
Abstract
Background:
While contributors to system delay in ST-elevation myocardial infarction (STEMI) are well described, predictors of patient-related delays are less clear. The aim of this study was to identify predictors that cause delayed diagnosis of STEMI in a metropolitan system of care (VIENNA STEMI network) and to investigate a possible association with long-term mortality.
Methods:
The study population investigated consisted of 2366 patients treated for acute STEMI in the Vienna STEMI registry from 2003–2009. Multivariable regression modelling was performed for (a) onset of pain to first medical contact (FMC) as a categorical variable (pain-to-FMC⩽60 min versus >60 min: ‘early presenters’ versus ‘late presenters’); and for (b) onset of pain-to-FMC (min) as a continuous variable.
Results:
After multivariable adjustment, female sex (odds ratio (OR) 1.348; 95% confidence interval (CI) 1.013–1.792; p=0.04) and diabetes mellitus (OR 1.355; 95% CI 1.001–1.835; p=0.05) were independently associated with late presentation in STEMI patients, whereas cardiogenic shock (OR 0.582; 95% CI 0.368–0.921; p=0.021) was a predictor of early diagnosis. When onset of pain-to-FMC was treated as a continuous variable, female sex (p=0.003), anterior infarction (p=0.004) and diabetes mellitus (p=0.035) were independently associated with longer delay, while hyperlipidaemia (p=0.002) and cardiogenic shock (p=0.017) were strong predictors of short pain-to-FMC times. Three-year-all cause mortality was 9.6% and 11.3% (p=0.289) for early and late presenters, respectively. After adjustment for clinical factors (sex, age, diabetes, current smoking, hypertension, hyperlipidaemia, cardiogenic shock and location of myocardial infarction) only a trend for increased risk of all-cause death was observed for longer pain-to-FMC times in a cox regression model (hazard ratio (HR) 1.012; 95% CI 0.999–1.025 for every 10 min of delay; p=0.061). Interestingly, early presentation within one hour of symptom onset was not associated with three-year mortality survival (HR 1.031; 95% CI 0.676–1.573; p=0.886).
Conclusion:
In this all-comers study of STEMI patients in the VIENNA STEMI network, cardiogenic shock was the strongest predictor of short patient-related delays, whereas a history of diabetes and female sex were independent associated with late diagnosis in STEMI. After adjustment for clinical confounders, patient related delay did not significantly impact on long-term all-cause mortality.
Keywords
Background
Current guidelines recommend timely reperfusion for patients with ST-segment elevation myocardial infarction (STEMI).1,2 Accordingly, time from first medical contact (FMC) to wire passage into the culprit artery should not exceed 120 min (90 min are recommended in early presenters within three hours, 60 min in very early presenters within one hour) if reperfusion strategy is primary percutaneous coronary intervention (PPCI). This circumstance, also referred to as system delay was shown to be associated with short- and long-term mortality in patients with STEMI undergoing PPCI.3,4 System delay is regarded as modifiable 5 and serves as an indicator for quality of care in a STEMI network. 6 All STEMI networks are encouraged to document and disclose system delay on a regular base. 1 Previous studies identified factors predictive of door-to-balloon times in patients with STEMI.7,8
In contrast, few studies focused on patient-related delay (onset of pain to FMC (pain-to-FMC)) and relationship with mortality. Essentially, pre-hospital delay times remained more or less unchanged over the last decades in the USA 9 and Europe. 10 In this regard, the effectiveness of public campaigns to shorten patient-related delays has been doubted. 11 While factors predicting system delay are well investigated, 8 contributors for patient-related delay are less clear. Low neighbourhood household income, 12 certain geographic regions, advancing age, and medical history of either angina, diabetes, or hypertension, 13 and female sex 10 were associated with pre-hospital delay in previous studies. Most importantly, the association of patient-related delay and long-term outcome has not been reported efficiently as pain-to-FMC effects survival is still an ongoing matter of debate. 14 The aim of this study was to identify predictors of patient-related delay in our metropolitan VIENNA STEMI system of care and to investigate its potential impact on long-term mortality.
