
Abstract
Aims:
To examine the prognostic value of admission (A) and discharge (D) haemoglobin (Hb) and its relationship with N-terminal pro-hormone B-type natriuretic peptide (NT-proBNP) in patients hospitalised for acute heart failure (AHF). The outcomes of interests were rehospitalisation or death after one, six or twelve months after discharge.
Methods:
317 hospitalised AHF patients (74.7±9.4 years) were enrolled in two academic centres in Belgrade and Rome. Laboratory analyses, including NT-proBNP were assessed at admission, and Hb also at discharge. Patients were divided into two groups according to the presence of anaemia. Follow-up contact was made by telephone. Statistical analyses were performed using SPSS software version 21.0.
Results:
According to A and DHb levels (<120 g/l for women and <130 g/l for men), anaemia was present in 55% and 62% of patients, respectively (P=0.497). Lower DHb was associated with the rehospitalisation risk after one (OR=0.96, P=0.004), six (OR=0.97, P<0.001) and 12 months (OR=0.97, P<0.001). For every g/l decrease of DHb, the risk of rehospitalisation after one year was increased by 3.3%. In the first six months, DHb contributed to increased risk of death (OR=0.97, P=0.005), but NT-proBNP showed greater power (OR=2.1, P<0.001).
Conclusions:
In AHF patients discharge anaemia is a strong predictor for short and long-term rehospitalisation, while NT-proBNP seems to be a better predictor for mortality. Discharge Hb and NT-proBNP should be assessed together in order to detect the patients with higher risk of future death and rehospitalisation.
Introduction
Anaemia is a common comorbidity in patients with heart failure (HF), with a prevalence of about 15–40% in chronic HF,1–5 and 30–60% in acute HF,6–10 depending on the study and definition of anaemia. Anaemic HF patients are usually elderly, women, in an advanced stage of the disease, with worse renal function, diabetes mellitus (DM), arterial hypertension, and require longer hospitalisation.1–11 Anaemia is associated with a higher risk of HF rehospitalisation, and in many studies also with an increased mortality.1–12 In the study by Kosiborod et al., for example, it was suggested that anaemia might not be sufficient to explain the mortality risk of HF patients, because it was attenuated by other comorbidities and clinical conditions (atrial fibrillation, hypertension, etc.). 7
Haemoglobin (Hb) is also shown to be inversely associated with N-terminal pro-hormone B-type natriuretic peptide (NT-proBNP),13,14 which is already known to be an independent prognostic marker of HF mortality.15–17 However, the relationship between anaemia and NT-proBNP, as well as their predictive values, are still not completely clear.
Although there have been a number of studies on anaemia in HF, not many of them have dealt with its role in the acute phase of the disease. Its relationship with NT-proBNP is unclear, and there are still some controversies about its predictive value in HF, especially with regard to mortality.18,19 So far, only one study (Van der Meer et al. ) examined the prognostic value of Hb changes during hospitalisation. It has been shown that a rapid Hb increase during the first week is associated with lower mortality within 180 days. 20
The aim of this study was to examine the role of anaemia in acute heart failure (AHF), its relationship with other comorbidities, clinical characteristics, drugs and NT-proBNP, and association with adverse events after AHF hospitalisation.
Methods
The study included 317 patients hospitalised for AHF and discharged alive. Patients were recruited from emergency or cardiology departments of two academic centres, University Clinical Hospital Center, “Dr Dragisa Misovic-Dedinje”, Belgrade, Serbia, and Sant’Andrea Hospital, Rome, Italy. The study conformed to the principles of the Declaration of Helsinki, and was approved by the local institutional ethics committees. All patients provided written informed consent.
The diagnoses of HF and AHF were made according to the criteria of the European Society of Cardiology. 21 Histories of comorbidities, such as arterial hypertension (HTA), atrial fibrillation/flutter (AF), coronary artery disease, DM, chronic obstructive pulmonary disease (COPD), and haematological diseases were collected and recorded by the examining physician. Ischaemic cardiomyopathy (ICM) was defined as HF due to coronary artery disease. Patients with high blood pressure at examination or currently receiving antihypertensive drugs, were considered hypertensive. Paroxysmal and de-novo AF were considered as present. DM was defined according to the American Diabetes Association criteria. 22 Glomerular filtration rate (eGFR) was estimated by the Cockcroft–Gault formula,23,24 and renal failure (RF) was considered present if eGFR was less than 60 ml/min/1.73 m2. Respiratory insufficiency (RI) was defined as admission arterial oxygen saturation <94%. Left ventricular ejection fraction (LVEF) was measured by standard two-dimensional echocardiography, by the Simpson rule.
Routine laboratory measurements, including NT-proBNP, were performed at hospital admission. Total blood count was also done at discharge. Patients with detected low feraemia and high total iron binding capacity were considered to have sideropaenia.
