
Abstract
Background
A wrong traditional belief persists among people that opium consumption beneficially affects cardiovascular disease and its risk factors. However, no evidence exists regarding the effect of opium consumption or cessation on the long-term risk of major adverse cardio-cerebrovascular events after coronary artery bypass grafting. We therefore aimed to evaluate the effect of persistent opium consumption after surgery on the long-term outcomes of coronary artery bypass grafting.
Methods
The study population consisted of 28,691 patients (20,924 men, mean age 60.9 years), who underwent coronary artery bypass grafting between 2007 and 2016 at our centre. The patients were stratified into three groups according to the status of opium consumption: never opium consumers (n = 23,619), persistent postoperative opium consumers (n = 3636) and enduring postoperative opium withdrawal (n = 1436). Study endpoints were 5-year mortality and 5-year major adverse cardio-cerebrovascular events, comprising all-cause mortality, acute coronary syndrome, cerebrovascular accident and revascularisation.
Results
After surgery, 3636 patients continued opium consumption, while 1436 patients persistently avoided opium use. The multivariable survival analysis demonstrated that persistent post-coronary artery bypass grafting opium consumption increased 5-year mortality and 5-year major adverse cardio-cerebrovascular events by 28% (hazard ratio (HR) 1.28, 95% confidence interval (CI) 1.06–1.54; P = 0.009) and 25% (HR 1.25, 95% CI 1.13–1.40; P < 0.0001), respectively. It also increased the 5-year risk of acute coronary syndrome by 34% (sub-distribution HR 1.34, 95% CI 1.16–1.55; P < 0.0001).
Conclusions
The present data suggest that persistent post-coronary artery bypass grafting opium consumption may significantly increase mortality, major adverse cardio-cerebrovascular events and acute coronary syndrome in the long term. Future studies are needed to confirm our findings.
Keywords
Introduction
According to the United Nations Office on Drugs and Crime, in 2015, approximately 17.7 million people used opium or its derivatives illicitly worldwide. 1 Opium is still the most commonly consumed substance after tobacco in the developing countries of the Middle East and many Asian countries.2,3 In addition to geographical proximity to the major producers of opium in the world and ease of availability, one reason for the high consumption of opium in Asian countries might be a traditional belief among Eastern people and even medical staff that opium may have ameliorating effects on cardiovascular disease (CVD) as well as diabetes mellitus, hypertension and dyslipidemia.4–9 Based on this belief, opium consumption is common among patients undergoing coronary artery bypass grafting (CABG). Over the past decade, many studies have been performed to evaluate the effect of opium consumption on blood lipid and glucose profile and also on CVD. Multiple clinical and animal studies have shown that not only does opium consumption not confer a beneficial effect in improving glyaemic control and lipid profile and preventing CVD, but also it may aggravate metabolic disturbances and increase the risk of CVD.10,11 However, very little is known about the effect of persistent opium consumption after surgery on the outcomes of CABG, with the majority of the studies having evaluated only short-term post-CABG outcomes. Accordingly, in the present study, we sought to evaluate the effect of persistent postoperative opium consumption on the long-term outcomes of patients following CABG.
Methods
Study population
This historical cohort study was conducted using the CABG Follow-up Registry of Tehran Heart Center.12,13 Between 2007 and 2016, 28,691 patients (mean age 60.9 years, 20,924 men) underwent CABG at our centre and were included in this study. The patients were stratified into three groups according to their status of opium consumption (either smoking opium or drinking opium dissolved in tea) in follow-ups: those who never consumed opium (n = 23,619), those who continued their opium consumption after surgery either constantly or intermittently (n = 3636) and those who reported enduring postoperative opium cessation (n = 1436). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a prior approval by the ethics committee of Tehran Heart Center, and verbal informed consent was obtained from all the patients.
