
Abstract
Since the approval of sacubitril-valsartan for the treatment of chronic heart failure with reduced ejection fraction, a commonly raised suspicion is that a wider clinical use of this new drug may diminish the clinical utility of B-type natriuretic peptide testing as sacubitril may interfere with B-type natriuretic peptide clearance. In this education paper we critically assess this hypothesis based on the pathophysiology of the natriuretic peptide system and the limited published data on the effects of neprilysin inhibition on natriuretic peptide plasma concentrations in humans. As the main clinical application of B-type natriuretic peptide testing in acute cardiac care is and will be the rapid rule-out of suspected acute heart failure there is no significant impairment to be expected for B-type natriuretic peptide testing in the acute setting. However, monitoring of chronic heart failure patients on sacubitril-valsartan treatment with B-type natriuretic peptide testing may be impaired. In contrast to N-terminal-proBNP, the current concept that the lower the B-type natriuretic peptide result in chronic heart failure patients, the better the prognosis during treatment monitoring, may no longer be true.
Keywords
Introduction
A novel compound, sacubitril-valsartan, an angiotensin receptor neutral endopeptidase (neprilysin; EC 3.4.24.11) inhibitor, was recently documented to improve outcomes in patients with systolic heart failure (HF). 1 It is a salt complex of valsartan and sacubitril, the neprilysin inhibitor prodrug that is processed in the liver into its active moiety, 2 which then interacts with a variety of vasoactive peptides including enhancing natriuretic peptide (NP) activity. 2 Since its recent approval for the treatment of symptomatic chronic HF with reduced ejection fraction in the USA and the European Community a commonly raised suspicion is that the clinical use of this agent will diminish the clinical utility of B-type natriuretic peptide (BNP) testing because sacubitril may inhibit BNP degradation. In this paper we will critically assess this hypothesis based on the known pathophysiology of the cardiac NP system and the limited published data on the effects of neprilysin inhibition on NP plasma concentrations in humans.
Pathophysiology of the cardiac NP system and circulating NP forms
It is outside the scope of this paper to provide a detailed review on the pathophysiology and metabolism of the cardiac NPs, which has been done recently;3–7 instead only the essentials are briefly summarised in the text and figures. The family of NPs comprises atrial or A-type natriuretic peptide (ANP), B-type or brain natriuretic peptide (BNP), C-type natriuretic peptide (CNP) and urodilatin, which is a renal isoform of ANP isolated from human urine. ANP and BNP are key regulators of the body’s regulation of volume and blood pressure homeostasis. They do this by activating transmembrane guanylyl cyclase and elevating intracellular cyclic guanosine monophosphate (cGMP), which induces subsequent increases in renal sodium and water excretion and stimulation of vasodilation (see Figure 1). NPs also have an anti-hypertrophic function in the heart and prevent adverse vascular remodelling. ANP and BNP are primarily secreted from the heart in response to increased myocardial stretch mediated by volume or pressure overload, and thus NP increases can be regarded as markers of ‘cardiac stress’. In contrast to ANP, only limited amounts of BNP are stored in atrial granules, so most BNP secretion requires gene transcription and subsequent peptide synthesis mostly in the ventricles (see Figures 2 and 3). In settings where acute changes in atrial stretch occur the changes in ANP concentrations are more rapid and pronounced than BNP changes. However, with chronic myocardial stretch there is upregulation of ventricular NP production and particularly BNP.