Patients were divided into two groups according to the presence of anaemia: anaemic and non-anaemic patients. Anaemia was defined as an Hb level <120 g/l for women and <130 g/l for men, according to the World Health Organization definition of anaemia. Two separate analyses were performed. In the first one (A) patients were divided into groups according to admission Hb (AHb), and in the second one (D) according to discharge Hb (DHb).
Follow-up
Patients were contacted by telephone one month (31 days), six months and 12 months after discharge. The outcomes of interest for the analysis were HF rehospitalisation and death from any cause.
Statistical analysis
Statistical analyses were performed using SPSS software version 21.0. For all tests two-sided P values ⩽0.05 were considered significant. Prior to analysis, NT-proBNP was transformed using a natural logarithm because of significant skewness of distributions. Continuous variables are presented as means with standard deviation (SD), or medians with interquartile range (IQR), and categorical variables as frequencies and percentages. As noted, two separate statistical analyses were performed for AHb and DHb, as indicators of anaemia. Student’s t tests, Mann–Whitney, Pearson’s χ2 and Fisher’s exact tests were used for comparison of patient characteristics and discharge therapy (antiplatelets, angiotensin-converting enzyme (ACE) inhibitors, beta blockers, calcium channel antagonists (CCAs), oral anticoagulant therapy, anti-arrhythmics, aldosterone antagonists, iron supplements, folic acid supplements, erythropoetin) between groups where appropriate. The relationship between ln(NT-proBNP) and Hb was tested by Pearson’s correlation.
One, six and 12 month follow-up analyses were performed. The differences in frequencies of the appearance of adverse events between the groups were assessed by Pearson’s χ2 test. Hb levels of patients with and without adverse events were compared by independent t test. Binary logistic regression models were used for examining the association between Hb and adverse events, univariately and adjusted for baseline demographic characteristics (age, gender), comorbidities (ICM, HTA, AF, DM, RF, RI, haematological diseases), clinical (admission heart rate, LVEF) and laboratory findings (blood sodium, potassium, NT-proBNP), and therapies that were significant in univariate analysis, and also for NT-proBNP regardless of its significance. Results are reported as odd ratios (OR) with 95% confidence intervals (CI). The area under the receiver operating characteristic (ROC) curve (AUC) was used to evaluate the sensitivity and specificity of adverse event predictors.
Results
Patients’ baseline characteristics, with length of stay (LOS), discharge therapy and differences between anaemic and non-anaemic patients (A and D analyses), are shown in Table 1. The mean age of the study population was 74.7±9.4 years and 52.7% were men. Only 3.8% of patients had some of the haematological diseases and none has reported active bleeding complications, neither during hospitalisation nor follow-up.
