
Abstract
Background:
The diagnostic work-up of patients with acute chest pain in the emergency department (ED) is a challenging task. Serial troponin testing is required to rule-out acute myocardial infarction.
Objective:
To evaluate the value of myeloperoxidase (MPO) testing in sensitive cardiac troponin I (cTnI) negative patients with suspected acute coronary syndromes (ACS) in the routine setting of an ED.
Methods:
MPO was assessed in 432 consecutive patients presenting to the ED with ACS. In 266 patients, serial blood samples were available. After 6 weeks, major adverse cardiac events (MACE) were assessed. MPO and cTnI were measured in all available samples. For cTnI, a sensitive assay was used. Cut-off values were derived from an independent sample of 300 healthy volunteers.
Results:
Incidence of MACE in our population was 13%. MPO levels revealed sensitivity (Sens) of 82.1% and specificity (Spec) of 37.2% for MACE compared with 60.7% Sens and 61.4% Spec for sensitive cTnI. In serial sensitive cTnI negative patients (n=218), MACE incidence was 6.4%. MPO continued to demonstrate significant discriminatory power for the prognosis of MACE. Multivariate analyses confirmed these findings.
Conclusion:
MPO has an independent prognostic value overall and most notably in patients tested negative with a higher sensitive cardiac troponin I assay. MPO could be a promising biomarker for the initial evaluation of patients in chest pain units and is worth further investigation.
Introduction
In chest pain units (CPU), which are part of the emergency department (ED), large numbers of patients with chest discomfort are evaluated for acute coronary syndromes (ACS). The prevalence of true ACS is usually around 50% in this population; patients with atypical symptoms and initial negative troponin and ECG are often sent home 1 although the event rate in this group is reported to be up to 14% in 6 months 2 with a 2–5% mortality. 1 To exclude acute myocardial infarction (AMI) these patients require serial troponin testing. 3
Reactive oxygen species play an important role in cardiovascular disease including the events associated with AMI.4,5 They have been implicated in numerous cardiovascular pathologies including endothelial dysfunction, plaque rupture, ventricular remodeling and ischemia/reperfusion injury during AMI.6,7 Reactive oxidants can decrease nitric oxide availability in endothelial cells.8,9 Myeloperoxidase (MPO) is a neutrophil and monocyte enzyme that utilizes H2O2 as a co-substrate to generate other reactive oxygen and nitrogen species. 10 MPO and products of protein oxidation generated by hypochlorous acid have also been detected in atheromatous lesions.11–14 High plasma MPO is reported to be a risk factor for early adverse cardiac events in patients with chest pain 15 and ACS 16 and is also associated with endothelial dysfunction.7,17 Recently, it has been reported that plasma MPO is a useful prognostic marker of long-term survival in patients with MI in addition to other markers of cardiac dysfunction (plasma aminoterminal pro-brain natriuretic peptide (NT-proBNP) and left ventricular ejection fraction (LVEF)). 18
In prior studies MPO was particularly useful when combined with troponin testing, but these trials have utilized older, less sensitive troponin assays. The predictive value of MPO may be attenuated when using a higher sensitive troponin assay which may identify more patients at risk who were previously identified by MPO, making MPO less valuable.
This study investigated consecutive patients presenting with chest discomfort to the ED of a university hospital who were subsequently evaluated for suspected ACS. The main aim was to assess the use of MPO combined with a higher sensitive cTnI assay to predict future major cardiac events (MACE) during a 6-week follow-up particularly in sensitive cTnI negative patients.
Materials and methods
Patients
Patients presenting to our ED with its integrated CPU with chest discomfort and suspected ACS were enrolled after written informed consent was obtained. Patients were originally enrolled to develop a multimarker strategy for optimal risk stratification in a low to moderate risk population of the ED. 19 The inclusion was based on the judgement of the attending physician to classify a patient with suspected ACS. Patient management itself was not part of the study protocol but was based on the judgement of the attending physician. Like this, a real life ED situation was exhibited and included patients with non-cardiac chest pain.
