
Abstract
Aims:
To examine the use of the treatments for acute heart failure (AHF) recommended by ESC guidelines in different clinical presentations and blood pressure groups.
Methods:
The use of intravenous diuretics, nitrates, opioids, inotropes, and vasopressors as well as non-invasive ventilation (NIV) was analysed in 620 patients hospitalized due to AHF. The relation between AHF therapies and clinical presentation, especially systolic blood pressure (SBP) on admission, was also assessed.
Results:
Overall, 76% of patients received i.v. furosemide, 42% nitrates, 29% opioids, 5% inotropes and 7% vasopressors, and 24% of patients were treated with NIV. Furosemide was the most common treatment in all clinical classes and irrespective of SBP on admission. Nitrates were given most often in pulmonary oedema and hypertensive AHF. Overall, only SBP differed significantly between patients with and without the studied treatments. SBP was higher in patients treated with nitrates than in those who were not (156 vs. 141 mmHg, p<0.001). Still, only one-third of patients presenting acute decompensated heart failure and SBP over 120 mmHg were given nitrates. Inotropes and vasopressors were given most frequently in cardiogenic shock and pulmonary oedema, and their use was inversely related to initial SBP (p<0.001). NIV was used only in half of the cardiogenic shock and pulmonary oedema patients.
Conclusions:
The management of AHF differs between ESC clinical classes and the use of i.v. vasoactive therapies is related to the initial SBP. However, there seems to be room for improvement in administration of vasodilators and NIV.
Introduction
Acute heart failure (AHF) is still one of the most common reasons for hospitalizations in Western countries and most importantly associated with substantially increased mortality.1–3 Management of AHF is challenging given the heterogeneous clinical manifestations that vary from cardiogenic shock with extremely poor prognosis to less severe manifestations such as hypertensive AHF. 4
Since year 2005, ESC has published guidelines for diagnosis and management of AHF.5–7 The recommended therapies include vasodilators, diuretics, opioids, inotropes, vasopressors, and non-invasive ventilation (NIV). The evidence for beneficial effect on mortality of these treatments is mostly lacking but it has been increasingly recognized that vasodilators and diuretics are useful at least in terms of relieving symptoms. In contrast, the use of inotropes and vasopressors has been associated even with increased mortality8–10 and their recommended use is limited to hypotensive and/or hypoperfused patients.5–7 In addition, several studies have shown that higher initial systolic blood pressure (SBP) is associated with lower mortality in AHF.2,3,11,12
Data on the actual use of the treatments recommended by ESC guidelines are limited. We assessed the administration of these therapies in different clinical classes of AHF and evaluated differences in clinical presentation in relation to the administration of the treatments. Moreover, we investigated the relationship between initial SBP and the use of intravenous therapies.
Methods
All consecutive patients hospitalized due to AHF were enrolled at 14 hospitals at the FINN-AKVA study between February and May 2004. 2 Patients with new-onset (de-novo) HF as well as with worsening of chronic heart failure (CHF) were included and enrolled only once during the study period. Patients were classified according to the ESC 2005 AHF guidelines criteria 5 to five groups on the basis of their clinical presentation on admission:
(1) cardiogenic shock (CS): evidence of tissue hypoperfusion (e.g. oliguria) and low blood pressure (SBP <90 mmHg or need of vasopressors to uphold perfusion) caused by heart failure after correction of preload
(2) pulmonary oedema (PO): acute heart failure with severe respiratory distress, crackles on lung auscultation, and pulmonary oedema on chest X-ray, usually with O2 saturation <90% on room air.
(3) acute decompensated heart failure (ADHF): signs and symptoms of acute heart failure that do not fulfil the criteria of hypertensive crisis, pulmonary oedema, or cardiogenic shock
(4) hypertensive AHF: signs and symptoms of acute heart failure accompanied by high blood pressure (>160 mmHg) and a relatively preserved left ventricular function (LVEF >40%) with congestion or pulmonary oedema on chest radiograph
(5) right heart failure: acute heart failure predominantly due to right ventricular failure; signs and symptoms of decreased cardiac output, distension of jugular vein, enlarged liver, and severe oedema.
