
Abstract
Aims:
Little is known regarding consequences of frailty in patients with acute coronary syndrome (ACS). We assessed the associations of frailty and outcomes in ACS patients who were participating in a clinical trial.
Methods and results:
The TaRgeted platelet Inhibition to cLarify the Optimal strateGy to medicallY manage Acute Coronary Syndromes (TRILOGY ACS) trial randomized 9326 patients planned for medical management to prasugrel or clopidogrel. The primary endpoint was a composite of cardiovascular death, myocardial infarction (MI), or stroke over a period of 30 months. A frailty score based upon the Fried score was self-reported at baseline in patients aged ⩾65 years. Five frailty questions were recorded for 4996/5102 (97.9%) patients: 72.3% were classified as not-frail (0 items), 23.0% as pre-frail (1–2 items), and 4.7% as frail (⩾3 items). Increasing frailty score was associated with older age, diabetes, and higher Global Registry of Acute Coronary Events (GRACE) scores. Frailty was associated with a higher unadjusted incidence of the primary endpoint (pre-frail vs not-frail: 29.2% vs 23.1%; hazard ratio [HR]: 1.39; 95% confidence interval [CI]: 1.19–1.61; p<0.001; frail vs not-frail: 39.7% vs 23.1%; HR: 1.76; 95% CI: 1.36–2.28; p<0.001), and all-cause mortality (pre-frail vs not-frail: 21.7% vs 15.0%; HR: 1.45; 95% CI: 1.22–1.73; p<0.001; frail vs not-frail: 30.2% vs 15.0%; HR: 1.98; 95% CI: 1.47–2.68; p<0.001). After adjustment for baseline characteristics and GRACE covariates, frailty remained independently associated with the primary endpoint: pre-frail vs not-frail, HR: 1.33; 95% CI: 1.15–1.54; p<0.001; frail vs not-frail, HR: 1.52; 95% CI: 1.18–1.98; p=0.002. There was no association of frailty with bleeding.
Conclusion:
Frailty is associated with the composite of cardiovascular death, MI, or stroke. Frailty assessment contributes to risk prediction and adds to the GRACE score.
Introduction
Frailty is a well-established concept reflecting a state of weakened resistance to stressors and diminished physiologic reserve.1–3 Primarily noted among older adults, it can be assessed by a variety of methods that determine limitations along key domains defining the frail phenotype: slowness, weakness, low physical activity level, exhaustion, and shrinking. 4 Frailty has been shown to be associated with adverse outcomes in cardiovascular populations, including after transcatheter aortic valve replacement,5–11 in patients admitted to a coronary care unit, 12 in patients undergoing coronary artery bypass grafting (CABG) surgery,13–17 and in patients undergoing percutaneous coronary intervention (PCI), all in relatively modest sample sizes.18,19 Slow gait speed as a measure of frailty has also been shown to be associated with an increased risk of cardiovascular events in patients after ST-segment-elevation myocardial infarction (STEMI) and PCI after adjustment for the Framingham risk score and B-type natriuretic peptide (BNP) measurements. 20
Less is known about frailty and non-ST-segment elevation acute coronary syndrome (NSTEACS). In several small registries (one that examined 307 patients aged ⩾75 years with non-ST-segment elevation myocardial infarction [NSTEMI] and another in 342 patients with ACS) frailty has been associated with adverse clinical outcomes including mortality.21,22 In particular, there is no information about the effectiveness and safety of P2Y12 antagonists in ACS and frailty; moreover, the assessment of frailty, especially if it requires performance assessments (e.g. gait speed and grip strength), poses additional complexities in the setting of an international clinical trial. We therefore explored the relationship of frailty, as assessed at baseline by self-report in a clinical trial of planned medical management, to ischemic and bleeding risk in the TaRgeted platelet Inhibition to cLarify the Optimal strateGy to medicallY manage Acute Coronary Syndromes (TRILOGY ACS) trial.23,24 We also evaluated whether frailty added to the guideline-recommended and frequently used Global Registry of Acute Coronary Events (GRACE) score,25–28 which has also been shown to be the most accurate risk score.29,30
Methods
Study protocol and treatment
The study design and results of the TRILOGY ACS trial have been described previously.23,24 TRILOGY ACS was a double-blind, active-controlled, randomized trial in high-risk patients with unstable angina (UA)/NSTEMI who were managed medically without planned revascularization (ClinicalTrials.gov identifier: NCT00699998). Participants had at least one of four enrichment criteria: age ⩾60 years, diabetes mellitus, prior MI, or prior coronary revascularization at least 30 days before the index ACS hospitalization. Patients with a history of transient ischemic attack/stroke, PCI or bypass grafting within the previous 30 days, renal failure requiring dialysis, or concomitant oral anticoagulant treatment were excluded.
The pre-specified primary analysis cohort included 7243 patients aged <75 years who received prasugrel 10 mg/day (if body weight was ⩾60 kg) or prasugrel 5 mg/day (if weight was <60 kg) vs clopidogrel 75 mg/day. 23 For this analysis, we also included 2083 patients aged ⩾75 years who were randomized to prasugrel 5 mg/day vs clopidogrel 75 mg/day, for a total of 9326 patients from 52 countries.23,24,31
Randomization was stratified by treatment status with clopidogrel for the index event before randomization (no pre-randomization clopidogrel treatment; clopidogrel treatment started in-hospital for the index UA/NSTEMI event and continued until day of randomization; and home clopidogrel treatment continued until day of randomization). From June 2008–September 2011, 9326 participants were enrolled and were followed for a median of 17.1 (10.4–24.4) months. 23
All participants randomized to prasugrel or clopidogrel received concomitant aspirin treatment, with ⩽100 mg/day recommended. Study treatments were administered for a minimum of six months; maximum duration of treatment was 30 months for all patients regardless of age. There was no effect of prasugrel on the primary endpoint, and similar risks of major bleeding were observed with prasugrel and clopidogrel. 23
The TRILOGY ACS study was approved by regulatory authorities in all participating countries and by participating sites’ institutional review boards. All participants provided written informed consent. The TRILOGY ACS study was supported by Daiichi Sankyo, Inc. and Eli Lilly and Company. The study sponsors had no role in the design or conception of the present study. All statistical analyses were performed independently by the Canadian VIGOUR Centre (Edmonton, Alberta, Canada) and the Duke Clinical Research Institute (Durham, North Carolina, USA).