The exclusion criteria of the trial were severe anaemia (below 7 g/dL), lack of informed consent and age <18 years.
A medical history and a physical examination as well as an ECG and an initial routine cardiac troponin I (cTnI) measurement on a point-of-care device in the ED were obtained in all patients and therapy initiated in accordance with the German national guidelines.20,21 The final discharge diagnoses from the ED were assessed by a chart review conducted by an experienced physician who was neither involved in the treatment of the patients nor in the data analysis.
All patients were contacted after 42 days by telephone and in case of re-hospitalization the hospital charts were reviewed to determine the occurrence of the primary endpoint of MACE which was defined as cardiovascular death, non-fatal MI, unstable angina pectoris or congestive heart failure requiring admission, urgent unplanned percutaneous intervention (PCI) or coronary artery bypass grafting (CABG). All parts of the study were approved by the appropriate ethics committee (File no. 87/2002).
Biochemical analysis
Admission blood samples (citrate plasma) for MPO and sensitive cTnI were analyzed for all patients included in the study (n=432). Serial samples were available in a subset of n=196 and n=187 patients respectively after 6 hours and again after 12–36 hours, respectively, depending on whether a patient had been discharged at this time point; n=266 patients had two samples at any of these time points and n=117 patients had all three samples taken. MPO and sensitive TnI were tested retrospectively from frozen samples. Upon thawing, samples were centrifuged for clarification prior to testing. Values were corrected for the dilution by citrate.
Analytical variables
Sensitive TnI and MPO concentrations were determined using the ARCHITECT® instrument (Abbott Park, IL, USA). Both assays are two-step monoclonal antibody sandwich immunoassays using chemiluminescent technology. The total precision of the ARCHITECT STAT TnI assay ranged from 2.3 to 5.8% over a concentration range of 0.103 to 13.126 ng/ml. The lower level of detection was determined to be
The upper reference limit (URL) for both assays was determined in a population of 300 apparently healthy hospital employees with no history of coronary artery disease (CAD), prior MI, heart failure or other cardiac, renal or metabolic diseases. The URL for cTnI was 0.018 ng/mL based on the 99th percentile as recommended in the Universal Definition of Myocardial Infarction 3 and an absolute increase of cTnI was used to define AMI. The MPO URL based on the 95th percentile was 193 pmol/L. ROC-analysis (data not shown) resulted in an optimized MPO cut-off of 200 pmol/L. Still, the 95th percentile cut-off was chosen for better comparability with other data-sets and to avoid “over-optimization” of the MPO cut-off potentially resulting in an artificial superiority of MPO compared to the pre-defined and not data-optimized cTnI cut-off by means of better optimization alone.
Statistical analysis
Bivariate associations were all tested by exact binomial tests. For multivariate models (Logistic Regression (LR) and classification and regression tree (CART) dummy variables were calculated based on the following: Estimated Glomerular Filtration Rate (eGFR) was categorized into five groups using the 20% percentiles (cut-offs 70, 87, 95 and 110 mL/min) and age was categorized into four groups with cut-offs of 50, 60 and 70 years. A two-sided α-level of 5% was used for all tests unless indicated otherwise. Sensitivity and specificity maximization (Table 1) for both TnI and MPO were conducted by assessing dichotomies based on observed deciles (10% percentile, 20% percentile, etc.) of the sample distributions and choosing the decile with the best discriminatory power as a cut-off. For TnI the standard cut-off of 0.1 is also displayed.
Sensitivity maximization in unselected ED patients by means of troponin I and MPO.
