
Abstract
Objective
The study aimed to investigate which anthropometric indicator are most associated with cardiovascular risk (CVR) in low-income women with short stature and to determine the cut-off point that best determined CVR.
Methods
This cross-sectional study was conducted with meticulous attention to detail. We evaluated a comprehensive range of sociodemographic and anthropometric data, including body mass index (BMI), waist circumference, waist-to-hip ratio, waist-to-height ratio, and body adiposity index. Additionally, dietary and biochemical data such as glucose and lipid profile, ultrasensitive C-reactive protein (CRP), and blood pressure were assessed in 83 women. Body composition was measured using dual-energy X-ray absorptiometry.
Results
Approximately 85% had excess total body fat, 70% had low levels of high-density lipoprotein and increased levels of ultrasensitive CRP, 29.3% were hypercholesterolemic, and 13.4% were hypertensive. Multivariate logistic regression analyses indicated that BMI was the most associated factor of CVR (ultrasensitive CRP) (OR: 1.31, 95% CI: 1.10–1.56). The area under the receiver operating characteristic curve was 0.64 for cholesterol (95% CI 0.517–0.766; p = 0.04) and 0.72 for ultrasensitive CRP (95% CI 0.601–0.840; p = 0.002). BMI cut-off points with the best balance of sensitivity and specificity were 24.0 kg/m2 for identifying hypercholesterolemia and 23.8 kg/m2 for identifying elevated high-sensitivity CRP levels.
Conclusion
BMI was the most associated factor of CVR in low-income women with short stature. The results indicate that more sensitive BMI cut-off points should be considered to detect CVR in this population group.
This is a visual representation of the abstract.
Introduction
The most prevalent form of malnutrition worldwide is short stature, and it is identified to a greater extent in areas of poverty and populations living in urban areas.1,2 Short stature has been associated with adaptations in tissues and organs, which can cause an increase in the frequency and intensity of diseases throughout life.3,4 In women, short stature has been linked to unfavorable maternal and child health conditions, including an increased likelihood of premature births 5 and giving birth to children with low birth weight.5,6
It is also possible to identify that short stature in adulthood has been associated with obesity,7–9 dyslipidemia, 10 hypertension, 11 inflammation, 12 and increased morbidity and mortality from cardiovascular diseases (CVDs). 13 It is, therefore, important to determine how best to assess cardiovascular risk (CVR) factors in adults with short stature.
Epidemiological studies in populations without short stature have identified several anthropometric indices that are sensitive, specific, non-invasive, reproducible, and economical for predicting total and regional body fat, CVR, and CVD mortality.14–17 In this respect, it is clear that body mass index (BMI), waist circumference (WC), waist-to-hip ratio (WHR), waist-to-height ratio (WHTR), and body adiposity index (BAI) are all associated with a higher prevalence of CVR, such as hypertension, dyslipidemia, and an increase in inflammatory markers such as C-reactive protein (CRP).14–18
However, there is little evidence to suggest which anthropometric index are the most associated factors of CVR in women with short stature. Therefore, this study aimed to investigate which anthropometric indicator (BMI, WC, WHR, WHTR, and BAI) was most associated with elevated high-sensitivity CRP (hs-CRP) levels, an inflammatory biomarker associated with increased CVR, in low-income women with short stature.
Materials and methods
Ethical aspects
The procedures were conducted in accordance with the guidelines of the Helsinki Declaration, and all procedures involving human subjects were approved by the Research Ethics Committee of the Federal University of São Paulo (protocol number 1731/11). Written informed consent was obtained from all subjects.
Study design, location, and sample
A cross-sectional study was carried out in socially vulnerable areas of a capital city in northeastern Brazil. The study included low-income women with short stature, aged between 18 and 45 years. The women recruited were mothers of children attending the day-boarding school center at the Center for Recovery and Nutritional Education (CREN-Alagoas). Low-income was defined as a per capita household income below US$1.00 per day, consistent with extreme poverty thresholds. Socially vulnerable areas were defined as urban regions characterized by low household income, limited access to health services, reduced educational attainment, and precarious housing conditions.
