
Abstract
Background
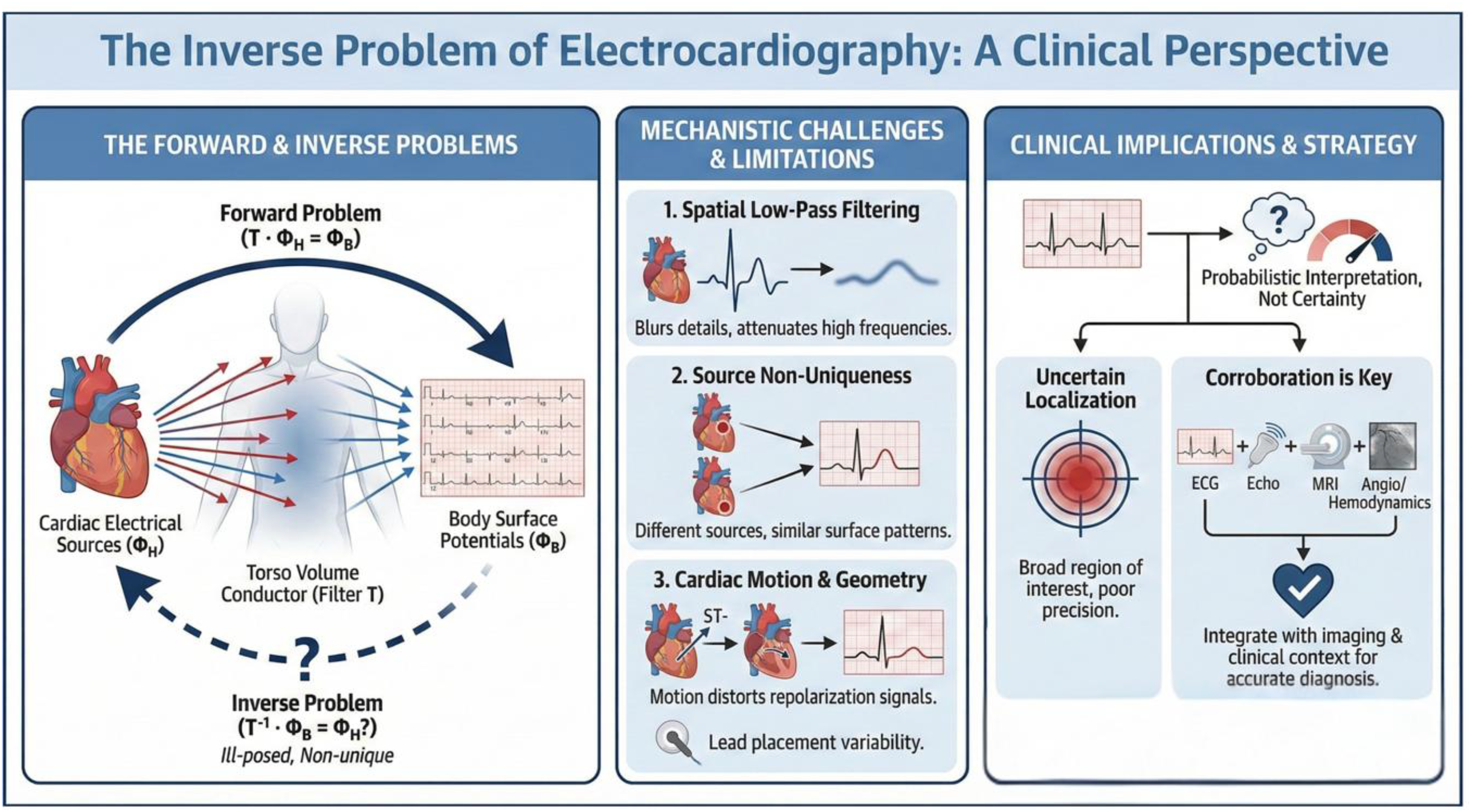
The 12-lead electrocardiogram (ECG) records body-surface potentials that represent cardiac electrical activity filtered through the torso. Recovering the original cardiac sources from these surface signals—the inverse problem of electrocardiography—is mathematically ill-posed: multiple distinct source configurations produce identical tracings. This constraint is seldom discussed in clinical practice, yet it underlies many recognized ECG diagnostic limitations.