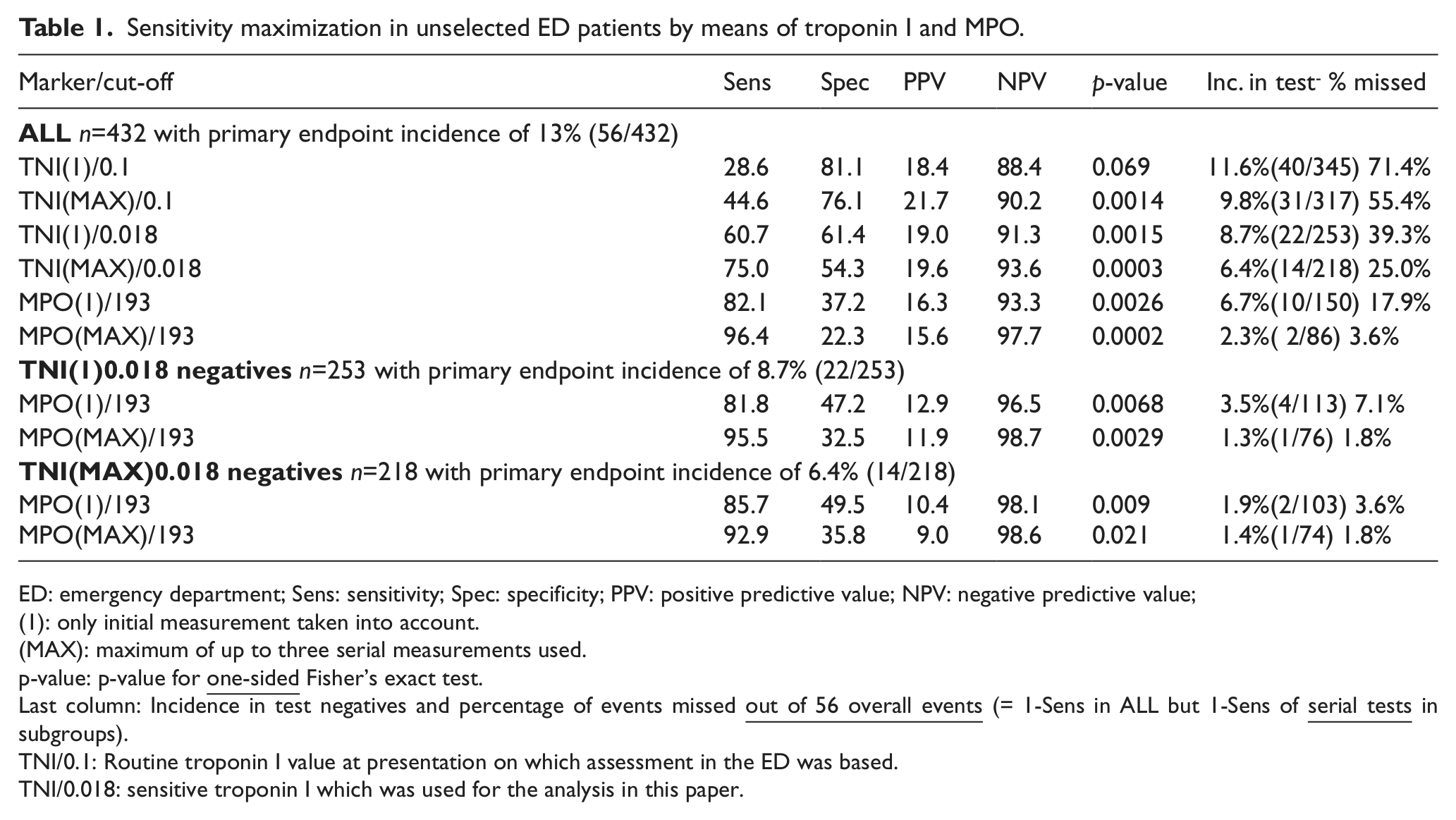
ED: emergency department; Sens: sensitivity; Spec: specificity; PPV: positive predictive value; NPV: negative predictive value;
(1): only initial measurement taken into account. (MAX): maximum of up to three serial measurements used.
p-value: p-value for
Last column: Incidence in test negatives and percentage of events missed
TNI/0.1: Routine troponin I value at presentation on which assessment in the ED was based.
TNI/0.018: sensitive troponin I which was used for the analysis in this paper.
Results
We enrolled 432 consecutive patients within a median of 6.6 hours after onset of chest pain (25%/75% quartiles 2.5 hours/27.4 hours). The baseline characteristics of the entire study group (n=432) and the sensitive cTnI negative subgroups (initial/serial negative; n=253/218) are shown in Table 2.
