
Abstract
Background:
Echocardiography is recommended for assessment of left ventricular systolic function in patients with acute heart failure but few randomised trials have validated techniques like tissue Doppler (TDI) and speckle tracking (STE) in patients with acute heart failure following ST-elevation myocardial infarction.
Methods:
This was a substudy from the LEAF (LEvosimendan in Acute heart Failure following myocardial infarction) trial (NCT00324766 ), which randomised 61 patients developing acute heart failure, including cardiogenic shock, within 48 hours after ST-elevation myocardial infarction, double-blind to a 25-hour infusion of levosimendan or placebo. TDI-derived systolic mitral annulus velocity (S′), STE-derived global longitudinal strain (Sl) and strain rate (SRl) were measured at baseline, day 1, day 5 and after 42 days.
Results:
Datasets rejected for analyses were 2% (TDI) and 17% (STE). S′ increased by 23% in the levosimendan group versus 8% in the placebo group from baseline to day 1 (p= 0.011) and by 30% vs. 3% from baseline to day 5 (p <0.0005). Significant, but less pronounced, improvements in global Sl (p = 0.025 and p = 0.032) and in global SRl (p = 0.046 and p = 0.001) in favour of levosimendan were also present.
Conclusion:
S′ by TDI and STE-derived Sl and SRl were sensitive indices for changes in left ventricular systolic function related to treatment with levosimendan. However, S′ by TDI was more feasible and sensitive and might be preferred for assessment of changes in left ventricular systolic function in critically ill patients with acute heart failure receiving inotropic therapy.
Keywords
Introduction
Echocardiography is the image modality of choice in patients with heart failure due to its availability, safety and low-cost. 1 However, use of echocardiography in patients with acute heart failure (AHF) is less well defined, both in clinical practice and in clinical trials. 2
Assessment of left ventricle (LV) systolic function by indices like wall motion score index (WMSI) and LV ejection fraction are largely based on visual judgement and their user-dependency represents a major limitation, especially in clinical trials. Less user-dependent indices such as peak systolic velocity of the mitral annulus (S′) by tissue Doppler imaging (TDI), and global longitudinal strain (Sl) and strain rate (SRl) by speckle tracking echocardiography (STE), offer both objective, quantitative and validated measurement of LV function.3,4 These indices have been studied in patients with chronic heart failure (CHF).5,6 However, no data exist regarding the feasibility of these indices in patients with advanced AHF complicating ST-elevation myocardial infarction (STEMI).
We have previously reported results from the randomised, placebo-controlled LEAF (LEvosimendan in Acute heart Failure following myocardial infarction) trial on patients with AHF following a percutaneous coronary intervention (PCI)-treated STEMI. 7 We were able to demonstrate that levosimendan improved the primary endpoint WMSI from baseline to day 5 compared with placebo.
The main objective of this substudy of the LEAF trial was to elucidate whether repetitive measurements of S′ by TDI and global Sl and SRl by STE were feasible and sensitive indices for changes in LV systolic function during inotropic stimulation by levosimendan in STEMI patients with AHF including cardiogenic shock.
Methods
The LEAF trial was an investigator initiated, manufacturer independent study conducted at Oslo University Hospital Ullevål. The Regional Ethics Committee approved the study, which was conducted in accordance with the principles of the Declaration of Helsinki. All patients provided written informed consent. The study was registered at www.clinicaltrial.gov; NCT00324766.
Study design and patient population
The LEAF trial was a randomised, double-blind, placebo-controlled, single-centre, parallel-group study. Details on study design and main results have been published previously. 7 Patients were included in an intensive care (ICCU) setting and assigned to an infusion of 0.2 µg/kg per min for 1 h followed by 0.1 µg/kg per min for 24 h of levosimendan or placebo. Included in the study were patients with AHF (including stratified randomisation of patients in cardiogenic shock) complicating a PCI-treated STEMI. The inclusion criteria were: (a) opening of an occluded or dilation of a stenotic coronary artery presumed to be the infarct-related artery, (b) signs of decreased wall-motion in at least three of 16 segments of the LV assessed by echocardiography, (c) clinical HF. Additional criteria in the cardiogenic shock subgroup were: (a) systolic blood pressure (SBP) < 90 mmHg after 60 min of adequate volume therapy or SBP between 90 and 100 mmHg in spite of inotropic support by catecholamine infusion and (b) signs of organ hypoperfusion such as oliguria, cold and clammy extremities or reduced consciousness.
All patients received standard medical therapy according to current guidelines. The use of intravenous inotropic drugs was restricted to patients with cardiogenic shock, except noradrenaline in the setting of hypotension not responding to volume therapy and reduction in study drug infusion.
Echocardiography
Examinations were performed with two digital ultrasonic device systems from the same vendor (GE Vingmed Ultrasound, Horten, Norway), Vivid i at baseline and on day 1 immediately after end of study drug infusion and Vivid 7 on day 5 and after 42 days (four echocardiograms in each patient). All recordings were analysed with the same software (GE Echopac v 108.15). Two experienced echocardiographers (TH, GØA) performed all the recordings and a single one (TH) performed all the analyses. Interobserver reproducibility was tested by an independent echocardiographer blinded to the results of the performed analyses. Three consecutive cardiac cycles were recorded, five if atrial fibrillation was present. Recordings included the standard parasternal and apical four-chamber, two-chamber and long-axis views.
