
Abstract
Background
Statins are the most widely prescribed drugs for dyslipidemia and CAD. But evidence on their cognitive effects is conflicting. A unique genetic makeup and variable lipid patterns make South Asians more susceptible to statin adverse effects. But literature on statin safety in this group is scarce. We aimed to assess the cognitive status of adult Indian statin users over two years and explore factors associated with it.
Methods
A prospective cohort was established for cognitive profiling of adult statin users, visiting the out-patient cardiology department of a tertiary care center in North India. The Montreal Cognitive Assessment Scale measured cognitive function. Analysis was conducted using mixed-effects linear regression modelling to account for repeated measurements.
Results
273 participants were enrolled. The mean cognitive score was 15. Age and education were significant predictors of cognition (P-value .005 and <.001 respectively). Participants over 60 scored had significantly lower scores and those who had completed secondary school and above scored significantly higher scores. No significant associations were observed between cognitive score and other covariates- sex, follow-up period, statin type and duration of use.
Conclusion
The statins-cognition relationship is controversial. This study demonstrated statistically significant relationships of cognition with age and education and showed no change in cognition over 2 years. The findings provide hypotheses for more in-depth assessments. Statins remain the most effective lipid-lowering treatment. However, further research is warranted for a more holistic understanding of the issue & optimizing their risk-benefit ratio.
Introduction
Cardiovascular diseases (CVDs) are the leading cause of global mortality and morbidity, with a disproportionately high burden and highest mortality rates in the low-and middle-income countries (LMICs). 1 In India, the CVD burden is escalating at an alarming rate, with ischemic heart disease and stroke contributing to almost 28% of the overall national mortality. 2 CAD presents at least a decade earlier in Indians than their western counterparts, with 50% of mortality and 25% of cardiac events occurring below 50 and 40 years respectively. 2 CAD is a consequence of atherosclerosis, making dyslipidemia a major predictors of CVDs, alone and combined with hypertension, diabetes, smoking, alcoholism, and physical inactivity. 3
Statins, or Hydroxy Methyl Glutaryl-Co Enzyme A (HMG-CoA) reductase inhibitors are highly effective and the most widely prescribed class of cholesterol-lowering drugs used in primary and secondary prevention of CAD. They can reduce death and morbidity by about 30% and the risk of cardiac events by almost 60% through a reduction in low density lipoprotein (LDL-C) levels. 4 Although their therapeutic benefit is large, they have been associated with adverse effects like myalgia, liver damage, nerve problems and cognitive issues.5–8 The relationship between statins and cognition has been a subject of debate for more than a decade. In 2012, the U.S. Food and Drug Administration (FDA) mandated the addition of warnings for possible memory loss to all statin drug labels. 9 While some studies have reported cognitive decline, 10 others have shown a protective effect of statins, 11 and a few others have reported no association. 12 The overall evidence is thus quite conflicting.
Dyslipidemia in South Asians is atherogenic, which, when combined with the variable pharmacokinetics of statins, increases their genetic predisposition to CVDs and their risk of statin adverse effects.13–15 Literature on statin safety in this population is inadequate, since vast majority of clinical trials are either conducted in the west or with minimal representation of ethnic minorities. Moreover, evidence on statin related cognitive effects in Asian populations is scarce, making it imperative to explore this relationship in an LMIC setting.11,16 We conducted a longitudinal cohort study to observe changes in the neuro-cognitive profile of statin users over a period of two years, and explored factors associated with the same. Additionally, we assessed out-of-pocket (OOP) costs associated with CAD treatment.
Methods
Study design and study setting
This study followed a prospective cohort design wherein eligible and consenting individuals were recruited from the Cardiology Out-Patient Department (OPD) of the Safdarjung Hospital in New Delhi, India, one of the largest tertiary care referral centers of North India with an annual OPD attendance of more than 1 million patients from all over the country.
Study participants
Patients aged 18 and above, visiting the Cardiology OPD and prescribed statins in the last 1.5 year prior to recruitment, were eligible for inclusion. New users were recruited to minimize pre-existing cognitive alterations. Patients on statins for more than 1.5 years, those with a history of psychiatric disorders, neuro-cognitive illnesses (Dementia, Alzheimer's Parkinson's Multiple Sclerosis), those on neurological or psychiatric medication (anti-psychotics, anti-epileptics, neuro-stimulants, steroids, anti-depressants) and those with severe illness like acute myocardial infarction, unstable CAD, stroke, advanced heart failure and HIV were excluded.
Study duration and recruitment process
The study duration was 3 years, with a 4 month recruitment period, 2 year longitudinal period of observing participants and collecting data, followed by data compilation and analysis. Participants visiting the OPD for routine check-ups were assessed for eligibility. Those that provided voluntary consent were enrolled in the study. Their names and contact details were collected, along with their current prescription, at the time of recruitment, following which they were contacted remotely for collection of study data & assessment of cognitive status.
