
Abstract
Aims:
Current guidelines for patients with non-ST-elevation acute coronary syndrome (NSTE-ACS) recommend early invasive treatment in intermediate-to-high risk patients based on medical history, electrocardiogram (ECG) and elevated troponin. Patients with normal levels of cardiac troponin measured with a high-sensitivity method (cTnT-hs) might not benefit from early invasive procedures.
Methods and results:
In this Prospective Randomized Platelet Inhibition and Patient Outcomes (PLATO) blood-core substudy, 1232 patients presented with NSTE-ACS had a high sensitivity cardiac troponin T (cTnT-hs) level <99th percentile (<14 ng/l) at randomisation. The outcomes in relation to a planned invasive (n=473) vs planned conservative treatment (n=759), were evaluated by adjusted Cox proportional hazard analyses. In patients with a normal cTnT-hs at randomisation, regardless of randomised treatment, a planned invasive vs conservative treatment was associated with a 2.3-fold higher risk (7.3% vs 3.4%, p=0.0028) for cardiovascular (CV) death or myocardial infarction (MI), driven by higher rates of procedure-related MI (3.4% vs 0.1%), while there were no differences in rates of CV death (1.3% vs 1.3%, p=0.72) or spontaneous MI (3.0% vs 2.1%, p=0.28). There were significantly more major bleeds (hazard ratio (HR) 2.98, p<0.0001), mainly due to coronary artery bypass graft (CABG)-related (HR 4.05, p<0.0001) and non-CABG procedural-related major bleeding events (HR 5.31, p=0.0175), however there were no differences in non-procedure-related major bleeding (1.5% vs 1.9%, p=0.45). Findings were consistent for patients with a normal cTnI-hs at randomisation.
Conclusions:
In patients with NSTE-ACS and normal cTnT-hs, a planned early invasive treatment strategy was associated with increased rates of procedure-related MI and bleeding but no differences in long-term spontaneous MI, non-procedure-related bleeding or mortality.
Introduction
The Platelet Inhibition and Patient Outcomes (PLATO) trial studied the efficacy and safety of ticagrelor compared to clopidogrel in a large population of patients with non-ST-elevation acute coronary syndrome (NSTE-ACS) and planned invasive or conservative treatment strategy, or ST-elevation myocardial infarction (STEMI) and planned primary percutaneous coronary intervention (PCI). 1 In the overall trial, as well as in patients with NSTE-ACS, treatment with ticagrelor compared with clopidogrel reduced the risk of the composite endpoint of cardiovascular (CV) death, myocardial infarction (MI) or stroke during 6–12 months follow-up, without increasing the overall risk of major bleeding.1,2 These results were consistent and more pronounced in patients with elevated cardiac troponin T (cTnT) measured with a high-sensitivity method (cTnT-hs), while there was no significant difference in the primary endpoint between treatment groups in patients with normal cTnT-hs at randomisation. 3
Previous trials and meta-analyses have indicated that benefits of an early invasive treatment strategy are predominantly observed in patients at intermediate and high risk, while patients at lower risk are less likely to benefit, and may even be harmed by procedure-related bleeding and peri-procedural MI following PCI.4–12 Therefore, current guidelines recommend the use of clinical risk scores or discrete risk variables as decision support concerning early invasive procedures in patients with NSTE-ACS.13,14 In the recent European treatment guidelines, presence of an elevated level of cardiac troponin (cTn) on its own has been proposed for identification of patients who might benefit from an early invasive treatment strategy. 13 This recommendation is based on several large-scale trials in NSTE-ACS demonstrating an association between elevated cTn levels and an increased risk of subsequent death and MI which is lowered by antithrombotic and early invasive treatment.3,15–18 Several trials have indicated that lowering the cut-off concentration of cTn improved risk stratification even further.17,19 Unfortunately, until now, standard cTn assays used have been limited by lower analytical sensitivity and inadequate assay precision at concentrations close to the lower limit of detection. 20 Recent cTn-hs assays enable an earlier and more accurate identification of non-ST-elevation myocardial infarction (NSTEMI), and hold the potential for superior risk stratification.13,14,21–23 Conversely, a normal cTn measured with a high sensitivity assay is regarded as very low risk obviating the need for routine monitoring, with the option of early discharge to a peripheral ward or home after risk assessment. 13
The objective of the present biomarker substudy from the PLATO trial was to examine the efficacy and safety of a planned invasive and a planned conservative treatment strategy in patients with an entry diagnosis of NSTE-ACS and a normal level of cTnT-hs or cTnI-hs at the time of randomisation.
Methods
Design
PLATO (www.clinicaltrials.gov; NCT00391872) was an international, prospective, randomised, double-blind, double-dummy, event-driven trial in patients hospitalised for NSTE-ACS, either managed invasively or medically, or STEMI scheduled for primary PCI. The criteria on which the entry diagnosis of NSTE-ACS was made are listed in the Supplementary Material. Details of the design, population and outcome measures for the main trial and for pre-specified subgroups have been published. 1 Briefly, patients were randomised to receive either ticagrelor or clopidogrel within 24 h of onset of the most recent cardiac ischaemic symptoms and before PCI.