TDI-recordings were obtained by colour tissue Doppler with a mean frame rate of 146 (±30)/s. Care was taken to avoid an angle of incidence >20° between the ultrasound beam and the direction of the motion of the basal segment of the LV walls. A sampling area of 6 mm × 6 mm was positioned in the basal segment of the LV wall within 1 cm of the insertion of the mitral leaflets (Figure 1). S′ (TDI) was measured as the average of the velocities acquired from the base of the septal, lateral, anterior and inferior walls over three consecutive cycles (five if atrial fibrillation).
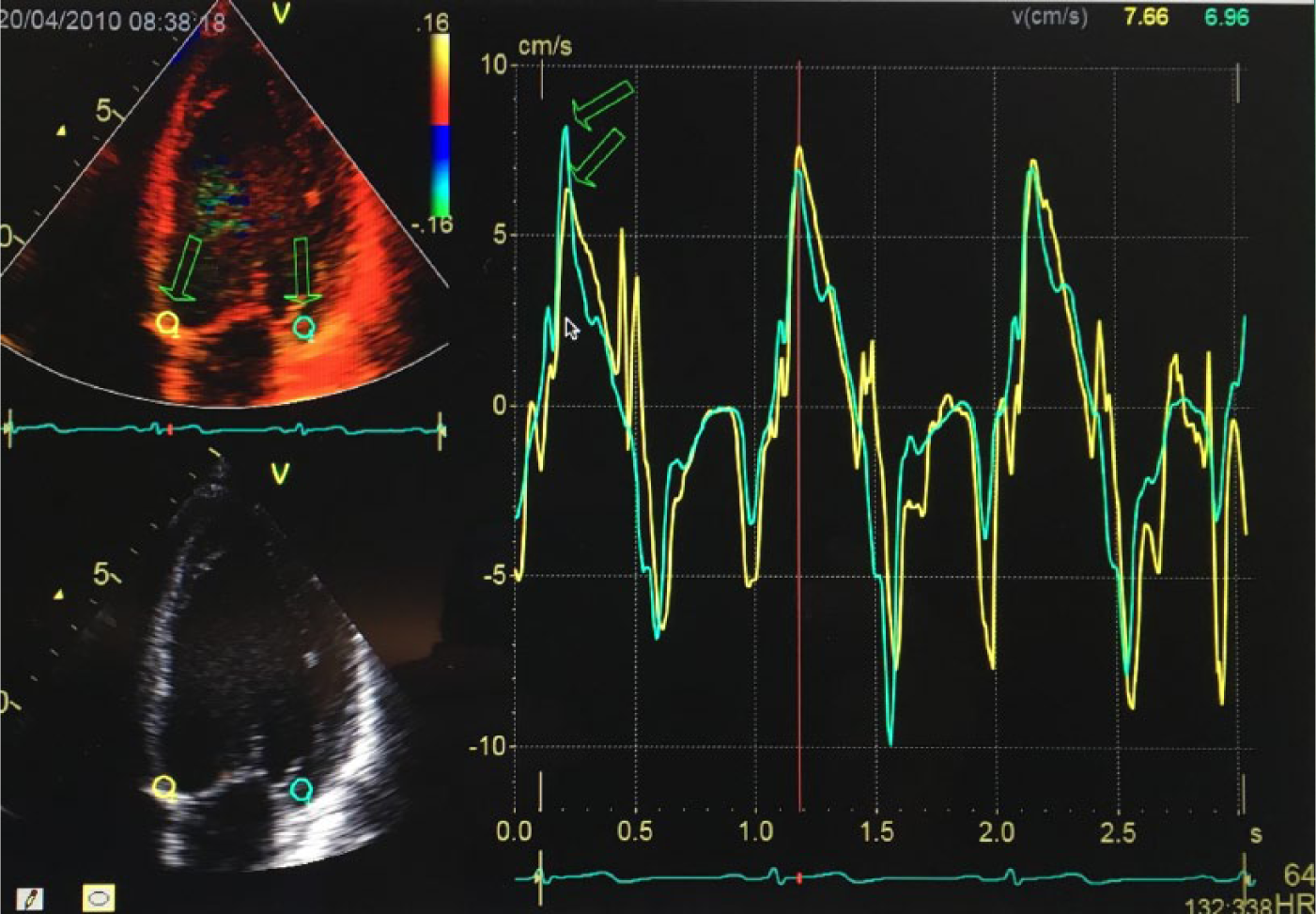
Measurements of left ventricular function by colour tissue Doppler imaging. Placement of sample volume for measurement of mitral annulus velocities in apical four-chamber view (arrows to the left) and the corresponding maximal velocities (arrows to the right) are shown.
Recordings for STE analyses were obtained from grey-scale images in the three apical views with a mean frame rate of 76 (±13)/s. Only the cycle with the best image quality was chosen for the analyses. Tracking of the myocardial walls was automatically performed by the software (GE Vingmed Ultrasound). Segments with suboptimal tracking were discarded. If ≥3 segments were discarded or if atrial fibrillation was present, the whole dataset was rejected for analysis. End-systole was defined as closure of the aortic valve determined from the apical long-axis view. Peak Sl was defined as the maximal shortening before end-systole and by the software given as a mean value in each of the three apical views. Global Sl was then calculated as the average value of the whole LV. Correspondingly, global SRl was calculated as the average of the mean values of the maximal systolic strain rate.