Sample size and sampling
This study profiled the neuro-cognitive status of statin users in an LMIC. Appropriate prior estimates for calculating a sample size were not available from the western literature. Hence, a formal power calculation was not undertaken. Based on the insights from the preliminary research conducted by the team on the prevalence of statin-associated adverse effects,5,7 the experience of the collaborating cardiologist and the daily OPD footfall, a sample size of 300 was arrived at, based on feasibility. All consecutive patients visiting the OPD were screened for eligibility using convenience sampling.
Study tools
Quantitative data were collected via interviewer-administered questionnaires using the WHO-STEPS tool to assess demographics, lifestyle, disease status, family history, medications, symptoms, and healthcare costs. 17 Cognitive status was measured using the universally used and validated Montreal Cognitive Assessment (MoCA) scale, 18 the Hindi version of which has been validated in Indian settings. 19 MoCA assesses seven cognitive domains- visuospatial/executive, naming, memory, attention, language, abstraction, delayed recall and orientation. 18 To comply with pandemic social distancing, the primary investigator (RM) collaborated with MoCA developers to create telephonic Hindi versions (MoCA Blind and MoCA Basic Blind) for literate and illiterate participants. They are similar to in-person MoCA, with visual components removed and are available for use on the official MoCA website. 20
Study variables
Age was measured as a continuous variable. Moderate and vigorous physical activity definitions were based on the World Health Organization (WHO) guidelines. 21 Disease history and adverse effects were self-reported. Details of the statin prescribed (name, dosage, duration) were obtained from the patient prescriptions. Cognitive domains were measured using MoCA and each participant was scored out of 22 points. 20
Data collection and management
Participants were recruited in-person, while data collection was conducted at three time points: baseline, end of year 1 and end of year 2. Anthropometric and physiological measurements were taken during recruitment at the OPD by trained staff, and biochemical tests were performed at the hospital's accredited laboratory, with reports shared by participants via WhatsApp. The primary investigator received formal MoCA certification, and tools were pre-tested on 10 subjects. Data entry was done using a validated CsPro database.