At the time of randomisation, patients were designated as planned for initial invasive or initial conservative management by the treating physician within the interactive voice randomisation system.
Patients
This analysis from the PLATO biomarker substudy addresses the subgroup of patients with an entry diagnosis of NSTE-ACS in whom blood samples were collected at randomisation and concentrations of cTnT-hs and cTnI-hs were later measured at the Uppsala Clinical Research Center (UCR) laboratory.
Patients fulfilling the study criteria of STEMI were not included in this substudy. All appropriate national regulatory authorities and ethics committees of the participating centres approved the PLATO trial. All patients gave written informed consent for participation in the trial before enrolment.
Biomarkers
Blood samples for the biomarker substudy were obtained via a direct venous puncture. Plasma was frozen in aliquots and stored at −70°C until analysed. cTnT was determined using the cTnT-hs assay on the Cobas Analytics e601 and c501 Immunoanalyser (Roche Diagnostics) according to the instructions of the manufacturer. 23 The tested cTnT-hs cut-off level of 14 ng/l (99th percentile value) for the diagnosis of MI was based on a multicentre reference study. 24 Values <14 ng/l were classified as normal cTnT-hs. cTnI was determined with a cTnI-hs assay (AccuTnI, Beckman Coulter) using an immuno-enzymatic sandwich assay format. For the cTnI-hs assay, the lower detection level was 0.01 µg/l, the 97.5th and 99th percentile upper normal limit (ULN) was 0.04 µg/l. 20 The lowest measurable concentration with a 10% coefficient of variation (CV) was 0.04 µg/l. The CV indicates the percentage of total imprecision for a specific cTn assay.
Event definitions
Definitions of ischaemic and bleeding events have been reported previously.1,25 The MI events were also classified post-hoc according to the universal MI definition from 2007 prior to the revised definition published in 2012.26,27
An independent blinded central adjudication committee adjudicated primary and secondary endpoints and bleeding events based on information from patient records and levels of cardiac markers measured at the local hospitals.
Statistics
The pre-specified primary efficacy endpoint for this PLATO substudy was time to first occurrence of the composite of CV death and MI (including silent MI) but as opposed to the PLATO main trial did not include non-haemorrhagic stroke as a component. Secondary efficacy endpoints were time to first occurrence of the individual endpoints: CV death, total mortality, MI (including silent MI) and spontaneous and procedure-related MI. The primary safety endpoint was time to first occurrence of major non-CABG-related bleeding.
The analysis set comprised all patients fulfilling the criteria of NSTE-ACS at randomisation with cTnT-hs<14 ng/l and who were randomly assigned to a treatment group and received at least one dose of study medication. A multivariable Cox proportional hazards model with planned treatment strategy (invasive/conservative), randomised treatment group (ticagrelor/clopidogrel), sex, age, body mass index (BMI), diabetes, smoking status, congestive heart failure, previous MI, previous CABG, chronic renal disease, previous PCI, hypertension, previous non-haemorrhagic stroke, peripheral artery disease (PAD) and angina pectoris as presenting symptom, as independent variables was used to analyse the primary and secondary endpoints. The hazard ratios (HRs) and their 95% confidence intervals (CIs) for planned invasive vs conservative treatment strategy were calculated. The proportional hazards assumption was evaluated by visual inspection of the log-cumulative hazards plots (results not shown).
A supportive analysis was performed for cTnI-hs at the 99th percentile cut-off (0.04 µg/l) instead of cTnT-hs, keeping all other variables unchanged.
Given that a substantial proportion of patients with a planned invasive treatment approach did not receive an invasive strategy treatment, additional Cox proportional hazards model including a factor for in-hospital invasive or conservative treatment approach and randomised treatment group was evaluated.
Consistency of effects among subgroups was assessed using the test for interaction between planned invasive or conservative treatment approach and the subgroup factor in the Cox model. The analysis of the cohort with normal cTnT-hs values was of explorative type. Values of p less than 0.05 were considered nominally significant. All analyses were done with SAS software (version 9.3, SAS Institute, Cary, North Carolina, USA).
Results
Patients
In the overall PLATO trial, 1232 patients met the criteria of NSTE-ACS and had normal cTnT-hs levels pre-randomisation (n=1639 patients with normal cTnI-hs, Supplementary Material, Supplementary Methods) of all randomised patients receiving at least one dose of study medication and available cTnT-hs (n=16,707). Blood samples for assessment of pre-randomisation cTn status were obtained after a median of 12.7 h (Q1–Q3: 5.2–21.0). Of the 1232 patients, 473 patients (38.4%) and 759 patients (61.6%) were planned for an invasive and non-invasive treatment strategy, respectively (Supplementary Material, Figure I). Out of a total of 613 patients who underwent coronary angiography, 225 patients (36.7%) had normal coronary arteries.