Methods
This narrative review provides a clinician-oriented summary of the forward and inverse formulations, and then organizes ECG interpretive pitfalls into five mechanistic categories: volume-conductor filtering, source-model ambiguity, cardiac motion during repolarization, patient-specific anatomy and lead-placement variability, and signal noise and filtering. Each category is linked to quantitative clinical data and to practical reporting recommendations.
Results
Volume-conductor attenuation limits VA localization accuracy to 38.9% at the AHA-segment level. Source ambiguity allows 59% of combined anterior–inferior ST elevation to originate from RCA rather than LAD occlusion, and permits unrelated diseases (pulmonary embolism, arrhythmogenic cardiomyopathy) to produce identical repolarization patterns. Cardiac motion during repolarization introduces time-variant geometric distortion independent of pathology. The Mason–Likar lead system erases established inferior infarctions and shifts QRS axes by up to 60°. Fragmented QRS detects scar (sensitivity 68%, specificity 80%) but fails territorial localization (sensitivity 1.7%). Electrocardiographic imaging reduces localization error but cannot recover spatial detail lost to the torso filter.
Conclusions
The inverse problem imposes identifiability limits on every 12-lead ECG. Territorial labels should be treated as probabilistic and corroborated with imaging or hemodynamics when localization carries therapeutic consequences.
Keywords
Introduction
For over a century, the 12-lead electrocardiogram (ECG) has been the bedrock of non-invasive cardiac diagnosis. Yet every clinician has faced the reality of its limitations: the confounding diagnosis, the localization that proves incorrect in the catheterization lab, the tracing that fails to match the clinical picture. These limitations arise directly from the inverse problem of electrocardiography.
An inverse problem is the process of discovering the cause from the end effect of a phenomenon. 1 In electrocardiography, this means reconstructing cardiac electrical activity from body surface potentials 2 —a task that imposes hard limits on what any surface tracing can resolve.