Statistical analysis
Descriptive statistics were used to summarize population characteristics, as means/standard deviations, medians/IQRs or frequencies/percentages, as appropriate. Each participant was scored between 0–22 on the MoCA scale. The cognitive status at each measurement was reported as an overall mean score. Two sample t-tests and ANOVA were used for a statistical comparison of the baseline mean scores by categories of age, gender, education, statin type, dosage and duration. A P-value for trend was obtained when the difference in the mean scores was significant. A logistic regression was carried out to ascertain the pattern of missingness in the data and ascertain if it was associated with any key covariates in the study. Additionally the Missing Completely At Random (MCAR) test was run to check if observations were missing completely at random or were dependent on observed or unobserved data. Multiple Imputation (MI) using the Multiple Imputations by Chained Equations (MICE) approach was undertaken to impute missing values for the primary outcome variable- the cognitive score, as well as the statin usage period. To assess the association between cognitive status and various predictors over two years, a mixed-effects linear regression model, commonly used for analysis of longitudinal data, was implemented on the complete case dataset as the primary analysis, and on the imputed dataset as an exploratory analysis. Age, gender, education, statin use period, statin name and follow-up period were incorporated as fixed predictors in the model. A random intercept was added for the participant ID and a random slope for the follow-up time variable. The models were checked for linearity, normality and homoscedasticity for residuals, normality of random effects, before running the regression. Stata version 15.1 was used for analysis.
Results
A total of 324 eligible and consenting participants were recruited and the final eligible sample was 273. There were a few drop-outs during the baseline assessment, and complete baseline data was obtained from 244 participants. Similarly, there were drop-outs at each follow-up with the final numbers for the first and second follow-up being 192 and 185 respectively. The participant flow from the recruitment stage till the final follow-up, along with reasons for loss to follow-up is diagrammatically presented. (Figure 1)