Baseline characteristics, discharge therapy and differences between anaemic and non-anaemic patients (A and D analysis).
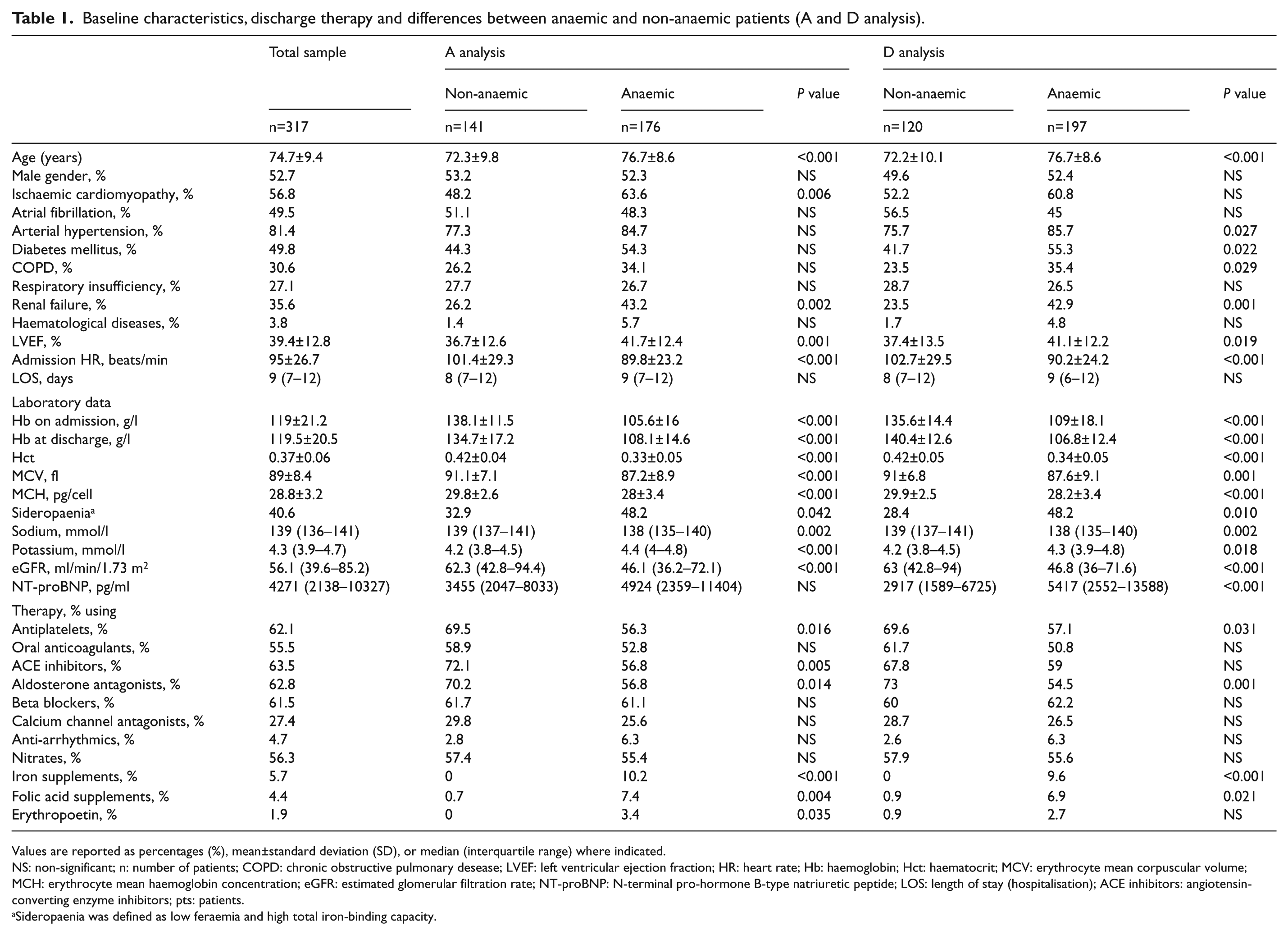
Values are reported as percentages (%), mean±standard deviation (SD), or median (interquartile range) where indicated.
NS: non-significant; n: number of patients; COPD: chronic obstructive pulmonary desease; LVEF: left ventricular ejection fraction; HR: heart rate; Hb: haemoglobin; Hct: haematocrit; MCV: erythrocyte mean corpuscular volume; MCH: erythrocyte mean haemoglobin concentration; eGFR: estimated glomerular filtration rate; NT-proBNP: N-terminal pro-hormone B-type natriuretic peptide; LOS: length of stay (hospitalisation); ACE inhibitors: angiotensin-converting enzyme inhibitors; pts: patients.
Sideropaenia was defined as low feraemia and high total iron-binding capacity.
Anaemia was detected in 176 (55.5%) patients on admission, and in 197 (62.2%) at discharge. Of all patients 49.8% had both A and D anaemia, 30.6% none, 7.3% only A, 12.3% only D. This last group of patients had normal Hb levels at A, but close to the lower limit, so although Hb change was not statistically significant, they still entered the anaemic group. Mean AHb for these men was 136.06 g/l and mean Hb change was 7.1 g/l, while for women it was 125.25 g/l, with Hb change of average 7.0 g/l. In about 50.3% of patients there was an increase in Hb (median 8 (4–15)), in 43.7% there was a decrease (median 9 (5–14)), and in 6% Hb did not change, but finally mean A and DHb did not differ (P=0.497). Neither an absolute increase nor a decrease of Hb correlated with adverse events in any of the three end-time points. Moreover, the 7.3% of patients who were anaemic only at A and not at D, did not show better outcomes. Regarding renal function, patients with A anaemia, as well as with D anaemia, had worse renal function than non-anaemic patients (Table 1), but the difference in eGFR and renal failure between A anaemic and D anaemic was not significant (P=0.728).
Anaemic patients were significantly older, more often had sideropaenia, worse RF, higher LVEF and lower admission heart rate. There was no difference in gender, presence of haematological diseases, atrial fibrillation, RI or LOS. According to AHb, anaemic patients were more likely to have ICM, but not HTA, DM and COPD, as according to DHb.
NT-proBNP was higher in those with D anaemia (Table 1). Both A and DHb showed a strong negative correlation with NT-proBNP (P<0.001).
Therapy
Sixteen anaemic patients received blood transfusion during hospitalisation (mean AHb=72.4±13.9 g/l, mean DHb=88.2±5.7 g/l). After hospitalisation, anaemic patients were less likely to be treated with antiplatelets, aldosterone antagonists or ACE inhibitors. The groups did not differ with regard to treatment with oral anticoagulants, nitrates, beta blockers, CCAs and anti-arrhythmics. The patients were discharged after they achieved compensation, determined mostly by clinical and radiological improvement, lower New York Heart Association class, and the same or improved renal function.
