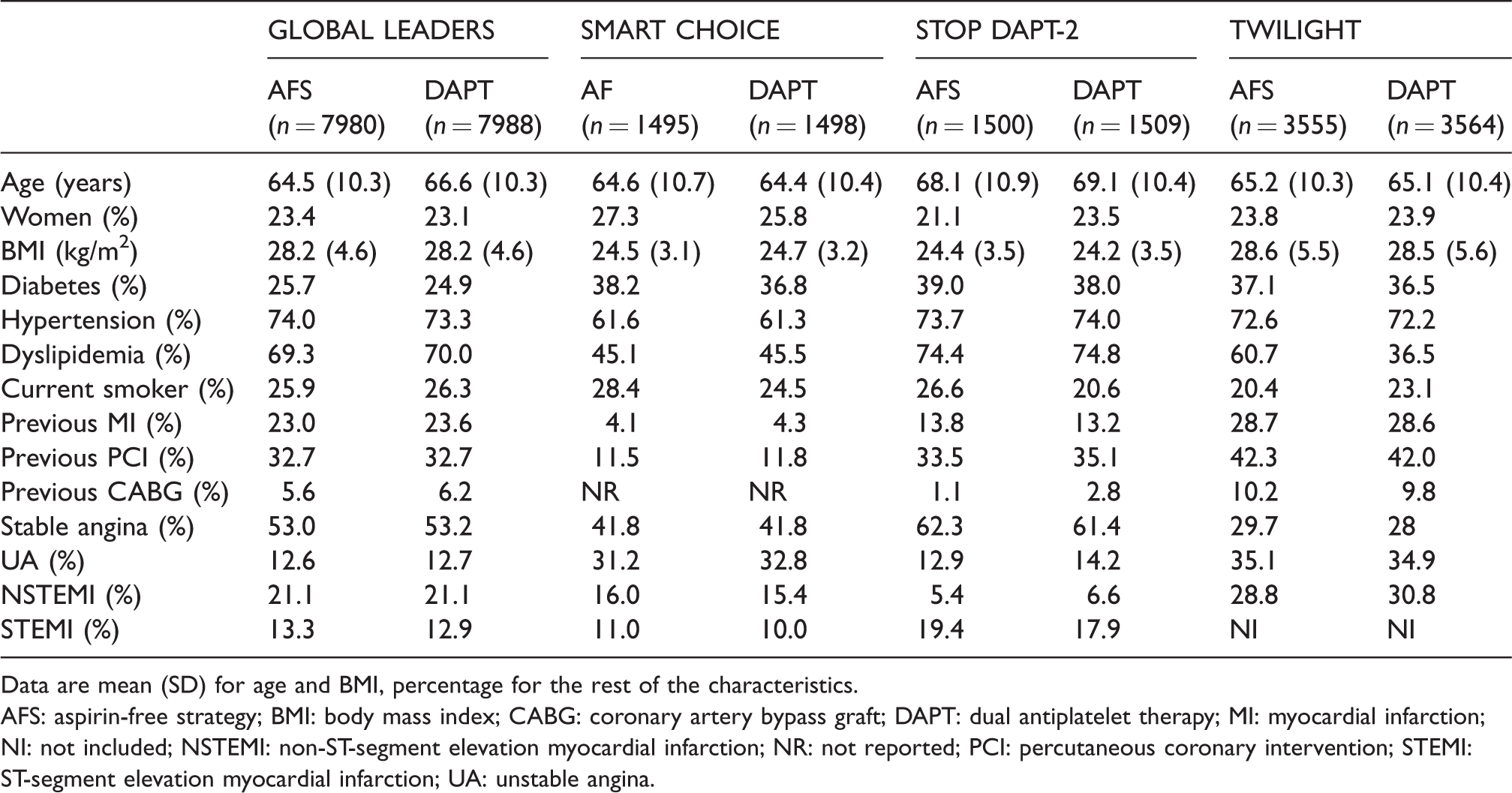
Data are mean (SD) for age and BMI, percentage for the rest of the characteristics.