Baseline characteristics of patients with normal cTnT-hs values are presented in Table 1 (data for cTnI-hs are provided in Supplementary Material, Table 1. A total of 221 patients (17.9%) had received open-label clopidogrel before randomisation. The total ‘intended’ dose of clopidogrel (open-label and blinded) given in the first 24 h was 300 mg in 1142 (92.7%), and 600 mg in 90 (7.3%) of the patients. Randomised treatment was given for a median (Q1–Q3) duration of 278 (179–365) days and discontinued prematurely in 139 (29.4%) and 155 (20.4%) of the patients in the planned invasive and conservative groups, respectively. Women were allocated more often than men to a planned conservative strategy (HR 1.67; 95% CI 1.365–2.0481, p<0.0001). Women were older, more often had a history of hypertension, higher median GRACE risk scores (data not shown). Of note, women with normal hsTnT less often had documented coronary artery disease (11.6 vs 69.7%, p<0.0001) and received PCI less often (3.5 vs 10.6%, p<0.001) during hospitalisation than men.
In-hospital and study drug characteristics for the total cohort of patients with non-ST-elevation acute coronary syndromes (NSTE-ACS) (by ECG) and normal cardiac troponin T measured with a high-sensitivity method (cTnT-hs) at baseline, by planned invasive or conservative treatment strategy.
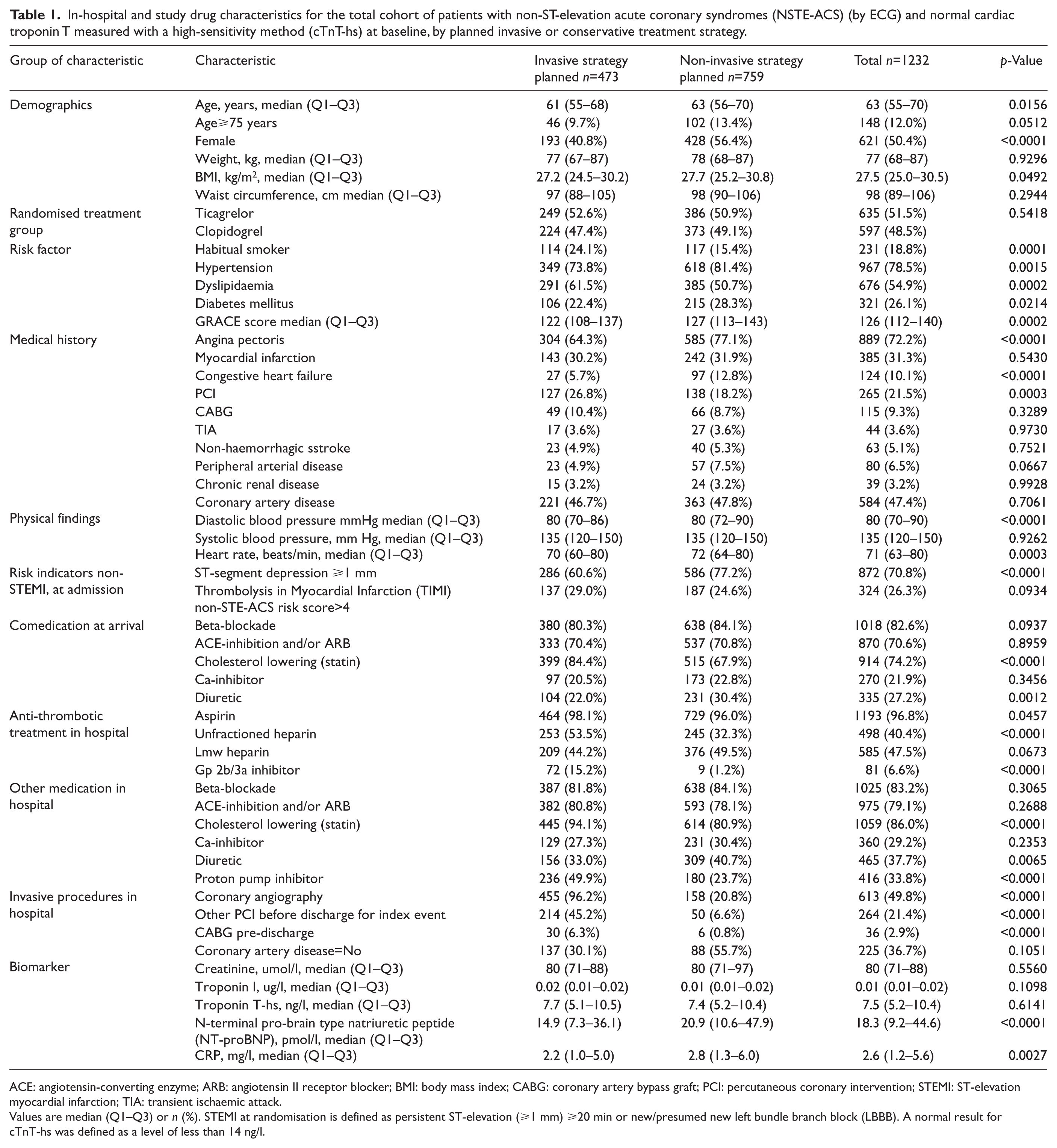
ACE: angiotensin-converting enzyme; ARB: angiotensin II receptor blocker; BMI: body mass index; CABG: coronary artery bypass graft; PCI: percutaneous coronary intervention; STEMI: ST-elevation myocardial infarction; TIA: transient ischaemic attack.