Frailty assessment
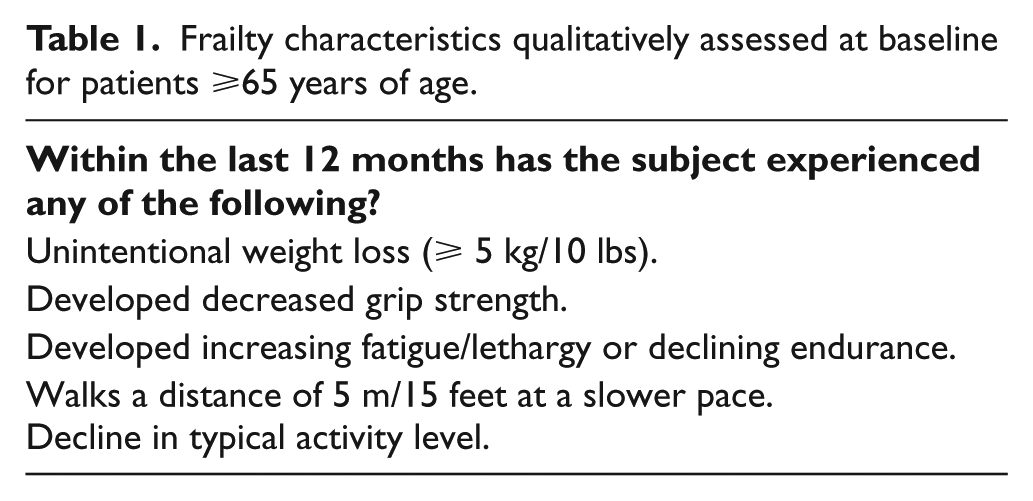
The questions patterned from the Fried Frailty score domains 4 were assessed at baseline in patients aged ⩾65 years as self-reported to the research investigator and responses were entered into the database. The questions address five domains of the frailty phenotype: (a) shrinking (weight loss of ⩾10 pounds in the prior year); (b) weakness (decreased or weakened grip strength); (c) exhaustion (fatigue or declining endurance); (d) slowness (slower walking pace); and (e) low activity (decline in physical activity). The questions are listed in Table 1.
Frailty characteristics qualitatively assessed at baseline for patients ⩾65 years of age.
Statistical methods
Baseline patient characteristics were examined according to frailty score with the following pre-specified groups: not frail (0 items); pre-frail (1–2 items); and frail (⩾3 items). Continuous variables are reported as medians (25th, 75th percentiles) and differences were compared using the Kruskal-Wallis test, whereas discrete variables are reported as counts (percentages) and differences were compared using the Pearson χ2 test. The association between frailty score and time to study drug discontinuation was also assessed.
Ischemic efficacy endpoints included the primary efficacy composite of cardiovascular death, MI, or stroke; the individual components of the composite; and all-cause death. All efficacy analyses were performed on the intention-to-treat population that included all randomized patients (n=4996/9326 [53.6%]). Bleeding endpoints (bleeding unrelated to CABG by Global Use of Strategies to Open Occluded Coronary Arteries [GUSTO] and Thrombolysis in Myocardial Infarction [TIMI] criteria) included GUSTO severe/life-threatening (±moderate) bleeding and TIMI major (±minor) bleeding and were evaluated among patients who received at least one dose of study drug during the “at-risk” period of study drug treatment, through 7 days after study drug discontinuation (n=4940/9240 [53.5%]).
Associations were assessed between self-reported frailty and ischemic and bleeding outcomes through 30 months after randomization using Cox proportional hazards regression. Event rates within each frailty group are presented as the total number of events and as Kaplan-Meier event rate estimates at 30 months after randomization with 95% confidence intervals (CIs). The log-rank test was used to test for differences among frailty groups. When examining relative associations, adjustment for baseline patient characteristics was performed in two manners: (a) covariates (age, heart rate, systolic blood pressure, Killip class, diuretic use, creatinine, renal failure, ST-segment deviation, elevated troponin, cardiac arrest at admission) from an established ACS risk tool (the GRACE risk prediction model for six-month mortality), 25 and (b) the TRILOGY ACS risk adjustment models for the ischemic and bleeding events, which were developed and validated in the overall TRILOGY ACS trial cohort (see Supplementary Material, Appendix 1).
To examine whether self-reported frailty modulated the study treatment association with these outcomes, the two-way interaction between frailty and randomized study treatment was tested. Results are reported by an adjusted hazard ratio (HR) and 95% CIs with the not-frail group serving as the reference group. All statistical tests were two-sided and the level of statistical significance was p<0.05; all analyses were performed using SAS (version 9.3; Cary, North Carolina, USA).
Results
Baseline characteristics and medications
Frailty scores were obtained on 4996/5102 (97.9%) of patients aged ⩾65 years. As patients younger than age 65 years are unlikely to have physiologic frailty, these measures were only collected in the older cohort: 72.3% (n=3612) of patients were classified as not frail, 23.0% as pre-frail (1–2 items), and 4.7% as frail (⩾3 items). Table 2 shows the number of patients who reported each frailty characteristic from among those who reported any frailty characteristic (n=1384) (categories not mutually exclusive). The most commonly reported characteristics were decline in physical activity (70.4%), fatigue or declining endurance (37.8%), and slower pace (35.3%).
Frailty characteristics among patients ⩾65 years of age.
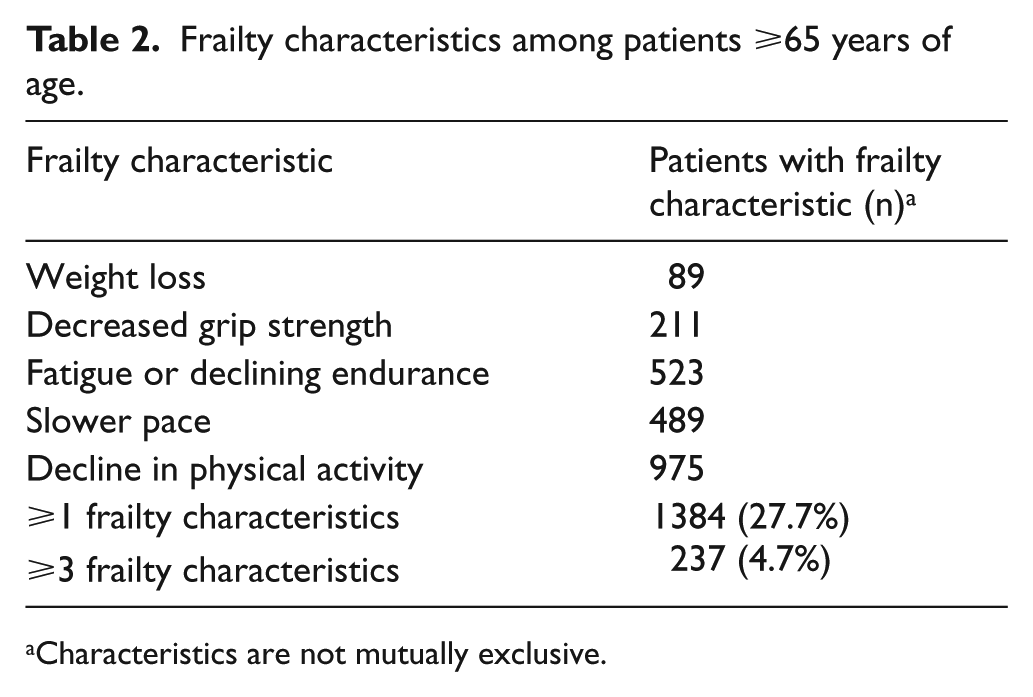
Characteristics are not mutually exclusive.
Table 3 shows the baseline patient characteristics for the three frailty groups. Increasing frailty scores were correlated with an increasing gradient for most risk factors: older age, diabetes mellitus, prior history of MI, prior heart failure, previous revascularization and higher GRACE risk scores (all p<0.001). There was lower use of angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) (p<0.001) as well as statins (p=0.011) and proton-pump inhibitors (p=0.009) in pre-frail and frail patients vs not-frail patients. The percentage of patients undergoing pre-randomization angiography did not differ across frailty groups (p=0.177). Angiography was performed in 26/237 frail patients (11.0%) during follow-up in comparison to 104/1147 pre-frail patients (9.1%) and 318/3612 not-frail patients (8.8%) (p=0.523).
