
Abstract
Background:
Acute kidney injury is associated with adverse outcomes after acute ST elevation myocardial infarction (STEMI). It remains unclear, however, whether subclinical increase in serum creatinine that does not reach the consensus criteria for acute kidney injury is also related to adverse outcomes in STEMI patients undergoing primary percutaneous coronary intervention.
Methods:
We conducted a retrospective study of 1897 consecutive STEMI patients between January 2008 and May 2016 who underwent primary percutaneous coronary intervention, and in whom acute kidney injury was not diagnosed throughout hospitalization. We investigated the incidence of subclinical acute kidney injury (defined as serum creatinine increase of ≥ 0.1 and < 0.3 mg/dl) and its relation to a composite end point of adverse in hospital outcomes.
Results:
Subclinical acute kidney injury was detected in 321 patients (17%). Patients with subclinical acute kidney injury had increased rate of the composite end point of adverse in-hospital events (20.3% vs. 9.7%, p<0.001), a finding which was independent of baseline renal function. Individual components of this end point (occurrence of heart failure, atrial fibrillation, need for mechanical ventilation and in-hospital mortality) were all significantly higher among patients with subclinical acute kidney injury (p< 0.05 for all). In a multivariable regression model subclinical acute kidney injury was independently associated with higher risk for adverse in-hospital events (odds ratio 1.92.6, 95% confidence interval: 1.23–2.97, p=0.004).
Conclusions:
Among STEMI patients treated with primary percutaneous coronary intervention, small, subclinical elevations of serum creatinine, while not fulfilling the consensus criteria for acute kidney injury, may serve as a significant biomarker for adverse outcomes.
Keywords
Introduction
Elevation of serum creatinine (sCR) resulting in acute kidney injury (AKI) is a frequent complication among ST segment elevation myocardial infarction (STEMI) patients undergoing primary coronary intervention (PCI), and is associated with adverse short and long term outcomes.1–6 Recent consensus classifications provide uniform criteria for AKI diagnosis including the RIFLE (Risk, Injury, Failure, Loss and End-stage Kidney Disease), 7 AKIN (AKI network) 8 and KDIGO (Kidney Disease: Improving Global Outcomes). 9 Emerging data suggest that about 15–20% of patients who do not meet the current sCr consensus criteria for AKI are nevertheless likely to have acute tubular damage.10,11 This subclinical AKI is diagnosed when renal damage or dysfunction does not reach the consensus threshold of sCr rise above 0.3 mg/dl. We investigated the incidence of small, subclinical sCr change (subclinical AKI) and its possible relation to in-hospital outcomes in a large cohort of STEMI patients undergoing primary PCI. We hypothesized that subclinical AKI would be associated with worse outcomes.
Materials and methods
Patients
A retrospective, single center observational study was performed at the Tel-Aviv Sourasky Medical Center, a tertiary referral hospital with a 24/7 primary PCI service.
Included were all 2281 consecutive patients admitted between January 2008 and May 2016 to the Cardiac Intensive Care Unit (CICU) with the diagnosis of acute STEMI.
Excluded were patients treated either conservatively or by thrombolysis (n=37), as were 82 patients whose final diagnosis on discharge was other than STEMI (e.g. myocarditis or Takotsubo cardiomyopathy). We also excluded patients who died within 24 h of admission (n=32) since we presumed there was insufficient time for subclinical AKI to occur, as well as patients requiring chronic peritoneal dialysis or hemodialysis (n=8) treatment. From the remaining 2122 patients we also excluded patients who were diagnosed with AKI according to the KDIGO criteria, defined as either a sCr rise > 0.3 mg/dl or more or an increase in sCr ≥1.5 times baseline within 48 h of hospital admission, compared with admission sCr 8 (n=225). The final patient population included 1897 patient whose baseline demographics, cardiovascular history, clinical risk factors, treatment characteristics and laboratory results were all retrieved from the hospital electronic medical records.
Protocol
Diagnosis of STEMI was established in accordance with published guidelines, including a typical chest pain history, diagnostic electrocardiographic changes, and serial elevation of cardiac biomarkers. 12 The study protocol was approved by the local institutional ethics committee. Primary PCI was performed in patients with symptoms ≤12 h in duration as well as in patients with symptoms lasting 12–24 h in duration if the symptoms persisted at the time of admission. Time to coronary reperfusion was defined as the time from symptom onset (usually chest pain or discomfort), recorded upon admission, to the restoration of Thrombolysis In Myocardial Infarction grade 3 flow in the infarct artery, as reported in the catheterization laboratory report. Following coronary interventional procedures, physiologic (0.9%) saline was given intravenously at a rate of 1 ml/kg per h for 12 h after contrast exposure. In patients with overt heart failure, the hydration rate was reduced at the discretion of the attending physician. The contrast medium used in procedures was iodixanol (Visipaque, GE healthcare, Ireland). Left ventricular ejection fraction was assessed in all patients, by bedside echocardiography, within the first 48 h of admission. Patient records were evaluated for the in-hospital course and occurrence of adverse outcomes. These included the development of heart failure episodes (defined as the occurrence of both clinical and radiological signs of congestion) treated conservatively, respiratory failure with the need for mechanical ventilation, new onset atrial fibrillation episodes as well as in-hospital mortality. These complications were united to form a composite outcome of adverse in-hospital events. The study protocol was approved by the local institutional ethics committee
Laboratory
The sCr level was determined upon hospital admission (prior to primary PCI) and at least once a day during the CICU stay and step down cardiology unit until hospital discharge and was available for all analyzed patients. The estimated glomerular filtration rate was estimated using the Chronic Kidney Disease Epidemiology Collaboration equation. 13 Baseline chronic kidney disease (CKD) was categorized as admission estimated glomerular filtration rate (eGFR) of ≤60 ml/min per 1.73 m. 14 Subclinical AKI was defined as a sCr rise ≥ 0.1 and < 0.3 mg/dl within 72 h of hospital admission, compared with admission sCr.