Consider a jazz quintet inside a concert hall. A listener outside hears a blended composite and can recognize instruments—but cannot determine where each musician stands on stage. The surface ECG faces the same constraint: it records a composite vector sum of countless simultaneous cardiac sources, and multiple distinct source arrangements can produce the same sum (Figure 1).
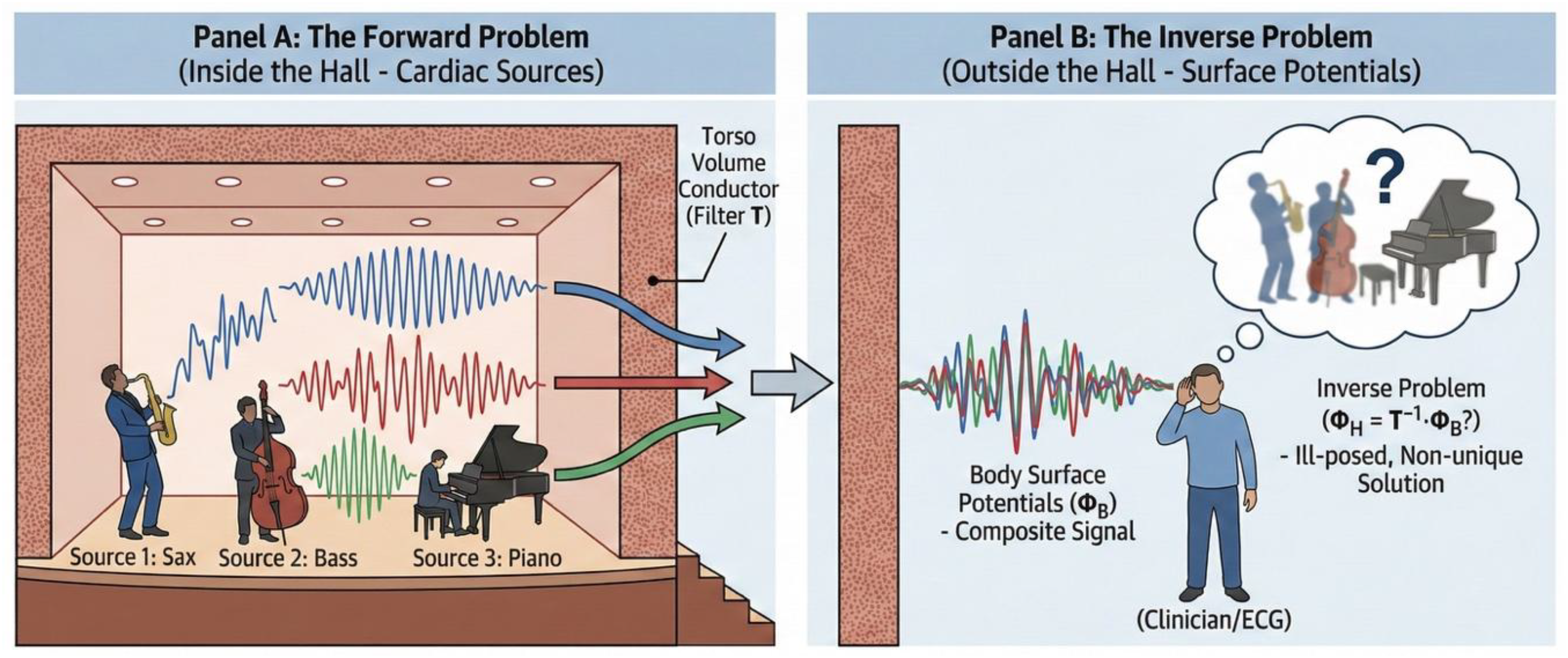
Distinct acoustic sources inside a performance hall can produce similar composite sound patterns when recorded outside, because propagation through the hall acts as a spatial filter that blurs and sums individual contributions. Likewise, cardiac electrical activity is transformed by the torso's conductive properties, so multiple intracardiac source configurations can generate indistinguishable body-surface potentials. The analogy illustrates the central limitation of ECG inverse reconstruction: ΦB does not uniquely identify ΦH. Note: Illustrative elements in this figure were generated using Gemini (Google) and are schematic representations for conceptual purposes only; they do not depict original research data or patient-derived images.
This review provides a clinician-oriented primer on the forward and inverse formulations, including the ill-posed, ill-conditioned nature of the inverse operator, then organizes common ECG pitfalls into five categories: volume-conductor filtering, source-model ambiguity, cardiac motion, lead configuration, and signal noise and filtering—so that each diagnostic limitation can be traced to a specific physical constraint (Table 1).
Mechanistic causes of ECG diagnostic limitation and their clinical consequences.

Legend: Each row maps one physical constraint of the inverse problem to its clinical manifestation and a concrete interpretive approach. The “Cause” numbering corresponds to the manuscript sections. AHA = American Heart Association; ECG = electrocardiogram; fQRS = fragmented QRS; LAD = left anterior descending artery; MI = myocardial infarction; PE = pulmonary embolism; RCA = right coronary artery; STE = ST-segment elevation; VA = ventricular arrhythmia; ΦB = body-surface potentials.
The forward and inverse problems
The forward problem states that if epicardial voltages (ΦH) are known, the body-surface potentials (ΦB) can be computed by solving Laplace's equation in the torso, treated as a passive volume conductor (a standard quasi-static approximation in which the torso's capacitive and inductive effects are negligible at cardiac frequencies).