Of the 100 mothers invited, 83 were included in the study. The inclusion process is described in Figure 1. This was a non-probabilistic convenience sample. Short stature was defined as height below the 25th percentile (<158 cm) of the growth curve for women at 19 years of age. 19 This cut-off has been used in epidemiological studies to identify adult women exposed to chronic undernutrition and adverse socioeconomic conditions during critical periods of growth.20–22 Women with known pathological causes of short stature, including genetic syndromes (e.g. Turner syndrome, Noonan syndrome), endocrine disorders, or congenital conditions associated with increased CVR, were not included.
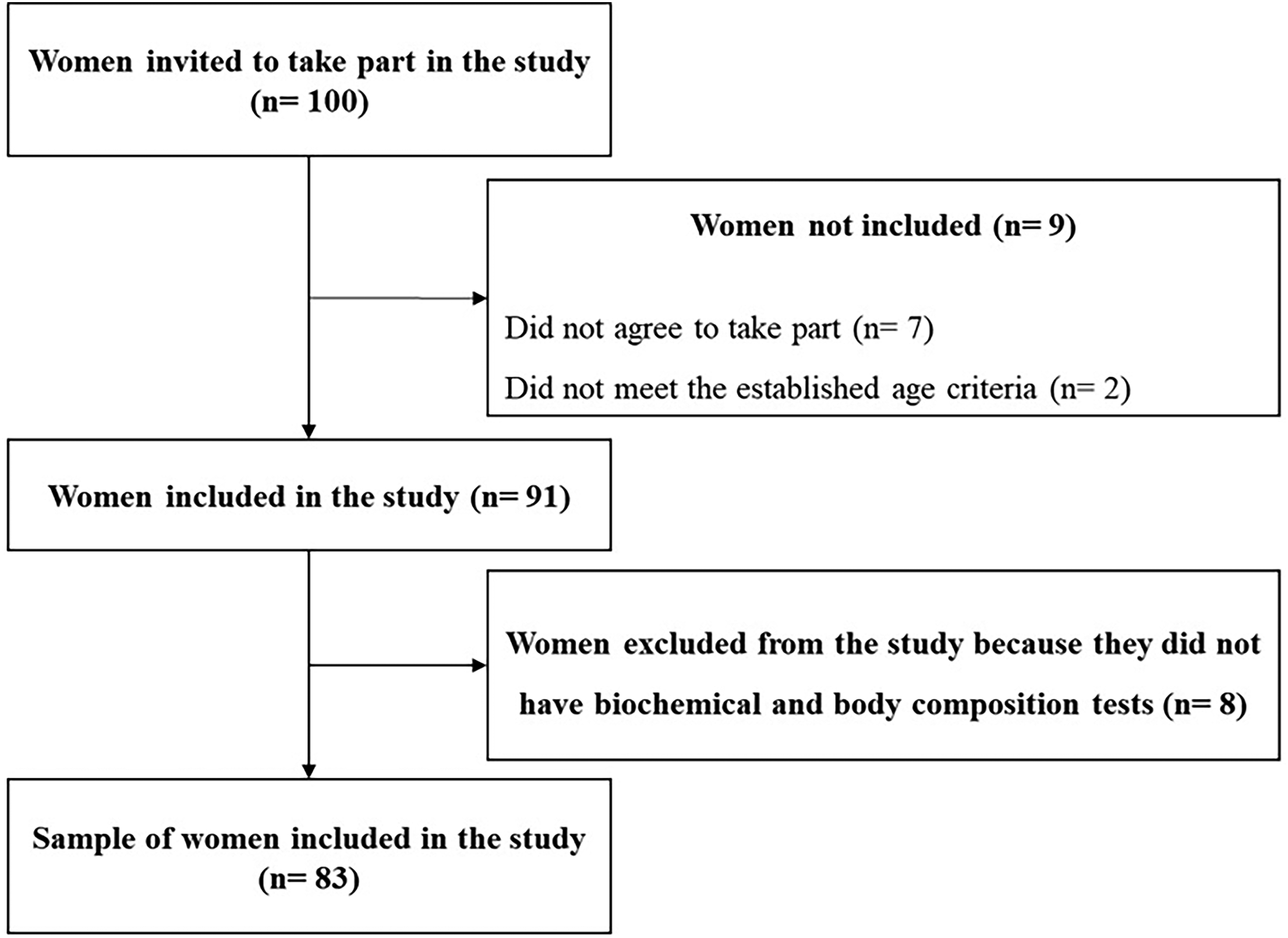
Flowchart showing the process of including women in the study.
