
Abstract

Despite a general improvement in the prevention, epidemiology and management of cardiovascular diseases, 1 heart failure (HF) still remains a major healthcare issue, affecting approximately 35 million people worldwide. 2 Because of its increasing prevalence, an unmet need in public health is to find novel strategies capable of slowing disease progression and reducing its high rate of mortality, still about 50% at 5 years. These necessities have led to a great and valuable effort in the HF community, with the implementation in the past decade of an even larger amount of clinical research studies aimed at understanding further pathophysiological models, HF phenotypes and the role of comorbidities, as well as investigating the possible effects of novel treatments.
As result, a huge amount of new evidence has become available in the past few years, with some improvement in the general knowledge of the disease. However, as a downside, this great accessibility of research data from several sources makes HF a field in which physicians have to disentangle themselves, in the difficult attempt to translate research findings into clinical practice. Furthermore, this massive amount of information paradoxically leads to the risk of misinterpreting the results, with an even greater spread of the simplistic view that wrongly considers as valuable only data derived from randomised controlled trials (RCTs), making data from observational studies (OSs) neglected as ‘children of a lesser God’. Testifying to these concerns, a European Society of Cardiology (ESC) work group recently published a statement that pointed out the strengths and weaknesses of both methods, 3 to provide physicians with a possible guide in interpreting research results.
Although RCTs can be considered the most powerful studies in clinical research in providing data on treatment effects, mostly thanks to random sampling (that limits the possibility of differences in study group characteristics, distributing known and unknown confounders between control and active arms), several limitations need to be acknowledged. 4 For instance, because of enrolment criteria, too often some categories of patients are underrepresented (e.g. elderly people, ethnic minorities, advanced disease stages, patients with more comorbidities, and those with a low education level). Furthermore, because of the study design, patients enrolled in clinical trials have the risk of being over-medicated and are invited to attend many follow-up visits, not reflecting real clinical practice; in parallel, RCTs habitually enrol more motivated patients and exclude patients who cannot strictly follow the study design dictates and/or attend to all controls scheduled, introducing an important selection bias difficult to delete. For example, it has been demonstrated that the patient response rate to a RCT screening invitation is generally pretty poor. In addition, RCTs usually do not have sufficient duration to show long-term effects, nor a large enough sample size to identify potential rare adverse drug effects. For these reasons, results from clinical trials need to be confirmed in the ‘real world scenario’ in which findings from RCTs could be occasionally confuted or reduced in importance when tested in a larger population. Finally, there are contexts in which RCTs do not perform well (i.e. in rare diseases).
On the other hand, OSs are able to solve several of these points. Indeed, subjects enrolled in OSs are usually more similar to patients genuinely observed in everyday practice; furthermore, the easier design allows a high participation rate, including categories of patients that are excluded by RCTs. In addition, higher numbers and longer follow-up provide information that is often not obtainable from RCTs. 3 Notably, small OSs can also be useful in investigating, for the first time, novel hypotheses, as proof of concept studies of future more wide investigations. 5
Therefore, there is ‘no need to argue’ that large OSs provide data that are still necessary; indeed, they are more appropriate to describe the natural history of a disease, to suggest novel risk factors and generate new hypotheses. In addition, large OSs can be used to obtain data about the evaluation of drug safety; finally, OSs can be used to get a snapshot of the performance of health systems (e.g. adherence to evidence-based guideline treatment) and to provide possible solutions to implement better health programmes (e.g. telemedicine services).6 However, it is necessary to be careful in claiming that OSs can address all the limitations of RCTs. The truth lies somewhere in the middle, and both instruments are fundamental tools in clinical research, able to provide high quality research data, with different roles in different stages of the research process (Figure 1).