Follow-up
Nine patients (2.8 %) were lost to one-month follow-up, 12 (3.8 %) to six-month and 14 (4.4 %) to one-year follow-up, so we analysed 308, 305 and 303 patients, respectively. During the first month after discharge, 16 (5%) patients died and 19 (6%) were rehospitalised. Six months after discharge 43 (13.6%) had died, and 51 (16.1%) had been rehospitalised. After one year, a death event was reported in 62 patients (19.6%) and rehospitalisation in 57 (18%).
One-month follow-up
Admission haemoglobin
There was no association between anaemia and adverse events in one-month follow-up (P=0.099); 8.2% A anaemic patients and 3.7% non-anaemic patients were rehospitalised P=0.101); while 5.8% and 4.4% died, respectively (P=0.564). AHb did not differ between patients with and without either adverse event (rehospitalisation: 112.7±26.3 vs. 120.6±21.5 g/l, P=0.125; death: 113.3±23.2 vs. 120.4±21.6 g/l, P=0.200).
Discharge haemoglobin
No difference was found between anaemic and non-anaemic patients, either in the frequency of rehospitalisation (8.1% vs. 3.7%, P=0.218), or death (7% vs. 1.8%, P=0.058), but anaemic patients had more adverse events in total (15.0% vs. 5.5%, P=0.014).
DHb was lower in those with a later event (rehospitalisation: 105.5±21.1 vs. 120.1±20.1 g/l, P=0.003; death: 103.5±17.5 vs. 120±20.5 g/l, P=0.002).
Lower DHb was associated with an increased risk of rehospitalisation, where for every 1 g/l decrease of Hb the odds of having a rehospitalisation increased by 4.1%. After adjustment with COPD that correlated with the event (P=0.008) and NT-proBNP that did not (P=0.240), the significance did not change. It was also associated with higher mortality, but was significantly confounded by NT-proBNP, which was an independent predictor (OR=3.80, 95% CI 1.48–9.74, P=0.005; Table 2).
Logistic regression analysis of admission and discharge haemoglobin on one-month, six-months and one-year outcomes.
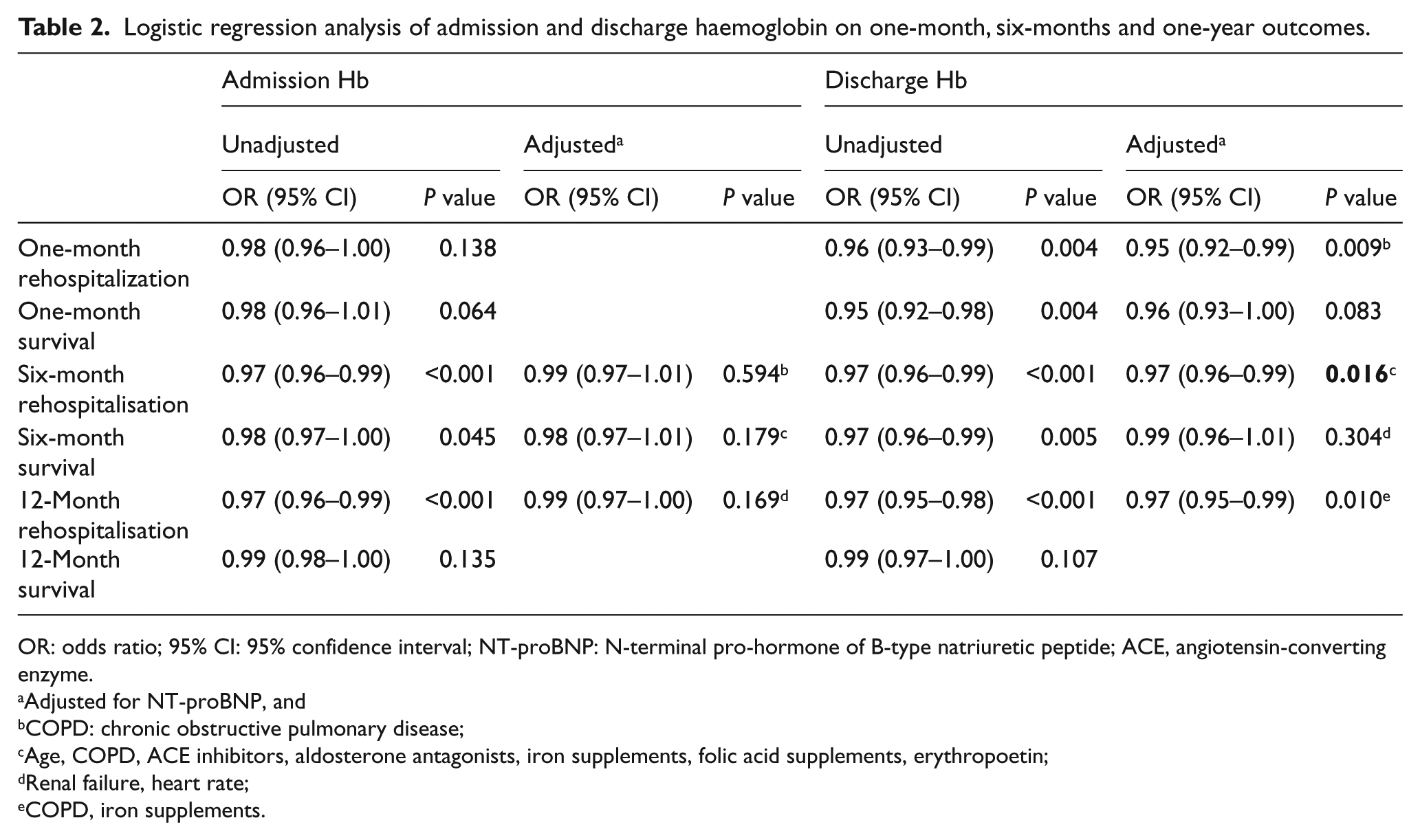
OR: odds ratio; 95% CI: 95% confidence interval; NT-proBNP: N-terminal pro-hormone of B-type natriuretic peptide; ACE, angiotensin-converting enzyme.