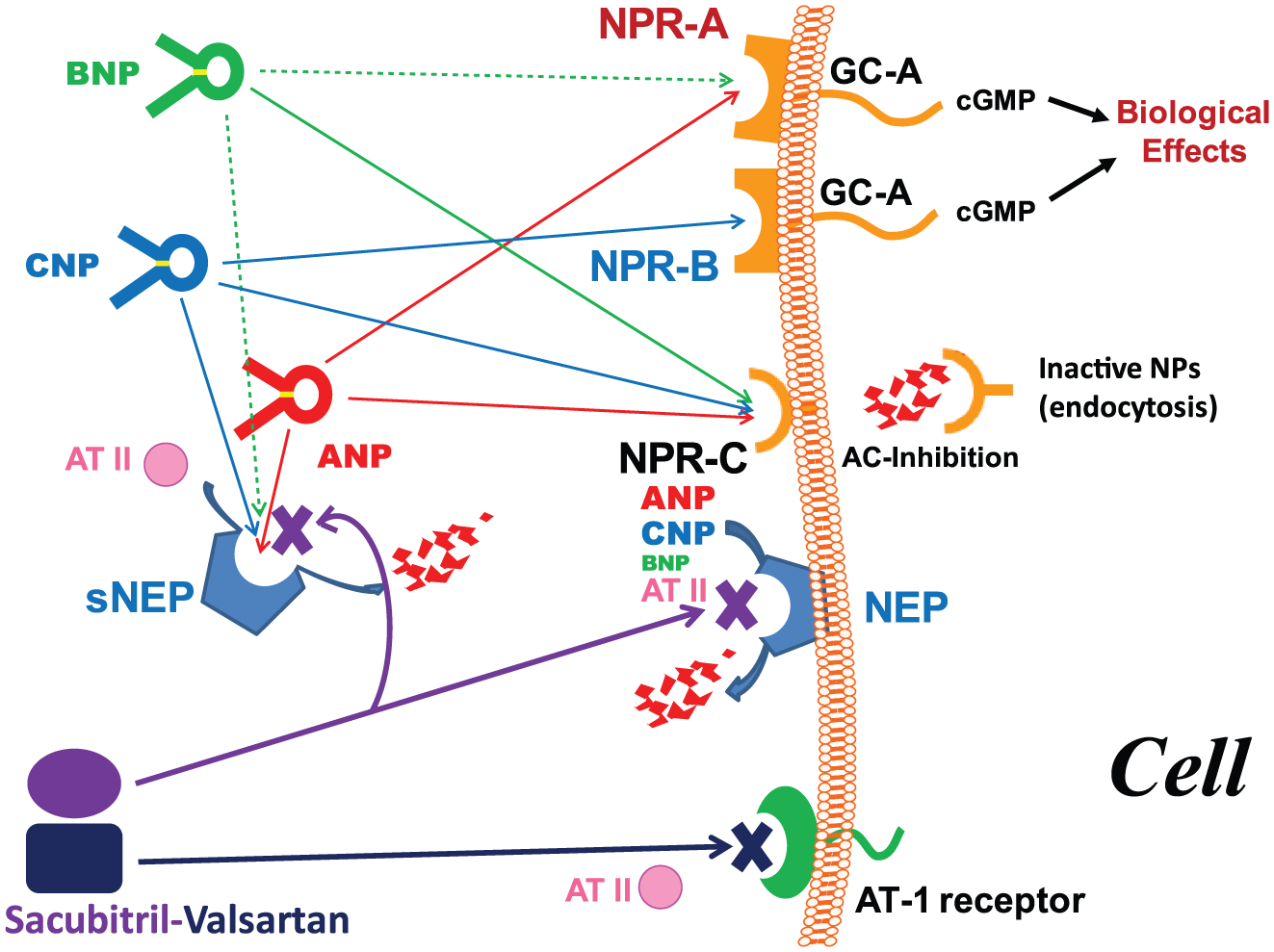
Clearance of natriuretic peptides with interference of sacubitril-valsartan.
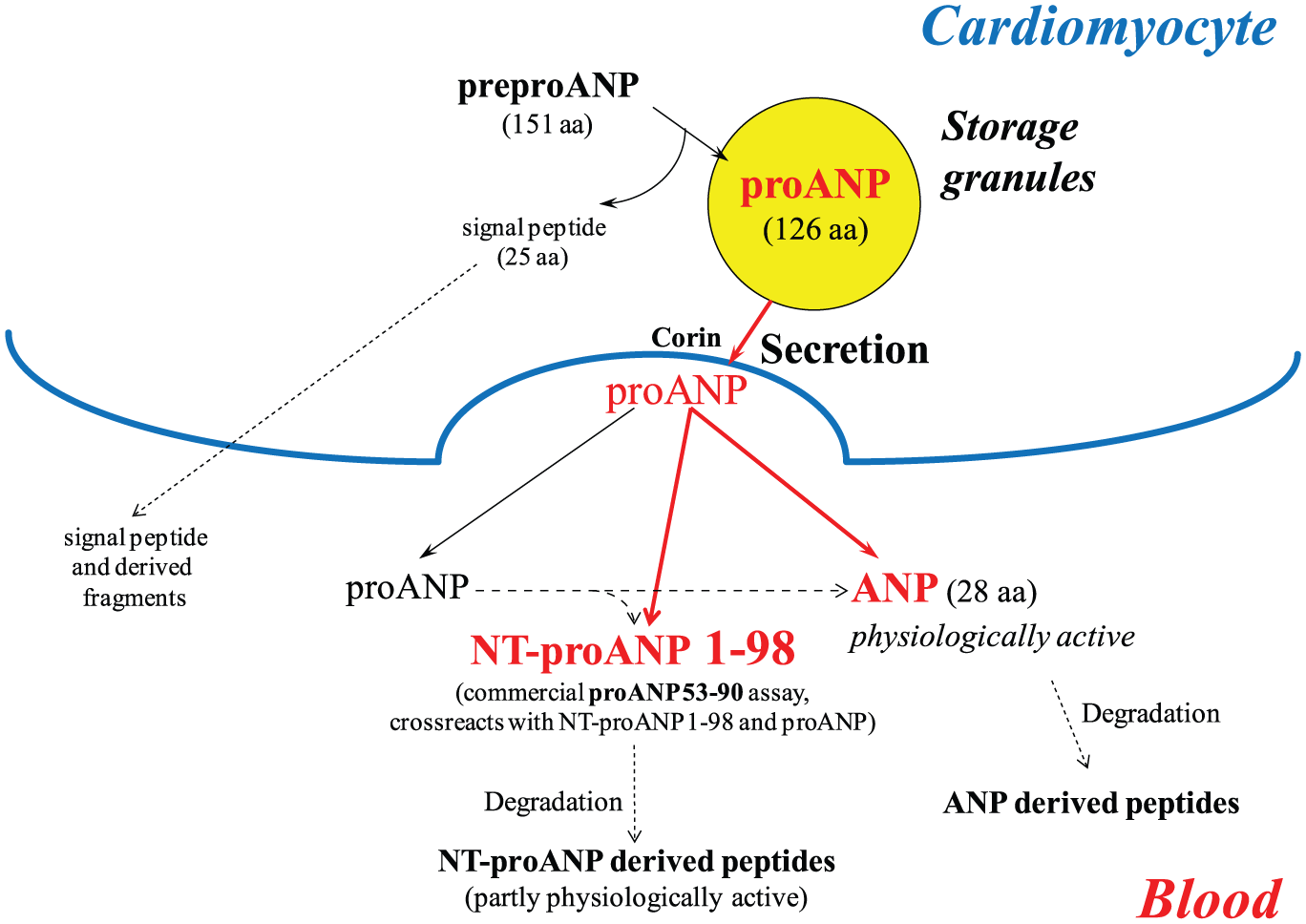
Synthesis, processing and circulating forms of pro A-type natriuretic peptide derived peptides.
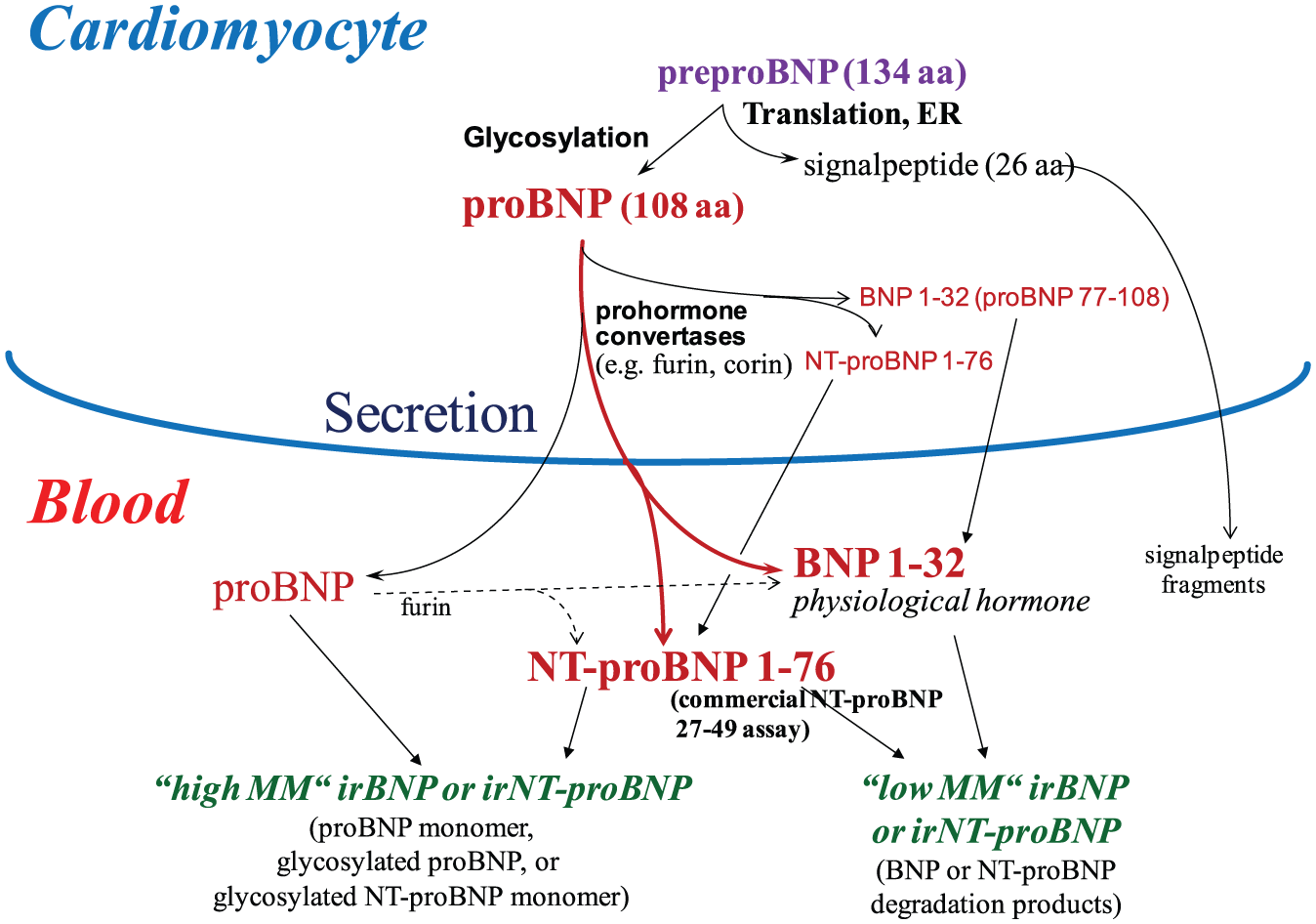
Synthesis, processing and circulating forms of pro B-type natriuretic peptide derived peptides.
ANP is synthesised as a precursor (preproANP, 151 amino acids). After removal of the signal peptide in the endoplasmatic reticulum, proANP (126 amino acids) is stored in secretory granules of atrial cardiomyocytes (see Figure 2). Upon secretion proANP is thought to be processed by the serin protease corin, which is anchored on the cell surface, at the site arginine-98–serine-99 generating a 98-amino acid N-terminal peptide (NT-proANP) and a 