Characteristics of patients at baseline in the overall study group and in the sensitive troponin negative subgroups (identified by the 99% percentile cut-off (0.018 µg/L) derived from a reference population).
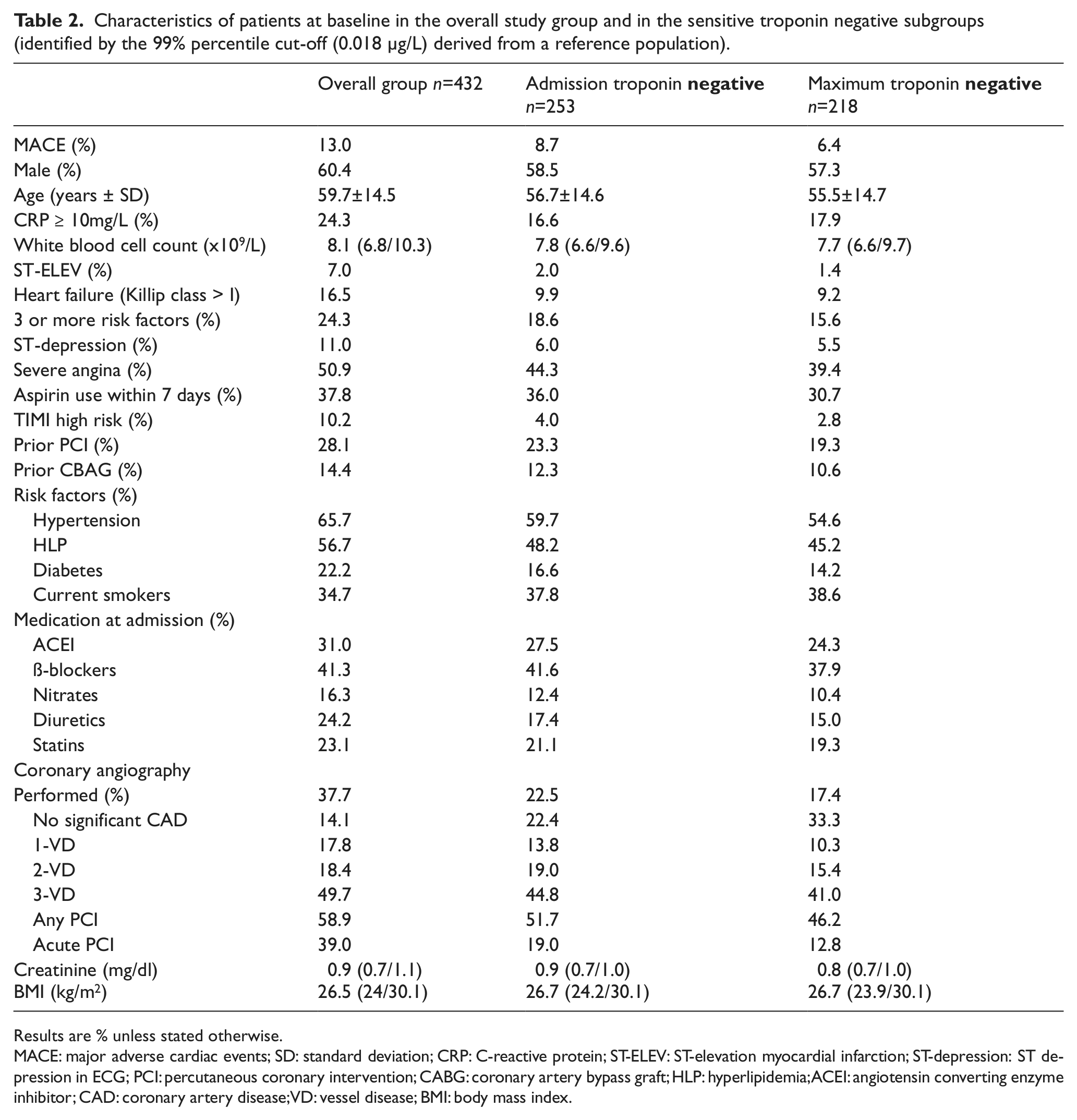
Results are % unless stated otherwise.