3
In matrix form, this is
This linear matrix formulation assumes a potential-based source model. Multiple alternative representations of ΦH exist (activation-time maps, equivalent dipoles, transmembrane voltage surrogates), each of which produces a forward operator of different form and dimensionality, and each can produce a similar ΦB—meaning the surface tracing cannot distinguish which model best describes the actual heart.
Recovering ΦH from the measured ΦB requires inverting T. In practice, T is usually rectangular (the number of body-surface electrodes does not match the number of epicardial nodes), so a standard inverse does not exist by definition. More importantly, the problem is ill-posed: even when a square formulation is constructed, T is severely ill-conditioned, meaning that small electrode noise or modeling error in ΦB is amplified enormously in the recovered ΦH and produces non-physiologic epicardial maps. Ill-conditioning, rather than literal non-invertibility, is the operative constraint.
Clinically usable solutions require regularization—mathematical constraints (most commonly Tikhonov smoothing 4 or Bayesian priors 5 ) that select a plausible map from the infinite set of valid ones, trading a small bias for large variance reduction. The choice of regularization parameter is itself consequential: it dictates the effective spatial cutoff of the reconstruction, and different selection criteria can yield materially different epicardial maps from identical patient data. 4 Regularization does not recover information destroyed by the torso filter; it selects the least implausible reconstruction given the data available.
The inverse problem imposes an epistemic limit on every ECG interpretation.
Cause 1—information loss in the volume conductor (spatial low-pass)
A primary use of the 12-lead ECG is to estimate the origin of a ventricular arrhythmia (VA) or premature ventricular complexes (PVC), 6 guiding subsequent invasive mapping and ablation - yet, accuracy is limited. 7 In structural heart disease, a validated algorithm correctly identified the AHA segment of VA origin in only 38.9% of cases. 8
Outflow-tract VA localization fares no better: sensitivity of published ECG criteria spans 29–89% and specificity 51–94%, 9 with correct sub-site identification (septum vs. free wall) in only 59.1% of cases. 10
Cause 2—source-model ambiguity (many-to-one mapping)
In practical terms, even when ST Elevation (STE) is unequivocal, the pattern does not uniquely specify the culprit wall or artery.