Follow-up protocol
The patients were followed at 6 and 12 months after surgery and then annually through direct visits. Those who were unable to attend direct clinic visits were followed through telephone interviews. On each visit, the patients’ demographic characteristics, CVD risk factors (i.e. diabetes mellitus, hypertension, dyslipidemia, family history of premature coronary artery disease, cigarette smoking and opium consumption), laboratory findings, and the occurrence of major adverse cardio-cerebrovascular events (MACCEs; defined as a composite of all-cause mortality, acute coronary syndrome (ACS), stroke or transient ischaemic attack, and the need for repeat revascularisation (percutaneous coronary intervention or redo-CABG)) were recorded. Also registered was the study population’s achievement of the target blood pressure and serum low-density lipoprotein levels. A family history of premature coronary artery disease was defined as having a first-degree relative with a history of coronary artery disease including acute myocardial infarction or \documented coronary artery disease (through invasive coronary angiography or computed tomography coronary angiography) in a male person aged under 55 years and/or a female individual aged under 65 years.
Study endpoints
In the current study, MACCEs constituted the primary composite endpoint, while ACS and all-cause mortality comprised the secondary endpoints.
Statistical methods
Normally distributed variables were described as mean with standard deviation (SD) and were compared between three groups of opium consumption status using the one-way analysis of variance (ANOVA) test. Skewed distributed variables were expressed as median with interquartile range boundaries. They were compared between the three above-mentioned groups applying the Kruskal–Wallis test. The normality of the variables was checked using histogram charts as well as descriptive measures of central tendency and dispersion. Categorical variables were compared between the three opium consumption status groups using the chi-squared test. The unadjusted and adjusted effect of opium consumption status on mortality and MACCEs was measured by applying the Cox proportional hazards model, and the results were reported through hazard ratio (HR) with corresponding 95% confidence intervals (CIs). The components of MACCEs, including ACS, revascularisation and cerebrovascular accident, were considered in the competing risks setting, and each was analysed considering death before the event occurred as the competing event. The unadjusted and adjusted effects were reported as sub-distribution HR with 95% CIs. Those covariates, which were known as risk factors for the above-mentioned events after surgery, and were not evenly distributed among the three groups of opium consumption status with P values less than 0.05, were considered as potential confounders. Statistical analyses were conducted using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA). Competing risk analyses were done applying the ‘stcrreg’ module in Stata software version 14.2.
Results
Population
The baseline characteristics of the study population are depicted in Table 1. Patients who were opium consumers at the time of surgery (either those who continued opium consumption after surgery or those who reported persistent cessation) were younger, were more likely to be men and to smoke cigarettes and were less likely to have diabetes mellitus, hypertension and dyslipidemia compared to never opium consumers. There were no meaningful differences between postoperative opium consumers and persistent opium quitters with respect to these variables. Furthermore, while significant left ventricular systolic dysfunction defined as left ventricular ejection fraction less than 40% was significantly higher in opium consumers who continued (40.8%) or quitted (39.7%) opium consumption after surgery compared to never opium consumers (33.9%); there was no significant difference between the two former groups in this regard. Although the amount of opium consumption at baseline was not different between the two groups of persistent postoperative opium consumption and enduring postoperative opium cessation, the patients in the second group had a significantly lower median duration of opium consumption before surgery than did those in the first group (10 months vs. 15 months, respectively; P < 0.001).
Baseline characteristics of the study population based on status of opium consumption.
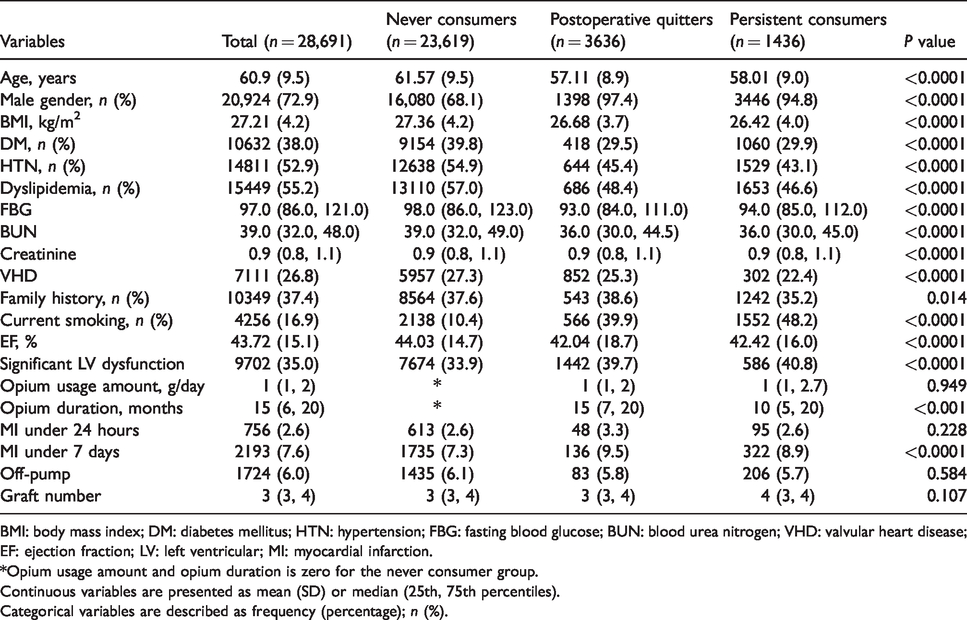
BMI: body mass index; DM: diabetes mellitus; HTN: hypertension; FBG: fasting blood glucose; BUN: blood urea nitrogen; VHD: valvular heart disease; EF: ejection fraction; LV: left ventricular; MI: myocardial infarction.