Baseline characteristics among patients ⩾65 years of age according to frailty status.
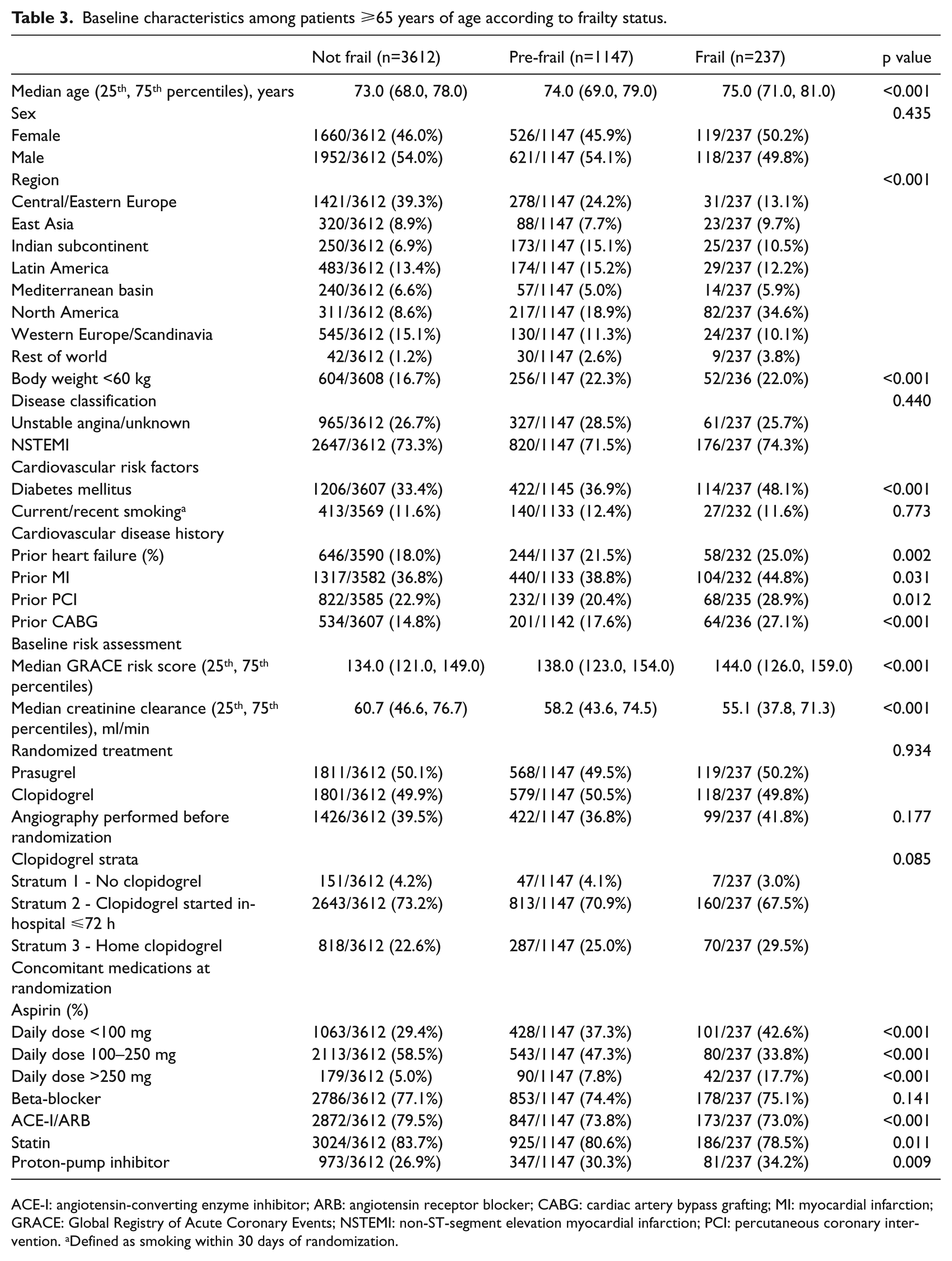
ACE-I: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; CABG: cardiac artery bypass grafting; MI: myocardial infarction; GRACE: Global Registry of Acute Coronary Events; NSTEMI: non-ST-segment elevation myocardial infarction; PCI: percutaneous coronary intervention. aDefined as smoking within 30 days of randomization.
Discontinuation of treatments
A total of 1352 patients ⩾65 years of age (27.4%) permanently discontinued randomized treatment. The discontinuation rate was similar for frail and pre-frail groups (31.1% vs 29.2%), but higher than that of not-frail patients (26.1%; p=0.003).
Relationship of frailty with ischemic outcomes
Frail patients experienced a higher unadjusted estimate of the likelihood of cardiovascular death, MI, or stroke events compared with not-frail patients (39.7% vs 23.1%; HR: 1.76; 95% CI: 1.36–2.28; p<0.001). Similar results were observed for frequency of cardiovascular death, MI, or stroke events for the pre-frail vs not-frail comparison (29.2% vs 23.1%; HR: 1.39; 95% CI: 1.19–1.61; p<0.001) (Figure 1). Among frail patients, nearly 40% had a cardiovascular event over 30 months of follow-up and one in four experienced cardiovascular death. Figures 2(a)–2(c) show the Kaplan-Meier survival estimates according to frailty group for each component of the primary composite endpoint.