Values are median (Q1–Q3) or n (%). STEMI at randomisation is defined as persistent ST-elevation (⩾1 mm) ⩾20 min or new/presumed new left bundle branch block (LBBB). A normal result for cTnT-hs was defined as a level of less than 14 ng/l.
Efficacy outcomes in relation to a planned invasive or conservative treatment approach
In patients with normal cTnT-hs values, the composite of CV death and MI occurred in 7.3% of the planned invasive and 3.4% in the non-invasive group (adjusted HR 2.3; 95% CI 1.33–3.99; p=0.0028) (Figures 1 and 2(a)). The adjusted point estimates from multivariable models were consistent for pre-specified subgroups (Supplementary Material, Tables 2 and 3). A planned invasive treatment was not associated with any increase in the incidence of CV death (Figures 1 and 2(b)) which occurred in 1.3% vs 1.3% of the planned invasive vs conservative treatment approach, respectively (adjusted HR 1.22; 95% CI 0.41–3.61; p=0.72). There was a difference in the incidence of MI occurring in 6.4% and 2.2% of the planned invasive and conservative treatment approaches, respectively (Figures 1 and 2(c)), (adjusted HR 3.02; 95% CI 1.59–5.74; p=0.0007), driven by a higher rate of procedure-related MI in the planned invasive as compared with the conservative group (16 (3.4%) vs 1 (0.1%)). The rate of spontaneous MI was not statistically different in the planned invasive vs conservative group (13 (3.0%) vs 14 (2.1%); adjusted HR 1.53; 95% CI 0.7–3.34; p=0.28) (Figures 1 and 2(c)). CV death as a consequence of spontaneous or procedure-related MI was rare, with only two cases after spontaneous MI and one case after procedure-related MI. All-cause mortality was 1.8% (n=8) vs 1.6% (n=12) with a planned invasive and conservative treatment approach, respectively (adjusted HR 1.31; 95% CI 0.51–3.39; p=0.58).
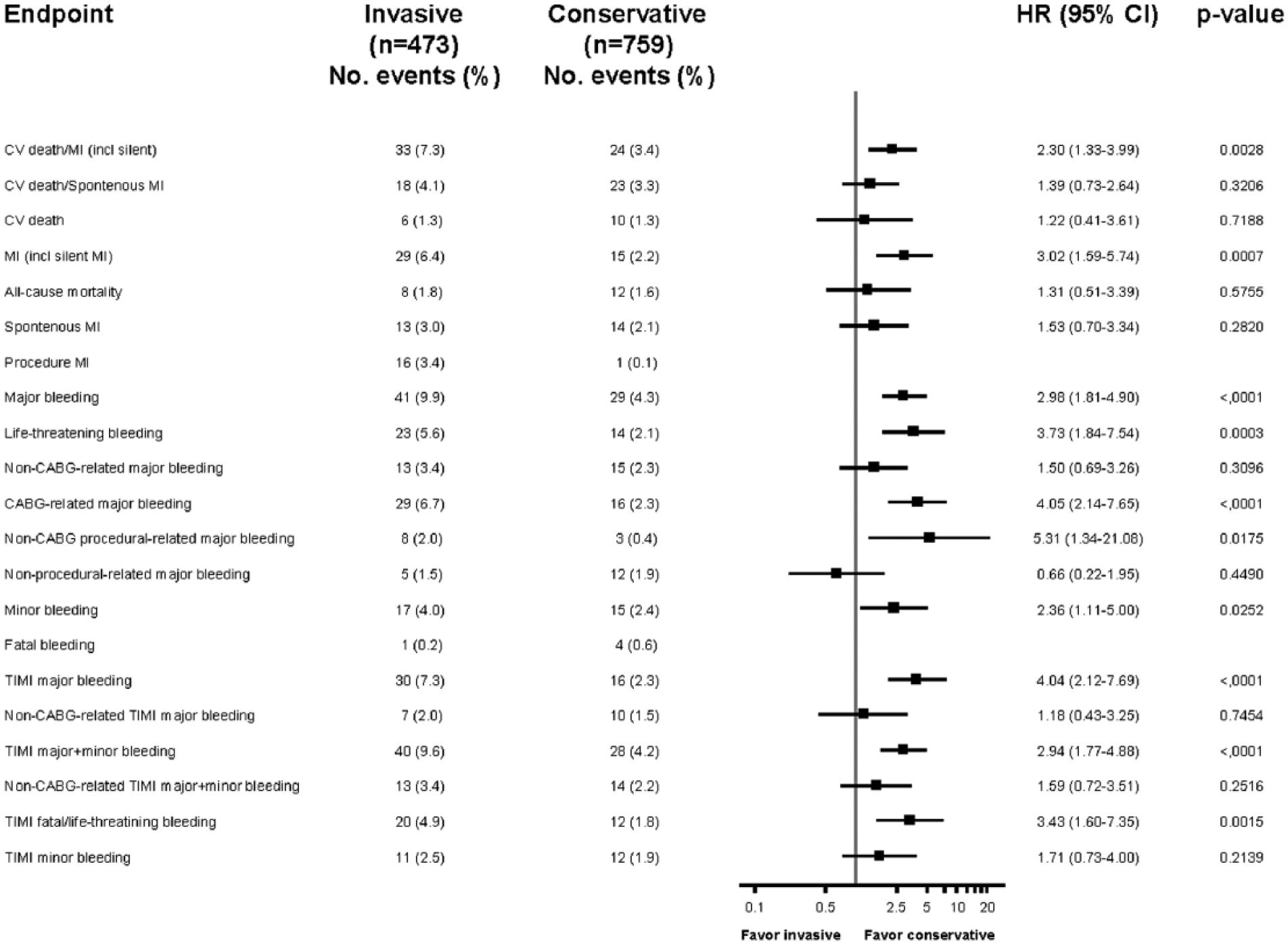
Efficacy and safety endpoints for non-ST-elevation acute coronary syndrome (NSTE-ACS) patients with normal cardiac troponin T measured with a high-sensitivity method (cTnT-hs) levels at baseline, by planned invasive/conservative treatment approach. The event rate in percentage form is the cumulative Kaplan-Meier estimate of the rate of the endpoint at 12 months. Values of p and hazard ratios (HRs) from multivariable Cox proportional hazards models with planned treatment approach (invasive/conservative), subgroup, treatment approach-by-subgroup interaction, treatment group (ticagrelor/clopidogrel), sex, age, body mass index (BMI), diabetes, habitual smoking, coronary artery disease, previous myocardial infarction (MI), previous coronary artery bypass graft (CABG) surgery, chronic