
Abstract
Elevated lipoprotein(a) (Lp(a)) has been established as an independent causal risk factor for cardiovascular disease (CVD) and recent guidelines suggest that Lp(a) should be measured at least once in an adult’s lifetime. 1 Lp(a), a subtype of low density lipoprotein (LDL) carrying a single molecule of apolipoprotein (apo) (a), is believed to have thrombogenic, atherogenic and inflammatory properties. 1 The critical questions are, however, how can we effectively decrease elevated Lp(a) and whether an Lp(a) reduction is translated into clinical benefit? Multiple clinical trials have shown that inhibition of proprotein convertase subtilisin/kexin type 9 (PCSK9) with monoclonal antibodies reduces Lp(a) levels by 20–30%. 2 Of particular interest, this moderate decrease seems to contribute to a reduction of non-fatal myocardial infarction as well as peripheral arterial disease and venous thromboembolism events, at least in patients with recent acute coronary syndrome on high-intensity statin treatment. 3 , 4
While recent investigations have attempted to unravel the underlying mechanisms of PCSK9 inhibition-associated Lp(a) decrease, these remain largely unclear. There are two possibilities: either increased catabolism or decreased production (Table 1).
Possible mechanisms for lipoprotein(a) (Lp(a)) lowering associated with proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibition.
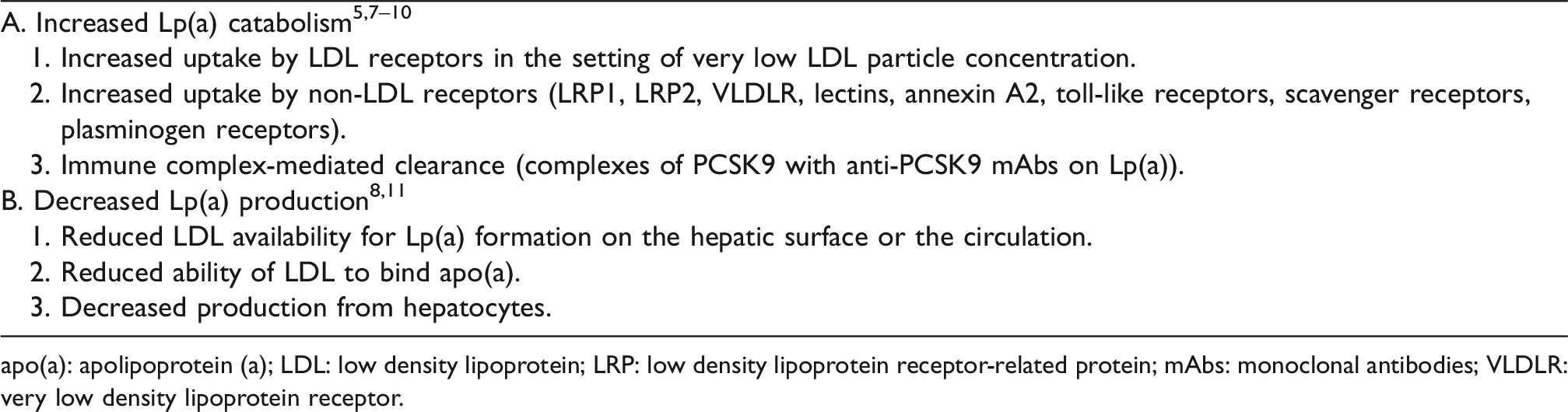
apo(a): apolipoprotein (a); LDL: low density lipoprotein; LRP: low density lipoprotein receptor-related protein; mAbs: monoclonal antibodies; VLDLR: very low density lipoprotein receptor.
Anti-PCSK9 monoclonal antibodies greatly upregulate LDL receptors and this could lead to increased uptake of circulating Lp(a) molecules. Indeed, a human kinetic study showed that alirocumab is associated with ∼25% increase of fractional catabolic rate of apo(a). 5 However, statins, which also enhance LDL receptor function, may actually increase circulating Lp(a) levels in humans. 6 To explain this discrepancy, we can speculate that Lp(a) uptake is modulated by other means than the LDL hepatic receptors. These could bind to apo(a), apoB, apoE or even oxidised phospholipids of Lp(a) and may include various lipoprotein receptors, lectins, annexin A2, toll-like and scavenger receptors as well as plasminogen receptors. 7 It is possible that PCSK9 facilitates degradation of these receptors, while inhibition of PCSK9 results in enhancing their capacity of removing Lp(a) from the circulation. Another possibility could be that in the case of very low LDL particle concentration, as frequently observed during combination lipid-lowering therapy with PCSK9 inhibitors, Lp(a) could become a competitive ligand for LDL receptors. This may explain why evolocumab and atorvastatin combination therapy, but not evolocumab monotherapy, accelerates Lp(a) particle catabolism. 8 Also, a greater Lp(a) reduction in patients with lower LDL cholesterol levels was noticed in another study. 9 A third possibility is that as PCSK9 preferentially associates with Lp(a) particles in subjects with elevated Lp(a), 10 administration of anti-PCSK9 monoclonal antibodies would result in the formation of immune complexes on the surface of Lp(a) and therefore increased immune complex-mediated clearance of Lp(a).
On the other hand, there is a growing body of evidence suggesting that anti-PCSK9 therapy may reduce Lp(a) synthesis, secretion or assembly. Extracellular assembly of Lp(a) may occur on the hepatocyte surface or in the circulation. In this case, decreased LDL particle concentration as a result of PCSK9 inhibition is expected to result in reduced LDL availability for Lp(a) formation. Also, inhibition of PCSK9, which is present on LDL particles, 10 may decrease their ability to bind with apo(a). Furthermore, decreased Lp(a) production from hepatocytes may be at play since PCSK9 enhances Lp(a) production from hepatocytes and this effect is blunted by alirocumab. 11 Although underlying molecular mechanisms remain unknown, a reduction in intracellular apo(a) seems to be the most likely one. 11 In this context, evolocumab monotherapy, but not in combination with atorvastatin, lowered plasma Lp(a) pool size by lowering the production of Lp(a) in a human kinetic study. 8 To what extent and under which circumstances the above mechanisms operate is currently unknown.