*Opium usage amount and opium duration is zero for the never consumer group.
Continuous variables are presented as mean (SD) or median (25th, 75th percentiles).
Categorical variables are described as frequency (percentage); n (%).
Follow-up
The follow-up ranges from 3 months to 10.5 years. The median follow-up duration was 55.95 months, with the interquartile range of 55.03–56.87 months. The follow-ups were successfully completed in 96.72% of the patients. We evaluated the 5-year outcomes of CABG.
Endpoints
At 5 years, all-cause mortality was reported in 9.7% of the never opium consumer group, 10.2% of the persistent postoperative opium consumption group and 5.3% of the enduring postoperative opium withdrawal group (P < 0.001). The univariate survival analysis revealed that persistent opium consumption after surgery was not associated with increased 5-year mortality compared to never opium consumers (HR 1.04, 95% CI 0.93–1.16; P = 0.466) (Table 2 and Figure 1). After adjustments for age, gender, body mass index, diabetes mellitus, dyslipidemia, hypertension, family history of premature CAD, cigarette smoking, history of previous myocardial infarction, and valvular heart disease, persistent opium consumption after surgery was associated with a 28% increased risk of 5-year mortality compared to never opium consumers (HR 1.28, 95% CI 1.06–1.54; P = 0.009) (Table 2). However, after adjustment for the afore-mentioned confounders, those who quitted opium consumption after surgery had no increased risk of 5-year all-cause mortality compared to never opium consumers (HR 1.09, 95% CI 0.83–1.43; P = 0.514). At 5 years, 18.7% of never opium consumers, 20.2% of persistent postoperative opium consumers and 14.8% of enduring postoperative opium quitters developed MACCEs (P < 0.0001). In the univariate survival analysis, persistent postoperative opium consumption was associated with increased 5-year MACCEs relative to never opium consumers (HR 1.10, 95% CI 1.02–1.20; P = 0.012) (Table 3 and Figure 2). After adjustments for competing confounders, persistent opium consumption after CABG was associated with a 25% increased risk of 5-year MACCEs compared to never opium consumers (HR 1.25, 95% CI 1.13–1.40; P < 0.0001) (Table 3). The multivariate competing risk analysis revealed that persistent post-CABG opium consumption increased the risk of ACS by 34% (sub-distribution HR 1.34, 95% CI 1.16–1.55; P < 0.0001). (Supplementary Table 1 and Figure 3). However, there was no statistically significant association between opium consumption and the incidence of cerebrovascular accident (Supplementary Table 2 and Supplementary Figure 1) and the need for repeat revascularisation (Supplementary Table 3 and Supplementary Figure 2).
Effect of continuing versus quitting opium consumption after CABG in relation to never opium consumption on all-cause mortality.