Adjusted for NT-proBNP, and
COPD: chronic obstructive pulmonary disease;
Age, COPD, ACE inhibitors, aldosterone antagonists, iron supplements, folic acid supplements, erythropoetin;
Renal failure, heart rate;
COPD, iron supplements.
On ROC analysis, both parameters seem to be useful tests to determine patients with a higher risk of death (DHb: AUC 0.73, P=0.002, 95% CI 0.61–0.86; NT-proBNP: AUC 0.77, P=0.002, 95% CI 0.62–0.92). When analysed together, the value of NT-proBNP increased (AUC 0.83, P<0.001, 95% CI 0.72–0.94), while for DHb it did not change (AUC 0.74, P=0.007, 95% CI 0.14–0.37). DHb was also fair for rehospitalisation (AUC 0.70, P=0.003, 95% CI 0.57–0.84) (Figure 1).
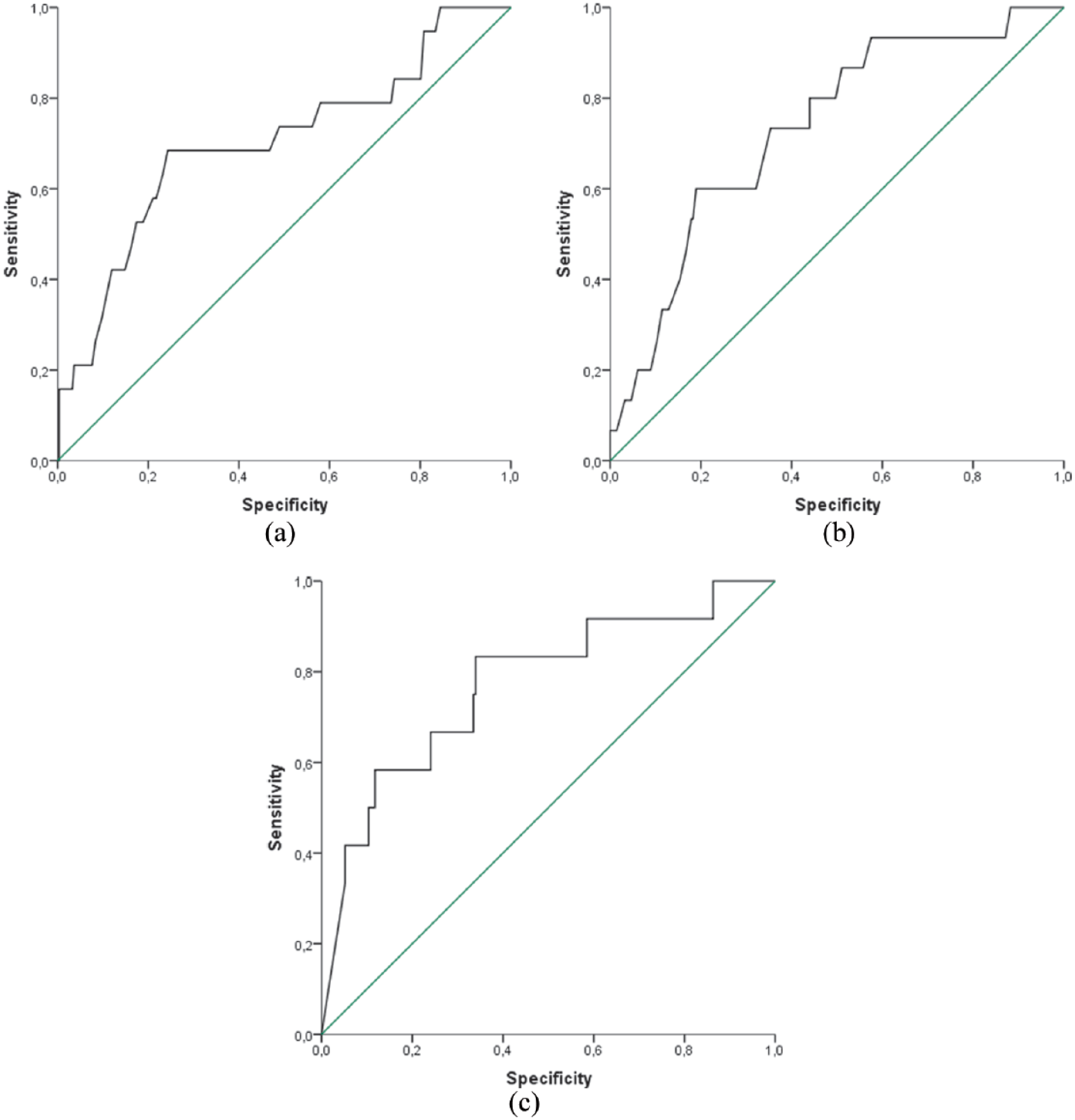
(a) ROC curve for discharge haemoglobin for predicting one-month rehospitalisation. (b) ROC curve for discharge haemoglobin for predicting one-month death event. (c) ROC curve for NT-proBNP for predicting one-month death event. ROC: receiver operating characterictic; NT-proBNP: N-terminal pro-hormone B-type natriuretic peptide.
Six-month follow-up
Admission haemoglobin
After six months from discharge, anaemic patients (A) had more adverse events (37.1 vs. 18.5%, P<0.001) in favour of rehospitalisation (22.4 vs. 9%, P=0.002), but not death (15.9 vs. 11.9%, P=0.315). AHb at baseline was lower in those who were later rehospitalised (108.1±24.5 vs. 122.3±20.1 g/l, P<0.001) and who died (113.7±22.7 vs. 120.9±21.1 g/l, P=0.043).