Patients with high-output heart failure were not included. Anthropometric measures, underlying diseases, precipitating factors, clinical presentation, and in-hospital treatments were recorded by local research fellows. At discharge, the diagnosis of heart failure had to be confirmed for final inclusion in the study. All patients gave written informed consent. The study was approved by the Ethics Committee of the Department of Medicine at Helsinki University Central Hospital and conducted in accordance with the declaration of Helsinki.
We examined the use of AHF therapies recommended by ESC guidelines. The administration of intravenous nitrates, furosemide, opioids, inotropes (dobutamine and levosimendan), and vasopressors (adrenaline, noradrenaline, and dopamine) as well as the use of NIV was assessed in a total of 620 patients. Initial treatment within 48 hours from admission was included in this analysis. More specifically data concerning the use of nitrates, furosemide, and opioids was collected only within the first 12 hours from admission. We compared use of the therapies between the clinical classes and also between patients with de-novo AHF and those with acute worsening of CHF. Differences in clinical presentation, comorbidities, precipitating factors, and biochemistry were analysed in patients receiving and those not receiving the treatments.
Furthermore, we examined the use of these treatments in relation to SBP on admission (<120, 120–160, and >160 mmHg) in the two major clinical classes, ADHF (n=394) and PO (n=163).
Statistical analyses were performed using PASW 18 statistical software (SPSS). Chi-squared test was used to compare categorical variables and t-test and Mann–Whitney U-test were used for continuous variables. The results are given as mean±standard deviation, median (interquartile range), or percentages, as appropriate. Determinants of the therapies administered were identified through multivariate logistic regression. Variables included in the multivariate model: age (per 1 year increase), gender, CHF, coronary artery disease, hypertension, cerebrovascular disease, diabetes, acute coronary syndrome (ACS), atrial fibrillation/flutter, valvular disease, pneumonia, SBP, and estimated glomerular filtration rate (calculated using the CKD-EPI equation). A p-value <0.05 was considered statistically significant.
Results
Patient characteristics
The FINN-AKVA study included a total of 620 patients with mean age of 75±10 years, and 307 (49.5%) were women. ADHF was the most common clinical manifestation (63.5%) whereas 26.3% of patients had PO, 2.3% CS, 3.1% hypertensive HF, and 4.8% right heart failure. Patients with de-novo AHF had higher systolic blood pressure (151±33 vs. 144±33 mmHg, p<0.013), diastolic blood pressure (86±21 vs. 78±18 mmHg, p<0.001), and heart rate (96±28 vs. 87±25 bpm, p<0.001) compared with patients with acute worsening of CHF. In addition, patients with de-novo AHF had more often ACS and atrial arrhythmias as precipitating factors (40 vs. 24%, p<0.001; 34 vs. 25%, p=0.009). Table 1 describes patient characteristics in different clinical groups. A detailed description of the study population has been published previously. 4
Study population and characteristics in different clinical classes.
Values are mean±standard deviation, %, or median (interquartile range).
ADHF, acute decompensated heart failure; AHF, acute heart failure; CS, cardiogenic shock; PO, pulmonary oedema; right HF, right heart failure.
ACE-i, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; CRP, C-reactive protein; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate (calculated using the CKD-EPI equation); NT-proBNP, N-terminal pro-B-type natriuretic peptide; SBP, systolic blood pressure.
The use of therapies in different clinical conditions
Overall, 76% of patients received i.v. furosemide, 42% nitrates, 29% opioids, 5% inotropes, and 7% vasopressors (Table 2). In addition, 24% of patients were treated with NIV, of which the majority (148/150) was continuous positive airway pressure with face mask. Invasive ventilation was used in 4% of patients. As shown in Table 2, furosemide was the most common treatment irrespective of clinical class and the use ranged from 69% in ADHF to 93% in PO. The use of nitrates was frequent in PO and hypertensive AHF but they were administered to less than one-third of patients with ADHF. With regard to inotropes and vasopressors, they were used the most often in CS but also given to a proportion of PO patients. Only about half of PO and CS patients were treated with NIV.