Sociodemographic and lifestyle habits
Information was collected on age, per capita income, number of years of schooling, number of rooms per household, number of residents per household, hours spent in front of the television, hours of physical activity, and whether the women consumed alcohol or smoked.
Information on current medication use was collected, including lipid-lowering agents, corticosteroids, and hormonal contraceptives. Women using medications known to significantly interfere with lipid or inflammatory markers, including lipid-lowering drugs, systemic corticosteroids, chronic anti-inflammatory or immunosuppressive agents, were not included in the analysis.
Anthropometric parameters
Weight and height were collected to determine the BMI of the women. BMI was then classified as underweight (< 18.5 kg/m2), adequate weight (≥ 18.5 < 25 kg/m2), overweight (≥ 25 < 30 kg/m2), and obesity (≥ 30 kg/m2). 23 WC and hip circumference (HC) were also measured using a flexible tape measure, and the cut-off point used for WHR and WC was 0.80 and 80 cm, respectively. WHTR was calculated as the ratio between WC (cm) and height (cm), with a cut-off point for abdominal obesity associated with increased CVR as a ratio ≥ 0.5. BAI was obtained based on HC and height, according to Bergman et al., 16 using the following equation: BAI = [HC/(height)1.5]-18. Individuals with values between 33 and 38 were considered overweight, and those with values above 38 were considered obese.
All anthropometric measurements were obtained by trained health professionals following standardized protocols. Measurements were performed by two previously trained examiners, using calibrated equipment. Weight was measured with the participants barefoot and wearing light clothing. Height was measured using a stadiometer, with participants standing upright, barefoot, and with the head positioned in the Frankfurt plane. WC was measured at the midpoint between the lowest rib and the iliac crest, and HC at the widest portion of the gluteal region. Measurements were taken in duplicate, and the mean value was used for analysis.
Body composition
Body composition (trunk fat, android fat, gynoid fat, and total fat) was assessed using dual-energy X-ray absorptiometry (DXA, GE healthcare®, Bedford, UK). The DXA was calibrated using a phantom, and quality control was assessed according to the manufacturer's specifications.
Dietary parameters
A 24-h food recall was carried out on 3 non-consecutive days, one of which was a weekend. The individual's food intake was assessed according to its nutrient content using the Nut Win program, Version 1.5.2.51 (Nutrition Support Program, developed by the Department of Health Informatics at the Federal University of São Paulo, São Paulo, Brazil). An average amount of food consumption was calculated from the three food recalls carried out.
Blood pressure
Blood pressure was measured in triplicate with an automated blood pressure monitor (OMRON HEM-705CP, Vernon Hills, IL). Women who were using antihypertensive medication or had systolic blood pressure ≥ 140 mmHg and/or diastolic blood pressure ≥ 90 mmHg were classified as hypertensive.
Biochemical parameters
For this procedure, blood samples were collected after a 12-h fast in a specialized laboratory. The values for total cholesterol (TC), high-density lipoprotein (HDL), triglycerides (TG), and glucose were determined using an enzymatic assay. The concentration of low-density lipoprotein (LDL) was determined according to Friedewald's formula: LDL = TC-(HDL + TG/5). The following ratios were calculated: the Castelli I index: TC/HDL, the Castelli II index: LDL/HDL, and TG/HDL.