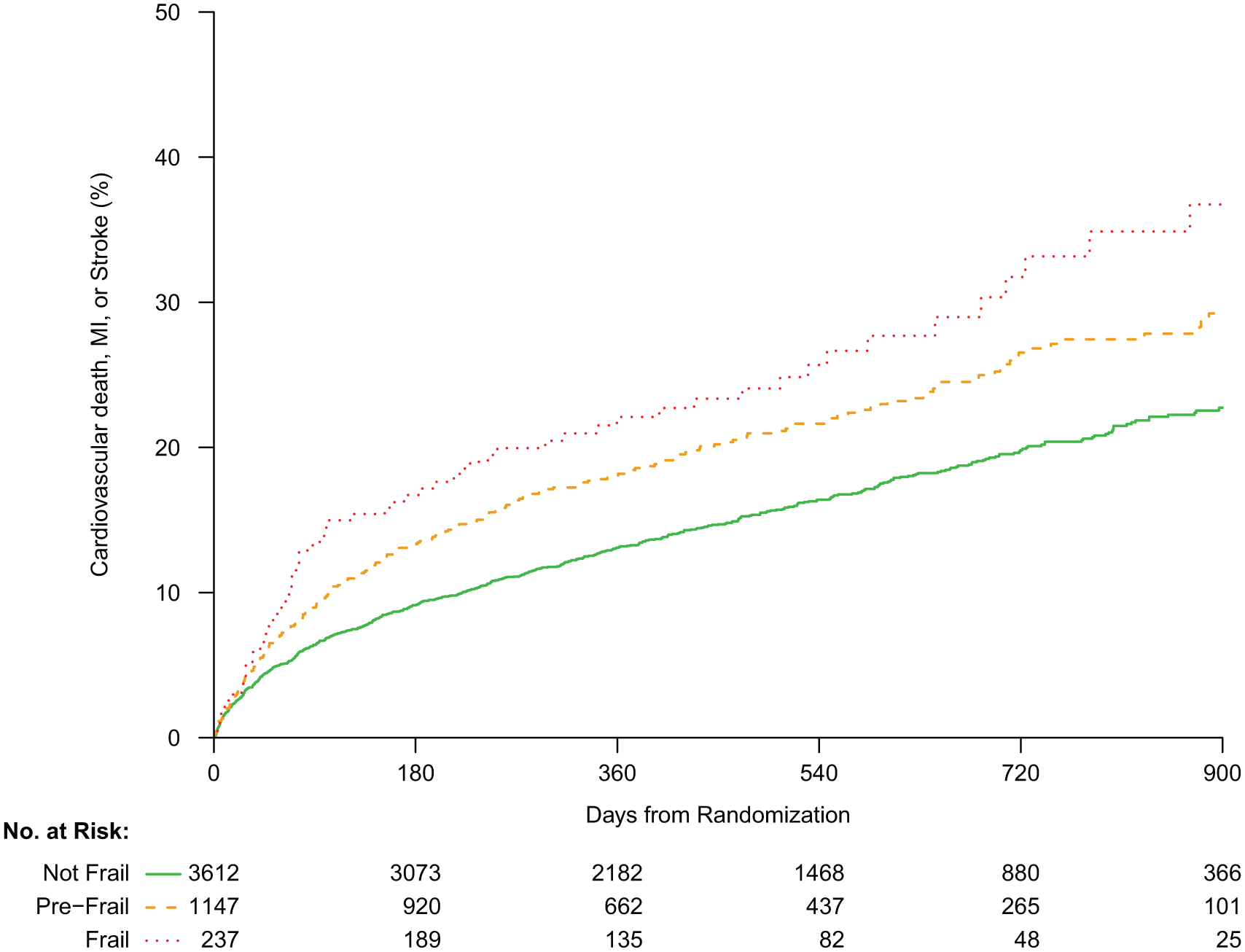
Kaplan-Meier survival curves for the composite of cardiovascular death, myocardial infarction (MI), or stroke according to frailty status (reference group: not frail).
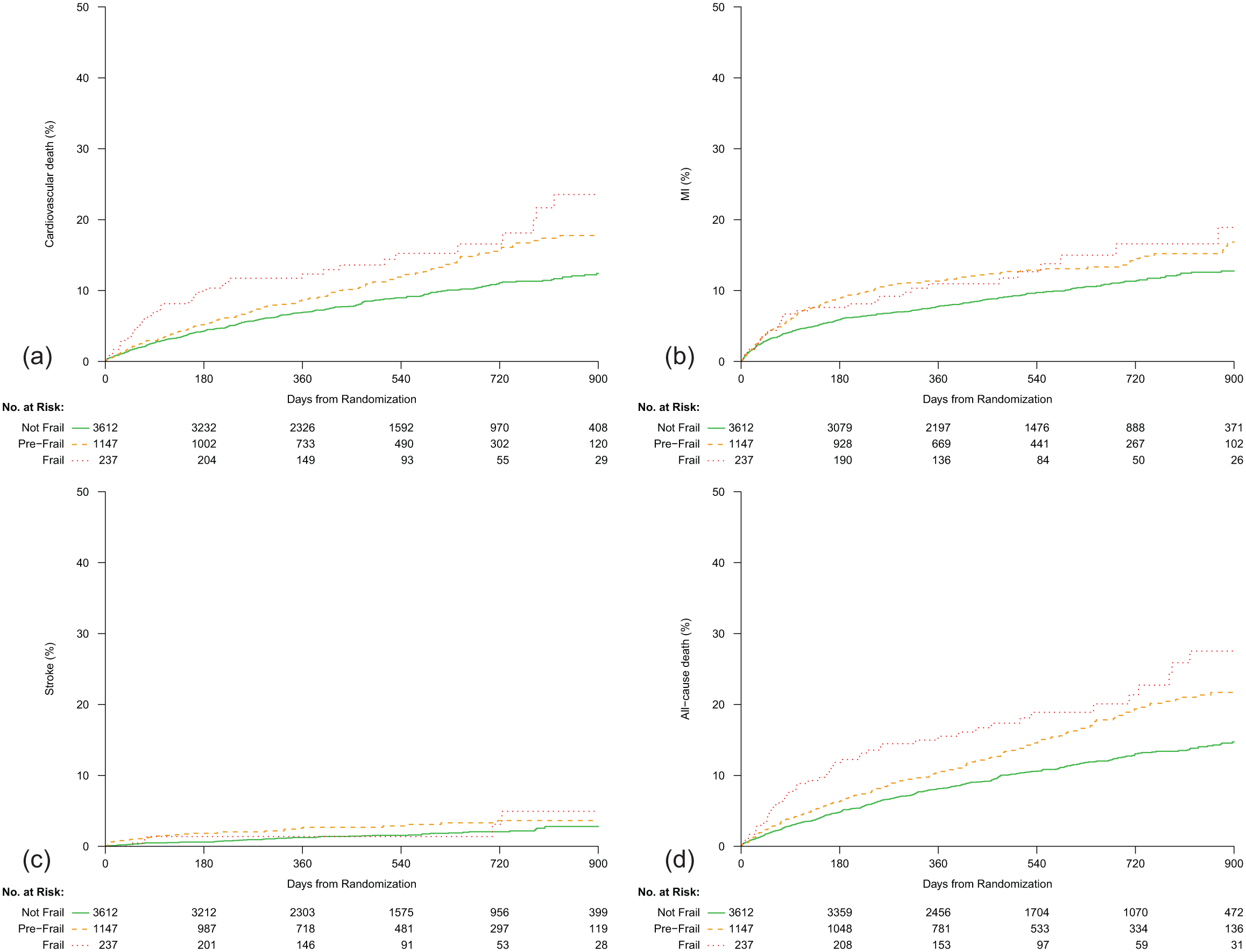
Kaplan-Meier survival curves according to frailty status (reference group: not frail). (a) cardiovascular death; (b) myocardial infarction (MI); (c) stroke; (d) all-cause death.
Relationship of frailty with all-cause mortality
Patients classified as frail experienced a higher unadjusted estimate of the likelihood of all-cause mortality compared with those classified as not frail (30.2% vs 15.0%; HR: 1.98; 95% CI: 1.47–2.68); p<0.001). Similar results were observed for the estimate of the likelihood of all-cause mortality for the pre-frail vs not-frail comparison (21.7% vs 15.0%; HR: 1.45; 95% CI: 1.22–1.73; p<0.001) (Table 4, Figure 2[d]).
Kaplan-Meier event rates and unadjusted associations of frailty status with ischemic and bleeding outcomes through 30 months among patients ⩾65 years of age.