Methods
Patients
The Vienna STEMI network in its present form was established in 2003 with a rotation principle between five non-academic hospitals and the Medical University of Vienna offering a 24-hour PPCI service on a routine basis (on-call) for patients with acute STEMI. The observational Vienna STEMI registry was established to include an all-comers population presenting with STEMI in the metropolitan area of Vienna with roughly two million inhabitants. The study population consisted of 2366 patients with STEMI enrolled from January 2003–December 2009 (Figure 1). Patients presenting within the first 12 h of symptom onset who were directly referred for PPCI (excluding those with initial thrombolytic therapy) and in whom delay times were documented were eligible for the present analysis. Patients with unclear symptom onset were excluded.
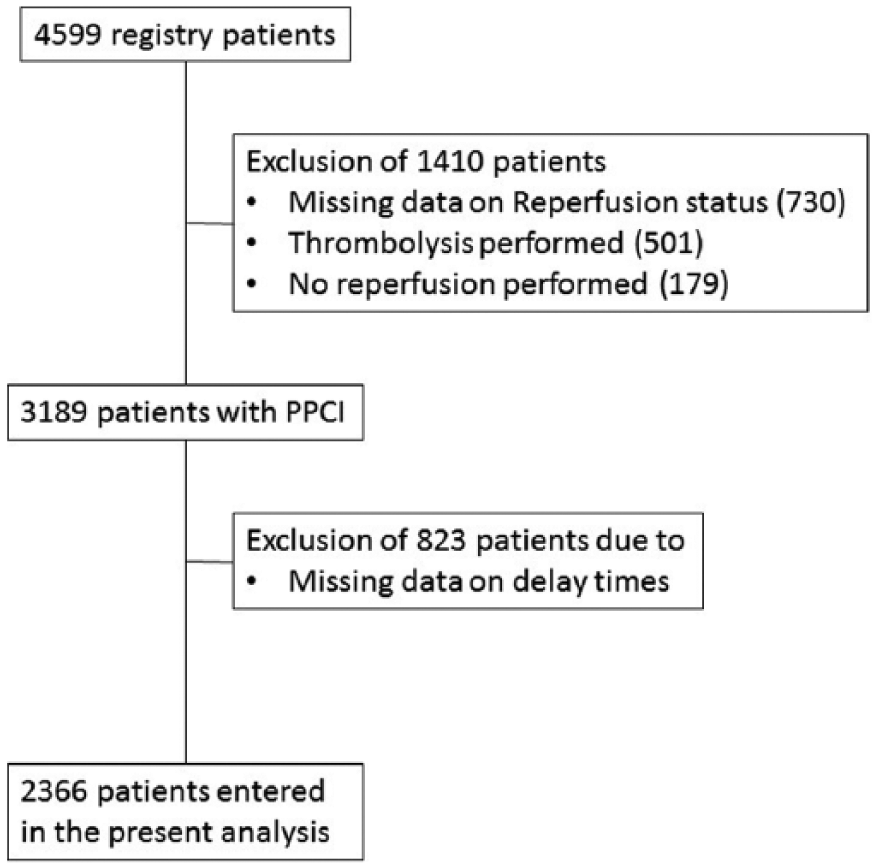
Patient flowchart. PPCI: primary percutaneous coronary intervention.
STEMI was diagnosed according to the European Society of Cardiology (ESC) guidelines valid at time of enrolment (2003–2009).15,16 Briefly, criteria for STEMI were evidence of ST-segment elevation of 1 mm or more in two or more contiguous leads. In all cases, typical increases of necrosis markers were found during hospital stay (but evaluation of biomarkers was not a prerequisite for diagnosis and treatment strategy). Cardiogenic shock was diagnosed by the local investigators in case of clinical signs of reduced cardiac output and systolic blood pressure less than 90 mm Hg without use of inotropes or vasopressors, or as the necessity for vasopressors. Infarct location was categorised as anterior or non-anterior according to electrocardiogram (ECG) and angiographic findings. All charts were reviewed by trained study personnel to extract medical history and risk factors from the registry data set. All patients received contemporary background therapy consisting of aspirin, P2Y12-inhibitor, ACE-inhibitor/angiotensin-receptor-blocker, beta-blockers and statins. The study was performed according to the Helsinki Declaration and approved by the local ethics committee.