AFS: aspirin-free strategy; BMI: body mass index; CABG: coronary artery bypass graft; DAPT: dual antiplatelet therapy; MI: myocardial infarction; NI: not included; NSTEMI: non-ST-segment elevation myocardial infarction; NR: not reported; PCI: percutaneous coronary intervention; STEMI: ST-segment elevation myocardial infarction; UA: unstable angina.
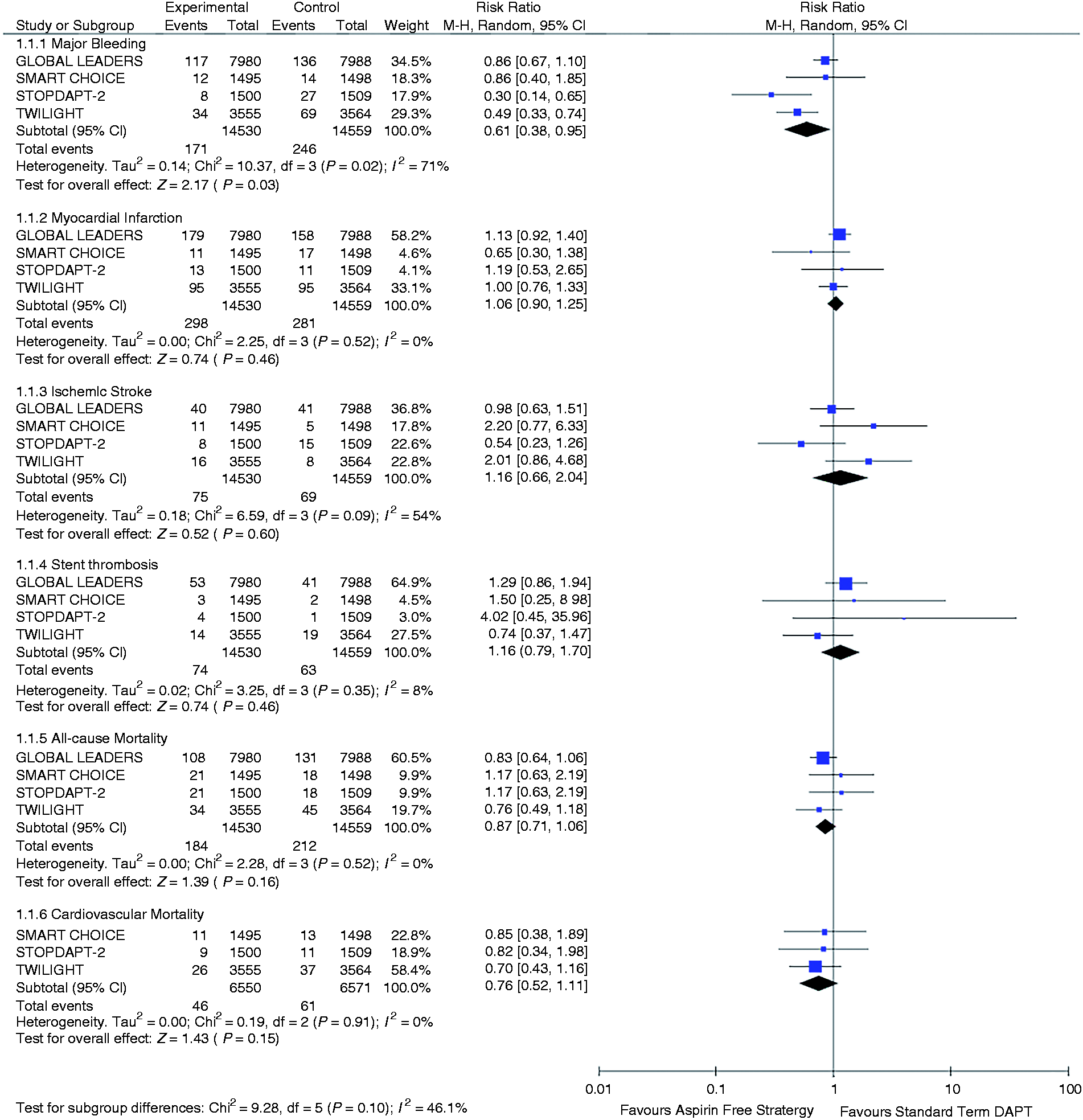
Forest plot comparing aspirin-free strategy and standard term dual antiplatelet therapy for the outcomes included.