WMSI was measured using a 16-segments model. 8 LV ejection fraction was measured by Simpson’s biplane method or by visual assessment. 8 The LV outflow tract (LVOT) peak velocity and stroke volume (SV) was measured according to current guidelines. 9 Total afterload was determined by the effective arterial elastance (Ea) (0.9 × SBP/SV).10,11 Mitral regurgitation was graded as mild, moderate or severe. 12
Outcome data
Major adverse events were defined as a composite of all-cause death, heart transplantation and implantation of implantable cardioverter-defibrillator (ICD) after successfully surviving cardiac arrest.
Feasibility and reproducibility
The acquired frame rates, both by TDI and STE, were not significantly different between the levosimendan and placebo groups at any timepoint. Figure 2 shows the number of patients analysed by TDI and STE according to treatment groups. Less than 2% of the datasets were discarded for analyses by TDI compared with 17% by STE (Figure 2).
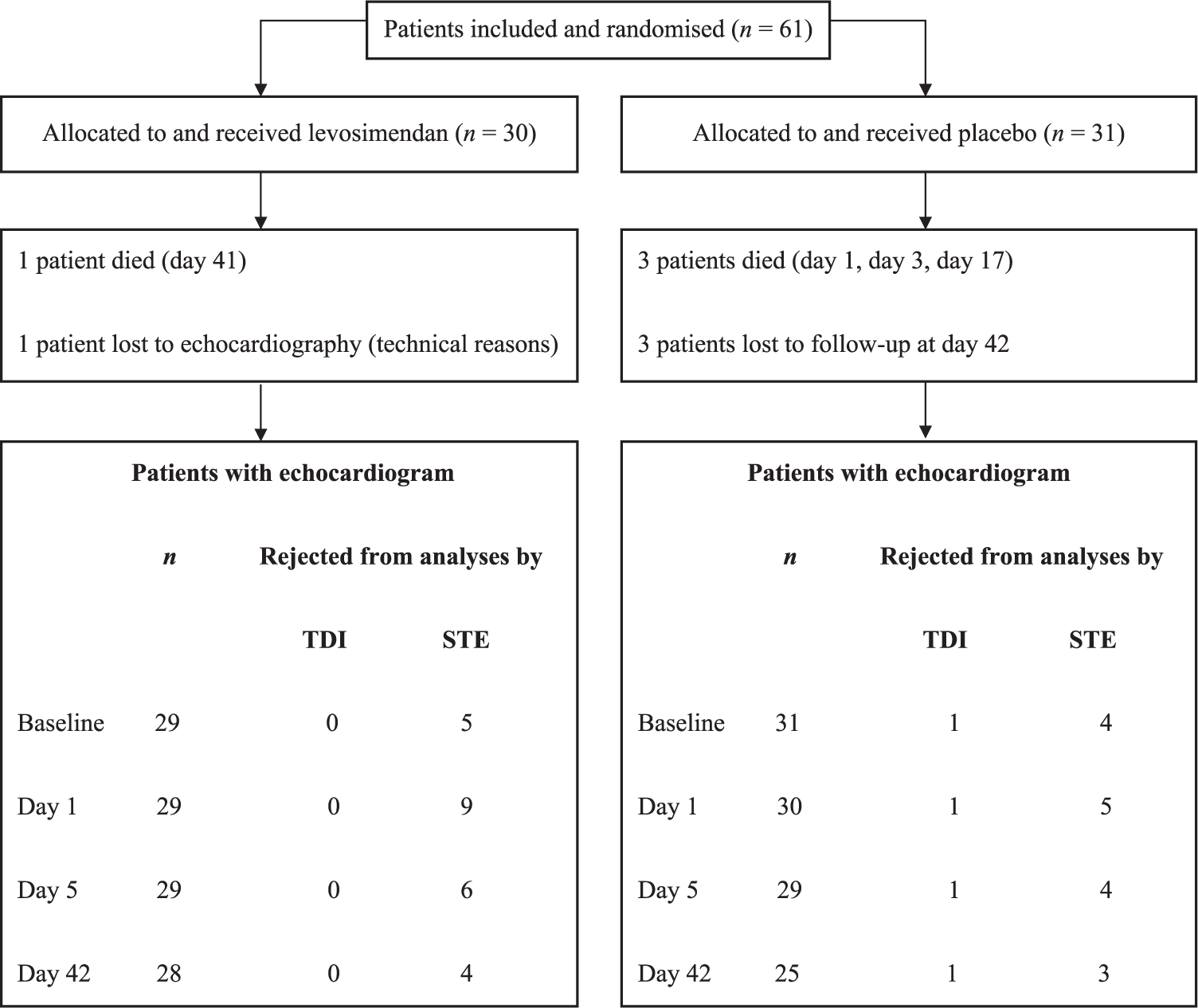
Echocardiograms analysed in the levosimendan and placebo group. Total number and the number rejected from analyses by TDI and STE from baseline until day 42 are shown.
Reproducibility was tested in 20 datasets randomly selected from the LEAF-database. The intraobserver/interobserver intraclass correlation coefficients (95% confidence interval (CI)) for S′(TDI) were 0.97 (0.93–0.99,)/0.94 (0.85–0.98), for global Sl 0.98 (0.95–0.99)/0.93 (0.84–0.97) and for global SRl 0.91 (0.79–0.96)/0.91 (0.78–0.96), respectively.