The use of treatments in different clinical classes, de-novo acute heart failure and acute worsening of chronic heart failure.

Values are %. p-values are for comparison between awCHF and de-novo AHF groups.
ADHF, acute decompensated heart failure; awCHF, acute worsening of chronic heart failure; AHF, acute heart failure; CS, cardiogenic shock; PO, pulmonary oedema; right HF, right heart failure.
NIV, non-invasive ventilation.
Patients with de-novo AHF received significantly more often opioids and vasopressors than those with acute worsening of CHF, with a similar trend seen with nitrates. However, furosemide was given more frequently in acute worsening of CHF compared with de-novo AHF.
Clinical presentation, systolic blood pressure, and the use of i.v. therapies
Apart from SBP on admission, the differences in clinical presentation were scarce between patients treated and those not treated with the therapies studied. With the exception of furosemide, the use of i.v. medications was strongly related to SBP on admission. Patients treated with nitrates had higher SBP than those not treated (156±36 vs. 141±29 mmHg, p<0.001) and a similar observation was made for patients who received opioids or were treated with NIV. Conversely, SBP was lower among patients given inotropes (120±25 vs. 149±33 mmHg, p<0.001) and vasopressors (120±31 vs. 150±33 mmHg, p<0.001) than among those who did not receive these therapies.
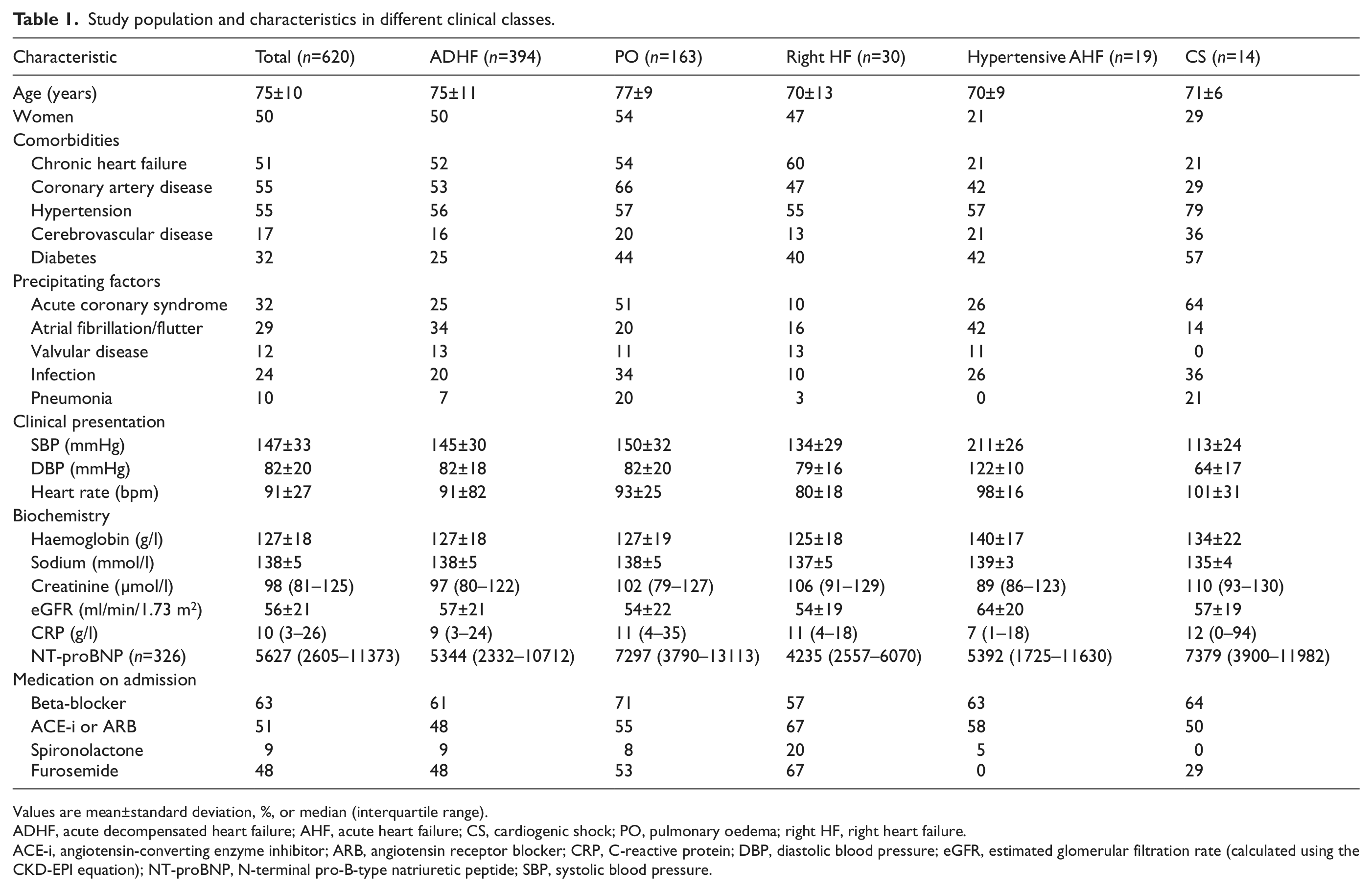
In ADHF and PO groups, there was a similar relationship between initial SBP and the use of nitrates, inotropes and vasopressors as in the overall study population (p<0.05 for all). However, only half of ADHF patients with initial SBP >160 mmHg and even fewer of those with SBP 120–160 mmHg received nitrates (Figure 1a). The use of nitrates in PO was higher, with up to 68% of patients with SBP 120–160 mmHg treated with