MACE: major adverse cardiac events; SD: standard deviation; CRP: C-reactive protein; ST-ELEV: ST-elevation myocardial infarction; ST-depression: ST depression in ECG; PCI: percutaneous coronary intervention; CABG: coronary artery bypass graft; HLP: hyperlipidemia; ACEI: angiotensin converting enzyme inhibitor; CAD: coronary artery disease; VD: vessel disease; BMI: body mass index.
The overall incidence of MACE within 42 days was 13.0% (56/432) for the entire cohort, 8.7% (22/253) in the admission sensitive cTnI negative group and 6.4% (14/218) in the serial sensitive cTnI negative group reflecting a mild to moderate risk population. The 56 MACE events (referring to the first occurring event) were death (seven patients), acute MI (one patient), hospitalization for unstable angina (10 patients) or heart failure (seven patients), PCI (26 patients) and bypass-surgery (five patients). In the admission sensitive cTnI negative patients the 22 MACE events were death (three patients), acute MI (one patient), hospitalizations for unstable angina (five patients) or heart failure (one patient), PCI (nine patients), bypass-surgery (three patients) and in the serial sensitive cTnI negative patients death (two patients), acute MI (no patients), hospitalizations for unstable angina (two patients) or heart failure (one patient), PCI (seven patients) and bypass-surgery (two patients).
Patients who were sent home after clinical judgement by the attending emergency physicians provided only one blood sample and displayed a MACE incidence of 7.8%.
Table 1 summarizes the sensitivity for prediction of MACE events for MPO and sensitive cardiac TnI in the overall group and for MPO in the admission sensitive cTnI negative as well as in serial sensitive cTnI negative group. Sensitivity ranged from 60.7% for the initial cTnI to 96.4% with the maximal MPO value for all patients. In the troponin negative population, either initial or maximum value, the sensitivity for MPO ranged from 81.8 to 95.5%. Also of note is the negative predictive value (NPV) for MPO of 97.7% for all patients and up to 98.7% in sensitive cTnI negative patients.
Figure 1 shows the frequencies of the clinical discharge diagnoses and the frequency of MACE events by diagnosis in patients who were discharged from the decision unit after initial or serial sensitive cTnI negative test results.
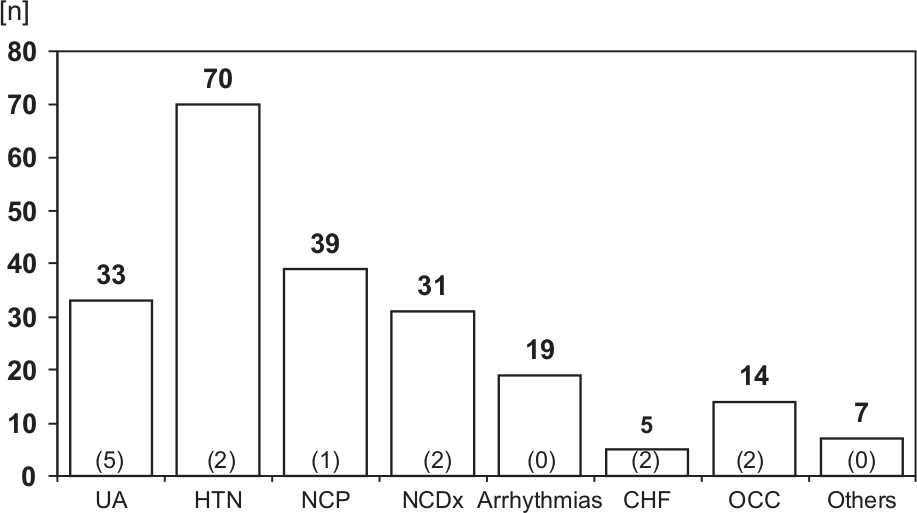
Clinical discharge diagnoses of troponin negative patients.