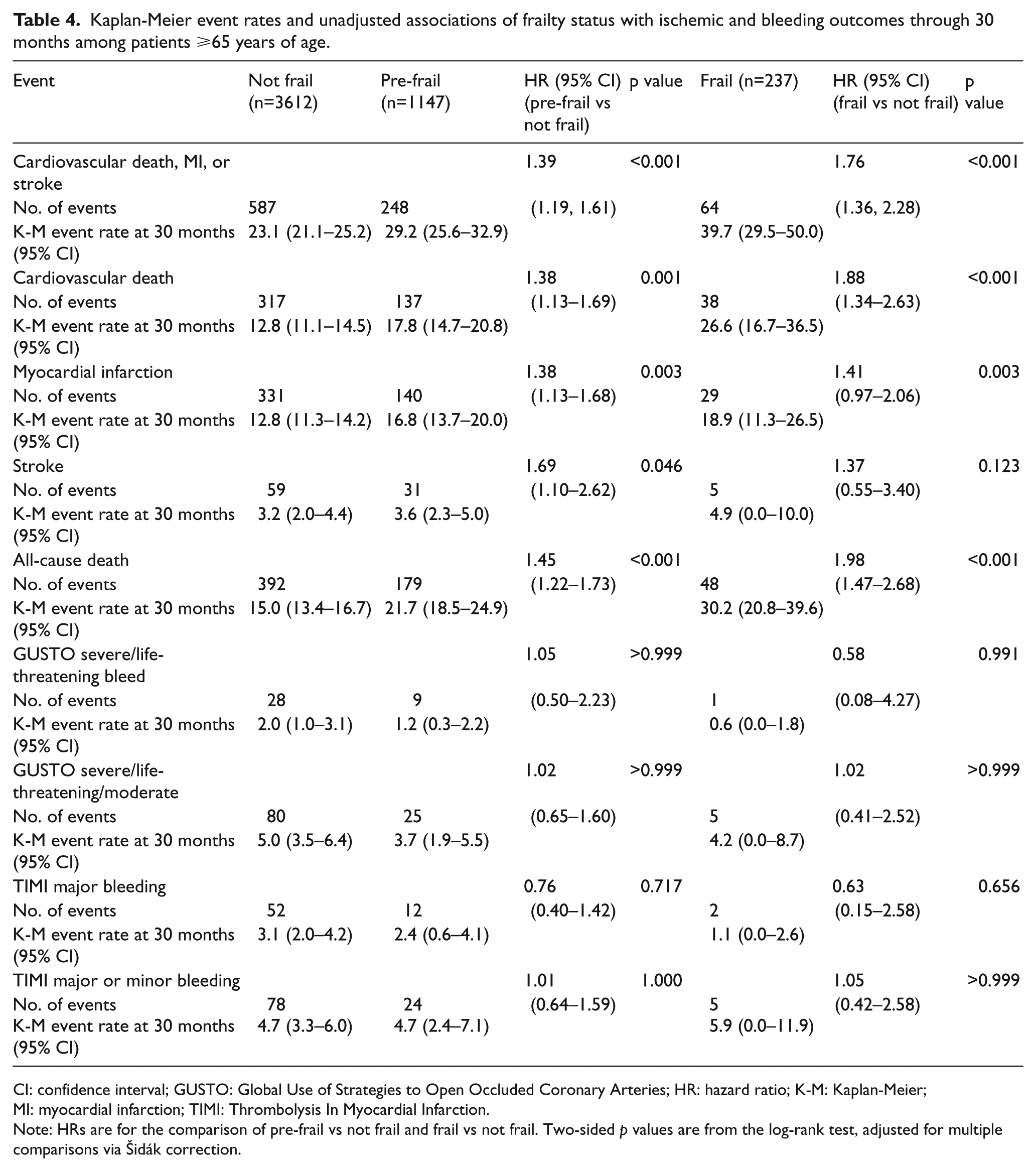
CI: confidence interval; GUSTO: Global Use of Strategies to Open Occluded Coronary Arteries; HR: hazard ratio; K-M: Kaplan-Meier; MI: myocardial infarction; TIMI: Thrombolysis In Myocardial Infarction.
Note: HRs are for the comparison of pre-frail vs not frail and frail vs not frail. Two-sided p values are from the log-rank test, adjusted for multiple comparisons via Šidák correction.
Comparison of GRACE and TRILOGY risk adjustment
Table 5 presents a comparison of the adjusted associations of ischemic outcomes from the GRACE six-month mortality model (i.e. death within six months after hospital discharge) 25 and the TRILOGY ACS risk adjustment model, showing qualitatively similar associations. For the primary endpoint of cardiovascular death, MI, or stroke, the pre-frail vs not-frail the GRACE adjustment was HR: 1.33; 95% CI: 1.15–1.54; p<0.001 and the TRILOGY adjustment HR: 1.20; 95% CI: 1.03–1.41; p<0.019 and for frail vs not-frail the GRACE adjustment was HR: 1.52; 95% CI: 1.18–1.98; p=0.002 and the TRILOGY adjustment HR: 1.27; 95% CI: 0.97–1.67; p=0.081.
Adjusted associations of frailty status with ischemic and bleeding outcomes among patients ⩾65 years of age.
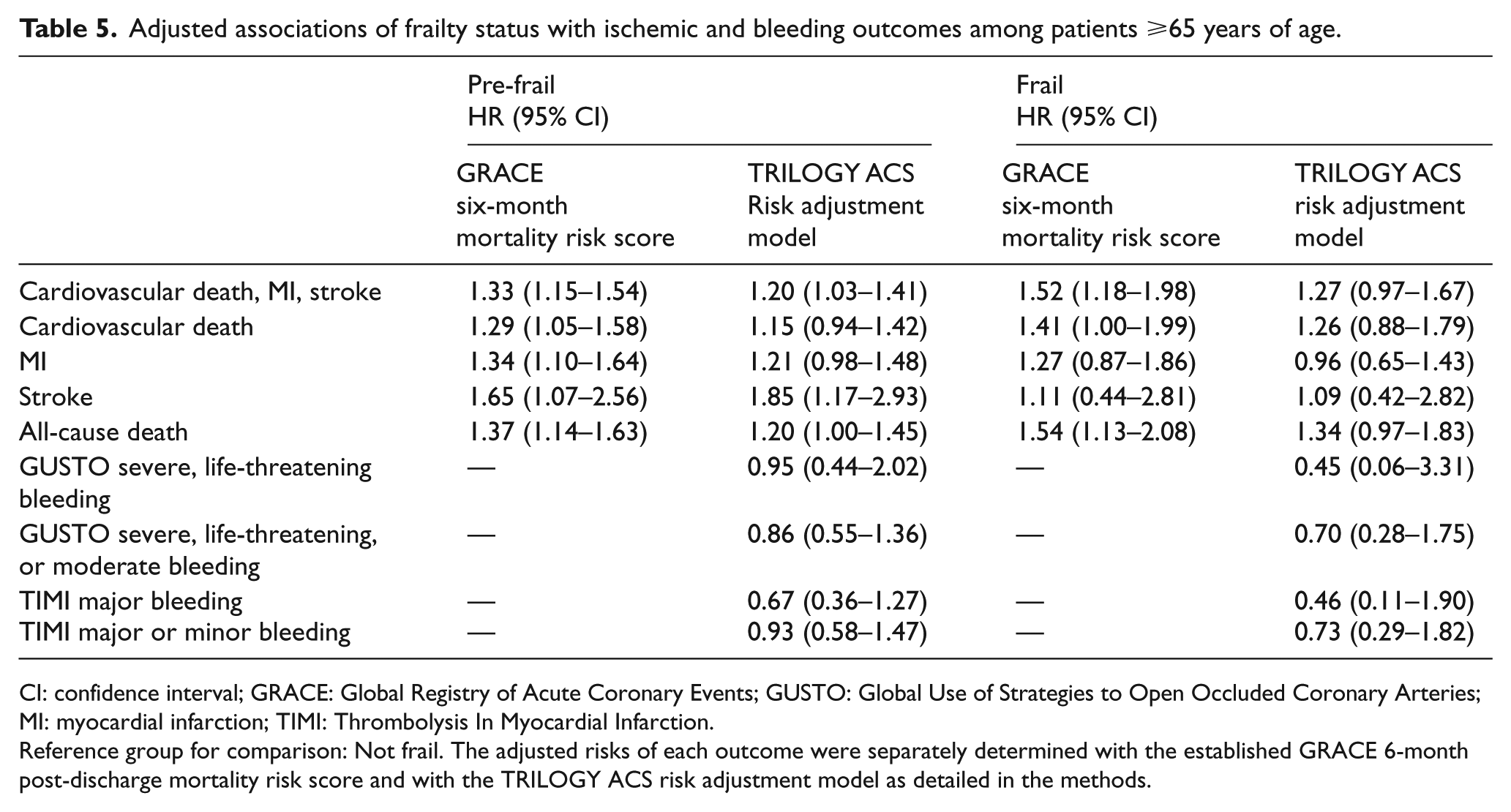
CI: confidence interval; GRACE: Global Registry of Acute Coronary Events; GUSTO: Global Use of Strategies to Open Occluded Coronary Arteries; MI: myocardial infarction; TIMI: Thrombolysis In Myocardial Infarction.