Based on the available data from RCTs, the aspirin-free strategy was associated with a significant reduction in major bleeding as compared to standard term DAPT in patients with ACS or stable coronary artery disease undergoing PCI. There was no significant difference in the rate of MI, stent thrombosis, ischemic stroke, all-cause mortality and cardiovascular mortality between the two groups.
The strategy of short-term DAPT followed by P2Y12 monotherapy post-PCI was first investigated in the GLOBAL LEADERS trial. 4 This trial randomly allocated 15,968 patients undergoing PCI to receive either one month of DAPT followed by ticagrelor monotherapy for 23 months or standard term DAPT of 12 months followed by aspirin for 12 months. No significant difference in the incidence of bleeding was identified between the two groups. Subsequently, three more RCTs5–7 have investigated this strategy and found that short DAPT followed by P2Y12 monotherapy was associated with a significantly reduced bleeding risk without any increased risk of ischemic events compared to standard term DAPT. Similar results were also found in our meta-analysis. Although the exact reason for the observed benefits with an aspirin-free strategy may not be elucidated, there are several possible explanations. First, in the presence of effective P2Y12 blockage, aspirin offers limited advantages in platelet inhibition. The P2Y12 signaling pathway plays a central role in platelet activation and aggregation, and effective blockage of the P2Y12 receptor itself can result in a substantial degree of platelet inhibition. 8 Second, aspirin is associated with an increased risk of bleeding, especially gastrointestinal bleeding. So, withdrawing aspirin can help reduce bleeding complications without compromising antithrombotic effects. Also, with the advent of new second-generation stents there is a reduced incidence of stent thrombosis, and a shorter duration of DAPT might be sufficient to prevent thrombosis. Reduced adverse bleeding events with shorter duration DAPT might also result in improved treatment adherence.9,10
This study has certain limitations. First this was a study-level meta-analysis and individual patient data were not available. Second, the studies varied in their design and patient populations. Only one study was double blinded and the rest were open label studies, therefore a potential risk of bias exists in these studies. Similarly, one study enrolled patients at high risk of ischemic or bleeding complications based on predefined clinical and angiographic criteria, while the rest of the studies enrolled all comers undergoing PCI. Third, the studies differed in the choice of P2Y12 inhibitors in the DAPT regimen as well as for monotherapy, which might influence outcomes. Finally, we did not perform subgroup analysis in high-risk patients presenting with ACS as the outcomes were not separately reported in all the studies included. Given the limitations of current evidence, it would be appropriate to individualize DAPT regimens, after taking into consideration the ischemic and bleeding risk of a patient. The ongoing TICO trial (NCT02494895), which is comparing 3 months of DAPT followed by ticagrelor for 9 months to DAPT for 12 months in ACS patients, will provide more data and address some of these issues.
In conclusion, short-term DAPT (≤3 months) followed by P2Y12 monotherapy (aspirin-free strategy) is associated with a lower incidence of major bleeding with no significant difference in MI, ischemic stroke, stent thrombosis, all-cause mortality and cardiac mortality compared to standard term DAPT (12 months) in patients undergoing PCI.
Footnotes
Author contribution
All author(s) have contributed substantially to the manuscript and meet the criteria for authorship.
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.