
Abstract
Background
Timely fibrinolysis remains the cornerstone of reperfusion for ST-elevation myocardial infarction (STEMI) in settings without reliable access to primary percutaneous coronary intervention (PCI). International guidelines recommend a door-to-needle time (DTNT) of 30 min or less.
Aim
We conducted the first continent-wide meta-analysis to quantify real-world DTNTs and adherence to guideline benchmarks in African hospitals.
Methods
We systematically searched PubMed/MEDLINE, Scopus, and Web of Science through July 2, 2025, for studies reporting DTNT for adult STEMI patients treated with thrombolysis in Africa. Pooled mean DTNT was estimated via random-effects meta-analysis with restricted maximum likelihood and Knapp–Hartung adjustment. Heterogeneity was assessed by Cochran's Q and I2, and sensitivity analyses evaluated robustness.
Results
Across 12 eligible studies encompassing a total of 2193 STEMI patients, about 1261 individuals (57.5%) received thrombolytic therapy. Among the 11 studies reporting mean reperfusion times (1011 patients), the overall pooled mean DTNT was 74.8 min (95% confidence interval: 44.4–105.2; I2 = 99.4%), substantially exceeding the recommended benchmark. Notably, only 36.3% of thrombolyzed patients achieved a DTNT of ≤30 min. Furthermore, none of the included study cohorts reported an overall mean DTNT within 30 min.
Conclusion
African STEMI patients experience door-to-needle delays more than twice the guideline target, with fewer than 4 in 10 receiving timely fibrinolysis. In such settings lacking widespread PCI, implementation of standardized reperfusion protocols, optimized in-hospital workflows, and targeted quality-improvement initiatives is urgently needed to accelerate fibrinolysis, maximize myocardial salvage, and reduce adverse cardiovascular outcomes.
Introduction
Ischemic heart disease now ranks among the fastest-growing causes of death in sub-Saharan Africa (SSA), where acute coronary syndromes (ACS) accounts for a growing number of all hospitalized cardiovascular cases and continue to rise as populations age and risk factors proliferate.1,2 Despite this growing burden, access to primary percutaneous coronary intervention (PCI), the gold-standard reperfusion strategy for ST-elevation myocardial infarction (STEMI), remains severely constrained. In South Africa, for example, there is one PCI facility for every 887,096 people, most of which are clustered in private, urban hospitals; smaller and rural facilities often lack catheterization laboratories entirely. 3 In Nigeria, there are only about 12 operational PCI-capable centers nationwide, amounting to one PCI facility per 16.8 million people. 4 These stark deficits in infrastructure are even more pronounced elsewhere in SSA.
When primary PCI is unavailable or delayed, fibrinolytic therapy is the cornerstone of reperfusion. Along these lines, international guidelines explicitly recommend administration of fibrinolytics within 30 min of hospital arrival in non-PCI-capable settings—the “door-to-needle” time (DTNT) target—because every minute of delay in STEMI care translates into lost myocardium and higher mortality. 5 Indeed, the GRACE registry data demonstrated that each 10-min delay in DTNT between 30 and 60 min is associated with a 0.3 percentage-point increase in 6-month mortality. 6
Despite this well-established importance of rapid fibrinolysis, and its particular value in low-resource settings, no prior study has synthesized DTNT performance across the African continent. To address this gap, we conducted the first continent-wide meta-analysis of STEMI care in Africa addressing the subject. By highlighting the timeliness of pharmacologic reperfusion in such settings, we aimed to quantify real-world DTNTs, assess adherence to guideline benchmarks, and identify any critical system-level barriers that may be an essential foundation for targeted interventions designed to improve survival and reduce major adverse cardiovascular events.
Materials and methods
This review was registered on PROSPERO (CRD420251116485) and follows PRISMA 2020 guidelines. Together with a clinical librarian, we developed a comprehensive search strategy using MeSH and free-text terms for “door-to-needle time,” “thrombolysis,” and “ST-elevation myocardial infarction.” PubMed/MEDLINE, Scopus, and Web of Science were searched from inception to July 2, 2025, without language or publication-status restrictions (full search syntax is given in Supplemental Figures 1 to 3). All records were de-duplicated in Zotero v7.0.18, and reference lists of the included studies were hand-searched for additional reports.