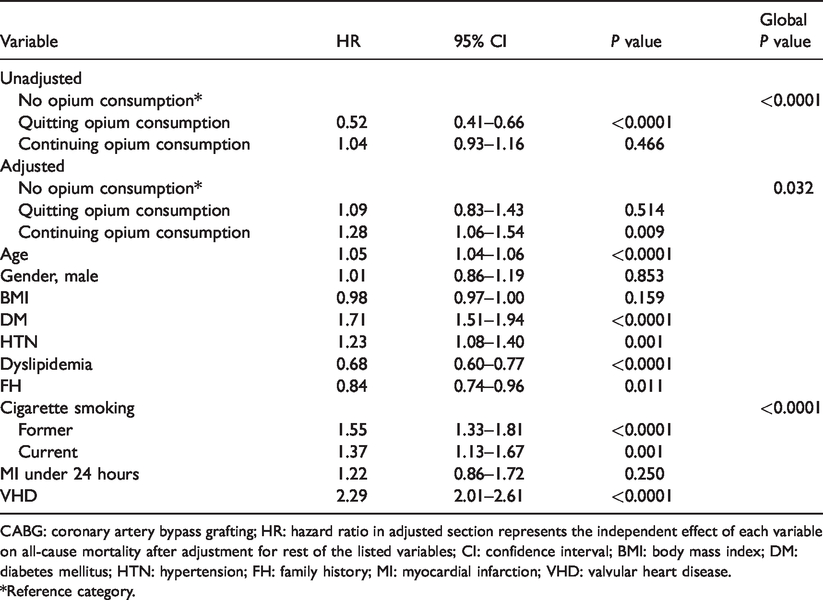
CABG: coronary artery bypass grafting; HR: hazard ratio in adjusted section represents the independent effect of each variable on all-cause mortality after adjustment for rest of the listed variables; CI: confidence interval; BMI: body mass index; DM: diabetes mellitus; HTN: hypertension; FH: family history; MI: myocardial infarction; VHD: valvular heart disease.
*Reference category.
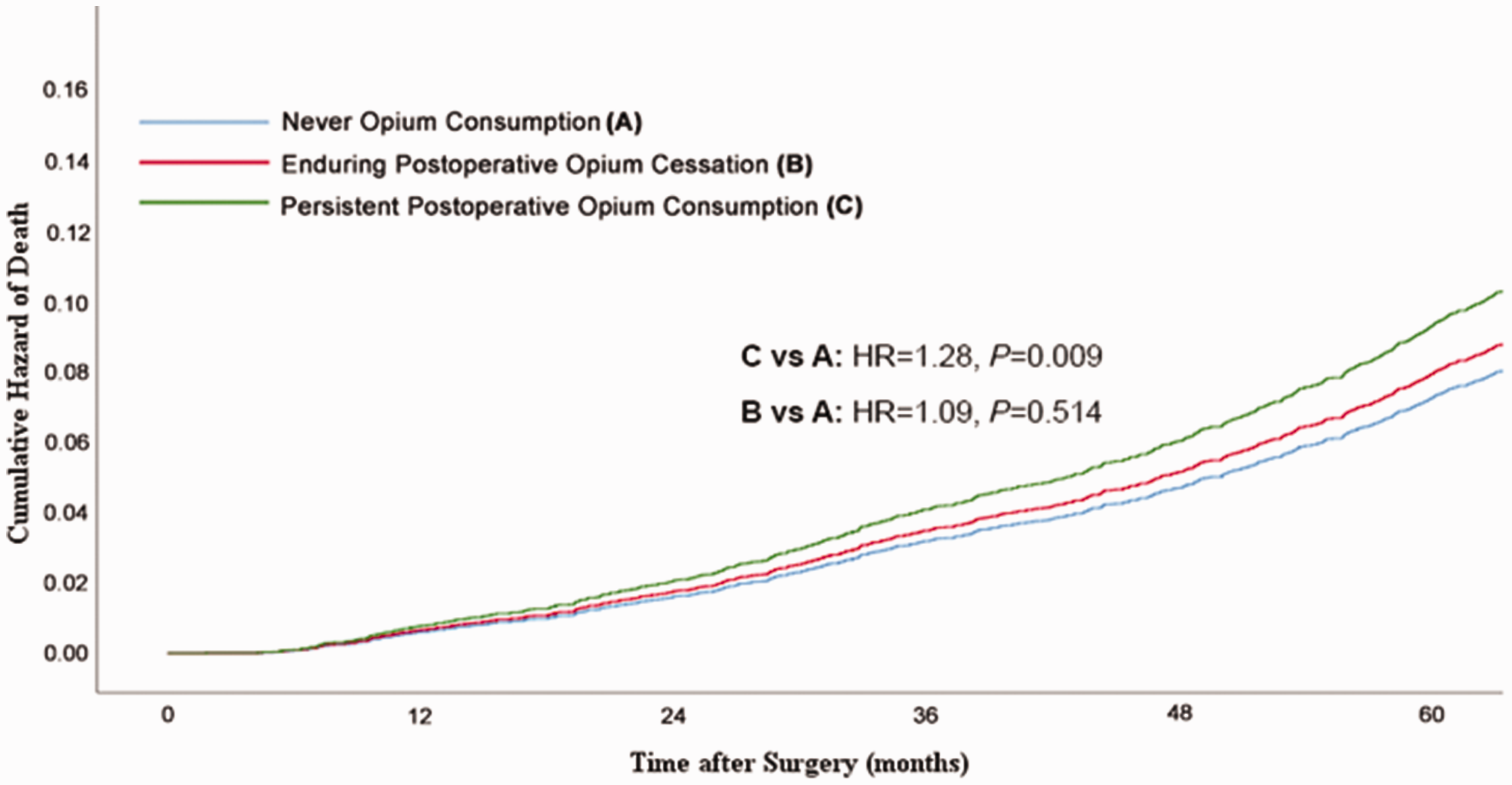
Adjusted cumulative hazard of death after coronary artery bypass grafting (CABG) surgery according to status of opium consumption.