Reference group for comparison: Not frail. The adjusted risks of each outcome were separately determined with the established GRACE 6-month post-discharge mortality risk score and with the TRILOGY ACS risk adjustment model as detailed in the methods.
Relationship of frailty with bleeding
Regardless of bleeding classification, there was no evidence of an association between frailty and bleeding, either by GUSTO or TIMI criteria (Table 4). These findings persisted after risk adjustment.
Modulation of study treatment and outcomes by frailty
There was a significant interaction between study treatment and self-reported frailty (three levels) for the primary ischemic endpoint (cardiovascular death, MI, or stroke; p=0.032) (Figures 3 and 4). There was no relationship between study treatment and frailty (three levels) on bleeding events: GUSTO severe/life-threatening bleeding, pinteraction=0.671; GUSTO severe/life threatening/moderate bleeding, pinteraction=0.541; TIMI major bleeding, pinteraction=0.999; TIMI major/minor bleeding, pinteraction=0.625.
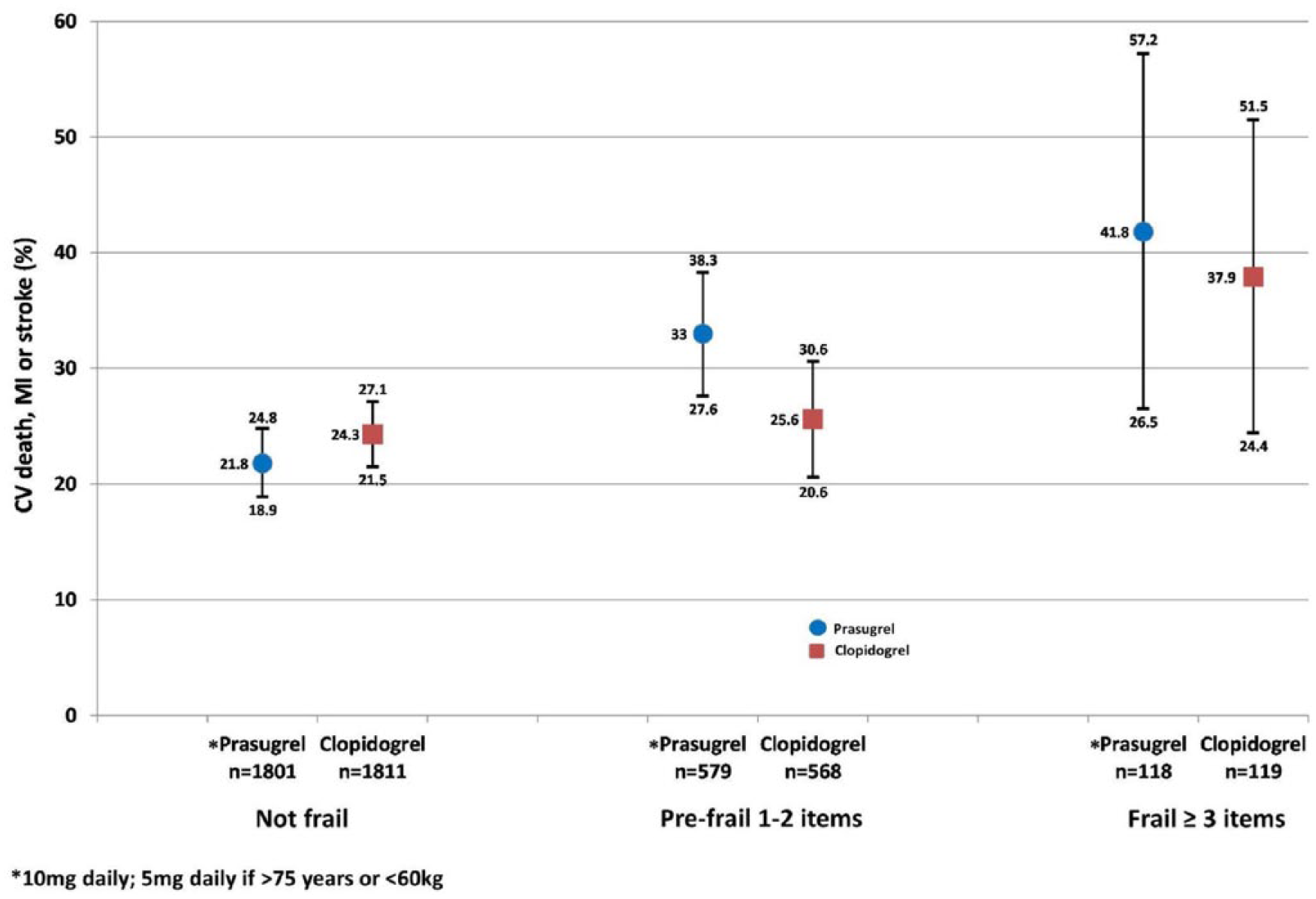
Association of prasugrel vs clopidogrel on cardiovascular death, myocardial infarction, or stroke according to frailty status. Event rates and 95% confidence intervals (CIs). CV: cardiovascular; MI: myocardial infarction.