This ambiguity is clearest when anterior and inferior STE appear together. 59% of cases reflect proximal RCA occlusion rather than LAD disease. 11 In an ST-elevation myocardial infarction (STEMI) series, 7% of patients with V1–V5 elevation had RCA occlusion. 12 In another study, 8% of patients with RCA occlusion had anterior STE. 13 A pooled analysis of 156 inferior STEMIs tested nineteen ECG algorithms for RCA-versus-circumflex discrimination: the best rule reached 81% accuracy (AUC 0.77) and several popular criteria hovered near 75%. 14
The ‘wrap-around LAD’ explanation is also unreliable. Bozbeyoğlu showed that although a wrap-around anatomy was more common when inferior STE was present (62% vs 30%), sensitivity and specificity were both too low for confident bedside prediction. 15
Reciprocal ST changes compound the ambiguity. They arise from electrical mirroring of the injury vector, true ischemia at a distance in multivessel disease, or right-ventricular involvement that rotates vectors anteriorly and mimics LAD injury. 16 Distal lesion location and coronary anatomic variants further shift vector orientation across conventional territorial boundaries. 15
The same anterior ST–T pattern can arise from unrelated diseases because the surface ECG reflects a geometry-dependent projection of global repolarization. Deep symmetric T-wave inversion in V1–V3—classically attributed to reperfused LAD ischemia (Wellens syndrome)—occurs in acute right-ventricular pressure overload from pulmonary embolism (Figure 2),16–19 and in arrhythmogenic right-ventricular cardiomyopathy. 20
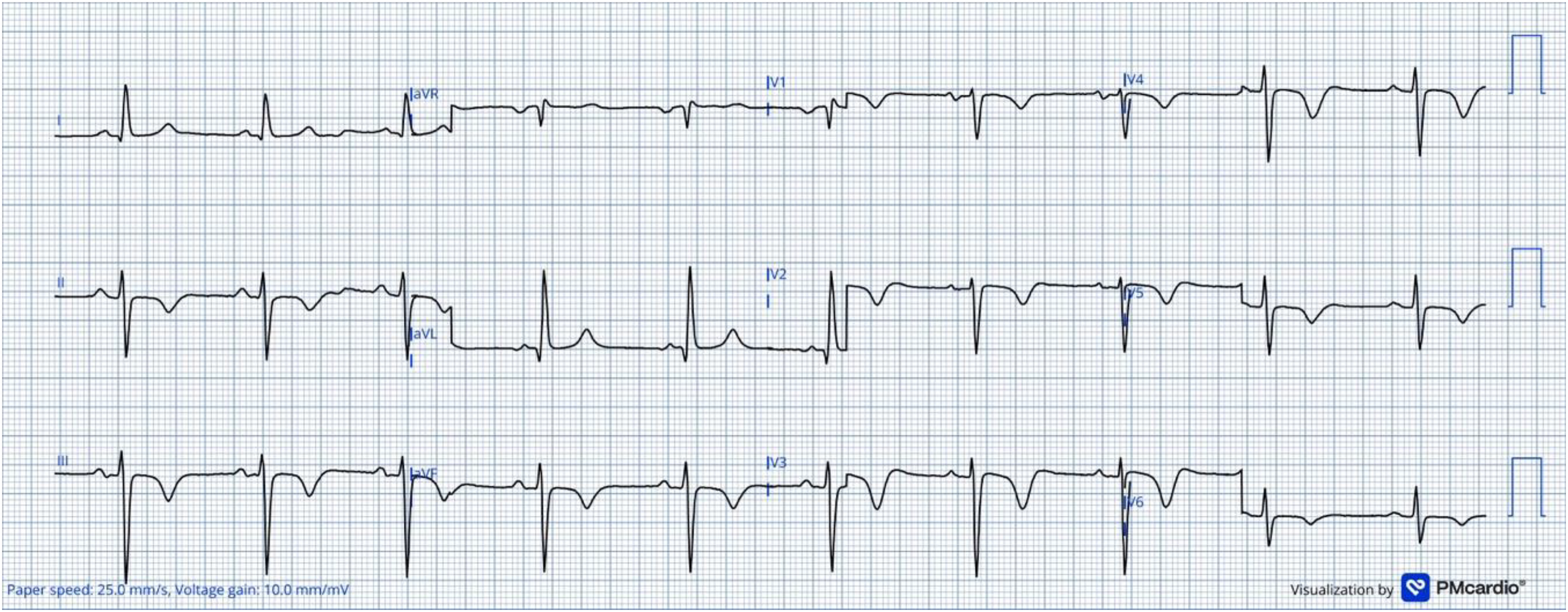
A 12-lead ECG from a patient with acute pulmonary embolism showing deep, symmetric T-wave inversions across V1–V4—a morphology classically associated with proximal LAD reperfused myocardial infarction (Wellens pattern). In the absence of chest pain, this pattern reflects acute right-ventricular pressure overload, septal bowing, and altered repolarization vectors rather than anterior-wall injury: a mechanical pseudo-ischemia in which the ECG signature is generated by abrupt changes in ventricular geometry and loading conditions rather than by compromised coronary flow. Because surface electrodes record a geometry-dependent projection of repolarization currents, the same waveform can represent distinct pathophysiologic states. Context—not morphology alone—determines whether this pattern indicates LAD jeopardy or right-ventricular strain.