We included observational studies of adult STEMI patients treated with any kind of intravenous fibrinolysis in African hospitals that reported DTNTs as mean ± SD or median with interquartile range (IQR)/range. We excluded case reports, reviews, conference abstracts without full text, and any study lacking sufficient summary data to compute mean ± SD or median with spread.
Two reviewers independently screened titles, abstracts, and full texts; disagreements were resolved by consensus or third-party adjudication. Data were extracted into a standardized form capturing author, year, country, design, sample size, patient demographics, and DTNT metrics. Study quality and risk of bias were assessed using the STROBE checklist and Newcastle–Ottawa Scale, with inter-rater agreement quantified by Cohen's κ.
To include studies reporting medians, we converted medians and IQRs to means and SDs using Luo et al.'s 7 method for sample means and Wan et al.'s 8 formulas for SD estimation. For studies reporting only minimum and maximum values, we applied Wan et al.'s range-based estimators. 8 All DTNTs were then meta-analyzed as means ± SD using a random-effects model with restricted maximum likelihood estimation and Knapp–Hartung adjustment in Stata 17 (StataCorp). Heterogeneity was evaluated by Cochran's Q and I2, with τ2 reported. In cases of I2 > 50%, we conducted prespecified subgroup analyses by region and study design, and meta-regression on sample size, mean age, and sex distribution. Publication bias was assessed via funnel plots and Egger's test. Sensitivity analyses included leave-one-out diagnostics. Statistical significance was defined as two-sided p < 0.05. Continuous data are presented as mean ± SD or median (IQR/range), and categorical data as counts and percentages.
Results
A systematic search across electronic databases and gray literature yielded 962 unique records. After removing 356 duplicates, 606 articles proceeded to title and abstract screening. Eighteen full-text manuscripts were independently assessed, of which 12 met the predefined inclusion criteria (Figure 1). These studies, published between 2012 and 2023, assessed DTNTs in patients with acute STEMI undergoing fibrinolytic therapy in various regions of Africa. Comprehensive cohort details and patient demographics are presented in Table 1.