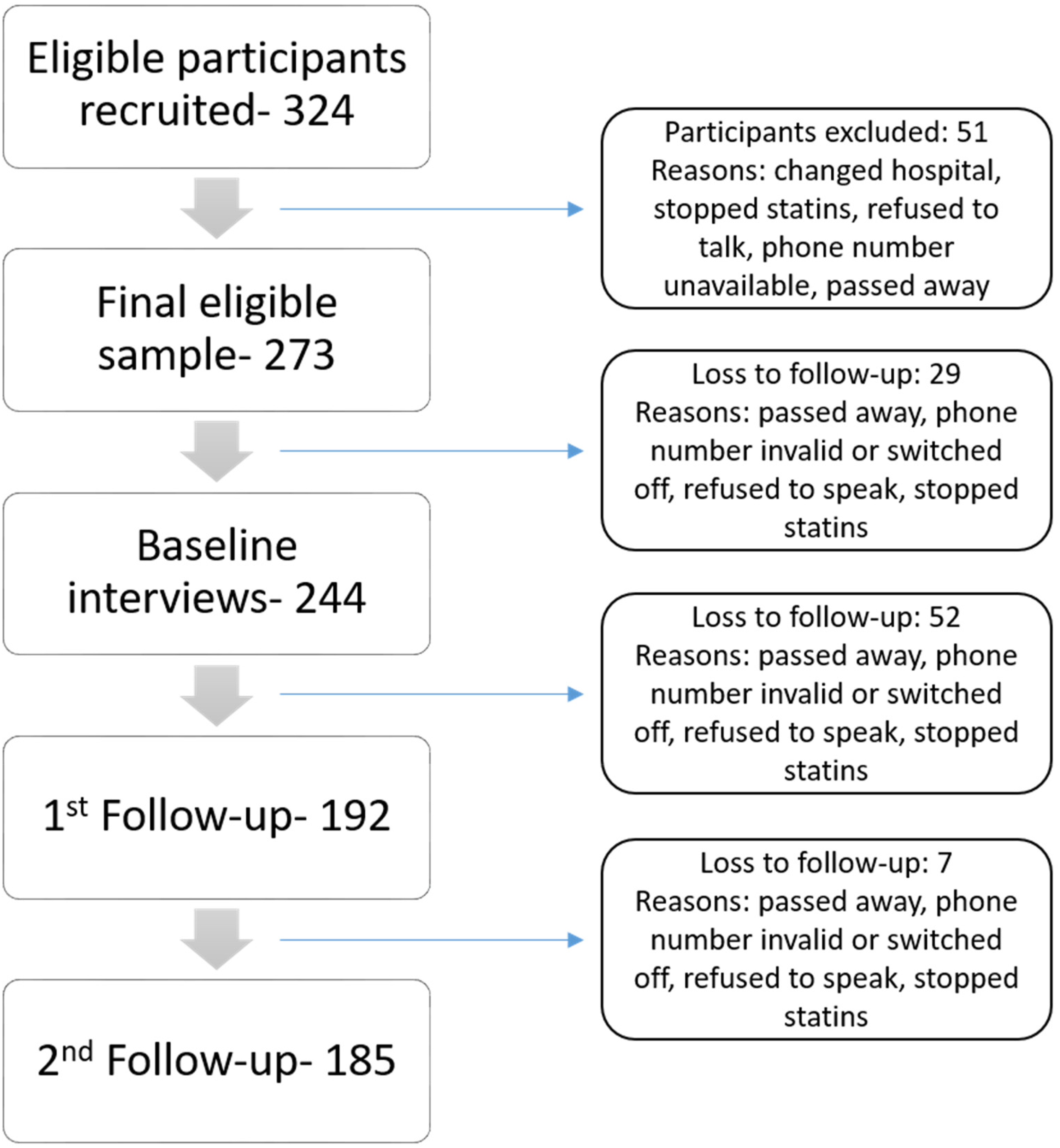
Flow of participants throughout the study and reasons for loss to follow-up.
The mean age of the participants was 52.5 years, with over 50% aged 50 and above; 64% were male. More than 50% had completed primary school or lesser, and only 25% had completed high school. Less than 40% were employed, with a median monthly household income of INR 15000 (USD 175), and over 70% earning below INR 20000 (USD 233). (Table 1)
Baseline socio-demographic profile of the study population

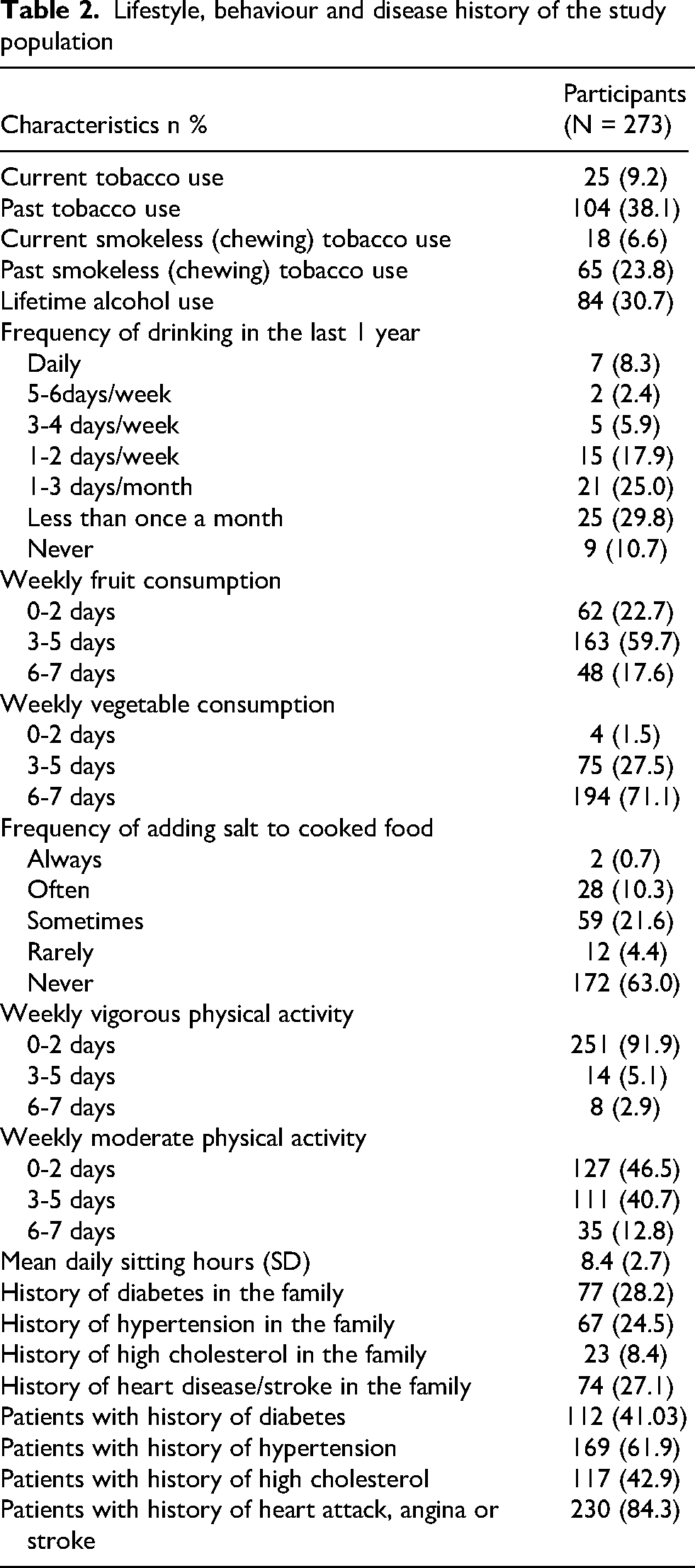
Tobacco and alcohol use were reported by 16% and 30% of participants, respectively. Only 5% engaged in regular vigorous physical activity, while 40% engaged in moderate activity, and average daily sitting time was 8 h. About 25–30% had a family history of diabetes, hypertension, heart disease, or stroke, while 8% reported a family history high cholesterol. Self-reported chronic illnesses included diabetes (40%), dyslipidemia (43%), hypertension (62%), and a history of heart attack, angina, or stroke (85%). (Table 2)
Lifestyle, behaviour and disease history of the study population
The majority of participants were on atorvastatin (88.3%), with most receiving 20–40 mg doses, while over 50% of rosuvastatin users were prescribed 40 mg. About 60% had started statins within six months of recruitment. Commonly reported adverse effects included muscle-related ailments (21%) and nerve-related symptoms (20%). Around 19% missed at least one dose in the past month, and 11% had discontinued statins at some point, citing reasons like the COVID-19 lockdown, feeling better, financial constraints, and forgetfulness. (Table 3)
Statin use, adverse effects and treatment adherence among the study population

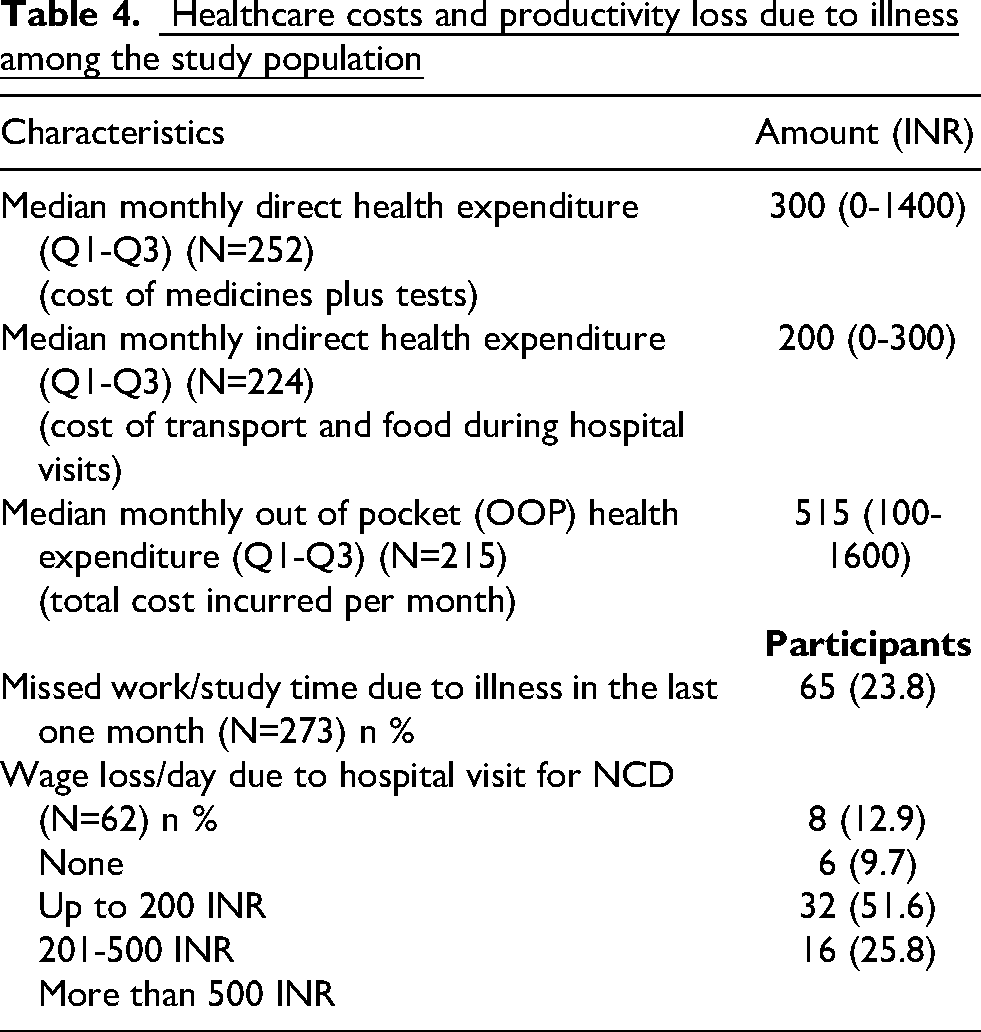
The median direct and indirect costs of treatment per month were INR 300 (USD 3.5) and INR 200 (USD 2.3) respectively. The median monthly OOP health expenditure was INR 515 (USD 6), with 20% of the population spending more than 10% of their household income on their CAD treatment monthly. Thus, at least one-fifth of the participants met the WHO's threshold for catastrophic OOP health spending. 22 About 24% reported a loss of productive work hours, with about 26% of those losing more than INR 500 (USD 5.8) in daily wages. (Table 4).