Insulin values were determined using the electrochemiluminescence method. The homeostatic model assessment index for insulin resistance (HOMA-IR) was calculated using laboratory glucose and insulin concentrations using the formula proposed by Matthews et al. 24 : HOMA-IR = insulin (mU/mL) x glucose (mg/dl)/22.5.
hs-CRP was used as an inflammatory marker and measured using an ultrasensitive immunonephelometric method. According to the literature, hs-CRP concentrations between 1 and 3 mg/L are indicative of intermediate CVR.25,26 In the present study, elevated inflammatory status was defined as hs-CRP >1 mg/L, considering that hs-CRP acts as an early marker of CVR even at moderate concentrations 27 and that CVR increases progressively across the CRP distribution rather than only at markedly elevated levels. 28 Furthermore, this cut-off represents a more sensitive threshold for detecting low-grade systemic inflammation in apparently healthy adult women, in whom inflammatory marker levels are typically lower.25,27
TC and hs-CRP were selected due to their well-established association with cardiovascular morbidity and mortality, and their frequent use as intermediate CVR markers in population-based studies.
In this study, hs-CRP was used as an inflammatory biomarker associated with cardiometabolic and CVR, rather than as a direct measure of CVD.
Statistical analysis
As previously described, the sample size was determined using a non-probabilistic convenience sampling approach. However, the final analytical sample (n = 83) is consistent with methodological recommendations indicating that samples ranging from approximately 50 to 100 participants allow reliable estimation of the area under the receiver operating characteristic curve (AUC) in receiver operating characteristic (ROC) analyses, particularly in exploratory diagnostic studies.29,30 Furthermore, this sample size is comparable to that adopted in previous studies investigating cardiovascular outcomes using ROC curve analysis,31,32 supporting the adequacy of the present sample for evaluating discriminatory performance and estimating cut-off values. The Lilliefors test was used to test normal distribution. The chi-square test was used to compare the frequency of overweight among different methods (DXA, BMI, IAC).
We conducted a series of multivariate logistic regressions, with the dependent variable being the category of hs-CRP (normal or high) and the independent variables being those that could influence CRP (anthropometrics and DXA components). All variables were adjusted for sociodemographic, behavioral, and dietary covariates (age, per capita income, education, smoking, drinking, physical activity, and saturated fat intake). Subsequently, several multivariate logistic regression models with the “forward” technique using the best likelihood ratio (including anthropometric variables and the components of DXA, separately) were built to see which parameter within each group (anthropometric measures and DXA) could be associated with the risk of presenting elevated CRP levels.
ROC curves were used to establish BMI cut-off points for SS women that could be used as a discriminatory factor for the risk of hypercholesterolemia (>200 mg/dl) and increased CVR, according to the CRP levels (CRP>1 mg/dl). The area under the ROC curve was used to determine the overall accuracy of BMI as an associated factor of high cholesterol and CRP levels. ROC curve analyses were performed using hs-CRP and TC due to their established role as early biomarkers of cardiometabolic and CVR in population-based studies.
Only participants with complete data for the variables included in each specific analysis were considered. Missing data were handled by complete-case analysis, and no imputation procedures were applied.
Statistical analyses were carried out using the R statistical package (R Foundation for Statistical Computing, Vienna, Austria). For the levels of statistical significance, alpha values of 5% were adopted.
Results
Our study sample consisted of a total of 83 women with short stature, whose characteristics are summarized in Table 1. Per capita income was <$1.0 US/day, and the average schooling was <5 years of study, with 45.8% of the subjects considered as functionally illiterate. The prevalence of overweight found by the DXA was significantly higher than the prevalence obtained by the BAI and BMI (p < 0.001) (Table 2).
Sociodemographic, nutritional, and metabolic characteristics of the studied sample (n = 83).