Effect of continuing versus quitting opium consumption after CABG in relation to never opium consumption on major adverse cardio-cerebrovascular events.
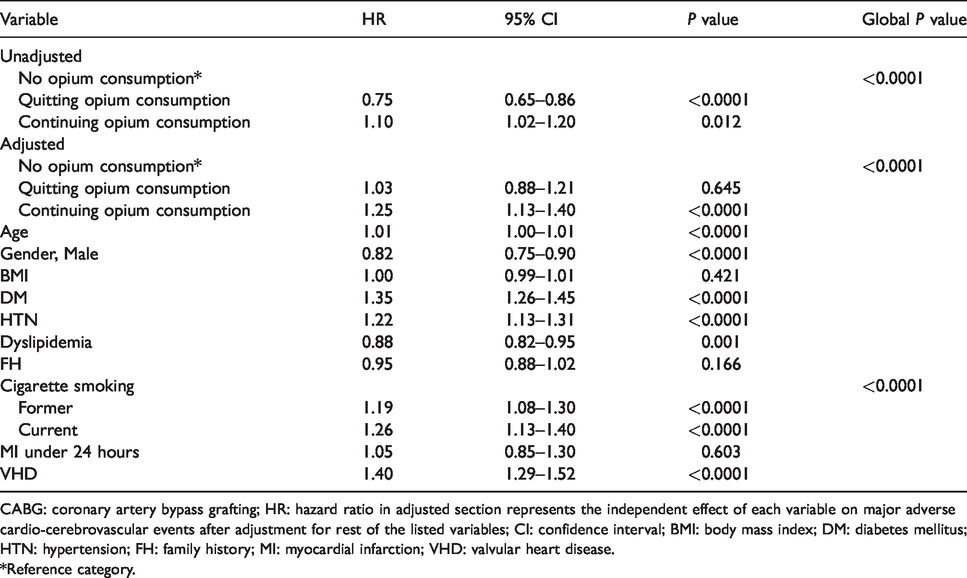
CABG: coronary artery bypass grafting; HR: hazard ratio in adjusted section represents the independent effect of each variable on major adverse cardio-cerebrovascular events after adjustment for rest of the listed variables; CI: confidence interval; BMI: body mass index; DM: diabetes mellitus; HTN: hypertension; FH: family history; MI: myocardial infarction; VHD: valvular heart disease.
*Reference category.