Statistical analyses
Values are reported as mean (SD) or median (25th, 75th percentiles) according to the distribution of the data. Analyses of covariance were used for changes from baseline between treatment groups in S′(TDI) and global Sl with the respective baseline values as covariates. Analyses of other continuous data were performed by two-sample t-test. If data were not normally distributed, differences in changes from baseline between groups were tested by Mann–Whitney U-test. Univariate Cox proportional hazard analyses were performed in order to explore a possible association between S′, Sl and ejection fraction at baseline and time to a first major adverse event. The relatively low number of events precluded a complete multivariate analysis, and outcome results were therefore only adjusted for age. Log rank test was used for analysis of difference between the levosimendan and placebo groups. A significance level of 5% with a two-sided test was used. Adjustments for multiple comparisons were not performed due to the exploratory design of the study. Statistical analyses were performed using IBM SPSS version 20.0 (SPSS Inc., Chicago, IL, USA).
Results
A total of 61 patients were randomised double-blind to levosimendan (n = 30) or placebo (n = 31). The two treatment groups were not significantly different with respect to baseline characteristics (Table 1). Patients were characterised by large infarct size (peak troponin T ~ 12,000 ng/l) and severe heart failure at inclusion (28% treated with an intra-aortic balloon pump and 15% were in cardiogenic shock).
Baseline characteristics of the study population according to treatment arms.
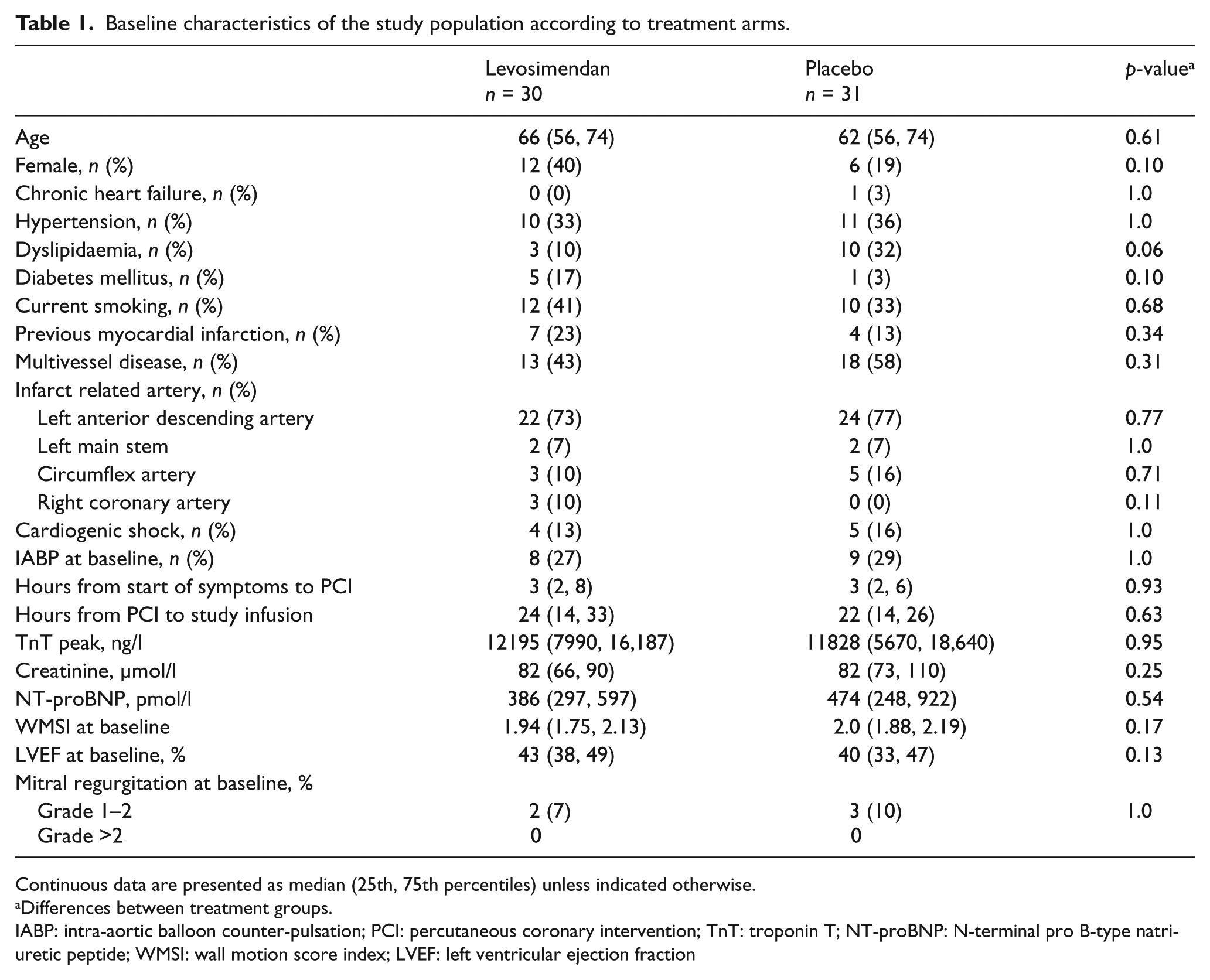
Continuous data are presented as median (25th, 75th percentiles) unless indicated otherwise.
Differences between treatment groups.