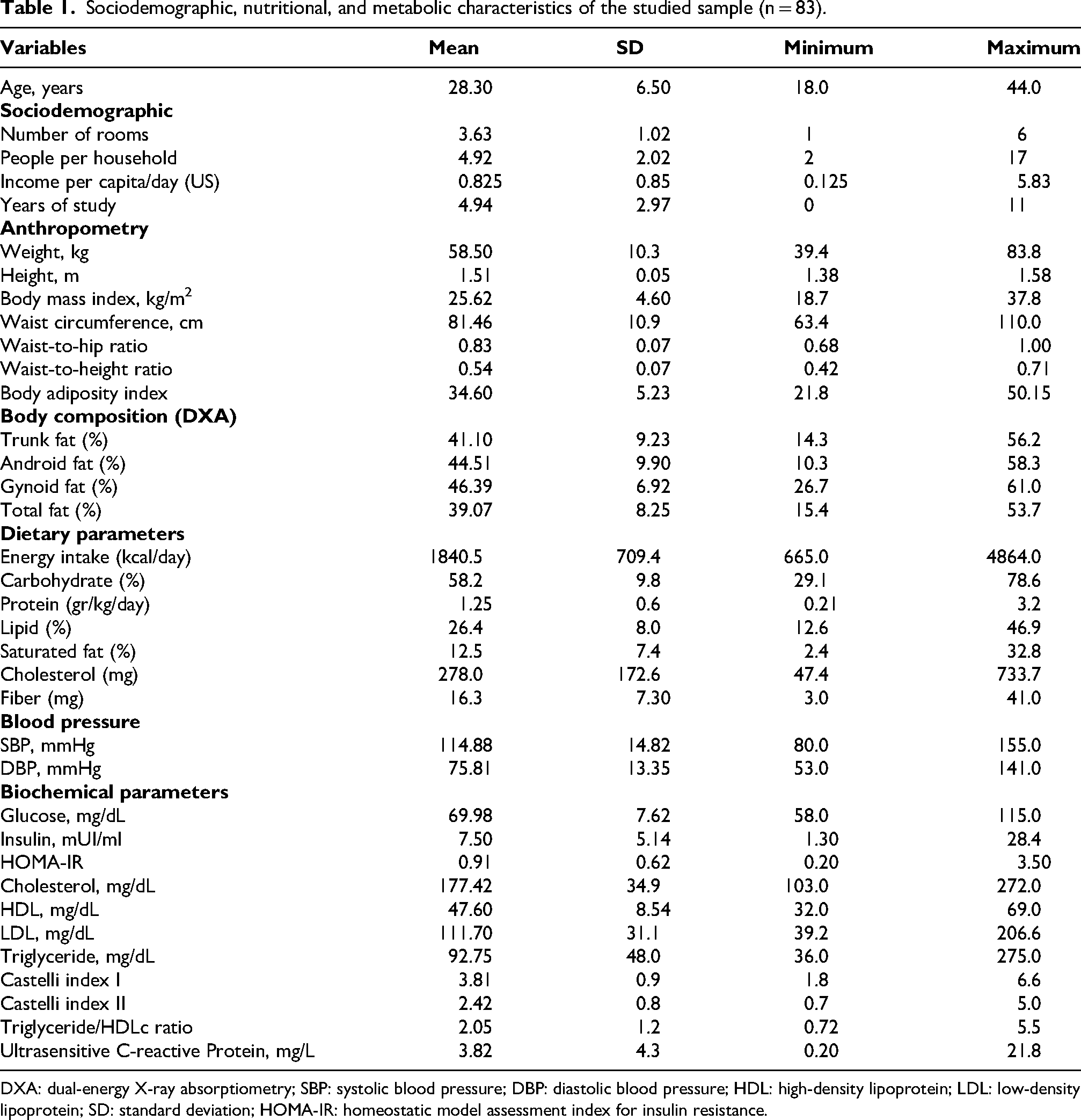
DXA: dual-energy X-ray absorptiometry; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein; LDL: low-density lipoprotein; SD: standard deviation; HOMA-IR: homeostatic model assessment index for insulin resistance.