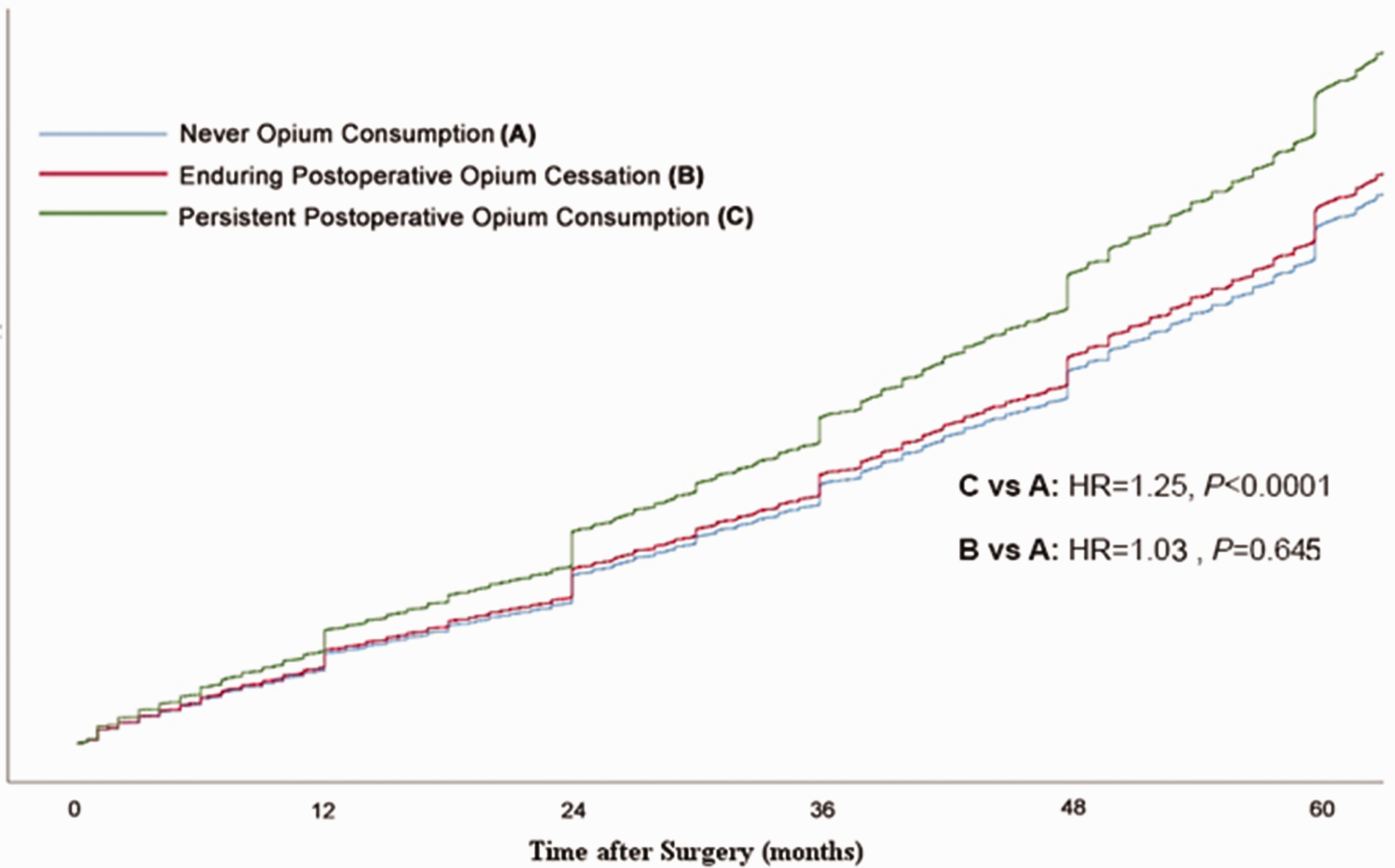
Adjusted cumulative hazard of major adverse cardio-cerebrovascular events (MACCEs) after coronary artery bypass grafting (CABG) surgery according to status of opium consumption.