nitrates (Figure 1b). In contrast, 14% of PO patients received inotropes and 8% vasopressors even though the mean SBP on admission among these patients was as high as 130±26 and 134±37 mmHg, respectively.
Administration of intravenous therapies in relation to systolic blood pressure in acute decompensated heart failure (a) and pulmonary oedema (b).
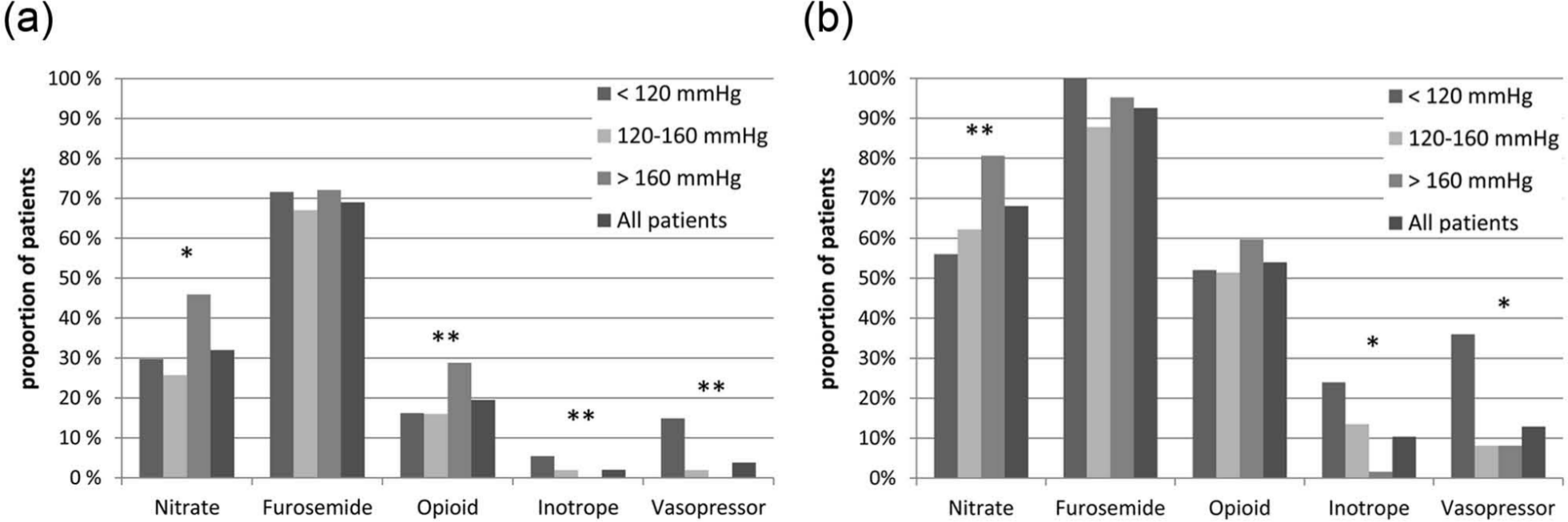
The use of therapies in de-novo AHF and acute worsening of CHF in relation to SBP is shown in Figure 2. In the group with <120 mmHg, vasoactive medications were used more than twice as often in de-novo AHF compared with acute worsening of CHF. In higher SBP groups, there were no significant differences in the administration of i.v. medications.
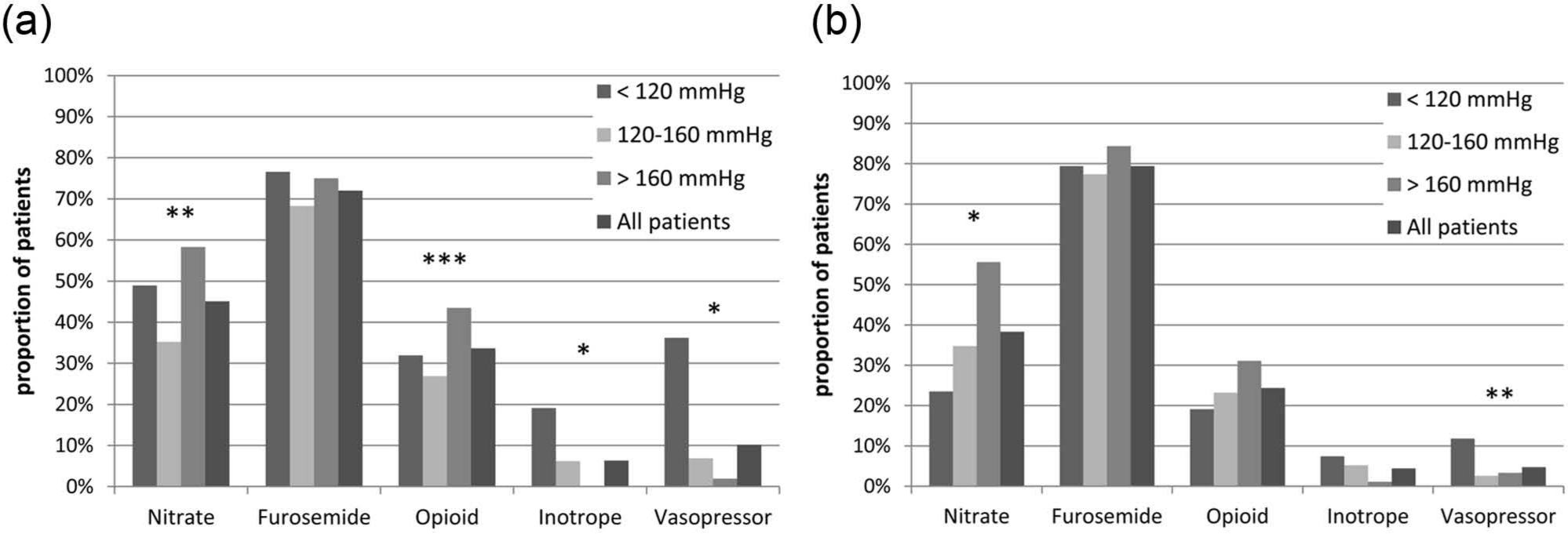
Administration of intravenous therapies in relation to systolic blood pressure in de-novo acute heart failure (a) and acute worsening of chronic heart failure (b).