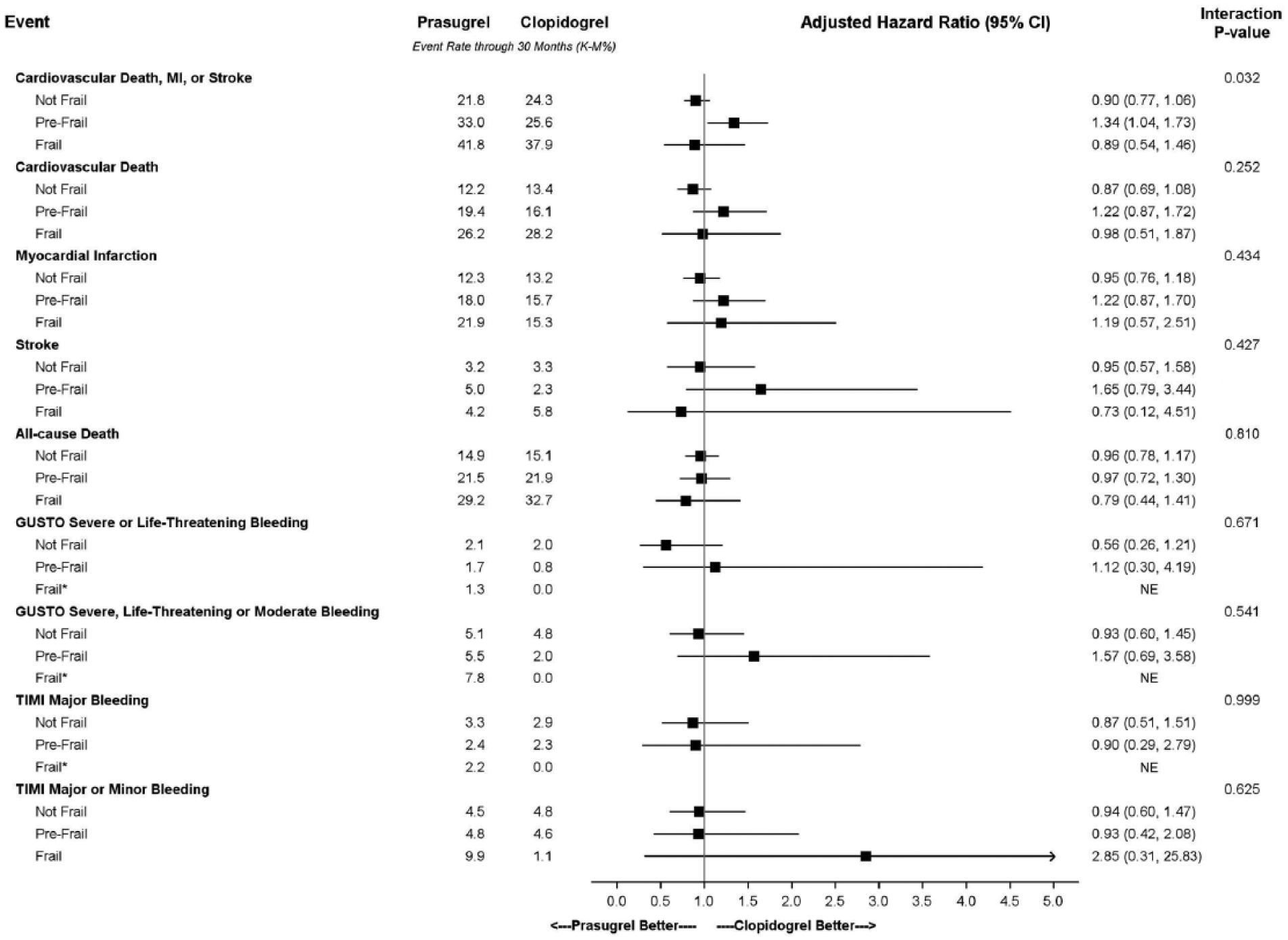
Adjusted treatment hazard ratios and rates of ischemic and bleeding events for frail, pre-frail, and not frail patients. GUSTO: Global Use of Strategies to Open Occluded Arteries; MI: myocardial infarction; NE: hazard ratio not computed due to insufficient data; TIMI: Thrombolysis In Myocardial Infarction.
Discussion
TRILOGY ACS is the first trial to prospectively assess the impact of frailty in a randomized trial of medically managed NSTEACS patients for whom long-term follow-up data were available. The self-reported domains that distinguish the frailty phenotype were categorized into one and two elements as pre-frail and three or more elements as frail. 4 Frailty was easily assessed by self-report with a high degree of completeness in this fashion in a large phase 3 cardiovascular clinical trial and demonstrated expected correlations with risk factors and cardiovascular outcomes. Self-reported frailty was also related to all-cause mortality: among frail patients, nearly 40% experienced a cardiovascular event over 30 months of follow-up, and one in four experienced cardiovascular death.
Frailty was present in over a quarter of patients: 23.0% of patients were classed as pre-frail and 4.7% as frail. The percentage of frail patients is lower than other estimates in community-based populations,32–34 either because of the selected nature of a clinical trial cohort or because of under-reporting by coordinators and/or patients. Frailty rates in registry populations with coronary artery disease have ranged from 27–63%, depending on the definition of frailty. 12 In patients >65 years with ACS, 34% had a Fried score ⩾322 and in a registry of patients with NSTEMI aged ⩾75 years, 48.5% were considered frail. 21
We found no relationship between frailty and bleeding, with pre-frail and frail patients having very few bleeding events overall. Frail patients tend to have decreased skeletal muscle mass and poor nutrition, factors that could predispose to increased bleeding risk. However, frail patients also have low activity levels, which may decrease propensity to bleeding from falls or trauma. More frail and pre-frail patients received proton-pump inhibitors at baseline, which may have reduced the incidence of gastrointestinal bleeding. In addition, more pre-frail and frail patients stopped their randomized study drugs as compared with not-frail patients, which could have reduced their exposure to bleeding risk over time. Other anticoagulants, with different mechanisms of action, metabolism, or clearance, may have different bleeding risk profiles among frail patients than those studied in the TRILOGY ACS trial.
There was no difference in the incidence of bleeding as measured by the GUSTO and TIMI bleeding criteria between patients randomized to receive prasugrel vs clopidogrel. More intensive antiplatelet therapy with prasugrel did not lead to more bleeding in frail patients. This may relate to the use of a 5 mg/day dose of prasugrel in low- body-weight and/or older (>75 years) patients.
Frail patients underwent angiography and invasive management prior to randomization at rates similar to those seen in not-frail patients. The rate of follow-up angiography was numerically greater in frail patients, but there was no statistically significant difference among frail, pre-frail, and not-frail patients. However, pre-frail and frail patients received evidence-based medications such as ACE inhibitors/ARBs and statins at lower rates than not-frail patients.
Frailty was associated with most risk factors for cardiovascular disease, as well as non-cardiovascular comorbidity. Frailty and aging are often associated in the community populations of older adults,2,4 but in this study among a population aged >65 years with recent ACS, frailty groups were of similar median ages. Our findings are important, as frailty may characterize the age-associated heterogeneity of older populations better than chronological age alone, and the assessment of frailty was easily performed.
GRACE risk model
Use of the GRACE score is recommended by European Society of Cardiology (ESC) guidelines for the management of ACS in patients presenting without persistent ST-segment elevation for the assessment of risk, 26 by the American College of Cardiology Foundation (ACCF)/American Heart Association (AHA) Task Force, 27 and by the UK National Institute for Health and Care Excellence (NICE) guidelines. 28 The GRACE risk score is in widespread clinical use for risk prediction and as a supplement to clinical reasoning and decision-making. Objective risk assessment with the GRACE risk score has been shown to be superior to physician estimation. 35 Risk prediction models such as GRACE are intended to estimate the probability or risk an outcome will occur within a specific time period in an individual with a specific predictor profile. In adjusting for the covariates that comprise the GRACE six-month mortality model, we found that frailty assessment added to this risk assessment, thus adding important prognostic information for clinicians.