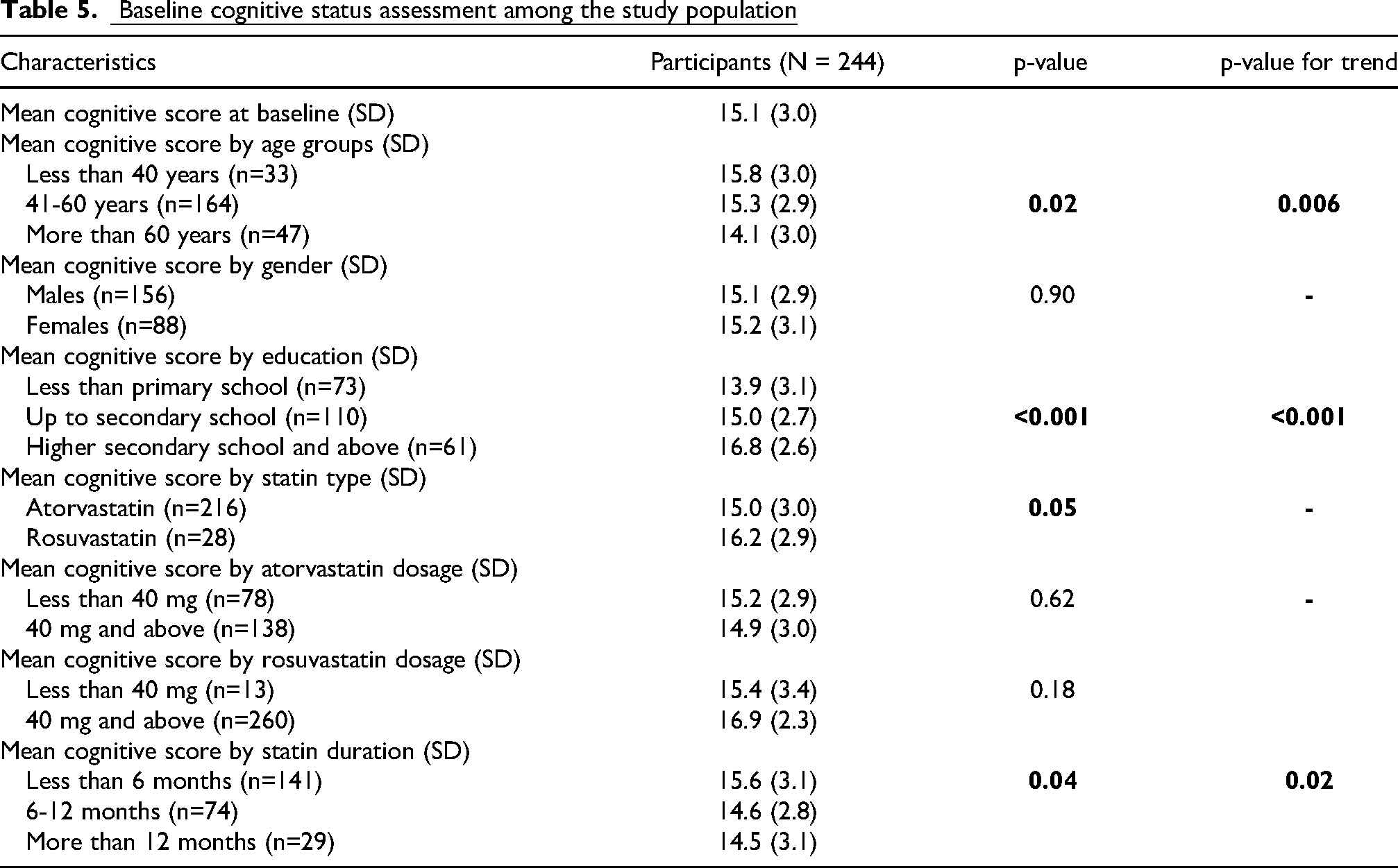
The mean cognitive score of the participants at baseline was 15.1 points (out of 22) (Table 5). The mean score decreased with higher age and longer duration of statin use. This downward trend was statistically significant across categories. Similarly, the mean score was higher in the higher education category, and this upward trend was also statistically significant. The mean score at baseline was also significantly lower among atorvastatin users as compared to rosuvastatin users. The score was not different across categories of gender or statin dosage.