In multivariate regression analysis of the entire study population, initial SBP was independently associated with the use of NIV and all i.v. medications except furosemide. Of the precipitating factors, ACS and pneumonia were major determinants of the use of these therapies. In fact, ACS was independently associated with the use of all studied treatments. In particular, patients who were treated with nitrates more frequently had ACS compared with those who were not treated (53 vs. 17%; p<0.001).
Discussion
This study examines the initial treatment of AHF in relation to different clinical presentations and SBP on admission. As expected, the use of i.v. therapies and NIV differs between different clinical classes. Nevertheless, differences in characteristics at presentation between patients receiving and those not receiving the treatments were few with only clinically relevant differences seen only in SBP. This strong relationship between admission SBP and various i.v. medications has not been previously described. Furthermore, we found that i.v. nitrates were used in less than half of the patients with AHF despite normal–high SBP (>120 mmHg) at presentation while some PO patients with similar SBP still received inotropes and vasopressor therapy.
Therapies in clinical classes
In line with previous studies, the most common treatment was i.v. furosemide.3,13–16 Indeed, it plays a central role in relieving congestion and symptoms even though the effect on mortality has not been shown. 17 The choice between i.v. and oral route of administration may be subject to physician preference, the perceived severity of patients’ clinical condition, and also local practices. Therefore, use of furosemide varies in different studies, ranging from 84 to 98%.3,13–16 However, the use of oral furosemide was not included in the present analysis.
The use of i.v. nitrates seems to be less clearly established and there are regional differences. 13 In the present study, a similar proportion of patients received i.v. nitrates as in previous studies,12,14,15 more frequently in PO than in ADHF. The use of nitrates in oral or sublingual form is more common in the USA than in Europe. This may explain why the use of i.v. vasodilators was less common in ADHERE 16 than in present study. Nevertheless, considering available data18–20 and recommendations in recent guidelines,5–7,21,22 we find the use of i.v. nitrates rather low in the overall population as well as in ADHF and PO patients. Thus, it seems reasonable to recommend that vasodilators should be used more frequently.
When interpreting the use of vasopressors and inotropes, it is important to consider the proportion of patients with cardiogenic shock or hypotension, which was lower in the present study than in the recently published ALARM-HF. 15 Certain inclusion criteria in some previous studies (such as need for i.v. medication or admission to cardiac or intensive care) also affect patient characteristics and treatments, (i.e. use of vasopressors and inotropes) accordingly.3,10
Surprisingly, only a half of CS and PO patients were treated with NIV. Still, the use of NIV was considerably more common than in other studies.3,12,14 This is probably more related to local practices than explained by a difference in the patient population between the studies. Indeed, continuous positive airway pressure therapy has been included in the Finnish national recommendations for years. While the impact of NIV on mortality is controversial, it has been demonstrated to relieve symptoms and reduce the need for intubation and thus might be used more actively.23,24
Admission SBP and the use of i.v. therapies
The use of nitrates, inotropes, and vasopressors was related to SBP on admission in this study. Initial SBP may guide the administration of i.v. medications in clinical practice. Indeed, apart from furosemide, SBP was an independent determinant of the use of studied therapies.