28-amino-acid C-terminal hormonally active peptide (ANP, see Figure 4). These peptides circulate without binding to plasma proteins. In addition, several split products of ANP and NT-proANP, but also intact proANP, have been detected in HF patients. 6 At the mid-region of proANP little proteolytic degradation occurs. 8 Recent data suggest that it is the unproceesed proANP that is the more important stimulator of biological activity. 9
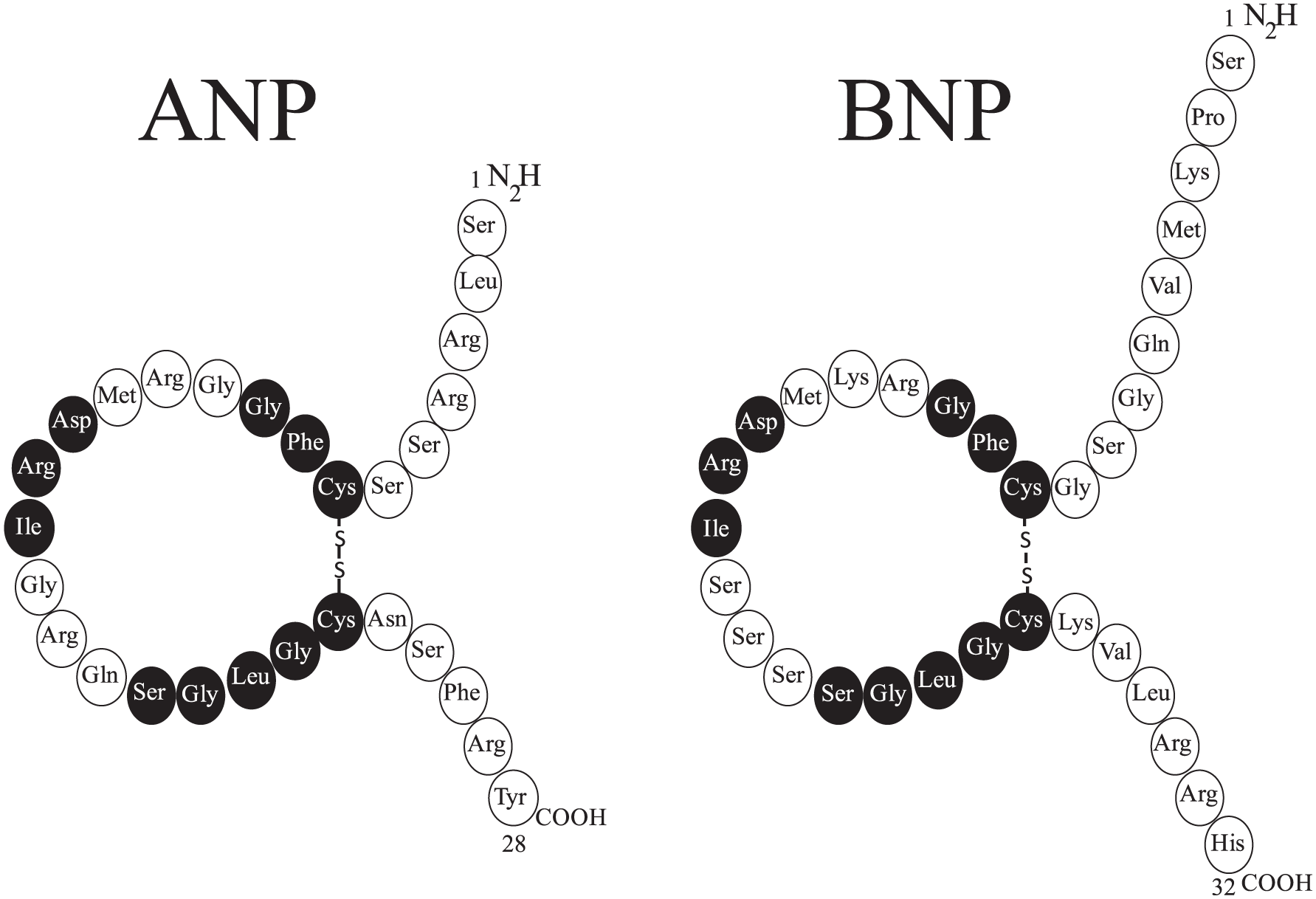
Structure of A-type and B-type natriuretic peptides.
Figure 3 summarises our current understanding of BNP synthesis and processing. The initial gene product is pre-proBNP 1-134, which undergoes removal of a 26-amino acid signal peptide in the sarcoplasmatic reticulum during translation, leading to the formation of proBNP 1-108. ProBNP may be glycosylated