The five patients who experienced a MACE in the unstable angina group comprise of one patient with CABG after 6 days, three patients with unplanned PCI due to recurrent symptoms at 22, 39 and 42 days and one patient with unstable angina with urgent PCI at 34 days. Two of these patients, both who were re-admitted and received an unplanned PCI, had three blood samples taken at the index hospital stay and remained sensitive cTnI negative throughout.
Table 3 displays results of logistic regression models for predicting MACE in admission sensitive cTnI negative patients using MPO, renal function (as measured by eGFR using the Modification of Diet in Renal Disease (MDRD) formula), gender and age in the assessment. The relevance of MPO for risk stratification in sensitive cTnI negative patients seen in bivariate analyses remains significant (even slightly increased) when adjusted for eGFR, gender and age with an odds ratio (OR) of 4.20.
Logistic regression models on major cardiac events (MACE) during the first 6 weeks.
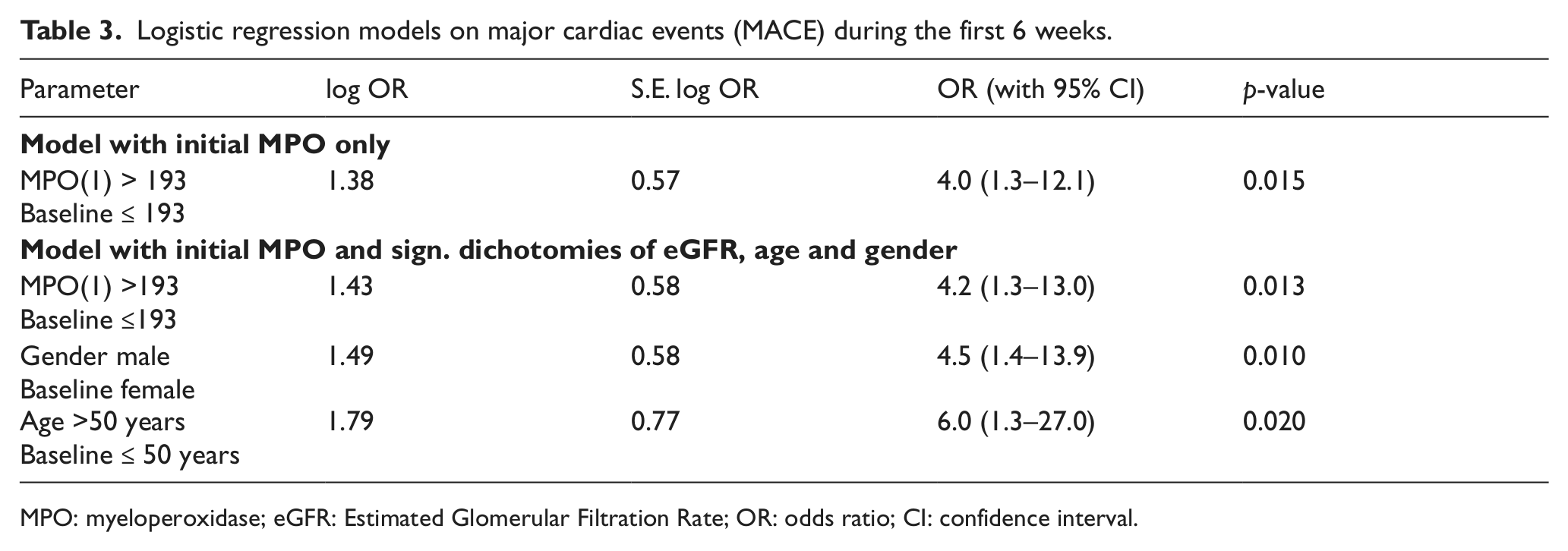
MPO: myeloperoxidase; eGFR: Estimated Glomerular Filtration Rate; OR: odds ratio; CI: confidence interval.