Cause 3—time variance from cardiac motion during repolarization
Repolarization coincides with continuous cardiac motion. ECG electrodes remain fixed, but the heart undergoes twist, shortening, and basal–apical translation while the ST segment and T-wave are inscribed, 21 making the forward operator T itself a function of time, T(t), and rendering the inverse problem time-variant and still more ill-conditioned. 3
Adams and Drew showed that simply rolling patients from supine to side positions could produce new ST deviation and marked axis shifts, solely by rotating the heart within the thorax and altering its geometry relative to fixed electrodes. 22
Computational models confirm this: introducing realistic ventricular deformation alters simulated ST–T morphology while leaving QRS largely intact, because repolarization coincides with maximal geometric change. (Figure 3).23–26

During the cardiac cycle, dynamic changes in cardiac position, orientation, and geometry alter the forward transfer matrix T(t) that maps intracardiac electrical sources (ΦH) to body-surface potentials (ΦB). Because repolarization occurs during phases of maximal ventricular deformation, even small shifts in cardiac motion can modify the projection of repolarization vectors onto the fixed electrodes. As a result, ST-segment and T-wave morphology may reflect both electrophysiologic processes and time-varying geometric distortion, increasing uncertainty in inverse estimates of ΦH. Note: Illustrative elements in this figure were generated using Gemini (Google) and are schematic representations for conceptual purposes only; they do not depict original research data or patient-derived images.
In pathology, the effect is amplified. Ionic models of transmural ischemia that rely on transmembrane voltage as the source variable assume a static heart, 27 but ischemia itself alters regional contractility—the ventricle moves differently during precisely the interval when injury currents are projected to the surface. Paradoxical systolic bulging shifts the heart's center of mass and reorients the injury vector. 3 A left-ventricular aneurysm produces the same effect chronically, yielding persistent ST elevation that mimics acute injury. 28
Cause 4—patient-specific anatomy and lead placement variability
Both patient anatomy and electrode position enter the forward operator T. Anatomical variability (cardiac rotation, lung volume, habitus) changes how identical sources project to the skin; lead-placement variability changes what the ECG “sees,” sometimes inverting territorial heuristics.
The right and left ventricular outflow tracts and valve cusps share an intricate three-dimensional sleeve of myocardium that lets a single focus exit from several neighboring sites, possibly blurring chamber boundaries on the surface tracing. 6
The Mason–Likar lead system, used routinely in exercise testing and telemetry, moves limb electrodes to the torso and alters territorial representation. 29 When electrodes are placed on the upper chest and lower torso, leads II, III, and aVF cease to view the inferior wall and instead record predominantly anterior or anterolateral activity. 30 Quantitative data show mean QRS axis shifts of roughly 16–17° rightward, with individual deviations exceeding 60°. T-wave axes shift even more, by +40° on average. 31
Clinically, this geometric distortion erases genuine inferior patterns and creates false anterior or lateral changes. In Jowett et al.'s study, five of six established inferior MIs disappeared when electrodes were moved to torso positions. 32 R-wave amplitudes in II, III, and aVF correlated closely with anterolateral chest leads (V4–V6) rather than inferior. 33 False lateral-infarct patterns occurred in ≈20% of subjects because R-wave amplitude fell > 2 mm in I and aVL, mimicking lateral Q-wave loss. Voltage distortions are systematic: R waves decrease in I and aVL but increase in II, III, and aVF, creating pseudo-hypertrophy or apparent multi-territory injury.30,31 The problem extends to stress testing: because torso electrodes predominantly detect anterior signals, exercise ECGs with the Mason–Likar configuration have poor sensitivity for inferior ischemia. 33
Cause 5—signal noise, filtering, and the illusion of precision
Each surface electrode records the vector sum of all simultaneous cardiac activity, including both scar-related fragmented signals and the dominant healthy-myocardium wavefront. 34 Fragmented QRS (fQRS) is a high-frequency perturbation within a large-amplitude complex—precisely the class of feature most degraded by the torso's low-pass filtering and most sensitive to acquisition bandwidth, filter cutoffs, and noise. 35 Consequently, fQRS topography on the surface is unstable: small processing differences shift where fragmentation appears, and vector summation can project distant substrate into unrelated leads.