renal disease, previous percutaneous coronary intervention, hypertension, previous non-hemorrhagic stroke, carotid stenosis, peripheral artery disease and angina pectoris as independent variables (note: age was used as a continuous variable except when age was the subgroup variable being considered). HRs and p-values are not reported when the total number of events is <10 or <3 in one of the groups. CI: confidence interval; CV; cardiovascular.
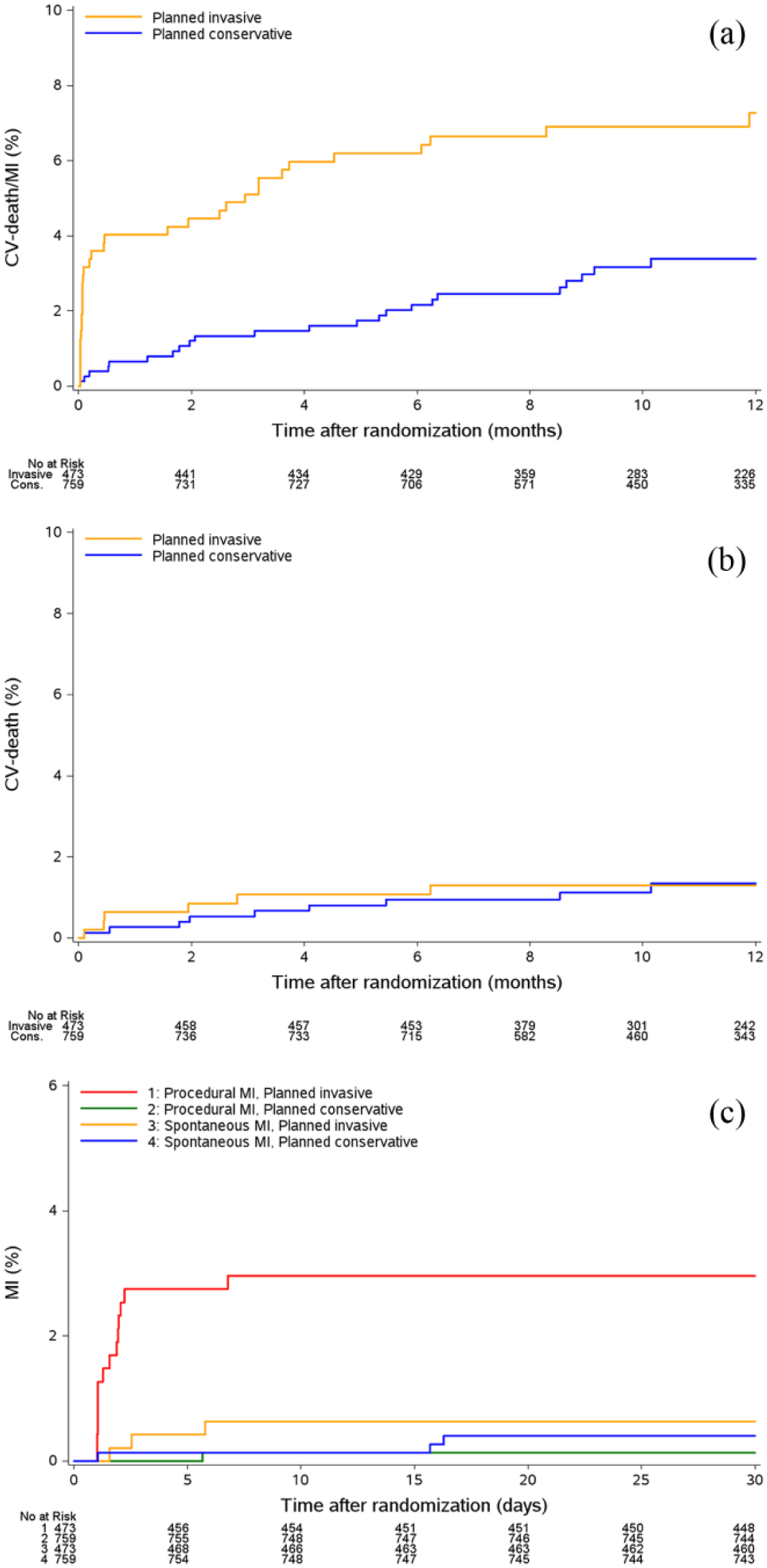
(a) Cumulative Kaplan-Meier estimates of the time to cardiovascular (CV) death and myocardial infarction (MI) (including silent) for non-ST-elevation acute coronary syndrome (NSTE-ACS) patients with a normal cardiac troponin T measured with a high-sensitivity method (cTnT-hs) value at baseline, by planned invasive/conservative treatment approach. (b) Cumulative Kaplan-Meier estimates of the time to CV death for NSTE-ACS patients with a normal cTnT-hs value at baseline, by planned invasive/conservative treatment approach. (c) Cumulative Kaplan-Meier estimates of the time to spontaneous and procedure-related MI, respectively, for NSTE-ACS patients with a normal cTnT-hs value at baseline, by planned invasive/conservative treatment approach. A normal cTnT-hs value was defined as less than 14 ng/l. The analyses included 1232 patients with a normal cTnT-hs value at baseline, excluding ST-elevation myocardial infarction (STEMI) at randomisation. STEMI at randomisation was defined as persistent ST-elevation (⩾1 mm) ⩾20 min or new/presumed new left bundle branch block (LBBB) at baseline.
Safety outcomes in relation to a planned invasive or conservative treatment approach
In patients with normal cTnT-hs at randomisation, the rate of major bleeding was significantly greater among patients with a planned invasive treatment approach (9.9% vs 4.3%, adjusted HR 2.98; 95% CI 1.81–4.9, p<0.0001) explained by the higher rate of procedure-related bleeding i.e. CABG-related major bleeding 6.7% vs 2.3% (adjusted HR 4.05; 95% CI 2.14–7.65; p<0.0001) and non-CABG procedure-related major bleeding 2.0% vs 0.4% (adjusted HR 5.31; 95% CI 1.34–21.08; p=0.0175) in the planned invasive compared with the non-invasive group (Figure 1). There were no differences in the rates of non-procedure-related major bleeding between the treatment strategies (1.5% vs 1.9%, adjusted HR 0.66; 95% CI 0.22–1.95, p=0.45). Accordingly, life-threatening bleeding was more common with a planned invasive treatment approach (5.6% vs 2.1%, adjusted HR 3.73; 95% CI 1.84–7.54; p=0.0003). Fatal bleeding was rare in both groups (0.2% vs 0.6%, Figure 1). Results were consistent for the