The score was almost unchanged across the three time points, with a mean of about 15 and a standard deviation of 3 units. All 3 scores had a normal distribution (Table 6).

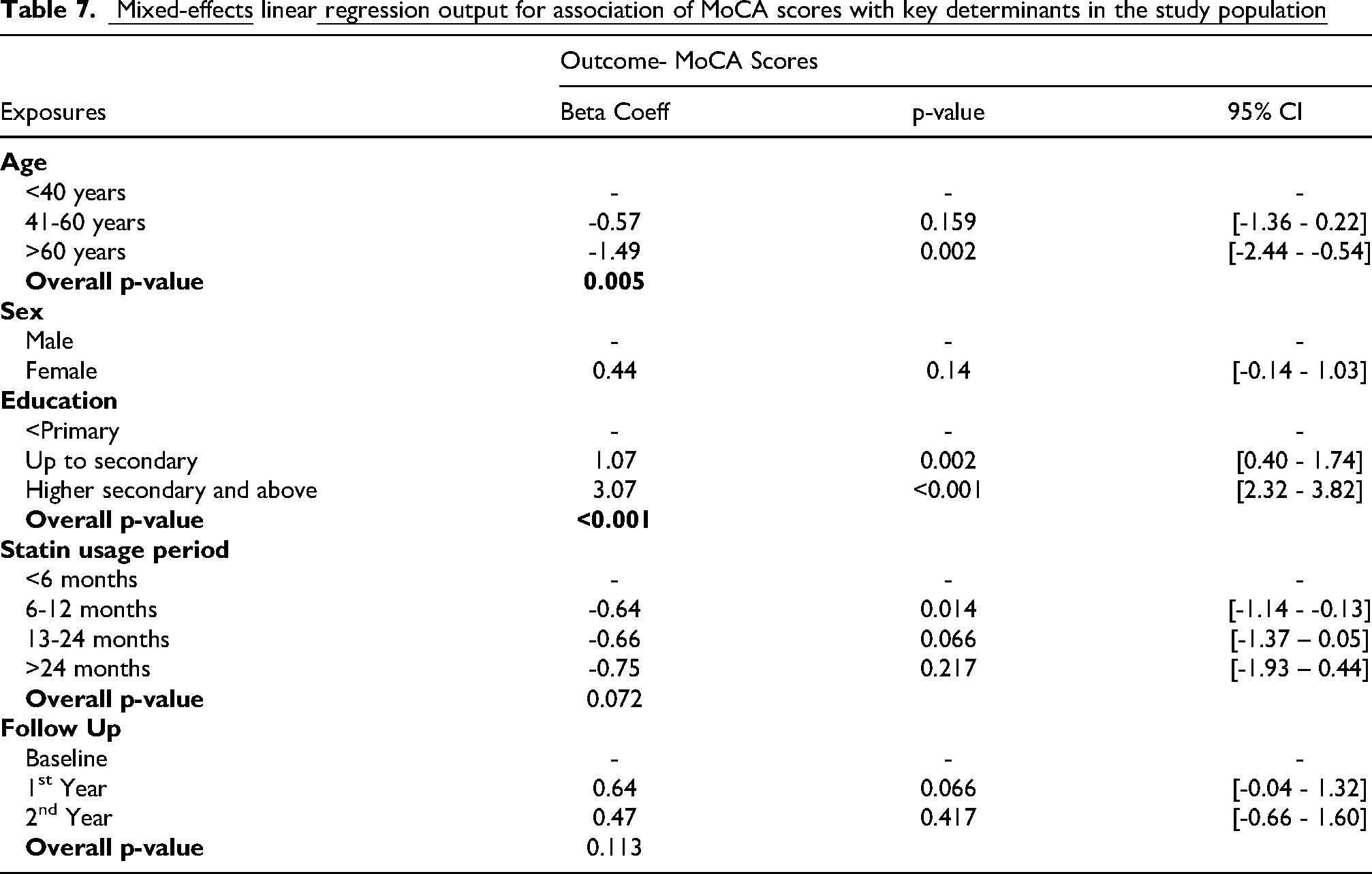
A mixed effects linear regression model was run to study the association of age, gender, education, statin use duration and follow-up period with the MoCA score over time. Age and education were found to be significantly associated with MoCA scores over time (P-value .005 and <.001 respectively). Participants aged 60 and above scored 1.5 units lower on the MoCA, compared to the youngest group (younger than 40 years). Also, those who had completed secondary school scored 1.07 units higher on the MoCA and those who had completed higher secondary school scored 3.07 units higher on the MoCA, compared to the base category of participants with less than primary school education. The association between statin use duration and cognitive scores was not significant in the adjusted analyses. Sex and follow-up time were not associated with MoCA scores in either crude or adjusted models (P-values .14 and .113, respectively) (Table 7).