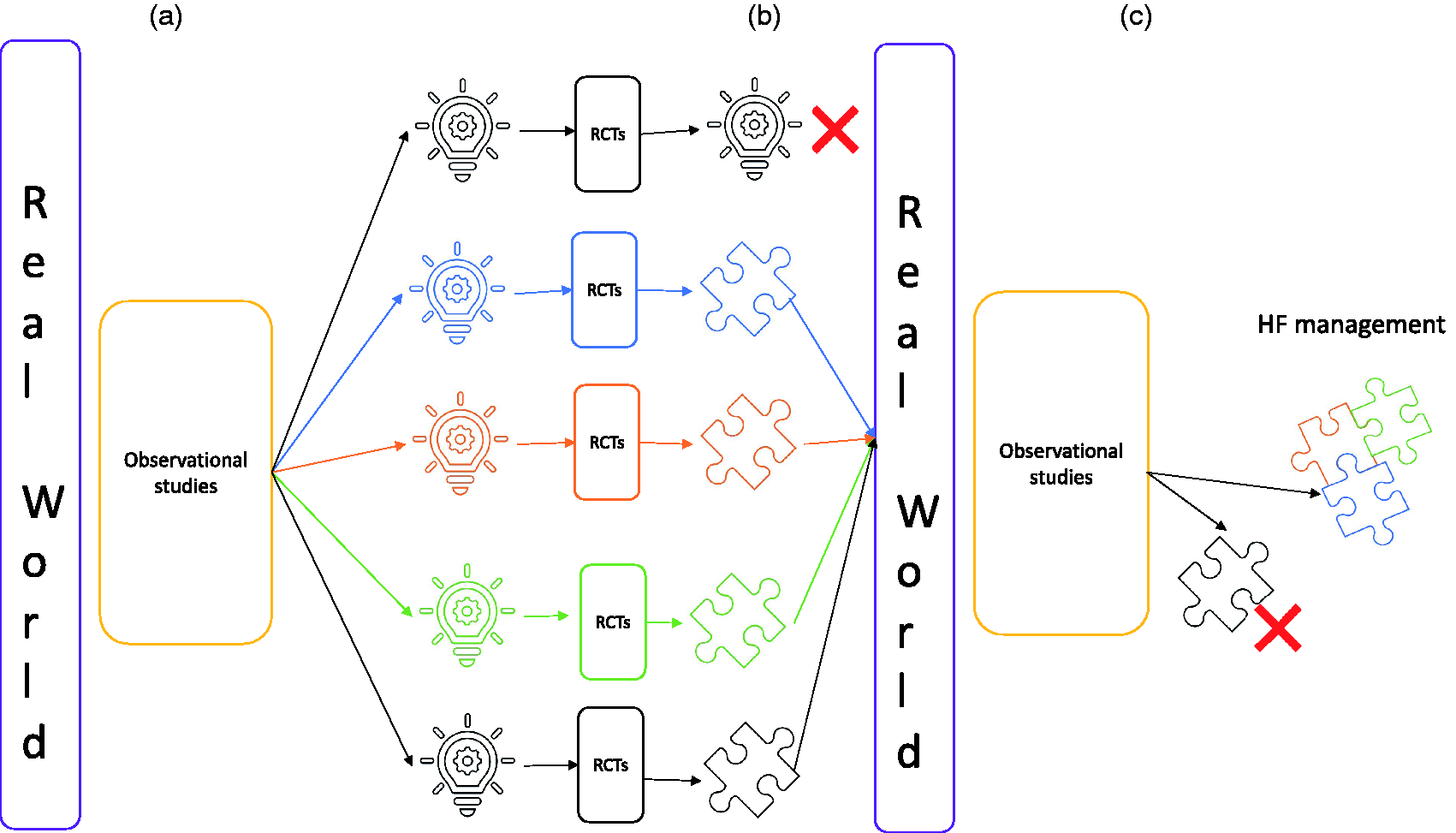
(a) From the real-world experience, observational studies (Oss) allow us to make new hypotheses (light bulb), that need to be tested in randomised control trials (RTCs). (b) RCTs can be confirmative of these hypotheses, providing useful results (puzzle piece), or can reject them. (c) Useful results from RCTs, when applied in the real world, can be validated in large OSs, and enter into clinical practice (puzzle pieces together), or be rejected.