post-translation at several sites in its N-terminus to a variable degree,10,11 and glycosylation at amino acid 71 threonine appears to be involved in the regulation of proBNP processing by furin. 12 Subsequently, proBNP is cleaved by prohormone convertases, such as furin and corin, to release the 76-amino acid N-terminal portion NT-proBNP 1-76, and the biologically active C-terminal 32-amino acid molecule BNP 1-32 (see Figure 4). The cleavage site is located between amino acids 76 and 77. Furin is a membrane-associated endopeptidase, and in contrast to corin it is ubiquitously found in various tissues. An increase in furin activity in the blood of acutely decompensated HF patients as well as a decrease in proBNP glycosylatioin have been reported. 13 Thus, some processing of proBNP can occur in the blood as well. It has been recognised that both BNP and NT-proBNP are modified into a mixture of various fragments in the blood (see Figure 3). At the mid-region of NT-proBNP little proteolytic degradation occurs. 8 Intact circulating proBNP, glycosylated NT-proBNP and glycosylated proBNP have been observed in HF patients.11,14 Only a small portion of BNP circulates as the full-length BNP 1-32, and plasma from HF patients contains diverse degraded forms truncated from the N and C-terminal end (e.g. BNP 3-32, 5-31, 8-31, 1-25, 1-26). 15
Due to short in-vitro half life, ANP itself turned out to be not suitable for routine diagnostics, but NT-proANP or mid-regional proANP, BNP and NT-proBNP are all suitable routine laboratory biomarkers for HF.16–20 The N-terminal fragments from the prohormones can serve as a surrogate marker for the actual natriuretic hormone.