Bayés de Luna's correlation of Q-wave patterns with cardiac magnetic resonance imaging (MRI) demonstrates that localization succeeds when the surface marker is broad and low-frequency. In coronary patients, a pathologic Q in II, III, aVF identified inferior fibrosis with roughly 90% accuracy 18 —consistent with the fact that cardiac geometry changes little during the QRS, making the projection stable.
The territorial assumption—that fQRS in V1–V4 indicates anterior scar—is contradicted by the data. A meta-analysis found a pooled sensitivity of 68% and a specificity of 80% for fQRS detection of scar. 36 Localization accuracy is worse. An inferior-wall scar generates fragmented signals that, summed with dominant healthy-ventricle forces, can project a net vector onto the anterior leads, creating fQRS in V1–V4. In Wang et al.'s 460-patient perfusion series, territorial sensitivity of fQRS fell to 1.7%, with a 15.8% false-positive rate in territories with normal perfusion. 37 Similarly, patients with confirmed anterior infarction showed higher fQRS incidence in inferior leads than in anterior leads. 38
Enhanced methods: capabilities and limits
Noninvasive enhancements improve average performance but cannot escape the identifiability limits imposed by the forward operator T.
A comparison of dipole-based and potential-based inverse models using up to 240 electrodes for paced beats and 128 electrodes for spontaneous premature ventricular contractions (PVCs) showed median localization errors of 25.2 mm and 13.9 mm for paced activation, and 30.2–39.2 mm for spontaneous PVCs, depending on model choice. 39 Incorporating torso inhomogeneities modestly increased these errors. A hybrid “ECGI–dipole tracking” model that constrains dipole motion reduced localization error for left-ventricular free-wall PVCs from 31.2 to 6.9 mm. 40
These systems extract and reinforce low-spatial-frequency descriptors that survive the torso filter while suppressing high-frequency noise. Increasing electrode count or adding posterior leads improves field coverage and signal-to-noise ratio, but does not resurrect high-spatial-frequency content lost to the volume conductor.
These advances reduce variance: regularization and learned priors suppress noise amplification, yielding more physiologic reconstructions and reframing outputs as probability regions rather than exact sites. Within these limits, ECGI has established clinical utility in specific settings, including pre-procedural planning of scar-related ventricular tachycardia ablation, localization of accessory pathways, and noninvasive characterization of complex atrial arrhythmias, where its spatial resolution—though coarse relative to intracardiac mapping—is sufficient to shape procedural strategy.7,8,40
The inverse problem also sets hard limits on what a normal ECG can exclude. Because the torso filter preferentially attenuates signals from sources that are far from the anterior chest wall or oriented tangentially to it, some substrates are systematically under-represented on the 12-lead surface. True “posterior” (lateral) myocardial infarction is the archetypal example: isolated posterior injury produces only reciprocal anterior ST depression in V1–V3 in a substantial proportion of cases, and may generate no diagnostic ST elevation on the standard 12-lead at all. 16 The same happens in other situations like right-ventricular infarction, basal-septal scar, and intramural ischemia. The operational consequence is that a “negative” 12-lead ECG cannot rule out these territories with the same confidence that it can rule out, for instance, a large anterior transmural injury. 41
Practical implications for clinicians
Three principles follow from the preceding analysis. First, signal frequency predicts territorial reliability: broad pathologic Q waves survive the volume-conductor filter and localize scar with ∼90% accuracy; fQRS does not reliably localize. Second, large territory-wide ST shifts carry more diagnostic weight than isolated single-lead deviations, which may reflect posture, pressure overload, or paradoxical wall motion rather than focal ischemia. Third, precise spatial localization should not be expected from a standard 12-lead recording; interpretations are better framed as “compatible with” or “suggestive of” a territory, accompanied by the known sensitivity and specificity of the finding, and corroborated with imaging when localization carries therapeutic consequences. When the ECG must guide an irreversible decision—catheterization laboratory activation, ablation target selection, thrombolytic administration—the clinician should explicitly acknowledge the inverse problem's constraints and seek confirmatory data before committing to a territorial diagnosis.