In recent years, there have been several examples of OSs that have provided (or are supposed to provide in the very near future) very useful information in HF, that changed or will change our management of HF. For example, in the context of the ESC Eurobservational Research Programme (EORP), a series of cardiovascular registries launched in 2009, the EORP-HF registry, 7 currently in phase III, will assess contemporary patterns of HF management, prevalence of HF clinical profiles, phenotypes and clusters across Europe. Another successful example is the Swedish Heart Failure Registry (SwedeHF), a nationwide continuous health quality and research registry, founded in 2000 throughout Sweden, that showed for the first time that enrolment in a HF registry improves outcome in HF patients. 8
A further evolution of OSs, recently developed, is the possibility to collect blood samples, building biobanks available for future analyses; this allows to test supplementary hypotheses, often different from the main hypotheses of the principal study aims, further supporting the versatility of OSs. 9 In addition, this possibility allows also to develop multiparametric biomarkers (i.e. based on demographic data, blood and imaging biomarkers). For instance, the BIOSTAT-CHF (BIOlogy Study to TAilored Treatment in Chronic Heart Failure),10,11 a multicentre, multinational, prospective, OS from 11 European countries, aimed at characterising biological pathways related to response/no response to guideline-recommended treatment for HF, has in recent years provided a great amount of data that might have a strong impact on HF management (e.g. showing a sex difference in required doses of HF drugs, with women who might need lower doses when compared to men), 10 with the possibility of further investigating several different aspects, thanks to the availability of a wide biobank. 11 Another interesting example is the DIAMONDHFpEF (Developing Imaging And plasMa biOmarkers iN Describing Heart Failure With Preserved Ejection Fraction), a prospective, observational, cohort study aimed at developing imaging and plasma biomarkers in heart failure with preserved ejection fraction (HFpEF), 12 that is providing useful data to define further the HFpEF phenotype, linking blood biomarkers with imaging. Finally, the TOSCA (TrattamentoOrmonale nello Scompenso CArdiaco; Hormone Therapy in Heart Failure) Registry, a prospective multicentre OS, has been specifically designed to investigate the prognostic impact of hormone deficiencies in HF, 13 with serial blood samples and imaging parameters available over the follow-up, and that is expected to provide the first results in the next few months.
In this context, in the current issue of the European Journal of Preventive Cardiology, Göbel and colleagues presented the rationale, design and baseline characteristics of the MyoVasc, a prospective, observational, cohort study, investigating the development and progression of HF in a cohort of subjects enrolled from the University Medical Centre Mainz, Germany. 14 Preliminary information to bear in mind when reading the present article, is that the MyoVasc investigators, by protocol, used the American College of Cardiology/American Heart Association HF classification (which comprises four progressive and inviolate stages of HF), rather than the ESC classification. As a result, in the MyoVasc study not only subjects with overt HF (HF patients following the ESC guidelines are equivalent to stages C and D of the American guidelines) have been enrolled, but also subjects at high risk of HF but without structural heart disease or HF symptoms (stage A), and subjects with structural heart disease but without HF signs or symptoms of HF (stage B). In total, from January 2013 to April 2018, 3289 subjects have been enrolled. Of these, 1741 were overt HF subjects, with HFpEF as the prevalent phenotype (37.1%), whereas 19.7% were heart failure with reduced ejection fraction (HFrEF) and 23% were HF mid-range (or HFpEF with borderline ejection fraction). In addition, 1253 individuals were not HF patients (considered as stage A/B following the American guidelines).
The particular features of the MyoVasc study are several. Firstly, the presence of stage A/B HF will allow to observe the natural history of the development of HF, from risk factor to overt HF. Notably, the results of the Characteristics and Course of Heart Failure Stages A–B and Determinants of Progression (STAAB) cohort study have recently been published, aimed at identifying the frequency and characteristics of individuals at risk of HF in the general population of a representative sample of residents of Würzburg, Germany. 15 It will be of great interest to compare these results with those of the MyoVasc study, considering the geographical proximity between the two cohorts. Secondly, the presence of all three HF phenotypes will allow to investigate the featuring of HF across ejection fraction. Finally, the biobank, with blood sampling every 2 years for 6 years of follow-up, will provide a valuable resource for future analyses.
In conclusion, in the intricate but even more fascinating scenario of HF, observational data still remain necessary, even in the era of the big trials, in particular if biobanks are collected. The continued interplay between OSs and RCTs is the road map to success in HF research. ‘There’s no need to argue, anymore’*.
*The Cranberries, No need to argue, Island Records – CID 8029, Island Records – 524050-2, Island Records – 524 050-2, release date 4 October 1994.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AS receives research grant support from CardioPath, Department of Advanced Biomedical Sciences, Federico II University, Naples, Italy, and UniNA and Compagnia di San Paolo in the frame of the STAR (Sostegno Teritoriale alla Attività di Ricerca) programme. IBS has received research grant support from Novartis and fees for participation in advisory boards and educational events from Novartis, Astra Zeneca, and Vifor.