NP clearance and possible interferences of sacubitril
NP clearance has recently been reviewed by Potter. 5 In brief, ANP clearance is rapid (half-life approximately 2 minures) compared with BNP (half-life approximately 20 minures) in men. Clearance of NPs occurs by two major mechanisms, that is, enzymatic extracellular degradation by neprilysin and intracellular degradation by insulin-degrading enzymes, as well as by binding to the NP receptor C. The primary role of this receptor, which is expressed in many tissues, is to clear NPs by internalisation and degradation (see Figure 1). It binds all three NP family members. Insulin degrading enzyme is a cytosolic enzyme, which is also found in membrane preparations. It initially cleaves ANP and BNP outside the ring. ANP and CNP are much better insulin degrading enzyme substrates than BNP. 21 Neprilysin is a zinc-containing, membrane-bound, ectoenzyme that cleaves various peptide substrates including insulin β-chain, β-amyloid and various peptide hormones of relevance in HF, such as angiotensin II, endothelin-1, bradykinins, substance P, adrenomedullin, calcitonin gene-related peptide and NPs. 5 Neprilysin is widely expressed, for example, in kidneys, lungs and vascular endothelial cells, and can be released from the cell surface yielding soluble neprilysin with catalytic activity. 22 Neprilysin cleaves ANP and CNP at the cysteine–phenylalanine bond and breaks the ring structure, which eliminates receptor binding. Human BNP is a poorer substrate for neprilysin and is not cleaved at the conserved cysteine–phenylalanine bond. 23 Neprilysin inhibitors failed to block BNP degradation by human kidney membranes. 24 Human BNP is also a poor substrate for insulin degrading enzyme, suggesting that another yet unidentified leupeptin-sensitive protease may be mainly responsible for its catabolism. 25
Clinical results in men: reported effects of sacubitril-valsartan treatment on NP concentrations
Oral neprilysin inhibitors elevate NP system activity as assessed by increases in plasma and urine cGMP concentrations in humans.26,27 As discussed above this effect may rely more on ANP than BNP because neprilysin plays a more significant role in ANP degradation, whereas human BNP is relatively resistant to neprilysin degradation.5,23,24 The known effects of oral sacubitril-valsartan treatment on neuroendocrine hormones are an increase in plasma ANP in dogs, 26 and a dose-dependent increase (maximum approximately 4 hours after oral administration) in plasma cGMP (up to an average of approximately 40% in a dose escalating study). These data provide evidence for the biological activity of the agent in healthy human volunteers, 26 with increases in NP system activity, 28 renin concentrations and activity and angiotensin II.
In the PARADIGM-HF study,1,27 plasma BNP and urinary cGMP concentrations were significantly higher in the sacubitril-valsartan group at 4 weeks and at 8 months in association with markedly better outcomes than in the enalapril group. This was suggested to reflect apparent NP system augmentation. However, the observed relative average BNP increase was small compared with the cGMP increase (on average only about 10% versus 90%, respectively). In contrast, NT-proBNP and cardiac troponin T were significantly lower (average decline of about 30% and 20%, respectively) in the sacubitril-valsartan group reflecting a sustained reduction in cardiac wall stress and associated myocardial injury. The population in the study was composed of chronic systolic HF patients with mild to moderate symptoms (70% New York Heart Association class II, left ventricular ejection fraction <40%, mean 30%). It was those with class II HF who seemed predominantly to benefit.