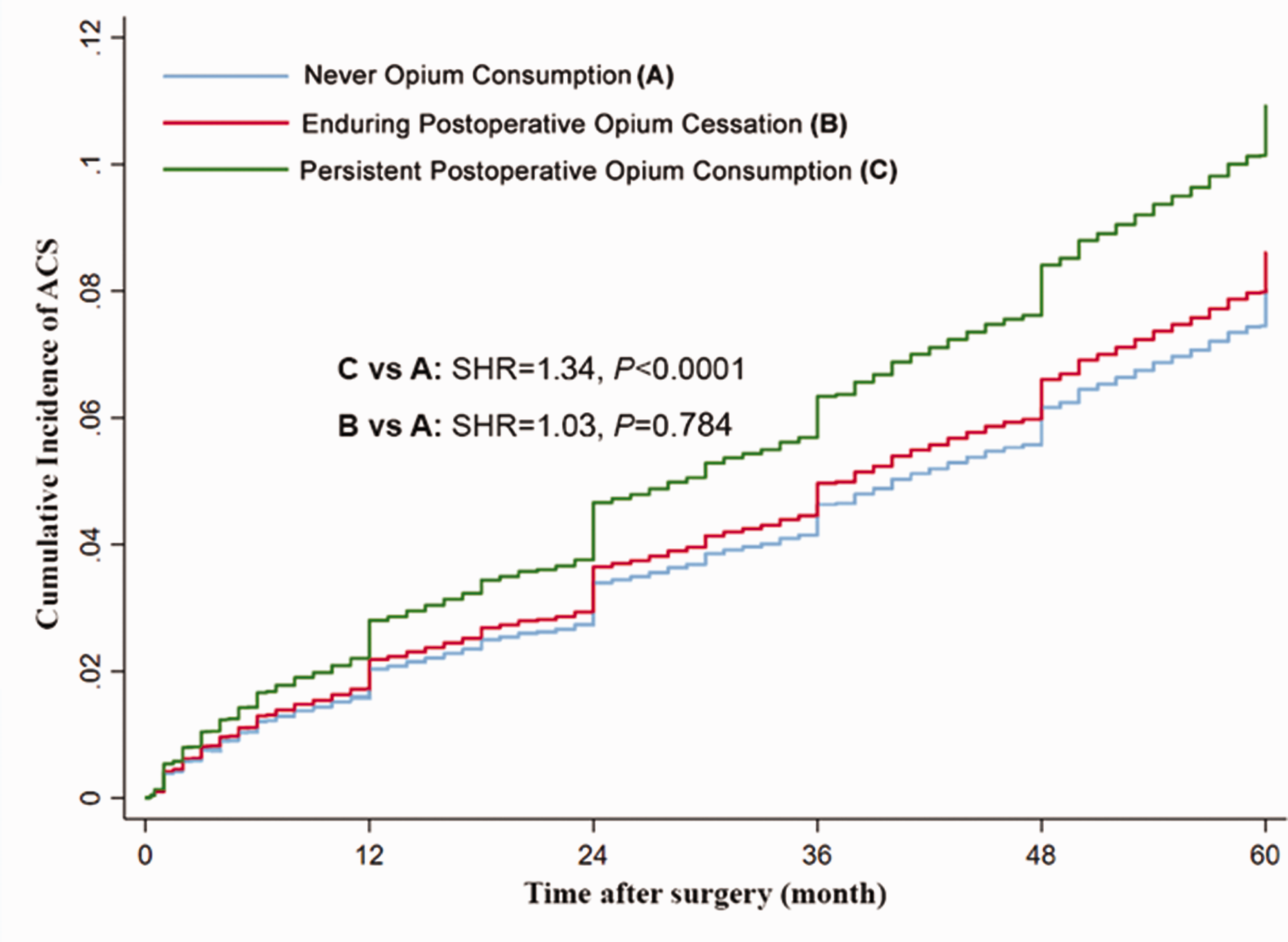
Adjusted cumulative incidence of acute coronary syndrome according to status of opium consumption in the presence of mortality as a competing event.
Discussion
Due to traditional beliefs regarding the heart-protective effect of opium and the fear on the part of cardiac surgeons and cardiologists of inducing acute coronary events as a result of opium withdrawal, many patients who undergo CABG continue opium consumption after surgery. In this study, we tried to evaluate the impact of persistent postoperative opium consumption on the long-term outcomes of CABG. The major finding of our study was that persistent post-CABG opium consumption increased the risk of mortality, MACCEs and ACS by 28%, 25% and 34%, respectively, while patients who quitted opium consumption after CABG had no increased 5-year risks of all-cause mortality and MACCEs compared to patients who never used opium.