Randomization to prasugrel or clopidogrel
There was a differential treatment effect among frailty groups for the primary efficacy endpoint of cardiovascular death, MI, or stroke (p=0.032). This effect appears to be driven by the pre-frail group, in which patients randomized to prasugrel exhibited a significantly higher risk of an event than patients randomized to clopidogrel. Interpretation of these findings must take into account the small numbers of frail patients.
Limitations
Several limitations to this study should be noted. The assessment of frailty was only collected at baseline and was not repeated later to assess change. Answers to questions were self-reported by patients and recorded by a research coordinator who filled out an electronic case report form, which may have allowed observer bias to enter. Although self-reporting is prone to many confounding factors, several studies have reported the value of self-reporting of frailty.36–38
More objective measures such as gait speed or hand grip with a dynamometer were not collected because of the complexity of doing so in an international trial conducted in >800 hospitals. In addition, the assessment of frailty was subjective, and weighting for low physical activity may have reflected other comorbid conditions. It is possible that our assessment of frailty and in particular questions about fatigue may also have captured elements of cardiac disease severity and heart failure. It may also be difficult to differentiate between frailty and depression. We did not collect data on the presence of depressive symptoms or antidepressant drug use in a systematic fashion.
Our study was performed in ACS patients for whom a course of medical management without revascularization was chosen by the treating physician; for this reason, our results may differ from those in patients undergoing an initial invasive strategy. Also, it is likely that very frail patients may have been excluded from the TRILOGY ACS trial and that the TRILOGY study population is not fully representative of registry populations.
The present study is small and not statistically powered for evaluating efficacy or safety in the three pre-specified frailty groups, and our results should be considered exploratory and hypothesis-generating. This is particularly pertinent with respect to the test for a treatment interaction based on a small sample of frail patients. Also, the randomized treatment discontinuation rates differed across frailty groups, which may have affected both efficacy and bleeding outcomes.
The strengths of our study include excellent ascertainment (97.9%), despite the complexity of doing this in the context of a clinical trial. Thus, we were able to detect a gradient, from normal to pre-frail to frail, in patient characteristics and outcomes.
In summary, 27.7% of the TRILOGY ACS trial population were either pre-frail or frail by self-report at baseline. Frailty was associated with baseline risk factors and higher GRACE score. Frailty was also independently associated with the primary composite outcome of cardiovascular death, MI, or stroke and with total mortality after adjustment for the GRACE six-month mortality score. Incorporating frailty assessment into clinical trials represents an important step in capturing data on previously unmeasured patient vulnerability. This evaluation of frailty improves risk assessment and prediction of future outcomes previously assumed to be adequately captured by chronological age and comorbidity alone in ACS patients and should be further developed into the assessment of elderly patients with ACS.
Footnotes
Acknowledgements
The authors would like to thank Charlene Nell, Team Support Administrator, Green Lane Cardiovascular Research Unit, for excellent secretarial assistance.
Funding
The TRILOGY ACS study was funded by Daiichi Sankyo Incorporated and Eli Lilly and Company.
Conflict of interest
HD White reports receiving grant support from Sanofi-Aventis, Eli Lilly, NIH, Merck Sharp & Dohme, AstraZeneca, GlaxoSmithKline, and Daiichi Sankyo Pharma Development; he also participates on advisory boards for AstraZeneca and is a consultant for Daiichi Sankyo Pharma Development. CM Westerhout, KP Alexander, and DD Cyr have no conflicts of interest to disclose. MT Roe receives research funding from Eli Lilly, Sanofi-Aventis, Daiichi Sankyo, the American College of Cardiology, the American Heart Association, and the Familial Hypercholesterolemia Foundation; and consulting payments or honoraria from AstraZeneca, Janssen Pharmaceuticals, Merck, Amgen, and Elsevier Publishers. All conflicts of interest for Dr. Roe from 2009 through 2014, inclusive, are listed at ![]() . KJ Winters is an employee and minor stockholder of Eli Lilly. KAA Fox reports receiving grant support from Eli Lilly, Bayer, Johnson & Johnson, and AstraZeneca; travel expenses from Eli Lilly; consulting fees from Eli Lilly, Bayer, Johnson & Johnson, AstraZeneca, Sanofi-Aventis, and Boehringer Ingelheim; and lecture fees from Bayer, Johnson & Johnson, AstraZeneca, and Sanofi-Aventis. D Prabhakaran reports receiving research grant funding from Eli Lilly and Medtronic Foundation and honoraria from Eli Lilly. JS Hochman reports receiving consulting fees from Eli Lilly and Company and GlaxoSmithKline. PW Armstrong reports receiving consulting fees from Eli Lilly, Hoffmann-La Roche, Merck, Axio Research, and Orexigen; grant support from Boehringer Ingelheim, Hoffmann-La Roche, Sanofi-Aventis, Scios, Ortho Biotech, Johnson & Johnson, Janssen Pharmaceuticals, GlaxoSmithKline, Amylin Pharmaceuticals, and Merck; and payment for developing educational presentations from AstraZeneca and Eli Lilly. EM Ohman reports receiving grant support and travel expenses from Daiichi Sankyo and Eli Lilly; consulting fees from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen Pharmaceuticals, Liposcience, Merck, Pozen, Hoffmann-La Roche, Sanofi-Aventis, The Medicines Company, and Web MD; grant support from Gilead Sciences; and lecture fees from Gilead Sciences, Boehringer Ingelheim, and The Medicines Company.
. KJ Winters is an employee and minor stockholder of Eli Lilly. KAA Fox reports receiving grant support from Eli Lilly, Bayer, Johnson & Johnson, and AstraZeneca; travel expenses from Eli Lilly; consulting fees from Eli Lilly, Bayer, Johnson & Johnson, AstraZeneca, Sanofi-Aventis, and Boehringer Ingelheim; and lecture fees from Bayer, Johnson & Johnson, AstraZeneca, and Sanofi-Aventis. D Prabhakaran reports receiving research grant funding from Eli Lilly and Medtronic Foundation and honoraria from Eli Lilly. JS Hochman reports receiving consulting fees from Eli Lilly and Company and GlaxoSmithKline. PW Armstrong reports receiving consulting fees from Eli Lilly, Hoffmann-La Roche, Merck, Axio Research, and Orexigen; grant support from Boehringer Ingelheim, Hoffmann-La Roche, Sanofi-Aventis, Scios, Ortho Biotech, Johnson & Johnson, Janssen Pharmaceuticals, GlaxoSmithKline, Amylin Pharmaceuticals, and Merck; and payment for developing educational presentations from AstraZeneca and Eli Lilly. EM Ohman reports receiving grant support and travel expenses from Daiichi Sankyo and Eli Lilly; consulting fees from AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, Janssen Pharmaceuticals, Liposcience, Merck, Pozen, Hoffmann-La Roche, Sanofi-Aventis, The Medicines Company, and Web MD; grant support from Gilead Sciences; and lecture fees from Gilead Sciences, Boehringer Ingelheim, and The Medicines Company.