Frequency of cardiovascular risk factors in the studied sample (n = 83).

BMI: body mass index; BAI: body adiposity index; DXA: dual-energy X-ray absorptiometry; SBP: systolic blood pressure; DBP: diastolic blood pressure; LDL: low-density lipoprotein; HDL: high-density lipoprotein; HOMA-IR: homeostatic model assessment index for insulin resistance.
Chi-square test < 0.05.
Table 3 shows the values for the multivariate logistic regression adjusted for sociodemographic, dietary, and behavioral variables with the use of CRP levels as the dependent variable. In regard to the anthropometric variables, only WHR was not significantly associated with CRP levels. The logistic regression analysis with the “forward” technique using all DXA variables (android fat, gynoid fat, trunk fat, and total fat) and based on the likelihood ratio showed that android fat was the most associated with CRP levels (OR: 1.15, 95% CI: 1.04, 1.20). The same model was performed for all anthropometric variables (BMI, WC, WHR, WHTR, and BAI) and showed that BMI was the most associated with CRP levels (OR: 1.31, 95% CI: 1.10, 1.56).
Multivariate logistic regression models according to ultrasensitive C-reactive protein category using the variables of interest (n = 83).

Adjusted for age, per capita income, education, smoking, alcohol consumption, physical activity and saturated fat.
CI: confidence interval; DXA: dual-energy X-ray absorptiometry.
Results from the ROC curve analysis (Figure 2(a)) was 0.64 for cholesterol (95% CI 0.517–0.766; p = 0.04) with a BMI cut-off point of 24.2 kg/m2, presenting a sensitivity and specificity of 0.586 and 0.750, respectively. The area under the ROC curve was 0.72 (95% CI 0.601–0.840; p = 0.002) for CRP. The cut-off point of 23.8 kg/m2 had the most suitable balance between a sensitivity of 0.661 and a specificity of 0.727 (Figure 2(b)).

Area under the curve, confidence interval and cut-off point of body mass index as a predictor.
At baseline, a substantial proportion of the participants presented metabolic alterations, including elevated TC, increased LDL cholesterol, reduced HDL cholesterol, and elevated hs-CRP levels, despite the absence of clinically diagnosed CVD.
Discussion
Taking into account the scarcity of evidence proposing to establish anthropometric measures, as well as their cut-off points, that are more sensitive for identifying inflammatory and cardiometabolic alterations associated with increased CVR in adults with short stature, we set out to minimize this gap in knowledge. Our findings show that BMI was the most sensitive anthropometric indices assessed for identifying elevated hs-CRP levels, which are associated with increased CVR, compared to WC, WHR, WHTR, and BAI. In addition, the results of a ROC curve analysis showed greater sensitivity for a BMI of 23.8 kg/m2. Although the observed AUC values indicate only modest discriminatory performance, they suggest that lower BMI cut-off points may be relevant for identifying early cardiometabolic alterations in women with short stature.
Establishing this type of information is relevant, given that chronic non-communicable diseases (NCDs) are responsible for almost 17 million deaths every year, 86% of which occur in low- and middle-income countries, and that CVDs are among those that most affect the population. 33 Several risk factors are related to the development of CVD, particularly age, dyslipidemia, diabetes, high BMI, smoking, and hypertension.34–36 Among these factors, hypertension deserves attention, given its relationship with height, and it is possible to identify that the prevalence of hypertension is inversely proportional to height. 11
It is also important to note the relationship between CVD and anthropometric parameters such as BMI and WHR, as well as body fat percentage. In this respect, a study carried out in Mexico that used the bioimpedance technique to assess the percentage of body fat identified that individuals with short stature had a higher percentage of fat compared to taller individuals, even among those with the same BMI value, suggesting that a BMI of 25 kg/m2 should be used as the cut-off point for obesity in this population. 37 However, the authors pointed out the limitations of their study, including the use of bioimpedance and the absence of a comparison of their results with biochemical markers, 37 which suggests caution in interpreting the results.