PLATO and the TIMI bleeding definitions. Causes of major bleedings (n=29) among patients allocated to a non-invasive strategy are listed in Supplementary Material, Table 4. The finding that the majority of major bleedings were procedure related reflects the fact that a considerable number of patients not planned for an invasive procedure indeed received an invasive strategy in hospital. Efficacy and safety outcomes in the actual treatment groups are displayed in Supplementary Material, Figures IV and V.
Verification analyses on efficacy and safety using cTnI-hs instead of cTnT-hs
The association between planned procedures and outcomes were verified with cTnI-hs (Supplementary Material, Table 3 and Figures II–V).
Discussion
The present substudy of the PLATO trial showed that, in patients with suspected NSTE-ACS and a normal cTn-hs level at randomisation, a planned invasive treatment approach was associated with higher rates of procedure-related MI and major bleeding while there were no statistically significant differences in CV mortality or spontaneous MI. These findings confirm previous studies showing that an early invasive treatment in NSTE-ACS is associated with an early risk of procedure-related events, that might exceed the benefits of the procedure for patients at low risk, e.g. in patients with normal cTn values.5,6,8,11,18 It is striking that these findings were verified in a contemporary trial such as PLATO where patients received current guideline-recommended adjunctive pharmacotherapy, including dual antiplatelet treatment, and were allocated to invasive procedures based on decisions at the discretion of their physician.1,13,14
cTn elevations are highly sensitive for the detection of the very minute extent of myocardial necrosis. Based on the present findings, it seems that determination of either cTnT or cTnI in NSTE-ACS provides fairly similar information. There is compelling evidence that even slight elevations of cTn-hs are associated with plaque instability and distal embolisation of thrombi from ulcerated plaques, explaining a reduction of mortality in troponin-positive patients with more intensive pharmacotherapies or early invasive strategy. 28 Supporting this hypothesis, previous studies found that elevated levels of cTn improved the identification of patients who benefited from early revascularisation, more potent antiplatelet therapies and effective antithrombin therapies.5,6,15–17 In contrast, absence of detectable troponin in blood was associated with a lower likelihood of plaque rupture and intracoronary thrombus formation and a low subsequent risk for spontaneous MI or CV death 29 .