For the imputation analyses, 20 imputed datasets were generated, a mixed-effects regression was performed on each dataset, and a pooled estimate was calculated. The findings from the imputation analysis were consistent with the complete case analysis (Supplementary File 1).
Discussion
Principal findings
This study profiled the cognitive status of statin users at a tertiary hospital in New Delhi over a 2 year period, through a prospective cohort design. Most research on statin-related effects is from the west, and focused on muscle ailments, making this a first of its kind Indian study.
Most participants were males aged 50 and above, had low literacy levels and were from the lower socio-economic strata. CAD treatment incurred high OOP costs relative to income. A majority had started statins (mostly Atorvastatin) six months prior to study start. The onset of statin induced adverse effects cannot be accurately predicted, but evidence suggests that symptoms usually start to appear within a year of use. 23 The mean cognitive score was 15 and did not change significantly over 2 years. Age and education remained significant predictors of the score over time in the adjusted analyses and no significant associations were seen between the score and sex, statin type, statin use duration and follow-up period.
Strengths and weaknesses
To the best of our knowledge, this is the first longitudinal study from our country assessing the neuro-cognitive profile of cardiac patients on statins, addressing the need for research on the effects of statins beyond cholesterol-lowering. This is also among the very few South-Asian studies on statins and cognition. The hospital's diverse patient base allowed findings to be generalized. Participants were new statin users, minimizing pre-existing cognitive decline. MoCA, a validated tool, ensured reliable MCI screening. The loss to follow-up from baseline to endline was about 24%, which is inevitable in longitudinal studies. The sensitivity analysis showed no socio-demographic differences between respondents and non-respondents.
This study has its limitations, as findings cannot be used for statistical inferences, though internal validity was maintained to inform future research. The telephonic administration of the tool excluded visual components, and remote data collection poses its own challenges, especially in resource-limited settings. 24 However, this approach was necessary to prevent in-person transmission during the pandemic. Additionally, we could not collect family history of dementia/MCI, since awareness levels regarding neurological conditions is low, especially in populations with lower education levels, which makes eliciting such information a challenge. Lastly, the study did not include a formal neurological test battery, as its focus was on cognitive status and complete medical diagnosis was beyond the study scope.
Comparison of findings with existing literature
A majority of participants had a low MoCA score, indicative of cognitive dysfunction. Currently, the telephonic versions of MoCA do not have a definitive MCI cut-off. However, a suggestive cutoff of 18 is used to differentiate the cognitively impaired from the normal. 25 According to this threshold, more than two-thirds of our population demonstrated MCI. This is higher than previously reported Indian estimates. A study among elderly Indian patients (mean age 70, 70% below primary education) reported a 32% prevalence of cognitive dysfunction, measured using the Mini-Mental State Examination (MMSE). 26 However, the reason for a much lower prevalence in this study could be the use of MMSE, which is has low sensitivity, considerable ceiling effects and is unsuitable in illiterate populations. 27 Another study among Indian type-2 diabetes patients (mean age 58, median years of education 10) reported a 54% prevalence of MCI in the age group of 40–60 years, measured using the MoCA. 28 This population had higher education levels than ours, which could indicate a lower MCI prevalence. Prevalence rates have varied considerably from 10–15% to 45–60%, across multiple Indian studies in different age and education groups, due to heterogeneity in diagnostic criteria and methods, and presence of comorbidities. 29 India has about 5.3 million dementia patients which accounts for more than 75% of the entire population of South Asians with dementia. Literature on the prevalence of MCI and dementia in Asian populations is limited. 30 It is also important to interpret the MCI prevalence in this study within the broader context of the pandemic (especially its second wave), during which the baseline assessment was conducted. COVID-19 introduced a wide range of psychological, social and financial stressors that may have transiently affected the cognitive functioning in this population. The association of COVID-19 related psychological distress on cognitive performance and memory deficits, especially in older adults with co-morbidities, has been well documented.31–34 Also, as mentioned in the limitations, remote testing, though viable, comes with its own shortcomings, and may have led to underperformance in certain cognitive domains. 35
The relationship of age and education with cognition in our study was consistent with existing literature. Age and education levels have been proven to be strong predictors for cognitive function, with higher cognition levels in younger and more educated individuals.28,36,37
The difference in scores between Atorvastatin users and Rosuvastatin users at baseline could be attributed to statin lipophilicity. 38 Limited studies have shown that lipophilic statins like Atorvastatin may be associated with higher risk of cognitive impairment in cognitively normal subjects, and elevate the risk of converting to dementia in cognitively impaired subjects.39,40 Lipophilic statins can cross the blood-brain-barrier, unlike hydrophilic statins like Rosuvastatin, which require a carrier protein for the same. However, there's contradictory evidence of a lower risk of cognitive decline as a protective effect of lipophilic statins, further complicating the dynamics.16,41,42
Our study found an inverse relationship between participant cognitive score and statin use duration in the preliminary baseline analysis. But this association was also not significant in the adjusted regression model. The existing evidence in this regard is negligible, with some studies suggesting that long-term use of statins might be correlated with increased risk of adverse effects. 43 However, this is disputable and needs more conclusive evidence.