Delay times
Delay times were evaluated at presentation at the PCI-hospital by interrogation of the patient, his/her relatives or emergency physicians, and by reviewing available medical records. Onset of pain was defined as first recognition of chest pain responsible for the call into the STEMI system (emergency number 144). FMC was defined as the time when the diagnostic ECG was performed and diagnosis of STEMI was confirmed. This happened in the majority of patients pre-hospitally (by well-trained physicians) or in cases of self-comers in the emergency departments of Viennese hospitals. Patients were termed ‘early presenters’ if time from symptom onset to diagnosis (pain-to-FMC) was 60 min or less. Patients were termed ‘late presenters’ if time from symptom onset to diagnosis exceeded 60 min.
Outcome
All-cause mortality data were obtained from Death Statistics Austria, an independent and non-profit federal institution under public law that supports scientific services. Cases of death occurring in Austria are centrally recorded by Statistics Austria and data are made available for authorised institutions upon request. For the respective query, patient’s name, birth date and gender were matched with the national database in order to identify events of death.
Statistical methods
Descriptive statistics were performed on baseline variables and stratified by time from pain-to-FMC, i.e. early presenters versus late presenters. Discrete characteristics are expressed as frequency counts and percentages, and differences between groups were determined by the Chi-square test. Continuous characteristics are expressed as means with standard deviations or medians and quartiles, where appropriate. Differences were examined using the Mann-Whitney test for comparison. For each risk factor, cumulative hazard for time to presentation (pain-to-FMC time) was analysed by means of Breslow test (i.e. observed versus expected min to diagnosis). Log rank testing was used for unadjusted comparison of three-year survival between early and late presenters and a Cox regression model was set up for adjusted impact of early presentation (as categorical variable) and longer pain-to-FMC (as continuous variable) on long-term outcome. Two models were established in order to investigate an association between baseline variables and pain-to-FMC:
Model 1. Pain-to-FMC was entered into a logistic regression model as the dependent variable in a categorical fashion, i.e. early presentation ⩽60 min versus late presentation >60 min. Multivariable modelling was performed with step-wise backward elimination of variables using a likelihood ratio test with p-value for entry of 0.05 and p-value for removal of 0.15. 17 The following variables were entered into the model: sex, age, diabetes, current smoking, hypertension, hyperlipidaemia, shock and location of MI.
Model 2. Pain-to-FMC was entered as a continuous variable into a linear regression model, backward elimination was performed as mentioned above. The level of significance used for all tests was a two-sided p-value of 0.05.
Calculations were performed using SPSS 22, IBM for Windows.
Results
Predictors of early diagnosis of STEMI
A total of 2366 individuals presenting with STEMI from January 2003–December 2009 fulfilled the criteria for the final analysis (Figure 1). Baseline characteristics are shown in Table 1. Median time from symptom onset to FMC was 91 (interquartile range (IQR): 53–180) min. Total ischaemic time was 225 min (145–364) for the entire cohort, and 153 (112–225) versus 280 min (202–423), for early and late presenters respectively (p<0.001).
Baseline characteristics.