Taking this limitation into account, we evaluated the serum lipid profile of the women included in this study, given its relationship with CVD, 38 and it was possible to observe various alterations such as hypercholesterolemia, increased LDL, and low HDL levels. This information is relevant given the need for more information on this type of assessment in women with short stature. A study carried out in the USA between 1984 and 2005 showed that an increase of 10 cm in height was associated with a reduction of between 8 and 18% in TC in women. 39
An increase in the TC/HDL ratio has also been observed in low-income women living in Brazilian favelas, as well as a decrease in HDL levels, 10 changes related to the lipid profile that can be observed from childhood in the poorest population. 40 Given this scenario, especially in relation to long-term changes in the lipid profile, the chance of CVD increases sharply, leading to a greater risk of coronary heart disease and myocardial infarction. This situation shows the need for permanent and continuous assessment of these biochemical parameters, 41 especially in women with short stature since they are more likely to have lipid changes. 42
Another point that deserves attention when it comes to CVD is dietary intake. This assessment was also carried out in this study, and it was possible to see that the proportion of macronutrients, as well as saturated fat and cholesterol, was within the recommendations. 43 However, it has been observed that the eating habits of low-income women have changed over time. It is possible to identify the greater inclusion of ultra-processed foods in their diet. 44 This situation contributes to a higher consumption of free sugars, total fats, and saturated fats, as well as a decrease in fiber, protein, vitamins, and minerals. 45
This scenario shows that poorer women have a greater chance of compromised nutritional status over time, especially in relation to higher BMI and WC. 44 This scenario tends to get worse, given the projections related to the price of ultra-processed foods, showing that by 2030, they will be substantially cheaper than fresh/minimally processed foods, favoring a progressive increase in their consumption, especially among the poorest. 46
These findings, coupled with the physiological disparities identified in women with short stature, such as a decrease in serum levels of the thyroid hormone T3, suggest a greater physiological program to save energy, 10 indicating a reduced basal metabolic rate, which can be inferred to impair their thyroid function, resulting in increased TC levels. 47 Therefore, it is possible to infer that the women in this study underwent similar physiological adaptations, leading to compromised energy expenditure and contributing to a higher proportion of body fat, increasing CVR.
In addition to the traditional CVR factors, 48 high levels of CRP, a biochemical parameter that indicates inflammation, have also been shown to be an important risk factor for CVD.49,50 In this study, more than 70% of the women investigated had moderate or high levels of CRP. This situation is noteworthy because, for every one standard deviation increase in CRP levels, there is a 20% increase in CVD risk. 51
A longitudinal study carried out in Turkey showed that in women of short stature, CRP levels are higher, and this parameter can be used as an independent risk marker for coronary heart disease in women of short stature. A height below 160 cm is a strong marker of death. 9 The authors concluded that influences in early life may be gender-specific in determining pro-inflammatory status and that short stature was an independent risk factor for coronary heart disease. 12 Even in light of the above, evidence like this, relating to women with short stature, still needs to be discovered, highlighting the need to assess this population group better.