A pragmatic decision framework follows from the categories above. Imaging or hemodynamic confirmation is essentially mandatory when: (i) the proposed intervention is irreversible and territory-specific (e.g. ablation targeting, bypass planning); (ii) the ECG pattern is known to have high many-to-one ambiguity (combined anterior–inferior ST elevation, isolated V1–V3 changes, reciprocal-only findings); (iii) pretest probability favors a territory poorly represented on the surface (suspected posterior, right-ventricular, or basal-septal involvement); or (iv) the recording conditions are atypical (Mason–Likar leads, altered posture, prior infarct geometry). Imaging is comparatively optional when the ECG finding is broad, low-frequency, and internally consistent with a high pretest probability—for example, territorial Q waves concordant with a classical clinical syndrome and stable hemodynamics, where the surface marker (Q waves) survives the torso filter well and the decision is not time-critical.
Conclusion
The 12-lead ECG offers extraordinary clinical leverage, but its accessibility comes at the cost of spatial precision. Each diagnostic pitfall examined here—volume-conductor attenuation, source ambiguity, cardiac motion, lead-configuration artifacts, and high-frequency signal degradation—traces to a specific, quantifiable physical constraint rather than to interpreter error alone. Interpretation should therefore be explicitly evidence-based: territorial labels treated as probabilistic, sensitivity and specificity cited alongside pattern recognition, and imaging or hemodynamic confirmation obtained whenever localization carries therapeutic consequences.
Footnotes
Ethical approval
Not applicable; narrative review of published data.
Patient consent
Not applicable.
Author contributors
G.S.B. conceived the review, performed the literature search, and drafted the manuscript. J.N.A. supervised the project, critically revised the manuscript for intellectual content, and provided final approval. Both authors take responsibility for the integrity and accuracy of the work presented.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Not applicable.
AI use disclosure
Two categories of AI use are disclosed for this manuscript, in accordance with Sage's policy on the use of artificial intelligence in research publishing. (i) Language editing (assistive use): Claude (Anthropic) was used to provide language editing to improve clarity and flow in American English. No identifiable patient information was shared with the tool; all material used for editing was de-identified or paraphrased. The authors reviewed, verified, and take full responsibility for all edited content. (ii) Figure preparation (generative use — disclosed): Selected illustrative elements in Graphical Abstract, Figure 1 and ![]() were generated with Gemini Nano Banana Pro, Google. The AI tool was used to produce schematic, non-data illustrative components intended as representative visual aids to explain conceptual aspects of the forward and inverse problems of electrocardiography. No patient images, no clinical data, and no measured electrophysiological recordings were used as input or output of the AI tool. The AI-generated elements do not represent original research data, clinical measurements, or experimental results; they are conceptual illustrations only. All AI-generated components were reviewed for anatomical and physiological plausibility by the authors, who take full responsibility for the final figure content. The schematic nature of these elements is indicated in the corresponding figure legends. No other individuals or organizations contributed to this work beyond the listed authors.
were generated with Gemini Nano Banana Pro, Google. The AI tool was used to produce schematic, non-data illustrative components intended as representative visual aids to explain conceptual aspects of the forward and inverse problems of electrocardiography. No patient images, no clinical data, and no measured electrophysiological recordings were used as input or output of the AI tool. The AI-generated elements do not represent original research data, clinical measurements, or experimental results; they are conceptual illustrations only. All AI-generated components were reviewed for anatomical and physiological plausibility by the authors, who take full responsibility for the final figure content. The schematic nature of these elements is indicated in the corresponding figure legends. No other individuals or organizations contributed to this work beyond the listed authors.
Author approval
All authors have seen and approved the final manuscript.
Guarantor
José Nunes de Alencar Neto.
Clinical trial registration
Not applicable.
Patient and public involvement statement
Patients or the public were not involved in the design, conduct, reporting, or dissemination plans of this research.
Permission to reproduce material from other sources
Not applicable.