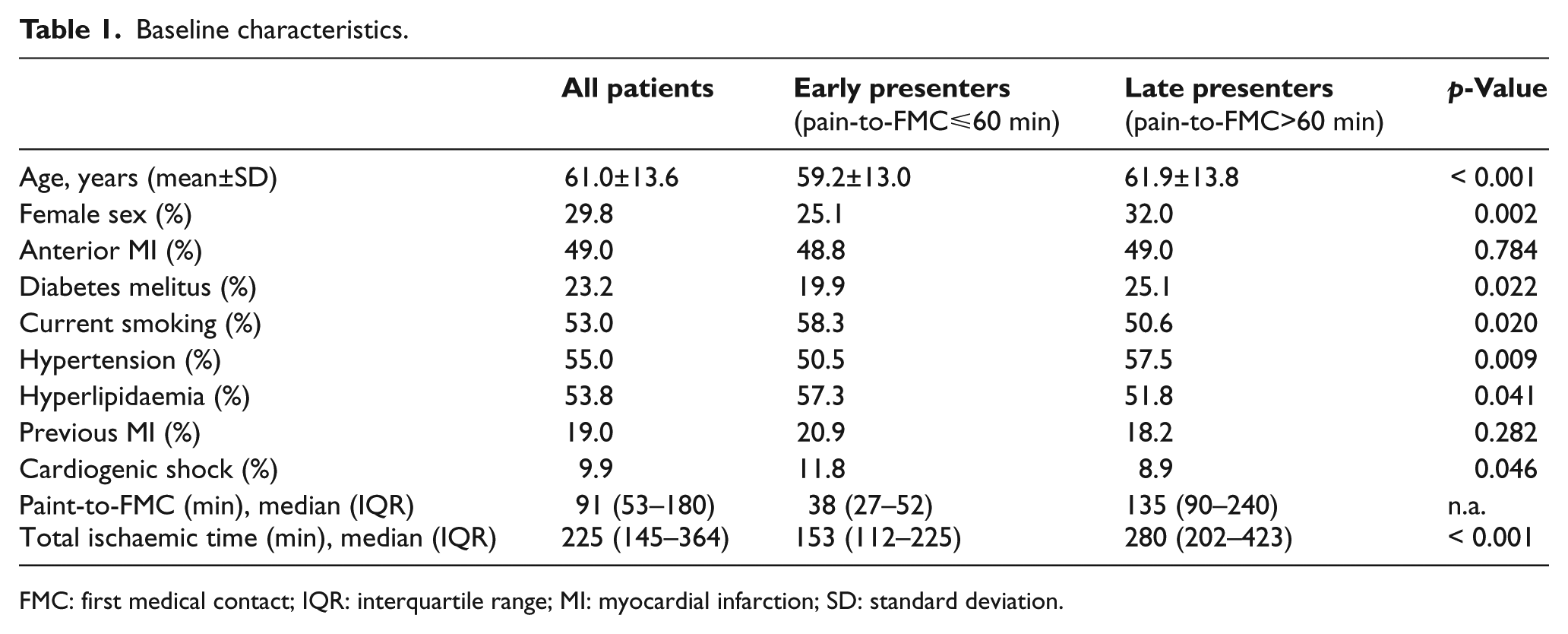
FMC: first medical contact; IQR: interquartile range; MI: myocardial infarction; SD: standard deviation.
In total 771 (32.6%) patients were diagnosed within the first hour of symptom onset and, thus, were classified as early presenters. These patients were younger, more frequently male and more likely to have a history of smoking or hyperlipidaemia (Table 1). The incidence of cardiogenic shock was significantly more frequent in early presenters (11.8% versus 8.9%, p=0.046). In contrast, diabetes and hypertension were significantly more prevalent in late presenters, while history of MI and infarct location did not differ between the two groups in univariable analysis. Pain-to-FMC was shorter for males (p=0.001), non-diabetics (p=0.006), patients with known dyslipidaemia (p=0.003), and age below 75 years (p<0.001) when analysed as a continuous variable. No significant association with pain-to-FMC was found for infarct location and cardiogenic shock in this unadjusted analysis.
Upon multivariable adjustment in Model 1, female sex (OR 1.348; p=0.04) and diabetes mellitus (OR 1.355; p=0.05) were independently associated with late presentation in STEMI, whereas cardiogenic shock (OR 0.582; p=0.021) was a predictor of early diagnosis (Table 2). When pain-to-FMC was entered as a continuous variable (Model 2) female sex (p=0.003), anterior infarction (p=0.004) and diabetes mellitus (p=0.035) were independently associated with longer delay, while hyperlipidaemia (p=0.002) and cardiogenic shock (p=0.017) were strong predictors of short pain-to-FMC times (Table 3).
Predictors of late presentation (pain-to-first medical contact >60 min) multivariable analysis (adjusted for age, infarct location, current smoking, hypertension).