In the earlier PARAMOUNT trial, 29 in which sacubitril-valsartan was studied in patients with chronic HF and preserved ejection fraction, there was a significant and greater decline in NT-proBNP (on average about 25%) 12 weeks after treatment compared to valsartan alone, which was associated with left atrial reverse remodelling and improvement in symptoms at 36 weeks. In that trial patients were required to have a NT-proBNP greater than 400 ng/l at screening. There was a rapid (at 4 weeks) and sustained decline in NT-proBNP at 36 weeks, but at 36 weeks the difference between both treatment groups was no longer statistically significant. 29
It should be noted that in both large clinical trials, BNP and NT-proBNP were measured with assays from only one manufacturer each, which has limitations (see below). To date, ANP and NT-proANP results have not been reported in humans taking sacubitril-valsartan. In addition, it appears that marked BNP elevations inhibit endogenous circulating neprilysin activity. 22 This supports the important role of the hormonal feedback system to protect against severe cardiac stress by reducing degradation of NPs and other vasoactive peptides of importance in HF. This may be a partial explantation for why neprilysin inhibition may be more effective in milder HF as in the PARADIGM trial. 1 In summary, all these reported study findings are consistent with an augmentation of NP family activity by sacubitril-valsartan treatment. However, reported average BNP and NT-proBNP changes, although statistically significant, were within the known relatively large week-to-week biological variation of these biomarkers.30,31
Reported results of NP testing in clinical studies of sacubitril: limitations and analytical pitfalls of interpretations due to non-specific nature of the current commercial BNP and NT-proBNP immunoassays
These issues are complex 32 and may not be of great relevance for the use of NPs as laboratory markers of HF. They are, however, important from a pathophysiological and pharmacological point of view. Immunoassays rely on antibodies that measure an epitope within the target molecule and not necessarily the actual full peptide. Thus, antibodies to NT-proANP and ANP immunoassays often have cross- reactivities with proANP and its fragments. For example, the commercially available so-called mid-regional proANP assay detects this peptide as a fragment, in intact NT-proANP, and proANP as well. 33 BNP immunoassays are also heterogenous and measure both proBNP and BNP as well as BNP breakdown products with varying assay dependent cross-reactivities. 34 BNP peptides do not substantially cross-react with NT-proBNP assays, and NT-proBNP peptides do not substantially cross-react with BNP assays. However, there is substantial assay-specific cross-reactivity of proBNP with commercial BNP and NT-proBNP assays. 34 The cross-reactivity of the commercial NT-proBNP assay with NT-proBNP and proBNP is dependent on the degree of glycosylation of both molecules, because glycosylation inhibits the assay’s antibody binding.10,14 Thus a significant amount of circulating NT-proBNP and proBNP may be missed in individual patients. 14 Therefore, to obtain a better understanding of the effects of sacubitril-valsartan on BNP the marker should be measured with additional assays that detect different epitopes on BNP, and NT-proBNP should be evaluated in deglycoslytated samples. Research immunoassays for measuring total NT-proBNP, total BNP and the total sum of proANP derived peptides have been developed.6,13–15,35 It is therefore important to consider the assay cross-reactivities when interpreting the data from these clinical studies.27,29 Because of the cross-reactivity of proBNP with BNP immunoassays and the effects of NT-proBNP glycosylation on recovery of circulating forms, drug-induced changes in proBNP glycosylation and furin and corin-mediated cleavage may not be reflected by changes in BNP and NT-proBNP immunoassay test results.
Thus, future clinical trials should consider these analytical limitations and should measure BNP with at least two commercial assays using different BNP antibodies, or ideally also test for ‘total BNP’ and/or ‘total NT-proBNP’ using research assays. 32 ANP and NT-proANP/proANP changes induced by sacubitril-valsartan in men still need to be investigated in more detail in clinical trials, which is also true for CNP changes.
Implications of sacubitril-valsartan for NP testing in clinical practice
Measurement of NPs plays a significant role in the assessment of HF patients.16,17 Their main clinical routine application in acute cardiac care is for the the rapid rule-out of acute HF in patients evaluated for acute dyspnoea. Using decision limits of 100 ng/l (BNP), 300 ng/l (NT-proBNP) and 120 pmol/l (mid-regional proANP) they have high negative predictive values (90–98% in a meta-analysis).16,17,34 However, the positive predictive values for all three NPs for HF are less robust (56–67%).16–20,36 Therefore, a second markedly higher rule-in cut-off is frequently recommended to increase clinical specificity for HF,16,36 leaving an obligtory grey area in which diagnostic accuracy is limited. In addition, NP increases are also found in a variety of other diseases including renal failure. 16
In addition, in acute HF NP value decreases from admission to predischarge are useful for risk stratification. Decreases of more than 30% of baseline values are a marker of good prognosis.37,38 In addition, the absolute predischarge value also has prognostic significance.38,39
Despite the above discussed possible analytical limitations, based on the recent data on the effects of sacubitril-valsartan on BNP and NT-proBNP, the interpretation of NT-proBNP testing in HF appears to be unaffected by neprilysin inhibition. It is also unlikely that the diagnostic utility of BNP testing will be significantly impaired by this new drug as usually patients suspected of having HF without established HF will not be treated before proof of diagnosis. Chronic HF patients or hypertensive patients on sacubitril-valsartan treatment developing HF symptoms may be challenging without knowing their previous BNP baseline values. However, the relative increases in BNP plasma concentrations reported in the PARADIGM HF trial 27 were modest (median baseline BNP value approximately 200 ng/l to a median of about 225 ng/l in the sacubitril-valsartan arm). BNP concentrations greater than 500 ng/l, the frequently used rule-in decision limit for HF,16,36 were rare (75% percentile of BNP concentrations in the sacubitril-valsartan arm approximately 450 ng/l). Thus, the high negative predictive value for the exclusion of acute HF for BNP testing will be maintained in patients with sacubitril-valsartan treatment. The positive predictive value of the rule-in cut-off of 500 ng/l may, however, be reduced to some extent and the proportion of patients with grey zone BNP values is likely to increase.