IABP: intra-aortic balloon counter-pulsation; PCI: percutaneous coronary intervention; TnT: troponin T; NT-proBNP: N-terminal pro B-type natriuretic peptide; WMSI: wall motion score index; LVEF: left ventricular ejection fraction
Echocardiographic indices
A total of four echocardiograms in one patient were discarded for analysis by TDI compared with 40 in 14 patients by STE (Figure 2). S′(TDI) at baseline was 4.67 ± 1.33 cm/s (levosimendan) and 4.73 ± 1.05 cm/s (placebo) and increased significantly at day 1 (p = 0.011) and day 5 (p <0.0005) in favour of levosimendan, relative increase 23% vs. 8 % (day 1) and 30% vs. 3% (day 5) (Figure 3(a)). Global Sl at baseline was −9.4% ± 1.75 (levosimendan) and −8.8 % ± 2.48 (placebo). There was a significant improvement at day 1 (p = 0.025) and day 5 (p = 0.032) in the levosimendan compared with the placebo group (Figure 3(b)). However, the differences in the relative changes in global Sl between the treatment groups were modest compared with the corresponding differences in S′(TDI) (Figure 3(b)). Baseline levels of global SRl were −0.59/s (−0.67, −0.53) (levosimendan) and −0.57/s (−0.67, −0.50) (placebo) and increased significantly at day 1 (p = 0.046) and day 5 (p = 0.001) in favour of levosimendan (Figure 3(c)). Significant improvements in LVOT peak velocity from baseline to day 1 (p = 0.030) and day 5 (p = 0.002) in favour of levosimendan were also found (Figure 3(d)).
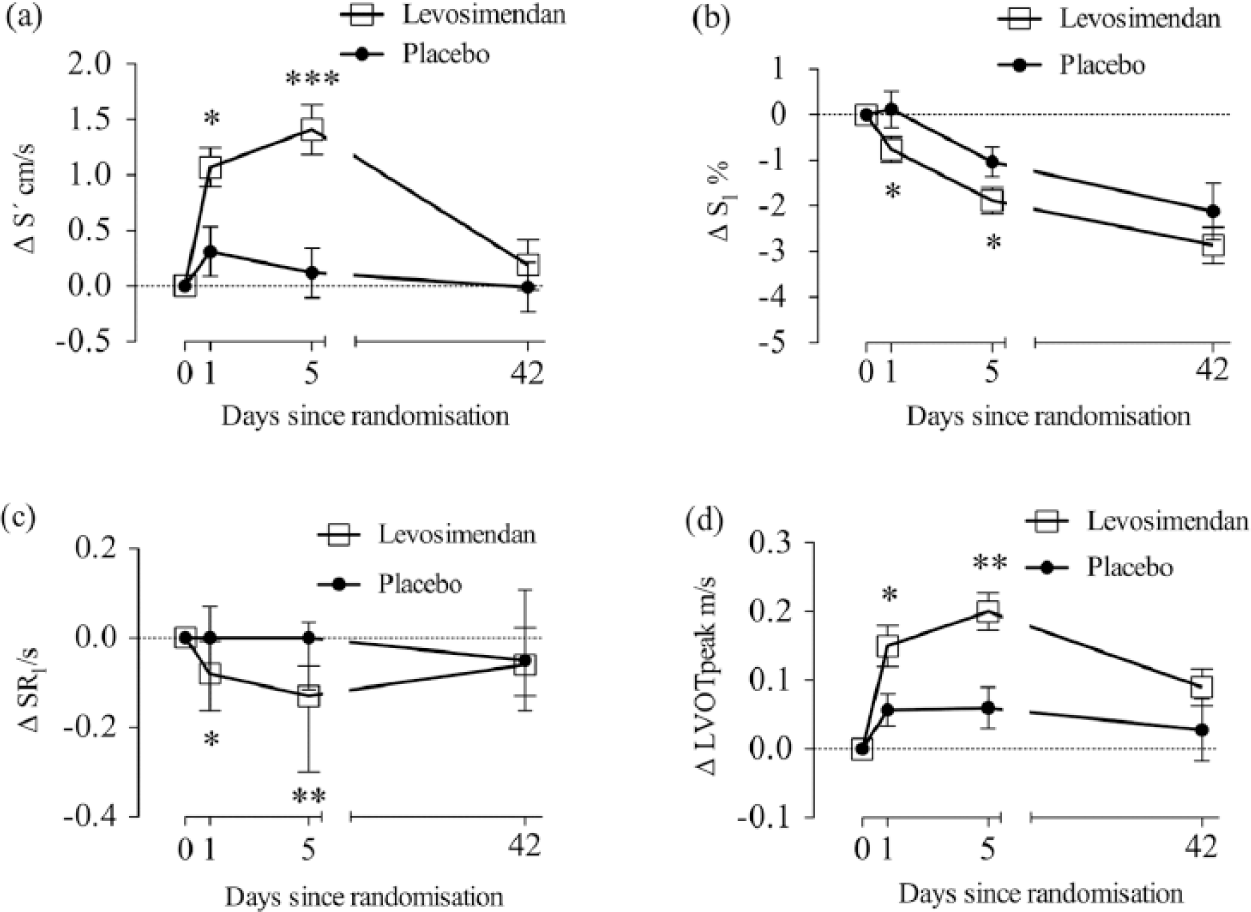
Changes from baseline in echocardiographic indices in patients treated with a 25 h infusion of levosimendan or placebo S′ by colour tissue Doppler (a), Sl by speckle tracking (b), SRl by speckle tracking (c) and LVOT peak (d). Mean values ± SEM ((a), (b) and (d)) or median values with 25th,75th percentiles (c). p-values (* p <0.05, **p <0.005, *** p <0.0005) are given for differences between treatment groups.