PRISMA search flow diagram for study inclusion.
Baseline characteristics and DTNT metrics of participants.
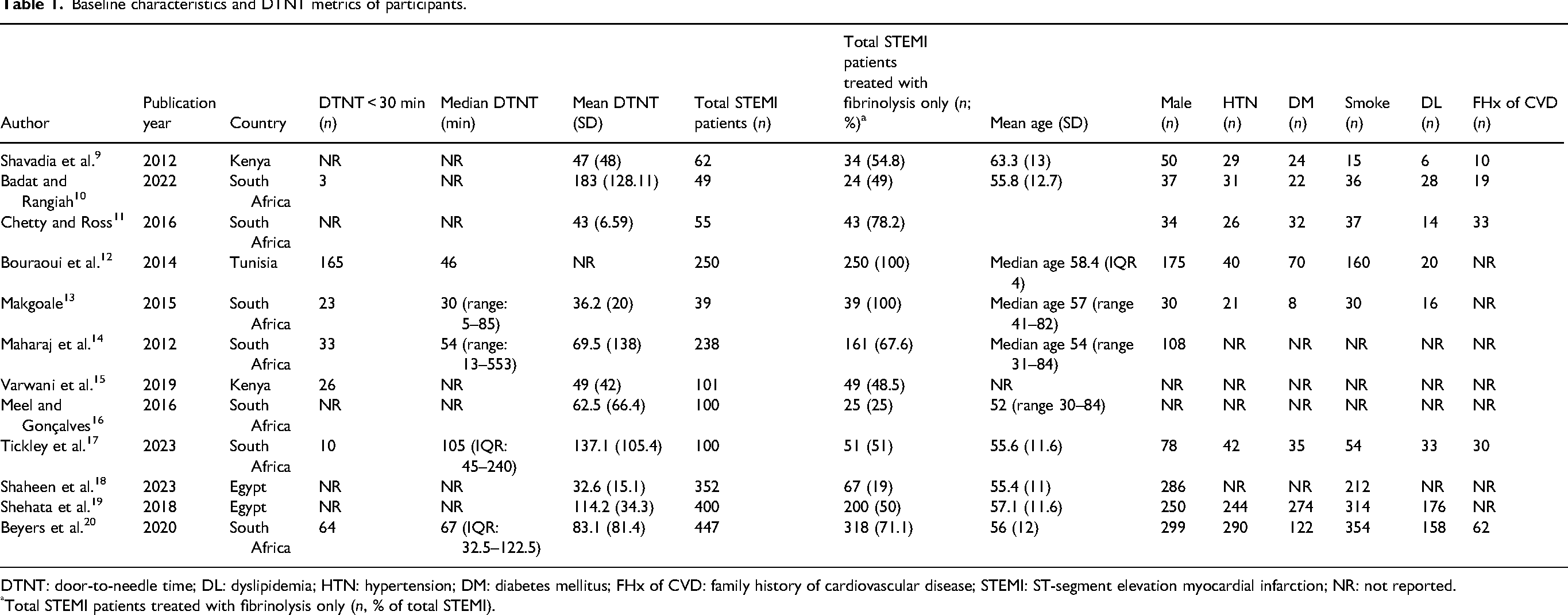
DTNT: door-to-needle time; DL: dyslipidemia; HTN: hypertension; DM: diabetes mellitus; FHx of CVD: family history of cardiovascular disease; STEMI: ST-segment elevation myocardial infarction; NR: not reported.
Total STEMI patients treated with fibrinolysis only (n, % of total STEMI).
Across the 12 included studies, a total of 2193 patients presented with STEMI. Among them, 1261 patients (57.5%) were treated with fibrinolytic therapy (population of interest), while the remainder underwent alternative reperfusion (primary PCI where available, managed conservatively, or received no reperfusion). Seven of the included studies (encompassing 892 thrombolyzed patients) specifically reported the proportion of fibrinolyzed patients achieving a DTNT of ≤30 min. Among these, only 324 patients (36.3%) met the recommended DTNT benchmark of ≤30 min (Table 1).
Of the 12 studies, seven reported mean DTNT with SDs, and four reported medians with either interquartile ranges or full range; these were converted to estimated means and SDs using validated methods.7,8 One Tunisian study 12 reported only the median without dispersion measures, making reliable conversion impossible; this study was therefore excluded from quantitative synthesis. Consequently, 11 studies were included in the meta-analysis of mean DTNT.
Importantly, no study, whether reporting mean or median DTNT, demonstrated an overall cohort time under 30 min. Regionally, the Tunisian study (North Africa) reported a median DTNT of 46 min. 12 In the remaining studies, random-effects pooling yielded a mean DTNT of 73.4 min in North Africa (two studies), 48 min in East Africa (two studies), and 84.2 min in Southern Africa (seven studies). Overall, the pooled mean DTNT across all 11 studies (1011 patients) was 74.8 min (95% confidence interval: 44.4–105.2) (Figure 2). Statistical heterogeneity was markedly high (I2 = 99.4%), and meta-regression analyses found no significant moderating effects of sample size, mean age, geographic region, sex distribution, or study design (Supplemental Tables 1 to 5).