In contrast, for treatment monitoring of chronic HF patients on sacubitril-valsartan the current concept of the lower the BNP test result the better the prognosis may no longer be true. New BNP assay specific cut-offs for risk stratification may need to be derived for BNP testing in ongoing clinical HF trials with sacubitril-valsartan. One could even suggest using an increase in BNP to define who might respond to sacubitril-valsartan or to assess patient compliance. However, after an initial rise, which is markedly smaller than in the case of cardiac decompensation, BNP may reach a new steady state during sacubitril-valsartan treatment and then begin to drop long term, if marked clinical improvement occurs. Undoubtedly, more clinical data are needed. From the perspective of following patients with serial values, it appears that NT-proBNP testing may be superior for monitoring patients taking sacubitril-valsartan as the current concept of the lower the better appears to be still valid. The potential of the BNP/NT-proBNP ratio (BNP possibly reflecting the action of the drug and NT-proBNP reflecting the effects of the drug on the heart) for chronic HF monitoring with sacubitril-valsartan also remains to be further investigated.
It is tempting to speculate that NT-proANP/mid-regional proANP behaves in a similar way to NT-proBNP without impairment of its diagnostic and prognostic utilities in HF patients, but no data have been published so far, and this still remains to be demonstrated.
Conclusion: critical clinical concepts
The clinical utility of BNP testing to rule out HF rapidly will not be negatively impaired by sacubitril-valsartan treatment.
The clinical interpretation of NT-proBNP test results in patients with HF is unaffected by neprilysin inhibition based on the currently published data.
Available data suggest that the concept of the lower the BNP test result the better the prognosis in treatment monitoring of chronic HF may no longer be true for patients on sacubitril-valsartan. This concept appears to be maintained for NT-proBNP testing in chronic HF.
Analytical pitfalls of commercial BNP and NT-proBNP assays have to be considered in the design of future clinical trials, particularly when testing the hypothesis that the action of sacubitril-valsartan is reflected by BNP concentrations and the effects on the heart are reflected by NT-proBNP concentrations.
Footnotes
Conflict of interest
During recent years JM received consulting fees from Philips Health Care Incubator and lecture fees from Roche Diagnostics.
BL received research support from bioMerieux and Fiomi, as well as speaker/consulting honoraria from bioMerieux, Roche, Radiometer, Philips, ThermoFisher and Fiomi.
EG received honoraria for lectures from Roche Diagnostics, BRAHMS ThermoFisher and Mitsubishi Chemical Europe. He has received an institutional research grant from Roche Diagnostics and serves as a consultant for Roche Diagnostics and BRAHMS ThermoFisher.
KH received lecture fees From Novartis.
MP received consulting fees from Roche Diagnostics, Abbott Diagnostics and Siemens Health Care Diagnostics.
MM received lecture and consulting fees from Novartis, Roche Diagnostics and BRAHMS ThermoFisher, and research grants from Roche Diagnostics and BRAHMS ThermoFisher.
CM received research grants from the Swiss National Science Foundation and the Swiss Heart Foundation, the European Union, the Cardiovascular Research Foundation Basel, 8sense, Abbott, Astra Zeneca, ALERE, BRAHMS ThermoFisher, Critical Diagnostics, Nanosphere, Roche, Siemens, Singulex, Sphingotec and the University Hospital Basel, as well as travel support or speaker/consulting honoraria from Abbott, ALERE, Astra Zeneca, BG medicine, Biomerieux, BRAHMS, Cardiorentis, Daiichi Sankyo, Lilly, MSD, Novartis, Pfizer, Roche, Siemens and Singulex.
ASJ has or presently consults for Abbott, Alere, Roche, Radiometer, Siemens, Beckman, Trinity, ET Healthcare, Dart Neurosciences, Lpath, Diadexus, Novartis and ![]() .
.
KT has no conflicts of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.