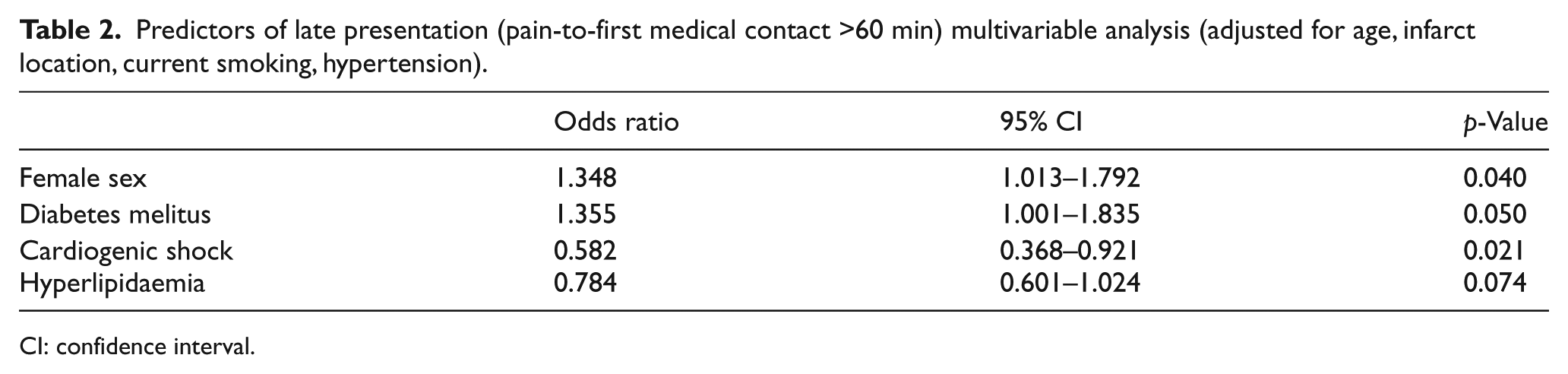
CI: confidence interval.
Predictors of longer pain-to-first medical contact (FMC) delay multivariable analysis (adjusted for age, infarct location, current smoking, hypertension).
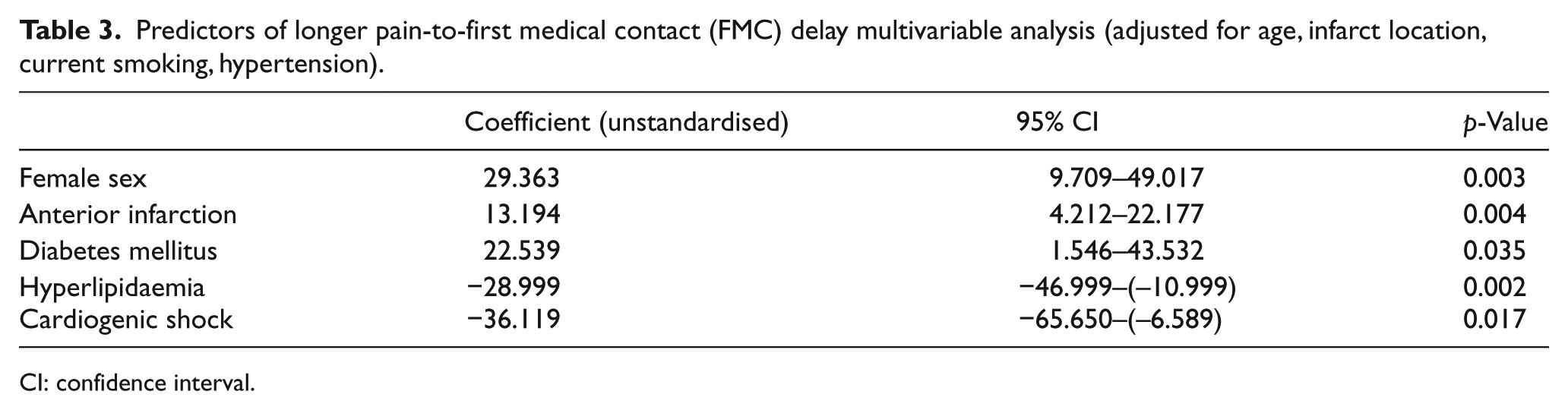
CI: confidence interval.