Lower AHb was associated with a higher risk of six-month rehospitalisation, and was not confounded by age (P=0.045), COPD (P=0.002), ACE inhibitors (P=0.002), aldosterone antagonists (P=0.005), iron (P=0.001) and folic acid supplements (P=0.002) and erythropoietin (P=0.028). After adjustment with NT-proBNP, which did not correlate with this event (P=0.079), the association was no longer significant (Table 2). ROC analysis showed similar results: AHb independently had poor prognostic value (AUC 0.66, CI 0.58–0.75, P<0.001), NT-proBNP had none (P=0.079), and in pooled analysis AHb was no longer significant (P=0.133).
Discharge haemoglobin
As for A anaemia, patients with D anaemia were more likely to be rehospitalised (21.5 vs. 10.3%, P=0.015), and not dead (16.7 vs. 9.3%, P=0.082). On the other hand, both rehospitalised patients and those who died had significantly lower DHb levels at baseline hospitalisation (rehospitalisated: 107.8±20.1 vs. 121.2±19.7 g/l, P<0.001; dead: 110.6±22.0 vs. 120.4±19.9 g/l, P=0.004).
DHb independently contributed to the higher risk of rehospitalisation, even when confounders were adjusted for (Table 2). The odds of having this event increased by 3.4% for every g/l decrease of DHb. It was almost a fair test to determine the patients with a higher rehospitalisation risk (AUC 0.68, 95% CI 0.59–0.77, P<0.001).
Both A and DHb, as well as heart rate (P=0.034), RF (P<0.001) and NT-proBNP (P<0.001) were associated with mortality, but only NT-proBNP remained an independent predictor (OR=2.03, 95% CI 1.27–3.23, P=0.003). The prognostic value of DHb was poor (AUC 0.64, 95% CI 0.53–0.74, P=0.006), but was slightly better than AHb (AUC 0.60, 95% CI 0.51–0.69, P=0.040) (see Figure 2). In pooled ROC analysis, both A and DHb remained significantly poor tests (AHb: AUC 0.63, 95% CI 0.53–0.74, P=0.018; DHb: AUC 0.65, 95% CI 0.53–0.76, P=0.010) and NT-proBNP was fair (AUC 0.72, 95% CI 0.18–0.38, P<0.001).
