
Abstract

Cancer and heart disease have been the most important causes of death in the past 30 years in the developed world. 1 Significant advances in cardiovascular prevention and therapy have led to reductions in cardiovascular disease (CVD) mortality over the past few decades. 2 While cancer mortality was relatively stable throughout most of those decades, recent improvements in the domains of screening, targeted therapy, radiation therapy and cancer surgery are having a favorable impact on outcomes. 3 Cancer survivors are increasing, with an expected 25 million cancer survivors in the United States alone by 2025. 3 Inevitably, many of these cancer survivors will develop CVD. Guidelines for CVD risk assessment and management in cancer survivors, however, are based on sparse evidence which is often extrapolated from non-cancer patients and seldom derived from high quality longitudinal data. 4 Herein lies an opportunity to apply more stringent prospective approaches to the growing problem of CVD in cancer survivors, and to bring stakeholders together to educate patients and providers.
In this edition of the European Journal of Preventive Cardiology, Caro-Codón et al. present data on 1324 patients 5 in the CARDIOTOX registry who were followed in a cardio-oncology clinic at La Paz University Hospital in Spain. The study consisted predominantly of women (80.5%) with breast cancer (60.4%). As expected, 67.4% of patients had at least one cardiovascular risk factor, the most common of which was hypercholesterolemia (48.3%). None of the individual CVD risk factors were directly associated with mortality, which is also not surprising given the limited duration of follow-up. However, the European Association of Preventive Cardiology SCORE, 6 which is derived from the combination of age, gender, systolic blood pressure and smoking status, was found to be associated with severe cardiotoxicity and all-cause mortality. Severe cardiotoxicity was defined as left ventricular ejection fraction reduction below 40% in an asymptomatic patient, clinical, symptomatic heart failure with any ejection fraction or cardiovascular death. 7 This finding is particularly timely given the newest version of the National Comprehensive Cancer Network (NCCN) survivorship guidelines, 8 which encourages aggressive risk factor reduction despite the lack of longitudinal evidence. Interestingly, in the current study, risk factor control tended to worsen during cancer therapy despite the fact that patients were being managed in a dedicated cardio-oncology clinic, which illustrates the challenge of implementing risk reduction strategies while patients and their caregivers are focused primarily on cancer treatment.
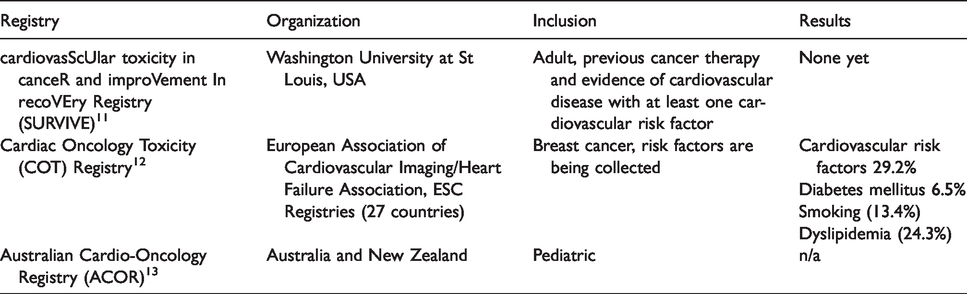
The findings of this study reinforce the idea of systematically performing prospective cohort studies, akin to the Malmo Heart Study 9 or the Framingham Heart Study, 10 specifically in cancer patients in order to identify shared risk factors for CVD and to define their interactions. Registries dedicated to studying these risk factors are currently enrolling in several centers around the world as noted in Table 1.11–13 The information obtained from these ongoing studies may provide additional support for the use of CVD-specific risk estimation tools in patients undergoing cancer therapy.
Ongoing cardio-oncology registries with similar scope as the CARDIOTOX registry.
As we advance the field of cardio-oncology, it will be crucial to develop a foundation of science that is truly based on cardio-oncology rather than either cardiology or oncology. This is highlighted in the joint statement of the International Cardio-Oncology Society (ICOS), which identified 10 pressing areas of research and development in the field. 14 In particular, pertaining to the prevention of CVD in cancer patients, the approach should be multi-pronged. Societies like the European Society of Cardiology (ESC), the American Heart Association (AHA), the American College of Cardiology (ACC), the American Society of Hematology (ASH), the American Society of Clinical Oncology (ASCO), the European Society for Medical Oncology (ESMO), ICOS, etc. should work with their local chapters to promote the education of shared risk factors among providers and patients. These organizations should also promote exercise as a cardiotoxicity mitigating tool in those undergoing chemotherapy. 15 , 16 In addition, providing resources to assist healthcare entities in building infrastructure to standardize the documentation of risk factors, in cancer survivors and in those undergoing treatment, is also important for these organizations. At the national level, these agencies should join forces with federal agencies to collect data specific to cancer patients in focused registries. Emphasis should initially be placed on the top three to five cancers which affect the greatest number of patients so that the maximum benefit can be accrued from the data that are collected. The registries can be structured like the PINNACLE registry 17 to collect granular CVD data, which can then be merged with state level cancer registries 18 to capture granular cancer-specific data. Other efforts at the national level should be focused on advocacy for furthering the policies to curb shared risk factors such as smoking, obesity, etc. In addition, professional societies should direct resources towards research that seeks to understand the mechanistic underpinnings whereby specific risk factors contribute to the development of CVD in cancer patients, thus enabling precision approaches in preventive cardio-oncology.
In conclusion, the study by Caro-Codón et al. illustrates the opportunity to improve outcomes in cancer patients by employing targeted strategies to assess cardiovascular risk. 5 At the same time, it reminds us of the challenge of implementing cardiovascular risk reduction approaches in patients undergoing cancer therapy. Through the joint efforts of the various stakeholders, we can develop the infrastructure, collaborations and research programmes required to make an informed impact on the lives of cancer survivors in order to reduce the burden of CVD.
Footnotes
Author contribution
AG drafted the manuscript. All authors provided critical revisions of the manuscript for important intellectual content.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NLW is supported by NIH grants HL124097, HL126949, HL134354, AR070029 and AG064895.