Mortality
Overall three-year-all-cause-mortality was 10.8% for the entire cohort of STEMI patients presenting within 12 h of symptom onset (9.6% and 11.3% (log rank: p=0.289) for early and late presenters, respectively). Kaplan-Meier plots are shown in Figure 2. Upon adjustment for well-established risk factors and confounders in Model 2 (sex, age, diabetes, current smoking, hypertension, hyperlipidaemia, shock and location of MI), a trend for increased rates of all-cause death was observed with every 10 min of longer pain-to-FMC delays after three years of follow-up (HR 1.012; 95% CI 0.999–1.025; p=0.061). However, early presentation ⩽60 min (Model 1) was not associated with three-year outcome (OR 1.031; 95% CI 0.676–1.573; p=0.886; Figure 2(c)).
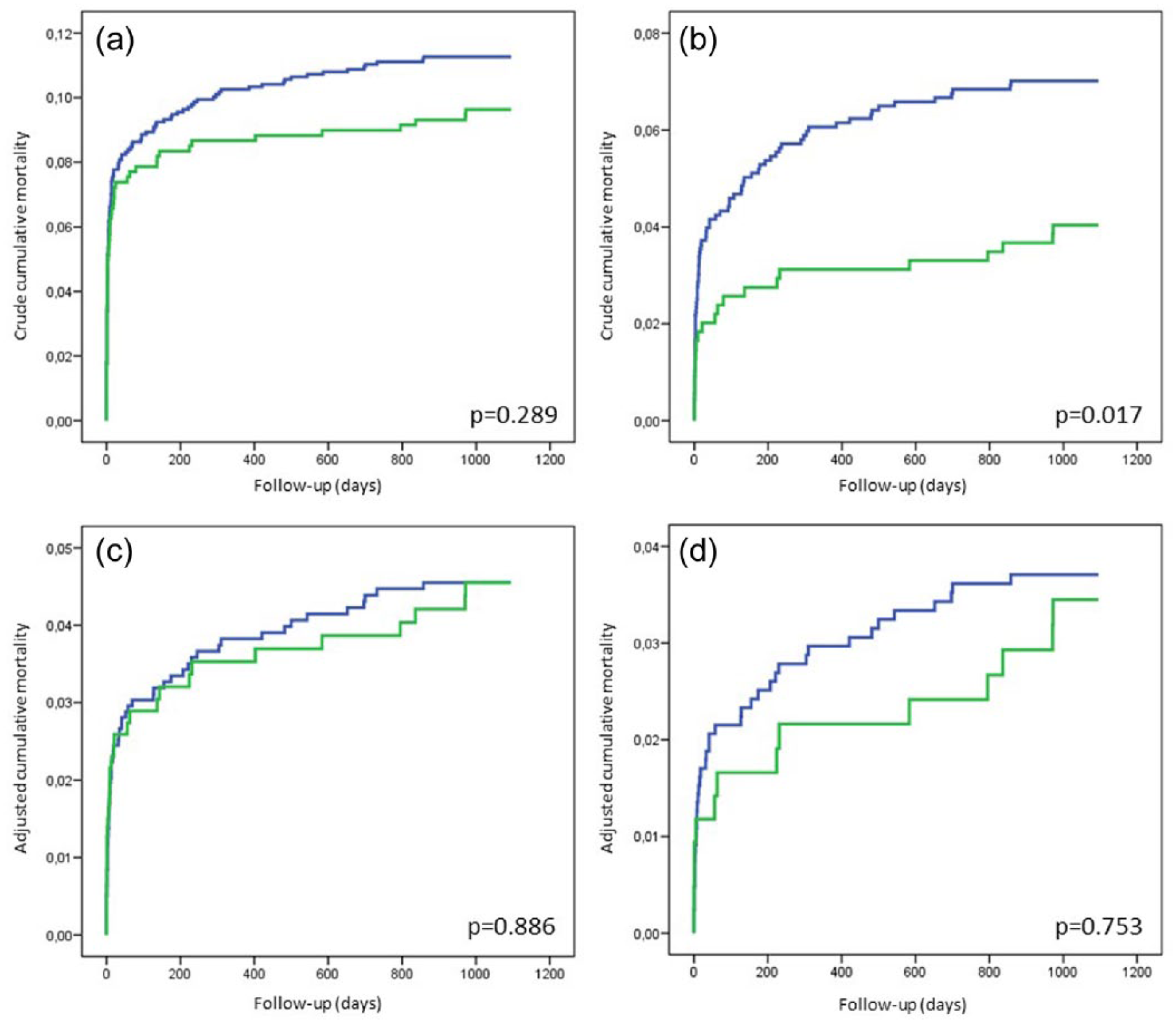
Survival curves. Kaplan Meier plots and adjusted long-term all-cause mortality (Cox model) for all patients ((a), (c)) and after exclusion of patients with cardiogenic shock ((b), (d)) for early (green) and late presenters (blue).