A CART analysis 22 (tree not displayed) also confirms these results: MPO reveals the strongest effect for risk stratification in sensitive cTnI negatives (MACE incidence 8.7%) by splitting this group into MPO negatives with an incidence of 3.6% and MPO positives with an incidence of 12.9%. Further splits are then found for gender and eGFR (with a cut-off of 70mL/min/1.73 m2). The final extreme risk groups (extremely low and extremely high) of this CART analysis are MPO negatives with an eGFR above 70 (1.1% incidence) and male MPO positives with an incidence of 18.3%.
Discussion
In the present study, MPO shows independent discriminatory power in unselected ED troponin positive as well as troponin negative patients using a contemporary sensitive troponin assay.
The multifactorial pathophysiology of chest pain and ACS with its potential complications are an important rationale for measurements of biomarkers related to different underlying pathophysiological aspects in order to optimize early biochemical risk assessment and avoid potential hazardous discharges.
Patients who are evaluated for ACS and sent home after negative results of ECG and troponin testing have an increased risk of cardiovascular events and death. Pope et al. looked at event rates of patients who were mistakenly discharged from the ED with AMI or unstable angina and found a 1.9 times increased risk of death after missed AMI and 5% mortality after missed unstable angina after 30 days. 1
A relevant proportion of patients who have events after a negative evaluation for ACS are those who lack compliance and would therefore benefit from hospital admission. 2 If a biomarker could provide evidence of a high risk of complications the treatment and care of this challenging group of patients would be made easier.
In our study, MPO showed an independent prognostic power in a low to intermediate risk unselected ED patient population. In the sensitive cTnI negative subgroup, 6.4% of the patients had adverse events that occurred within 6 weeks. This number fits into the event rate reported in the literature, 23 especially as our definition of MACE includes more event types than most other trials.
Our results are especially interesting because a sensitive cTnI cut-off, based on the 99th percentile of an independent normal range study, was used. This cut-off (0.018µg/L) is in alignment with the recent Universal Definition of MI 24 and is substantially lower than the recommendation in the package insert (0.1 µg/L). The sensitive cTnI cut-off, which was derived from 300 apparently healthy volunteers, agrees well with previously published data on the sensitivity of the assay used in this study. 25 The higher sensitivity and low cut-off suggest that the independent prognostic power of MPO is not due to the use of an insensitive troponin assay.
A second important aspect is that MPO showed prognostic power when the maximum of up to three available sensitive cTnI measurements were negative. This supports the hypothesis that elevations of MPO, due to its different pathomechanism, add independent information to troponin.
Our results are in line with other reports obtained from studies with higher risk patients. Baldus and colleagues reported that MPO had independent prognostic value in the CAPTURE study where all patients were diagnosed with ACS and underwent coronary angiography. 16
One important unanswered issue in the data discussed above is that the levels of MPO differ largely in the studies. In the paper of Baldus, nearly 10-fold higher values are reported compared to the study of Brennan et al. 15 This is most probably not only due to the differences in the patients studied and assay-related issues 26 but also to pre-analytical factors. We have recently shown that MPO levels in serum and lithium heparin samples increase 27 during the first hours after drawing as an in vitro artefact. As Baldus and colleagues used serum samples the values have increased most probably in the sample. However, since the samples were treated uniformly, it can be argued that the relative levels of MPO, which still showed prognostic values, can still be interpreted in a meaningful way although absolute levels are not comparable to other studies and cut-offs for clinical purposes cannot be derived from this study.