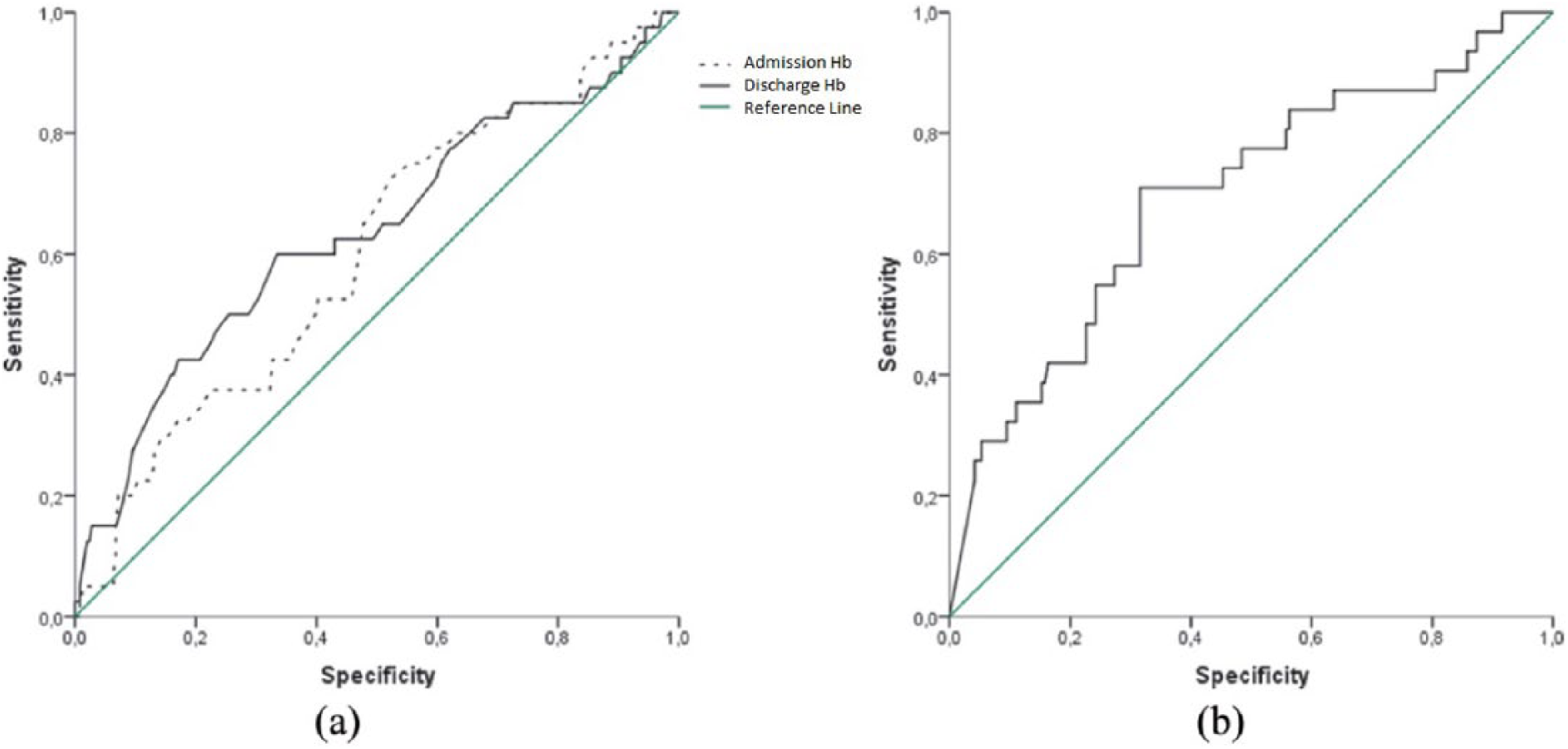
ROC curves on six-month survival: (a) Admission and discharge haemoglobin; (b) NT-proBNP. ROC: receiver operating characterictic; NT-proBNP: N-terminal pro-hormone B-type natriuretic peptide.
One-year follow-up
Both A and D anaemia correlated only with a higher rehospitalisation rate (A: 25.6% vs. 14.1%, P=0.013; D: 27.6% vs. 10.4%, P=0.001), and not with mortality (A: P=0.642; D: P=246). Baseline Hb levels were lower in rehospitalised patients (AHb: 110.8±23.4 vs. 122.5±20.5 g/l, P<0.001; DHb: 109.5±19.7 vs. 121.6±20.0 g/l, P<0.001), and there was no association between Hb and death (A: 117.0±25.1 vs. 120.8±20.6 g/l, P=0.272; D: 115.2±24.4 vs. 120.0±19.3 g/l, P=0.161).
A and DHb contributed to an increased risk of one-year rehospitalisation, but only DHb was independent. After adjustment AHb was again confounded by insignificant NT-proBNP (P=0.240), while not by COPD (P=0.044) and iron supplements (P=0.005). DHb showed poor prognostic value; AUC 0.67 (95% CI 0.6–0.75, P<0.001). For every g/l decrease of DHb, the rehospitalisation risk increased by 3.3%. NT-proBNP was an independent (OR=1.41, 95% CI 1.01–2.05, P=0.043) but poor predictor of one-year survival (AUC 0.63, 95% CI 0.54–0.72, P=0.004).