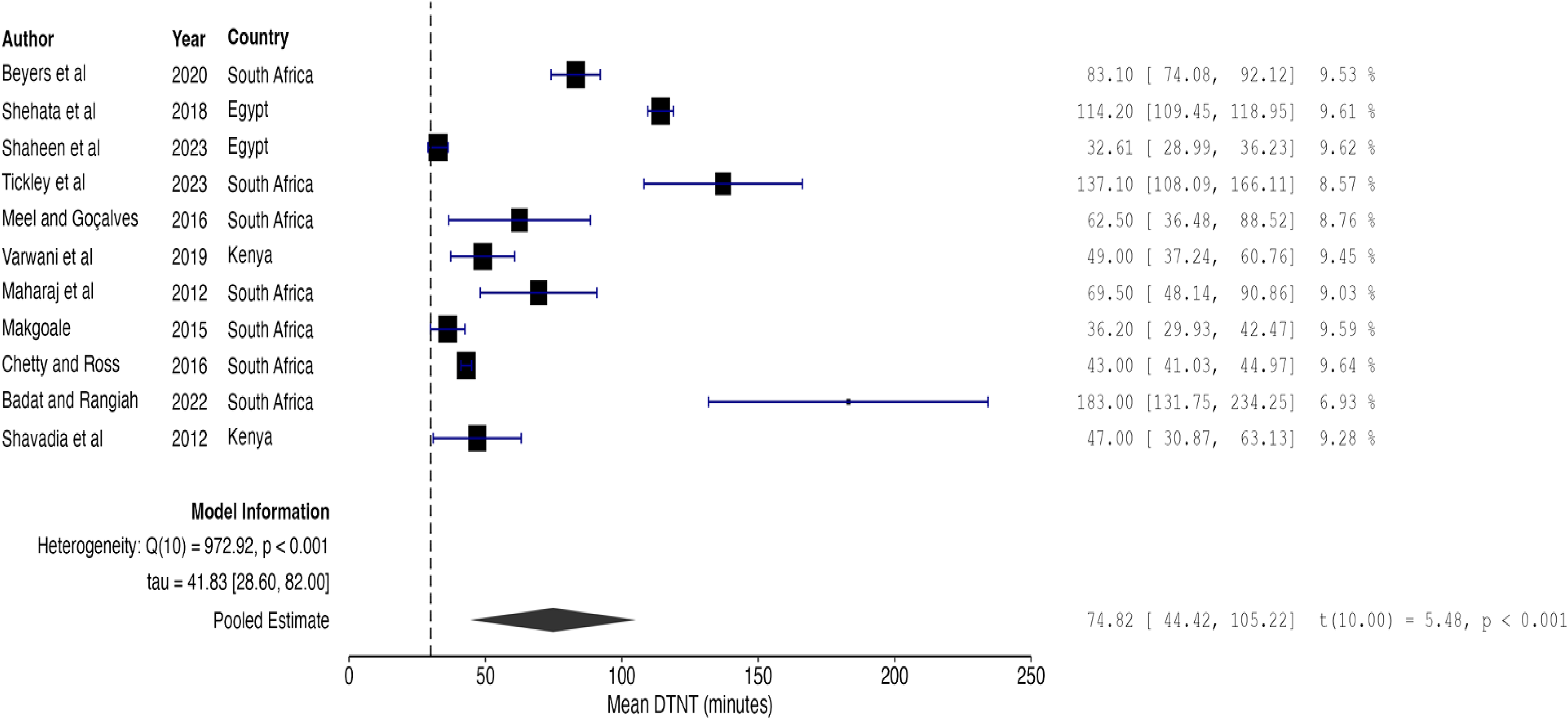
Forest plot showing pooled mean door-to-needle times in STEMI patients across Africa. STEMI: ST-elevation myocardial infarction.
Discussion
Both the American College of Cardiology/American Heart Association and European Society of Cardiology guidelines specify a DTNT of 30 min or less in non-PCI-capable hospitals, underscoring the critical “golden window” for myocardial salvage and mortality reduction. 5 Every minute counts and faster DTNTs are associated with significantly lower short- and long-term mortality.5,6,21
In this first continent-wide meta-analysis of STEMI care in Africa, which included 11 studies and 1011 patients, the pooled mean DTNT was 74.8 min, and only 36.3% of thrombolyzed patients met the 30-min benchmark. Importantly, not one study cohort achieved an overall mean DTNT below 30 min, revealing an alarming and uniform shortfall across diverse settings. By comparison, in the United States’ Get With The Guidelines Coronary Artery Disease registry, the median DTNT was 37 min, with approximately 38.2% of patients treated within 30 min. 22 European data from the Euro Heart Survey ACS III reported a median DTNT of 15–20 min, with more than 60% of patients receiving fibrinolysis within the guideline target timeframes. 23 Even accounting for differences in resources, African centers, where PCI is less available, are nearly twice as slow as U.S. benchmarks and more than four times slower than leading European registries.