In our study we used citrate samples, from patients as well as from healthy controls, which have been shown to reveal stable MPO values. 27
Our results add to the data published by Brennan et al. 15 The authors showed that MPO was predictive when analysed in a chest pain cohort and was independent of troponin T and C-reactive protein (CRP). The event rate was high in this study although this may be due to the relatively insensitive troponin T-test used as many prevalent MIs may have been overlooked in the initial evaluation. With respect to the pre-analytical issues stressed above, Brennan et al. used lithium heparin samples stored on ice early after drawing and therefore limited in vitro artificial elevations, which can occur with this type of tubes. 27 Again, the uniform treatment of samples guaranteed that the prognostic power could be detected although absolute levels were increased because of pre-analytical factors. 27
On the other hand Eggers et al. recently looked at the prognostic value of MPO in 303 patients with chest pain without ST-segment elevation and only saw non-significantly higher values of MPO in patients who suffered the composite endpoint of death and recurrent AMI within the 6 month follow-up period. They also assessed the long-term outcome after a median of 4.9 years; again MPO levels were only non-significantly higher in patients who died or suffered the composite endpoint during this period. 28
Likewise, McCann et al. assessed a multimarker approach including MPO and saw no predictive value for the long-term outcome (1 year) regarding death and MI. 29 Apple et al., also in a multimarker approach, saw no significant differences in all-cause mortality rates between increased versus normal concentrations of MPO. During the 4-month follow-up period though, MPO concentrations approached statistical significance and significantly added to the prognostic value of TnI. 30
Other studies on MPO again are in line with our results such as in the TACTICS-TIMI 18-study which analyzed the 30-day outcome of ACS patients 31 and a trial by Kahn et al. assessing the 30 day follow-up of STEMI-patients. 32
Our trial assesses the short-term outcome after 42 days. In a longer follow-up period the association to MPO might be weaker, as MPO activity reflects an acute inflammatory state with potential plaque instability. Thus, MPO may be a better predictor of short-term rather than of long-term risk.
In conclusion, potential clinical application of our finding is that MPO may be a tool for further short-term risk stratification in patients who are initially troponin negative. In cases of atypical symptoms, non-diagnostic ECG or other features, MPO results could indicate which patients could be safely discharged home and who should be kept for further evaluation and treatment. Due to the sample issues mentioned in this article and the expected implementation of high sensitive troponin assays in routine clinical practice more clinical research is required before clear recommendations concerning MPO can be given.
Limitations
The present study investigates the prognostic role of MPO in this all-comer, non-selected patient population of the ED. Due to clinical practice at the enrolling hospital, serial sampling only occurred in patients admitted to the hospital, thus only 266 out of 432 patients had at least two blood samples available. Therefore, the role of MPO may be overestimated in this population compared to serial TnI measurements.
The combined primary endpoint MACE was defined to include cardiovascular death, non-fatal MI, unstable angina pectoris or congestive heart failure requiring admission, urgent unplanned percutaneous intervention (PCI) or coronary artery bypass grafting (CABG), which is a wider MACE definition in this prognostic study of unselected patients as opposed to that usually applied in intervention trials.
MPO and sensitive TnI were measured in surplus samples from a trial designed to develop a multimarker strategy for optimal risk stratification 19 in which MPO and the sensitive cTnI assay used for this paper were not included. Analysis therefore depended on the samples and materials initially collected. Finally, we limited the biomarker measurements to TnI as current standard of care, eGFR as a strong prognostic marker in most acute patient populations and MPO as a new candidate biomarker. Other potential biomarkers could have been included; however, due to the limited number of patients enrolled with multiple time-points we think that a multimarker approach would not help here and must be subjected to further, multi-centre trials with larger patient populations.
Another potential limitation in this study is the use of citrate plasma for MPO determinations. While this is not the preferred sample type, data has been published showing the excellent correlation between samples collected in citrate and EDTA collection tubes. 27
Conclusion
MPO has independent prognostic value overall – most notably in troponin negative patients – in this unselected group of ED patients with chest discomfort who were evaluated for ACS using a sensitive TnI assay. MPO should be considered in the initial evaluation of these patients. MPO may lack a high specificity and may also vary widely over the first 24 hours but this study delivers clear evidence that it is advisable to subject MPO positive patients, notably also when TnI negative, to further in-hospital evaluation.
Footnotes
Acknowledgements
We thank Abbott Laboratories for unrestricted research grants.
Conflict of interest
Jessie Shih and Saul Datwyler are employees of Abbott. The other authors have no conflicts of interest to declare.
Funding
This research was funded by unrestricted grants from Abbott Laboratories, Abbott Park, IL, USA.