Although the mean SBP was rather high among patients receiving nitrates, it was surprisingly high among patients not receiving nitrates as well. While administered more often to patients with higher SBP, nitrates were given only to a minority of patients with SBP 120–160 mmHg. Thus, low SBP does not explain why nitrates were not used more frequently. Available data suggest mortality benefit even with lower SBP (<120 mmHg).19,20
In contrast to the rather low use of nitrates, there might be some overuse of inotropes and vasopressors since the mean SBP was relatively high, especially among PO patients who received these drugs. Since it is increasingly recognized that the use of inotropes and vasopressors is associated with adverse events and potential harm,8–10 their use should be restricted to patients with hypotension and signs of hypoperfusion due to low cardiac output.5–7
ACS and other determinants
ACS was found to be an independent predictor of the studied AHF treatments. Theoretically, the clinical use of i.v. nitrates and opioids may be better implemented in treating ischaemia and chest pain in ACS than congestion and dyspnoea in AHF. This might explain why nitrates and opioids were used more often in de-novo AHF than in acute worsening of CHF. At the same time, the use of inotropes/vasopressors may be particularly harmful in AHF patients with ACS25,26 and their use should be restricted to patients in cardiogenic shock.
Of note, ACS seemed to lead to more frequent use of furosemide as well. Especially in the setting of de-novo AHF ACS is not likely associated with fluid retention. Pneumonia was also found to be a significant factor for the use of nitrates, furosemide, vasopressors, opioids and NIV. Haemodynamic instability and respiratory distress may be more severe in AHF precipitated by pneumonia and the clinical picture warrants the need for ventilatory support.
Limitations
Some limitations in this study have to be acknowledged. First, the time frame of this analysis was limited to the first 48 hours of hospitalization. All analyses are based on clinical class and SBP determined at presentation. Consequently, changes in blood pressure or clinical picture warranting re-evaluation of therapies early in-hospital are not accounted for. However we feel that the length of this period reflects the initial phase of management adequately. Second, the results in CS, hypertensive AHF, and right heart failure should be interpreted cautiously due to small number of patients. Third, the diagnosis of ACS and pneumonia were based on the clinical judgement of local investigators and no centralized adjudication was performed. In any case, the strength of our study is the unselected population of patients reflecting real-life clinical practice.
Conclusion
The initial management of AHF differs between the ESC clinical classes. Apart from SBP on admission, the differences in clinical presentation between patients who received and those who did not receive therapies were scarce. Initial SBP and ACS as a precipitating factor were major determinants of given therapies. Nevertheless, there seems to be room for improvement in administration of guideline recommended therapies for AHF. Efforts should be made to increase the use of vasodilators and NIV, whereas the use of inotropes and vasopressors should be avoided in patients not being hypotensive or in cardiogenic shock.
Footnotes
Appendix
The FINN-AKVA study group comprises
V-P Harjola, K Siirilä-Waris, MS Nieminen, Helsinki University Central Hospital; J Melin, Central Finland Central Hospital; K Peuhkurinen, Kuopio University Hospital; M Halkosaari, Keski-Pohjanmaa Central Hospital; K Hänninen, Kymenlaakso Central Hospital; T Ilva, T Talvensaari, Kanta-Häme Central Hospital; H Kervinen, Hyvinkää Hospital; K Kiilavuori, Jorvi Hospital; K Majamaa-Voltti, Oulu University Hospital; H Mäkynen, V Virtanen, Tampere University Hospital; T Salmela-Mattila, Rauma Hospital; K Soininen, Kuusankoski Hospital; M Strandberg, H Ukkonen, Turku University Hospital; I Vehmanen, Turku Hospital; E-P Sandell, Espoo, Finland. The study nurses are K Hautakoski, Keski-Pohjanmaa Central Hospital; J Lamminen, Hyvinkää Hospital; M-L Niskanen, Kuopio University Hospital; M Pietilä, Helsinki University Central Hospital; O Surakka, Central Finland Central Hospital.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The FINN-AKVA study was supported by grants from Paulo Foundation, the Finnish Foundation for Cardiovascular Research and an unrestricted grant from Orion Pharma.