Haemodynamic parameters
There was a significant decrease in heart rate (HR) from baseline to day 5 in the placebo group compared with levosimendan. Cardiac output (CO) increased significantly from baseline to day 5 in patients receiving levosimendan compared with placebo. Otherwise no significant between-group differences in HR, SBP, SV or Ea were found (Table 2). In one patient in each treatment group mitral regurgitation was graded as >2 after 42 days, otherwise no changes in mitral regurgitation appeared during the study period.
Haemodynamic data according to treatments arms.
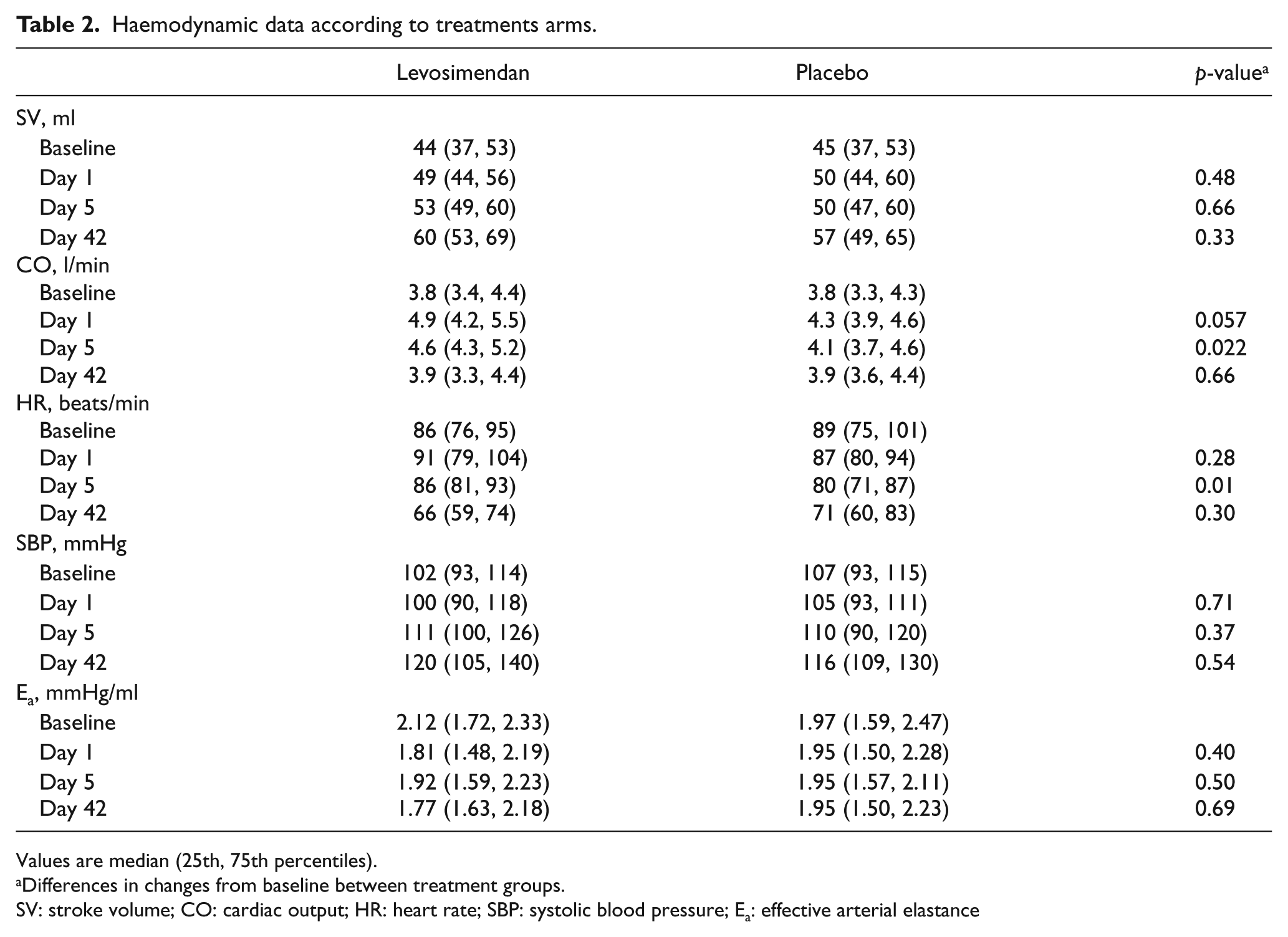
Values are median (25th, 75th percentiles).
Differences in changes from baseline between treatment groups.
SV: stroke volume; CO: cardiac output; HR: heart rate; SBP: systolic blood pressure; Ea: effective arterial elastance
Outcome data
There were 21 major adverse events (deaths (n = 19), heart transplant (n = 1), ICD after cardiac arrest (n = 1)) during follow-up (median 85 months, range 69–125); however, no significant difference between the levosimendan and placebo groups was found (p = 0.72). Both S′ and Sl at baseline were associated with the composite endpoint in univariate analyses, while LVEF only reached borderline significance (Table 3). The HRs were significant after adjusting for age (S′, HR 0.58 (0.37–0.91) p = 0.018), (Sl, HR 1.68 (1.27–2.21) p < 0.0005) and (LVEF (0.87–0.99) p = 0.016).
Cox regression analyses for the association between baseline factors and future adverse events (all-cause death, heart transplantation or implantable cardioverter-defibrillator implantation after surviving cardiac arrest).