Discussion
Data from this study confirmed the results of previous international trials, which investigated the prognostic role of anaemia in HF; although in the majority of these studies chronic patients were considered,2,3,25 in our cohort we only included AHF patients.6,18 In our population, according to the A and DHb level, anaemia was present in about 55% and 62% of AHF patients, respectively (P=0.497). This finding suggests that the prevalence of anaemia in the acute phase of HF seems to be higher than in the chronic phase, considering the large meta-analysis of around 150,000 CHF patients enrolled in 34 different studies, performed by Groenveld et al., in which the prevalence of anaemia in CHF was estimated to be around 37.2%. 26 Confirming the data already available in the literature, the results of our study showed that patients with anaemia both at A and at D were significantly elderly and presented with worse renal function. These results seem to strengthen the emerging consideration of the multifaceted aetiology of anaemia development in HF, such as: iron deficiency, chronic diseases, renal impairment, haemodilution, bone marrow dysfunction, gastrointestinal bleedings and/or side effects of medications, which should be assessed and considered in every patient with AHF and anaemia. However, as shown in Table 1, about 43% of all anaemic patients had renal failure, 48% had sideropaenia (29 patients had both) and only 3.8% had haematological diseases. Average mean corpuscular volume indicates normocytic anaemia. Moreover, considering the insignificant increase of haemoglobin and unchanged renal function, we cannot say that our results relate to haemodilution, as suggested by Van der Meer et al. 20 Otherwise, our findings suggest that anaemia per se, and not as a surrogate of haemodilution, is an independent negative predictor of rehospitalisation in patients with AHF. Obviously, further targeted studies on larger populations are required to confirm the role of chronic inflammation in AHF patients with a low Hb level. In our study we also found a significant relationship between anaemia and higher LVEF. This result, apparently surprising, confirms the independent predictive value of anaemia in HF patients irrespective of whether preserved or reduced ejection fraction is present, as it has already been demonstrated by von Haehling et al. 5 However, as for in-hospital LOS, no difference between anaemic and non-anaemic groups was found in our study, whereas Young et al. 9 and von Haehling et al. 6 showed that, compared to non-anaemic AHF patients, anaemic AHF patients require longer hospital stays. Our different finding may be explained by an ongoing underestimation of the impact of anaemia in our acute settings and the consequent undervaluation of the prognostic role of anaemia in AHF patients.
To our knowledge, no previous data are available about 30-day follow-up; therefore, in this study we first demonstrated that, compared to patients without anaemia, a lower DHb value was associated with an increased risk of rehospitalisation at 30 days after discharge. Moreover, in our cohort we proved the presence of an association between lower DHb, higher NT-proBNP levels and 30-day increased mortality. This finding encourages the use of both DHb and NT-proBNP to risk stratify AHF patients at D.
Similar results were obtained by Baggish et al. in 690 AHF patients, although they considered a longer 60-day follow-up, 18 while Tarantini et al. showed an increased in-hospital mortality of AHF patients from 5.3% of the non-anaemic group to 12.1% of the anaemic group. 27 Although we found the association between D anaemia and total one-month adverse events, the P value of either event analysis did not reach the threshold of statistical significance, probably due to the small percentage of adverse events.
Our results confirmed the negative impact of a lower DHb level in AHF patients in terms of increased six-month follow-up rehospitalisation, while the relationship between either A or DHb with mortality was strongly affected by NT-proBNP. Our study confirmed the independent predictive value of NT-proBNP for survival, when used alone 28 or when compared to A, DHb and absolute Hb change. 20
Finally, as in the majority of the published studies, we analysed the influence of anaemia on one-year follow-up and we found that A and DHb independently significantly contributed to the increased risk of one-year rehospitalisation.
Conclusions
In patients admitted for AHF, the presence of anaemia at the D moment from the hospital is a strong predictor for 30-day and long-term rehospitalisation. Thus, in our opinion, the presence of anaemia in AHF patients should always be investigated, although the presence of anaemia proved to be a significant independent predictor of future events. Our results confirmed the available data in the literature concerning an integrated use of DHb plus NT-proBNP in order to detect patients with a higher risk of death and rehospitalisation. However, further studies are needed to understand better the aetiology of anaemia in acute and in chronic HF, the relationship between natriuretic peptides and anaemia and their impact on HF prognosis.
Limitations
The first limitation of this study was the small population (317 subjects), even though it is a homogenous sample. In addition, this was an observational study that reflected the ongoing underestimation of the prognostic role of anaemia in AHF, and its under-treatment, despite its negative predictive value has already been confirmed in the literature by several trials. Moreover, we do not have enough data to establish the etiology of anaemia in different patients so we can speculate that DHb per se has a negative predictive value, apart from its cause; consequently, new research in this field is mandatory.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.