No association was seen between the cognitive score and time. Literature on the relationship between statin use and cognition is contradictory. Various randomized controlled trials (RCTs) and prospective studies have reported no change in cognitive status,44–50 some have reported a protective effect,51,52 & some have reported a detrimental effect.53–55 Systematic reviews and meta-analyses have also reported conflicting results, ranging from no benefit of statins on cognition,12,56–58 to lower risk of cognitive impairment with statin use,16,59–62 to somewhat higher risk of cognitive decline among statin users.63–65
Implications of the study findings
The relationship between statin use and neuro-cognitive effects continues to be a contentious topic of scientific debate. Studies have put forth opposing mechanisms for both improvement and deterioration in cognition following statin use.41,42 It is still unclear whether statins impair or improve cognition, or if no such relationship exists. A majority of primary studies as well as reviews have highlighted a few key reasons for inconsistencies in the current data, such as smaller sample sizes, inadequate follow-up periods, heterogeneity in study designs, populations, cognitive measurement techniques, type of statin, duration of statin therapy, adherence to treatment, apolipoprotein genotype differences, presence of comorbidities, as well as differences in diagnostic criteria for dementia. Issues like confounding and biases in observational studies could also affect study estimates. Moreover, cognition has mostly been assessed as a secondary or tertiary outcome in RCTs, hence the studies were not adequately powered to detect cognitive change outcomes and they were only exploratory. The relationship could also be mediated by Vitamin B12, homocysteine and Vitamin D levels, or genetics.66,67 Thus, a lack of consensus across current literature could be attributed to these shortcomings which warrant attention while designing future research studies. Thus, our study need to be further substantiated, and the current results warrant cautious interpretation.
It is also noteworthy that most literature on statins and cognition is from western, mostly Caucasian populations. Evidence on the statin-cognition relationship from LMICs is limited to a handful of studies5,68–70 highlighting the immense scope for research in our population.
Conclusion and need for further research
Statins are widely prescribed for cholesterol lowering, but their neuro-cognitive effects remain controversial due to conflicting and limited evidence. This study profiled cognitive function in adult statin users, explored key trends, and assessed longitudinal relationships of some key determinants with cognition, providing internally valid findings to generate future research hypotheses. Larger prospective studies and trials with standardized cognitive assessments and greater homogeneity in designs and methods are needed for more in-depth insights. Given the high global burden of both cardiovascular and cognitive disorders, further research is pivotal, especially in resource limited settings, for a more effective clinical and public health response.
Supplemental Material
sj-docx-1-cvd-10.1177_20480040251371770 - Supplemental material for Neuro-cognitive profile of adult statin users at a large tertiary care hospital in Delhi, India
Supplemental material, sj-docx-1-cvd-10.1177_20480040251371770 for Neuro-cognitive profile of adult statin users at a large tertiary care hospital in Delhi, India by Rubina Mulchandani, Ashish Kumar Kakkar, Sheetal Gandotra, HS Isser, Rajinder K Dhamija and Tanica Lyngdoh in JRSM Cardiovascular Disease
Footnotes
Acknowledgements
We are grateful to the study participants and the staff at Safdarjung Hospital for their time and support in conducting this study. We acknowledge the support provided by the Council of Scientific and Industrial Research in the form of a Senior Research Fellowship granted to RM (Apr 2021-Mar 2024).
Ethical approval
The Institutional Ethics Committees at both the institutes: IIPH-D, PHFI (File No: IIPHD_IEC_S_01_2020) and Safdarjung Hospital (File No: IEC/VMMC/SJH/Project/2020-06/CC) approved the protocol before study initiation. The research was conducted in accordance with the Declaration of Helsinki. Confidentiality of the patients was maintained throughout and patient identifiers were delinked from the final data. Any health related information requiring attention was flagged to the consulting physician.
Consent to participate
Each participant was provided with a Patient Information Sheet (PIS) in English and vernacular language – Hindi, for a simple yet detailed explanation of the study. Their participation was voluntary and independent of their therapeutic care. Consenting participants signed an informed consent form.
Author contributions
Rubina Mulchandani: conceptualization, data curation, formal analysis, methodology, software, supervision, validation, visualization, writing – original draft, writing – review and editing; Ashish Kumar Kakkar: conceptualization, methodology, supervision, writing – review and editing; Sheetal Gandotra: conceptualization, supervision, writing – review and editing; H.S. Isser: supervision, writing – review and editing, R.K. Dhamija: supervision, writing – review and editing; Tanica Lyngdoh: conceptualization, methodology, supervision, writing – original draft, writing – review and editing
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data for the study are not publicly available and can be obtained from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.