Before the implementation of cTn-hs assays, evidence from large randomised clinical trials and meta-analyses supported the use of early risk stratification using cTn and clinical risk scores.4–7,9,11,18 However, all these analyses depended on cTn measurements with major analytical limitations since cTn cut-offs were either used at the lower limit of detection (LLD) or at a cut-off for which available assays did not provide precision of less than 10% variation. The 2011 European Society of Cardiology (ESC) and updated 2012 American College of Cardiology Foundation (ACCF)/ American Heart Association (AHA) guidelines on management of patients with NSTE-ACS recommend an initial risk stratification of ACS patients using risk stratification models such as the GRACE or TIMI score.13,14 Presence of elevated cTnT or cTnI levels, particularly demonstrating a rise and/or a fall, represent relevant risk indicators or primary high risk criteria that stipulate a decision in favour of early invasive therapy within 24 h.13,14 Thus, the present findings support guideline recommendations that cTn-hs should be a key component in the decision making on early invasive treatment.
These novel, more sensitive, assays allow detection of more patients fulfilling the criteria of NSTEMI rather than NSTE-ACS, thereby reducing the number of patients with the uncertain diagnosis of unstable angina, enabling earlier diagnosis and improving risk stratification in patients with previously undetectable troponin.21–23 The present findings suggest that a normal cTn-hs value identifies patients at low risk for death/MI, or major bleedings, when allocated to a conservative strategy, and with limited benefit, possibly at risk of harm, from an invasive treatment even in the presence of other concurrent background risk factors such as higher age, diabetes mellitus, presence of ECG changes, impaired renal function, a low-to-intermediate GRACE score and history of non-haemorrhagic stroke.
Besides higher rates of procedure-related MI, the present study found that an invasive strategy in patients with normal troponin was associated with higher rates of procedure-related bleeding including life-threatening bleeding. This finding is in agreement with previous studies demonstrating an increase of bleeding events associated with early coronary angiography as compared with non-invasive treatment.4,5
The higher rates of procedure-related MI associated with an early invasive strategy found in the present PLATO substudy is in agreement with the experiences from the FRagmin and Fast Revascularisation during InStability in Coronary artery disease (FRISC)-II, Randomized Intervention Trial of Unstable Angina (RITA)-3 and Invasive Conservative Treatment in Unstable Coronary Syndrome (ICTUS) trials.6,8,11,12 In these trials, using less sensitive cTn assays, an invasive strategy in patients with normal cTn was associated with a two-fold higher risk of procedure-related MI. The prognostic relevance of procedure-related MI in otherwise optimally treated patients has long been a matter of debate. The collaborative analysis of the quoted three trials found no association between procedure-related MI and long-term mortality within five years. In contrast, spontaneous MI occurring within six months after randomisation was associated with an adjusted 2.8-fold higher risk for CV death. 12 In addition, a sub-analysis from the ACUITY trial showed that PCI-related MIs did not affect one-year mortality in patients with NSTE-ACS. 30 The current findings from PLATO support these findings as there was no difference in CV death or spontaneous MI despite the high rate of peri-procedural MI in the invasively managed cohort with normal cTn-hs values.
Findings on efficacy and safety of a planned invasive vs conservative treatment strategy observed in patients with a normal cTnT-hs value were similar, with only small numerical differences, when using a cTnI-hs assay. Procedure-related complications were even more pronounced among patients with normal cTnT-hs or cTnI-hs receiving in-hospital invasive treatment, supporting the hypothesis that patients at low risk are being exposed to procedure-related harm without deriving a substantial benefit from an early invasive treatment.
Limitations
Firstly, in the PLATO trial, patients were not randomised to an invasive or conservative treatment strategy. The allocation to an invasive or conservative treatment strategy was left at the discretion of the treating physician, giving the potential to select patients at higher risk to an invasive strategy. Indeed, there were significant differences regarding several baseline characteristics between planned invasive and conservative treatment groups. Multiple adjustments were therefore performed to minimise potential confounding effects on efficacy and safety outcomes. In addition, the decision to perform an invasive treatment was changed in a third of patients initially planned for an invasive strategy whereas the decision for a conservative treatment remained unchanged in the vast majority of patients initially assigned to a conservative treatment, suggesting an initial overestimation of risk.
Secondly, the findings of this substudy were based on a single pre-randomisation sample of cTn. The blood sample was obtained at a median of 12.7 h post onset of symptoms, minimising the risk of missing a patient with evolving NSTEMI as cTn-hs assays allows rule-out of an MI if obtained within three hours after presentation. 13 Although uncertainity remains due to the low numbers of coronary angiography in this subcohort, a diagnosis of unstable angina and thus ACS is still highly likely given the enrolment criteria of the PLATO trial (Supplementary Material data).