In a complementary approach, patients with cardiogenic shock were excluded from outcome analysis to assess the impact of diagnostic delay in haemodynamically stable patients. In these patients, three-year-mortality was significantly lower in patients with early compared to late diagnosis (4.0% versus 7.0% respectively (log rank: p=0.017), Figure 2(b)). After adjustment for the mentioned confounders neither longer pain-to-FMC (HR 1.010; 95% CI 0.993–1.027; p=0.255 for every 10 min increase), nor late presentation >60 min (HR 1.103; 95% CI 0.598–2.037; p=0.753; Figure 2(d)) were associated with adverse outcome in this subgroup of patients with STEMI not complicated by cardiogenic shock.
Discussion
As the main findings of our study, we were able to demonstrate that (a) cardiogenic shock was the strongest predictor of short patient-related delays, whereas (b) a history of diabetes or female sex were associated with late diagnosis of STEMI, and, interestingly, (c) after adjustment for other risk factors, patient-related delay did not significantly impact on long-term survival. The Vienna STEMI registry incorporates real-life data from a metropolitan area of two million people over a decade of years. These all-comers data are of importance since major subgroups, such as females, the elderly and haemodynamically compromised patients are usually under-represented in randomised controlled trials for legal reasons (childbearing potential, inability to give consent at presentation). Of note, these subgroups are important contributors to patient-related delay in STEMI, according to our analysis. Former studies mainly investigated predictors of system-related delays or pre-hospital delays in STEMI. In the present work. we exclusively focus on predictors of patient-related delay, i.e. time from symptom onset to FMC.
Cardiogenic shock
In the Worcester Heart Attack Study cardiogenic shock was reported as a predictor of early arrival in the emergency department (ED) in univariable analysis, but unfortunately the adjusted impact of shock on ED arrival was not reported. 9 Our results indicate that the presence of cardiogenic shock is the strongest predictor of early presentation after adjustment for other risk factors. In a large American registry, Killip class IV was similarly associated with the shortest prehospital delay times, however, mortality rates were not reported. 18 As mechanistic background, patients (or their relatives) perhaps recognise symptoms of myocardial infarction faster and react quicker in case of commencing or manifest haemodynamically instability.
Diabetes mellitus
In the present study a history of diabetes was an independent predictor of late diagnosis of STEMI. Longer onset of pain-to-hospital arrival times in diabetics were shown in clinical trials 7 as well as in registries. 13 Interestingly, diabetes was not a predictor of atypical symptoms in acute myocardial infarction (AMI) in a Swedish registry. 19 Although the type of symptom was not specifically documented in our study, we suspect that less impressive pain and atypical locations might have contributed to a later call into the system.