Based on these findings, we can suggest a possible relationship between the type of environment to which these women were exposed early in life and the presence of inflammatory mediators in adulthood, 12 a situation which, when we look at the poorest population, shows that the environment has a direct relationship with their health situation as early as childhood, directly influencing their nutritional status.52,53 It can also be seen that the environment influences the development of NCDs, which are a risk factor for CVD, 54 as well as their eating habits. 55
Thus, when evaluating anthropometric parameters while accounting for potential confounders, BMI was the anthropometric measure most strongly associated with elevated hs-CRP levels, an inflammatory biomarker associated with increased CVR, compared to WC, WHR, WHTR, and BAI. This remained significant after adjusting for age, education, per capita income, saturated fat intake, smoking, alcohol consumption, and physical activity. This finding is important, especially given that BMI, among the anthropometric parameters assessed, is the easiest to measure, 56 especially when looking at the material resources needed to measure it, given its greater availability in health services. 57
From these findings, ROC curves were constructed to establish which BMI cut-off points could be used to identify elevated hs-CRP levels (hs-CRP >1 mg/L) and hypercholesterolemia (>200 mg/dL). The findings from the ROC curves showed that these metabolic changes are already taking place in women with a BMI of 23.8 kg/m2. Similar values were found in the Asian population. 39 However, depending on the sample investigated, different BMI cut-off points from those usually recommended might be more reliable. 42 When combined with the use of methods that have yet to be validated for specific populations, this may result in erroneous diagnoses and interventions. Another study demonstrated that the suitability of BMI for detecting individuals with comorbidities associated with obesity was significantly lower in Mexicans with short stature compared to those without short stature. The findings were similar even when a more sensitive cut-off point for defining individuals as overweight was used. 58
Among the strengths of this study are that we highlight the population studied, adult women with short stature, and a population that has a lack of data and/or comparisons similar to those of this study available in the literature. In addition, the technique used to evaluate CRP was ultrasensitive immunonephelometric, which increases the sensitivity and reliability of the method. In order to guarantee the sensitivity of the measurements to the differential diagnosis of an infectious process, we excluded CRP levels >10 mg/L from the study. 26 These considerations reinforce the interpretation that hs-CRP levels in this study most likely reflect low-grade systemic inflammation associated with increased CVR, rather than acute infection. In addition to the number of biochemical and anthropometric assessments, which better characterized the study sample, it was also possible to investigate more factors related to the outcome assessed.
This study also has some limitations, such as its cross-sectional design, which does not allow us to determine a temporal relationship between BMI and CVR. As well as the sample size. However, taking into account the number of assessments carried out, the sample size is similar to that observed in other studies. Another point concerns the fact that the presence of acute infectious disease was not assessed, a situation which may be reflected in the CRP levels found. However, it is highly unlikely that more than 70% of the individuals had an acute infection at the time of the study. In addition, the lack of controls occurred because there were no individuals in this very low-income population who reached the 50th percentile of height or were close to it. The relatively small sample size may have limited statistical power, particularly for multivariable analyses. However, the sample size is comparable to that of similar studies involving detailed biochemical and body composition assessments. The generalizability of these findings is limited, as the study population consisted of low-income adult women with short stature living in socially vulnerable urban areas. Therefore, the results may not be directly applicable to populations with different socioeconomic or demographic profiles.
Conclusion
BMI showed the strongest association with CVR biomarkers in women with short stature compared to the other anthropometric parameters investigated (WC, WHR, WHTR, and BAI). The most sensitive and specific cut-off points for identifying hypercholesterolemia risk and elevated ultrasensitive CRP levels were 24.2 kg/m2 and 23.8 kg/m2, respectively. These findings suggest that women with short stature may be more susceptible to early alterations in biomarkers associated with CVR.
Footnotes
Acknowledgment
To the Nutritional Recovery and Education Center (Centro de Recuperação e Educação Nutritional—CREN) of Alagoas for all logistical support.
Ethical considerations
The study was approved by the Research Ethics Committee of the Federal University of São Paulo (protocol number 1731/11).
Consent to participate
Written informed consent was obtained from all subjects.
Author contributions
Conceptualization was done by RPAB and LGRSN. Investigation was done by TMMTF and NBB. Methodology was done by APGC and ALS. Writing–original draft was done by LAC and GYC. Writing–review and editing was done by EAJ and GYC. Supervision was done by LGRSN.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Foundation of the State Research of Alagoas [grant number 20090132001-6]. The funding sources had no involvement in the design or the study; collection, analysis, or interpretation of the data; or decision to submit the article for publication.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.