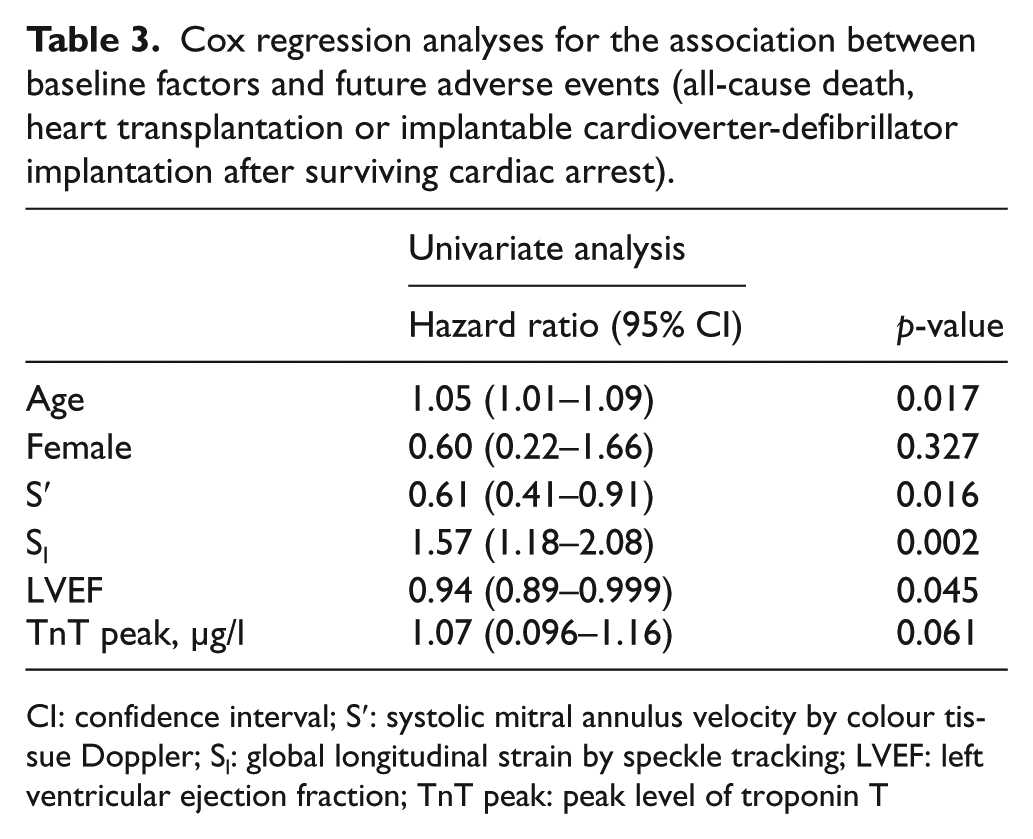
CI: confidence interval; S′: systolic mitral annulus velocity by colour tissue Doppler; Sl: global longitudinal strain by speckle tracking; LVEF: left ventricular ejection fraction; TnT peak: peak level of troponin T
Use of beta-blockers and inotropic drugs other than levosimendan
No significant differences in the use of beta blockers between the levosimendan and placebo groups were found; baseline: 6/30 vs. 6/31, day 1: 3/29 vs. 2/30, day 5: 18/29 vs. 18/29, day 42: 29/30 vs. 24/25, respectively. All patients in the cardiogenic shock group (n = 9) received inotropic drugs (dopamine or dobutamine) before inclusion and during the first day of the study. After five days, one patient in the levosimendan group and two patients in the placebo group received dopamine. A total of four patients in the levosimendan group and one patient in the placebo group received noradrenaline due to transient hypotension during the study drug infusion (first 25 h). This treatment was discontinued in all patients >30 min before the end of the drug infusion and did not affect the subsequent echo-recordings on day 1 or day 5.
Discussion
The principal finding of this prospective clinical study is that S′ measured by TDI was a feasible and sensitive marker of inotropic effect of levosimendan in patients with advanced AHF. This is, to our best knowledge, the first report of the use of this echocardiographic index to quantify effects of inotropic stimulation in patients with AHF complicating STEMI. It was more feasible and sensitive than STE-derived Sl and SRl in an ICCU setting with critically ill patients, including patients on a mechanical ventilator. The randomised, placebo-controlled study design ensured that changes in myocardial function related to inotropic stimulation and not to effects related to time per se were measured.
Feasibility of S′ by TDI and STE-derived Sl and SRl
S′(TDI) is easy to obtain, as visualisation of the mitral annulus is possible in nearly all patients. It has a satisfactory reproducibility when measured as the average velocity from the septal, lateral, anterior and inferior mitral annulus.4,13 In our study, as demonstrated in Figure 2, S′(TDI) was analysed in all patients except one, confirming the feasibility of the index.
STE depends on good quality grey-scale images of the whole LV. 4 This may limit its application in different clinical settings such as an ICCU. This was confirmed in this study on STEMI patients with AHF where many recordings were discarded due to image quality reasons. Our results indicate that STE may not be an ideal method for serial measurements in critically ill patients.
Assessment of inotropic alterations
The inotropic effects of levosimendan occur a few hours after start of the drug infusion and, due to its active metabolites, last for several days. 14 Due to systemic vasodilating properties, levosimendan may also improve LV function by afterload reduction. 15 However, the changes in SBP and the calculated total afterload (Ea) were not significantly different between the two groups during the first five days after start of treatment in this study. Therefore, the observed changes in S′(TDI) between the levosimendan and placebo groups were probably mostly explained by the inotropic effects of levosimendan and not by its vasodilating properties.