Few clinical studies have addressed the question of how PCSK9 inhibitors lower Lp(a) plasma levels. The idea is that if Lp(a) is cleared by the LDL receptor, similar to LDL, then PCSK9 inhibition would be expected to induce a concordant LDL cholesterol/Lp(a) response in an approximately 2:1 ratio. In a small study of patients (n = 26) receiving PCSK9 inhibition, although 96% of patients demonstrated a >35% reduction of LDL cholesterol, only 62% experienced a >10% reduction of Lp(a), thus suggesting a high level of discordance between LDL cholesterol and Lp(a) response. 12 The correlation between %LDL cholesterol reduction and %Lp(a) reduction was moderate (r = 0.56, p < 0.01). In fact, while some patients demonstrated negligible lowering or even an increase in Lp(a) levels, other patients experienced profound Lp(a) lowering (e.g. >60%). 12 Of note, in contrast to the ‘regression to the mean effect’, subjects with the greatest Lp(a) reduction had significantly lower baseline Lp(a) levels compared with those with minimal or no Lp(a) lowering. 12 In another study, data from four randomised phase 3 evolocumab trials were analysed (n = 895 patients). 13 The correlation between %LDL cholesterol reduction and %Lp(a) reduction was moderate (r = 0.37, p < 0.001). Although 94% of patients demonstrated a >35% reduction of LDL cholesterol, a discordant response (i.e. LDL cholesterol reduction >35% but Lp(a) reduction <10%) was observed in almost 20% of patients. Again, the prevalence of discordance was higher with increasing baseline Lp(a) levels. 13 Only ∼3% of study population experienced the opposite discordance pattern, i.e. LDL cholesterol reduction <35% but Lp(a) reduction >10%. Of note, greater Lp(a) reduction was observed in patients achieving lower on-treatment LDL cholesterol levels.
In this issue of the European Journal of Preventive Cardiology, a post-hoc pooled analysis of 10 randomised trials from the ODYSSEY phase 3 trials including 1709 patients is published. 14 Of patients receiving alirocumab, 71% exhibited a concordant response (i.e. LDL cholesterol reduction >35% and Lp(a) reduction >10%). However, ∼22% had a discordant response, which includes ∼13% demonstrating LDL cholesterol reduction >35% but Lp(a) reduction <10% as well as ∼9% experiencing an LDL cholesterol reduction <35% but Lp(a) reduction >10%. Surprisingly, ∼7% of patients had LDL cholesterol reduction <35% and Lp(a) reduction <10%. In contrast to previous studies, baseline Lp(a) levels did not alter the prevalence of discordant responses to alirocumab. 14 This analysis, although post-hoc, has many strengths. The authors did a great job analysing prospectively collected data from 10 randomised controlled double-blind trials. The sample size is large enough to perform comprehensive analyses. Also, Lp(a) was measured by a validated immunoturbimetric assay which is apo(a) isoform independent. Are there any limitations? First, the dose of alirocumab was not the same across study populations: most, but not all, patients received the 75 mg dose. This may have affected the degree of LDL cholesterol and Lp(a) lowering. Second, not all patients were receiving background statin therapy. The effect of PCSK9 inhibition on Lp(a) may be different depending on concomitant statin use. 8 Third, as many as 16% of study participants demonstrated an LDL cholesterol reduction of <35%. This is hard to explain since patients with known homozygous familial hypercholesterolaemia were excluded. Could this less-than-anticipated LDL cholesterol reduction be a marker of poor compliance with treatment? Determination of total PCSK9 levels pre- and post-treatment could have provided a diagnostic tool for explaining an apparent resistance to PCSK9 inhibitors. 15 Fourth, previous studies suggested that patients with low baseline Lp(a) levels respond better to PCSK9 inhibition. 12 , 13 This may imply that large apo(a) isoforms respond better to PCSK9 inhibition. The prevalence of specific apo(a) phenotypes is not known in the present analysis. However, the lack of association between baseline Lp(a) levels and degree of Lp(a) reduction is in line with a previous study showing that alirocumab-induced Lp(a) reduction is independent of apo(a) phenotypes. 9 Fifth, LDL cholesterol was not corrected for the cholesterol content of Lp(a) (Dahlen correction). Uncorrected LDL cholesterol may not achieve the expected reduction in the presence of high levels of Lp(a) and this may partially explain at least some of the discordant response. Finally, apoE genotyping would provide further information since apoE2 is associated with lower Lp(a) levels and could thus affect the degree of Lp(a) lowering. 7
So, what does this study add to our current imperfect wisdom about Lp(a) lowering with PCSK9 inhibition? It largely confirms that LDL receptor uptake is not the major pathway of Lp(a) lowering. Other mechanisms of decreased production and increased catabolism appear to operate as discussed above. The response of these LDL receptor-independent mechanisms to PCSK9 inhibition seems not to be the same in every patient and this may explain the observed discordant results. It is obvious that dedicated mechanistic studies will shed more light to this mystery. For the time being, any Lp(a) reduction with PCSK9 inhibition is more than welcome. For patients with extensive or progressive atherosclerotic CVD and very high Lp(a) levels, lipoprotein apheresis on top of standard treatment remains the most appropriate therapy while awaiting specific anti-apo(a) medications to arrive. 16
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.