Thirdly, adjudication of peri-procedural MI was done according to the second version of the universal MI definition that was valid during that time. 26 Using that definition, peri-procedural (type IV) MI was diagnosed in the presence of a post-procedural increase of cTn >3 times ULN, even in the absence of symptoms or other clinical findings suggesting myocardial ischaemia, provided that cTn was negative prior to PCI. Although some peri-procedural MIs might have been spontaneous MIs, this will not affect the interpretations of these analyses.
Conclusions
In patients with NSTE-ACS and normal cTn-hs values, planning and performing an early invasive treatment is associated with increased rates of procedure-related MI and bleeding events but is not associated with differences in long-term spontaneous MI, non-procedure-related bleeding or mortality. Accordingly, patients with suspected NSTE-ACS and a normal cTn-hs value may not benefit from a routine invasive strategy during hospital stay, provided they receive optimal pharmacotherapy and have the opportunity for invasive procedures at signs or symptoms of recurrent ischaemia. Considering that a normal cTn-hs value does not exclude the presence of significant coronary stenosis, the decision to perform diagnostic and invasive procedures at a later time point should be individualised according to the clinical situation. Our findings on high sensitivity troponin support the recommendations of current ESC guidelines on the distinct management of unstable angina, i.e. ACS with normal cTn values. 13
Footnotes
Acknowledgements
The complete list of PLATO investigators and main study committees has been published previously.1 The authors acknowledge Nils Åsenblad, formerly of UCR, for statistical support and Ebba Bergman at UCR for editorial assistance.
Funding
The PLATO study was funded by AstraZeneca. Support for the analysis and interpretation of results and preparation of the manuscript was provided through funds to the UCR and Duke Clinical Research Institute as part of the Clinical Study Agreement.
Conflict of interest
EG: honoraria for lectures, research grants and advisory board member for AstraZeneca, Roche Diagnostics; grant and personal fees from Bayer Health.
LW: institutional research grant, consultancy and lecture fees, travel support and honoraria from GlaxoSmithKline; institutional research grants, consultancy and lecture fees and travel support from AstraZeneca, Bristol-Myers Squibb/Pfizer, Boehringer Ingelheim; institutional research grant from Merck & Co.; institutional research grant from Roche; consultancy fees from Abbott; holds two patents involving GDF-15.
SKJ: institutional research grants, honoraria and consultant/advisory board fees from AstraZeneca; institutional research grants and consultant/advisory board fees from Medtronic; institutional research grants from Terumo Inc., Vascular Solutions; honoraria from The Medicines Company; consultant/advisory board fees from Dachii Sanchio, Janssen, Sanofi.
MB: institutional research grant from AstraZeneca.
AS: institutional research grants from AstraZeneca, Boehringer Ingelheim and Bristol-Myers Squibb/Pfizer.
RFS: institutional research grant, consultant fees, speakers fees, travel support from AstraZeneca, and named by the company as an inventor on a patent pending related to discoveries made during the PEGASUS-TIMI 54 study but has no personal financial interest in this; institutional research grant, consultant fees and speaker fees from Daiichi Sankyo/Eli Lilly; consultant fees, speaker fees and consumables from Accumetrics; institutional research grant and consultant fees from Merck; honoraria from Medscape; consultant fees from Aspen, Correvio, Plaque Tec, Roche, The Medicines Company, Thermo Fisher Scientific, Regeneron, Sanofi-Aventis; travel support from Medtronic.
SH: advisory board member and research support from Pfizer; advisory board member for AstraZeneca, Bristol-Myers Squibb, Bayer; research support from GlaxoSmithKline, Boehringer Ingelheim.
CPC: grant, consultant fees and travel support from Boerhinger Ingelheim; grants and consultant fees from Takeda, Merck, GlaxoSmithKline; grant and personal fees from Accumetrics; grant and travel support from AstraZeneca; grants from Arisaph, Janssen; consultant fees from Bristol-Myers Squibb, Alnylam, Pfizer, Essentialis, Kowa, Lipimedix, Regeneron, Sanofi; personal fees from CSL Behring.
PWA: research grants and consultant fees from Boehringer Ingelheim, Merck Sharp & Dohme, GlaxoSmithKline; research grants from Amylin Pharmaceuticals Inc., Sanofi-Aventis, Regado Biosciences; consultant fees from AstraZeneca, F. Hoffmann La Roche Ltd, Axio/Orexigen, Eli Lilly, Bayer Pharma AG.
PGS: institution research grants, honoraria and non-financial support from Sanofi, Servier; honoraria and non-financial support from AstraZeneca; honoraria from Amarin, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Daiichi-Sankyo, Eli Lilly, Merck-Sharpe-Dohme, Novartis, Pfizer, Medtronic, Janssen, The Medicines Company, CSL-Behring, GlaxoSmithKline; stockholder in Aterovax.
HAK: grants and personal fees from Roche Diagnostics, AstraZeneca, Bayer Health; personal fees from Roche Daiichi Sankyo.