Najafi et al. performed a study on 566 patients who underwent CABG and observed a borderline significant effect of opium consumption at the time of surgery compared to never opium consumers on long-term survival (HR 2.09, 95% CI 0.99–4.39; P = 0.06). 14 A thorough evaluation of the analysis signals for significant residual confounding and consequently overestimation of effect size due to lack of adjustment for gender and cigarette smoking. Meanwhile, they have not evaluated the effect of continuing or quitting opium consumption after surgery on long-term outcomes.
Not only is there a multitude of clinical and animal studies supporting an increased risk of CVD with opium consumption, 10 studies on chronic exposure to opioid analgesics demonstrate a substantial increased risk of incident CVD. Although the exact underlying mechanisms for the increased risk of MACCEs in opium-consuming patients remain to be elucidated, multiple mechanisms have been suggested for the increased risk of CVD and cardiovascular events in opium consumers.10,15 It is well known that inflammation and oxidative stress play a pivotal role in coronary atherosclerosis and also the susceptibility of existing atheromatous plaques to acute events. 16 Multiple studies have reported that opium could induce oxidative stress and inflammation by generating proinflammatory mediators.17–22 Recent studies have shown that opium consumption is associated with the presence of several novel risk factors for coronary artery disease. 22 Opium addicts have been shown to have higher levels of serum homocysteine, C-reactive protein, fibrinogen and plasminogen-activator inhibitor-1 than non-opium consumers, which may explain their tendency towards a higher burden of atherosclerosis and thrombotic events.23–25 It has been shown that low levels of testosterone in men and oestrogen in women are associated with coronary artery disease and increased risks of cardiovascular mortality.26,27 Previous studies have indicated that plasma testosterone and oestrogen levels are consistently low in opiate-addicted men and women, respectively, by comparison with controls. 28 Such findings might explain, at least in part, the association between opium consumption and the increased risk of cardiovascular events. Recent studies have also reported that opium consumption is associated with a type of hyperglycaemia and insulin resistance that is very similar to that seen in patients with type II diabetes, probably contributing to worse outcomes of CABG among opium consumers.29–31 There have also been recent reports of decreased efficacy and resistance to aspirin and clopidogrel in opium addicts, which might explain, in part, the increased risk of adverse events after CABG among opium consumers.32,33 Opium consumption suppresses the nervous system stimulation and causes sedation. 34 Hence, physical inactivity might be an underlying mechanism for worse outcomes among opium-consuming patients after CABG.35,36
Strengths and limitations
One of the major strengths of our study is its large sample size. Our study is, indeed, the largest study in the field, enabling it to demonstrate the differences in long-term outcomes between three groups of patients: those who never consumed opium, those with persistent postoperative opium consumption and those with enduring postoperative opium withdrawal. Our study, however, has some noteworthy limitations, which should be taken into consideration in the interpretation of its results. First, similar to other long-term follow-up studies, the design of the current study and the resultant loss to follow-ups precluded data assessment on the entire study population. Second, the opium consumption status among the study population was evaluated by means of self-reported data in the absence of biochemical testing for the confirmation of the accuracy of the information. Third, that opium lacks a standard size (like cigarettes) rendered the determination of the amount of opium consumption unfeasible, thereby preventing an assessment of a possible dose–response relationship between opium consumption and cardiovascular events. Fourth, our persistent postoperative opium consumption group could not have managed and maintained their risk factors within the normal range, resulting in a possible overestimation of the effect of persistent opium use as a result of such a confounding effect.
Based on the findings of the current study, persistent post-CABG opium consumption, in comparison with no opium consumption and enduring post-CABG opium cessation, was associated with an increased risk of all-cause mortality, MACCEs and ACS. These findings indicate that, contrary to the common concern among cardiac surgeons and cardiologists that stopping opium consumption after CABG might trigger acute cardiovascular events, opium withdrawal is safe and is associated with a decreased risk of mortality, MACCEs and ACS. Cardiologists and cardiac surgeons should be informed about the safety and beneficial effects of opium cessation and encourage their opium-consuming patients to participate in opium withdrawal programmes.
Footnotes
Author contribution
FMK and HRP contributed to the conception or design of the work. MP and AJ contributed to the acquisition, analysis, or interpretation of data for the work. NY drafted the manuscript. FMK critically revised the manuscript. All authors gave final approval and agreed to be accountable for all aspects of the work ensuring integrity and accuracy. All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support of the Research Council of Tehran University of Medical Sciences is kindly appreciated.