Female sex
In the American National Registry of Myocardial Infarction the co-incidence of female sex, diabetes and older age was associated with an increase of time to hospital presentation of up to 50 min 20 when analysed as a combination of characteristics. This is in contrast to our data, as female sex and diabetes independently predicted late presentation while advanced age did not. Female sex (29.8% in our registry) was associated with delayed diagnosis also after multivariable adjustment. It is well known that women present with atypical symptoms of MI more often, which may result in longer pre-hospital delays. In a population-based registry, female sex was significantly associated with misinterpretation of MI related symptoms: only 46.0% of women but 51.7% of men correctly attributed their symptoms to the heart. 21
Age
As discussed previously, higher age did not serve as an independent predictor of prolonged patient related-delay in our hands. Although we observed a significant association between advancing age and late presentation after symptom onset in univariable analysis, this finding was abolished after adjustment for other risk factors, which confirms recent data from Peng and colleagues. 22 In contrast, advancing age was associated with prolonged delay In the Worcester Heart Attack Study. 9 This study also included patients with non-Q-wave infarction or non-STEMI, which does not allow direct comparison with our study. It might be a matter of defining the elderly (>75 or >80 or more?) when a similar outcome between studies is expected. Moreover, elderly patients that have been described in other publications might suffer from different co-morbidities, which might have different impact on symptom recognition.
All-cause mortality
Our data exhibited a significant reduction of unadjusted long-term mortality with shorter patient-related delay in STEMI patients with stable haemodynamics while for the total cohort of patients, including those with cardiogenic shock, impact of pain-to-FMC on long-term survival no longer reached statistical significance. The later might be explained by the higher mortality rate in shock patients who were overrepresented in the early presenters, and underlines the important impact of haemodynamic conditions on outcome in this early phase after symptom onset. Our data are similar to recent analyses demonstrating that, against hypothetical considerations that time is muscle, 23 a reduction of time delays has no impact on long-term outcome, as shown for door-to-balloon times24,25 Our results are also in line with pooled data from randomised trials suggesting no significant increase in the cardiac event rate with increasing time to presentation after mechanical reperfusion, in contrast to thrombolytic therapy when time to reperfusion seems more important for clinical outcome. 26 Finally, our study was slightly underpowered for outcome given the low long-term mortality-rate in the era of PPCI. Nevertheless, we observed a strong trend for increased rates of all-cause mortality with every 10 min of prolonged pain-to-FMC delays, which was, however, not statistically significant.
Strengths and limitations
Several limitations of the present study need to be considered: Firstly, we only included patients with PPCI in the present study, therefore our results cannot be transformed to STEMI patients who receive pharmacological reperfusion, or no reperfusion strategy at all. Secondly, it is possible that a distinct group of very high-risk patients or patients in shock died prior to arrival at the PCI hospital and therefore were not entered into the registry. However, the rate of cardiogenic shock is within the range of other registries, indicating a representative sample.27,28 Thirdly, registry data are prone to entry bias and data quality is usually lower as opposed to clinical trials. Strengths of the current analysis include the fact that we were able to follow all our patients, that women, elderly, diabetics or patients in cardiogenic shock, who are often underrepresented in clinical trials, have been included in this all-comers analysis. These high-risk characteristics – as shown in our present work – are the most important factors predicting patient-related delays in STEMI. Moreover, all-cause mortality, as presented in here is a hard and definite endpoint unsusceptible to individual misjudgement.
Conclusion
In this observational registry-based study female sex and diabetes were associated with longer patient-related delays in STEMI, whereas cardiogenic shock was the strongest predictor for short pain-to-FMC delay. We observed no significant impact of short versus prolonged patient delay times on all-cause mortality in the Vienna STEMI network, which might be explained among other possibilities by the overrepresentation of cardiogenic shock in early presenters. As female patients, diabetics and patient in cardiogenic shock are usually underrepresented in randomised clinical trials, partially also for legal reasons, our data reflect a real-world setting and contribute to a better understanding of impact of patient-related delays, on hard clinical endpoints in STEMI networks.
Footnotes
Acknowledgements
The authors had full access to the data and take responsibility for its integrity. All authors have read and agreed to the manuscript.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the study was supported by the Ludwig Boltzmann Cluster for Cardiovascular Research, Vienna, and the Association for the Promotion of Research in Arteriosclerosis, Thrombosis and Vascular Biology (ATVB), Vienna.