Fibrinolysis is inexpensive, widely accessible, and does not require catheterization laboratory infrastructure. Thus, in regions where PCI capacity remains limited, as it is the case in Africa, one would expect rapid pharmacologic reperfusion to be a strength. Instead, our findings—mean DTNT 2.5 times the guideline target and fewer than 4 in 10 patients treated promptly—point to a catastrophic gap in STEMI care that demands urgent attention. Though not explored, contributing factors likely include patient factors (late presentation and delayed first medical contact), underdeveloped emergency medical services (EMS) and poor prehospital triage, need for multiple referrals (door-in/door-out delays), prolonged emergency department triage and time to electrocardiogram (ECG), absence of standardized reperfusion protocols, and limited availability/stocking of thrombolytic agents, among others. Our findings mirror prior reports from other low- and middle-income countries (LMICs) where timely reperfusion remains a challenge. A recent systematic review of ACS treatment delays in LMICs reported prolonged symptom-to-treatment intervals and identified weak emergency transport systems, poor communication between facilities, and organizational barriers as recurring contributors to delay. 24
Fortunately, existing structured quality-improvement initiatives offer a proven blueprint. The American Heart Association's Target: Stroke program, for example, reduced median DTNTs to ≤30 min by implementing multidisciplinary teams, EMS prenotification, and real-time feedback. 25 In STEMI care, strategies such as prehospital ECG transmission, point-of-care biomarker testing, standardized reperfusion pathways, pharmacist-driven order sets, multidisciplinary bundle interventions and continuous performance audit have similarly driven dramatic improvements in timeliness. Comparative reports from South Asia and other LMIC settings similarly reporting median DTNTs substantially exceeding 30 min emphasize pharmaco-invasive, prehospital ECG, and network strategies as pragmatic solutions in resource-constrained settings.26–28 Tailoring these evidence-based strategies to African health systems, emphasizing local leadership, resource-appropriate adaptations, and ongoing data collection could sharply shorten DTNTs and reduce major adverse cardiovascular events across the continent.
Several limitations warrant consideration. The extreme heterogeneity among studies likely reflects fundamental differences in healthcare infrastructure, patient referral patterns, and methodological approaches, which may reduce the precision and applicability of our pooled estimate. Most included investigations were retrospective and single-center, introducing potential selection and reporting biases, and key regions, particularly in Francophone and Lusophone Africa, remain underrepresented. We were unable to account fully for variations in thrombolytic agents, prehospital systems, and definitions of symptom onset, each of which may influence DTNTs. Finally, despite a comprehensive search strategy, relevant data published in non-English languages or housed within national and hospital registries may have been overlooked, potentially biasing our findings.
Conclusion
This study highlights an urgent shortfall in acute STEMI care across Africa: a pooled mean DTNT more than twice the guideline-recommended 30 min, with fewer than 40% of patients receiving timely fibrinolysis. In such settings where PCI remains limited and pharmacologic reperfusion is both inexpensive and broadly accessible, these delays represent a critical barrier to improving patient outcomes. Urgent implementation of standardized reperfusion protocols, strengthened prehospital coordination, multidisciplinary team activation, and continuous performance monitoring is essential to shorten treatment delays, enhance myocardial salvage, and reduce adverse cardiovascular events throughout the continent.
Supplemental Material
sj-docx-1-cvd-10.1177_20480040251396698 - Supplemental material for Door-to-needle performance in African ST-elevation myocardial infarction management: A systematic review and meta-analysis
Supplemental material, sj-docx-1-cvd-10.1177_20480040251396698 for Door-to-needle performance in African ST-elevation myocardial infarction management: A systematic review and meta-analysis by Carlson Sama, Efeturi Okorigba, Saim Rana, Basel Abdelazeem, Huzaifah Qureshi, Ademola Ajibade, Binita Bhandari, Jason Moreland, Mohamad Al-Saed, Meshal Alsulami, Charoo Iyer, Pooja Warrier, Muchi Ditah Chobufo, Bryan Raybuck and Sudarshan Balla in JRSM Cardiovascular Disease
Footnotes
Ethical considerations
Given that this study is based on already published data, a formal ethical approval was not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data supporting the conclusions of this study are included in the manuscript and Supplemental materials.
Guarantor
Carlson Sama.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.