The capability of systolic velocity by TDI to detect minor alterations in LV contractility has been documented in animal studies during dobutamine infusion.16–18 Although this index is influenced by LV load and elastic properties of the myocardium,11,19–21 S′ was reported to be relatively independent of haemodynamic parameters like blood pressure and systemic vascular resistance in 179 patients during dobutamine stress echocardiography. 22
Differences in the relative changes in global Sl between the levosimendan and placebo group were modest, while differences in global SRl and LVOT peak velocity were comparable to the relative differences in S′(TDI). SRl and LVOT peak velocity are, as S′, markers of events that occur in the first half of the systole, as opposed to Sl, which is measured at or near end-systole. 23 Previously, animal studies have shown that SRl correlated strongly with contractility, while Sl correlated best with SV.16,24 Also, in a study on healthy humans there was a significantly lower relative increase in global Sl than in global SRl, LVOT peak velocity and S′ during low-dose dobutamin infusion. 25 Our findings indicate that these relationships also apply during inotropic therapy in STEMI patients with AHF.
Levosimendan improved LV systolic function in post-ischaemic myocardium measured as change in WMSI from baseline to day 5 compared with placebo (p = 0.031, primary endpoint of the LEAF trial); however, no significant change was present the first day after start of drug infusion. 7 WMSI is based on visual assessment and the semi-quantitative scoring with only four levels makes it less sensitive to detect minor changes in LV systolic function over time. In this substudy, the TDI and STE-derived indices were more sensitive for such changes, probably because they measure on a continuous scale and are less user-dependent.
Haemodynamic changes
Only a non-significant increase in SV related to levosimendan treatment was found in the present study despite the improvement in LV function. A dose–response relationship between levosimendan treatment and changes in haemodynamic indices after 23–24 h was reported in a placebo controlled study on patients with acute decompensated HF. 26 The main effect of levosimendan in the low-dose range (<0.2 µg/kg per min) seemed to be reduction in ventricular filling pressure and increase in cardiac output due to increased HR, while a more modest increase in SV was observed. AHF in STEMI patients commonly is precipitated by high filling pressures due to reduced contractility and stiffness of ischaemic myocardium, more than reduced SV. Improvement of contractility of ischaemic myocardium consistent with anti-stunning effect of levosimendan has been reported. 27 An improvement in contractility of post-ischaemic myocardium resulting in reduced filling pressures, in spite of a modest increase in SV, might be of benefit in patients with AHF complicating PCI-treated STEMI and explain the results of our study.
Outcome data
Although the key message of the study was that measurements of S′ and Sl are sensitive indices for changes in LV systolic function in STEMI-patients with AHF, our study is also the first to report the prognostic information of early measurements of the indices. S′ has been reported to be a predictor of death in patients with CHF6,28 and clinical outcome in PCI treated STEMI patients, 29 while Sl was shown to be associated with future adverse events in patients with CHF 30 and in patients after AMI. 31 Our results expand the potential clinical importance of early measurements of S′ and Sl in STEMI patients complicated by AHF. However, these results must be interpreted with caution as the sample size and few endpoints generally restricted the use of multivariable analyses and should therefore be confirmed in larger study populations.
Limitations of our study
The sample size was based on changes in WMSI, the primary endpoint of the LEAF trial, and not on changes in the TDI and STE indices examined in this study. An inherent weakness of TDI is the impact of global heart motion and angle of incidence of the ultrasound beam on the measurements. Both factors may have affected the serial measurements of S′(TDI). Analysing only one cycle by STE may have introduced more random variability in the data compared with TDI. The low temporal resolution of the STE recordings in combination with high HR might have underestimated SRl in some patients. 3 Measurement of SRl by TDI might have avoided this. However, as both TDI derived strain rate and strain generally are significantly affected by noise, 3 we decided not to use these indices in this study. Calculations of SV, CO and total afterload were based on noninvasive measurements by pulsed wave Doppler. Serial measurements by this method are sensitive to errors in placement of the sample volume in LVOT. This might have affected the ability to detect significant changes over time.
Conclusion
We have for the first time demonstrated the feasibility and usefulness of serial measurements of S′ measured by TDI and STE-derived global Sl and SRl to assess changes in LV systolic function in an ICCU setting with critically ill patients with AHF. S′ was more feasible than STE-derived indices and performed better than the established index, WMSI. These results suggest that S′(TDI) might be the preferred echocardiographic index for assessment of changes in LV systolic function during inotropic therapy in patients with AHF.
Footnotes
Acknowledgements
We are grateful for skilful help from Dr Christian Shetelig and to the Centre for Clinical Heart Research, Department of Cardiology, Oslo University Hospital, with Professors Harald Arnesen and Ingebjørg Seljeflot, for research support in the LEAF trial.
Conflict of interest
The Department of Cardiology, Oslo University Hospital Ullevål received an unrestricted educational grant from the manufacturer of levosimendan, Orion Pharma in 2005. Orion Pharma did not, however, provide study medication or participate in the design, monitoring or analyses of the LEAF trial or the present substudy. TH has received a lecture honorarium from Orion Pharma in 2012.
Funding
This work was supported by the Centre for Heart Failure Research, University of Oslo, South-Eastern Norway Regional Health Authority and The Scientific Council at Oslo University Hospital Ullevål.