Statistical analysis
All data were summarized and displayed as mean (± standard deviation) or median (inter-quartile range) for continuous variables and as number (percentage) for categorical variables. The distribution of each continuous outcome variable was evaluated for normality using Kolmogorov–Smirnov Z test. Continuous variables were analyzed with the Student t test or Mann–Whitney U test. Categorical variables were compared using the Pearson chi-square test. The influence of subclinical AKI on the risk for adverse in-hospital events was evaluated using multivariate logistic regression adjusted for all parameters found to be statistically different in the univariate analysis. A similar model was used to determine possible predictors of subclinical AKI. A two-tailed p value of < 0.05 was considered significant for all analyses. All analyses were performed with the SPSS 20.0 software (SPSS Inc., Chicago, IL, USA).
Results
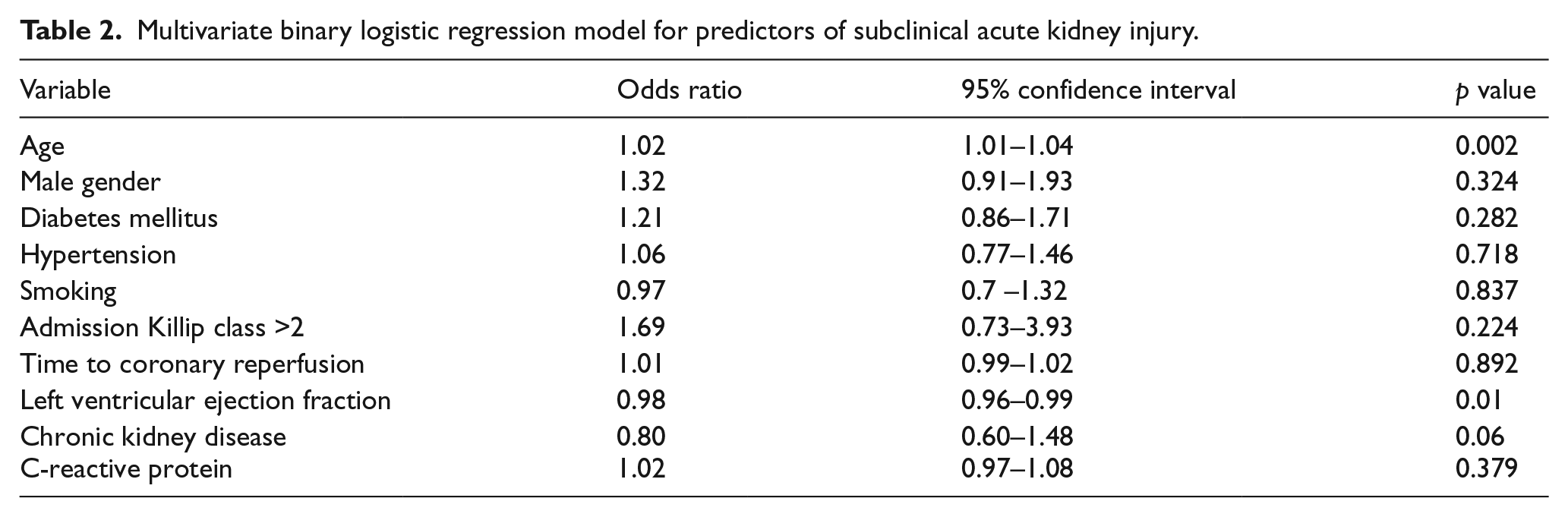
A total of 1897 STEMI patients treated by primary PCI were enrolled in the study, 321 of whom (17%) had subclinical AKI. The baseline clinical characteristics of patients with and without subclinical AKI are listed in Table 1. Patients with subclinical AKI were more likely to be older, of female gender, to have more co-morbidities, longer symptom duration and higher admission C-reactive protein level. Predictors of subclinical AKI included age, left ventricular ejection fraction and strong trend for CKD (Table 2).
Baseline characteristics, angiographic findings and laboratory results.
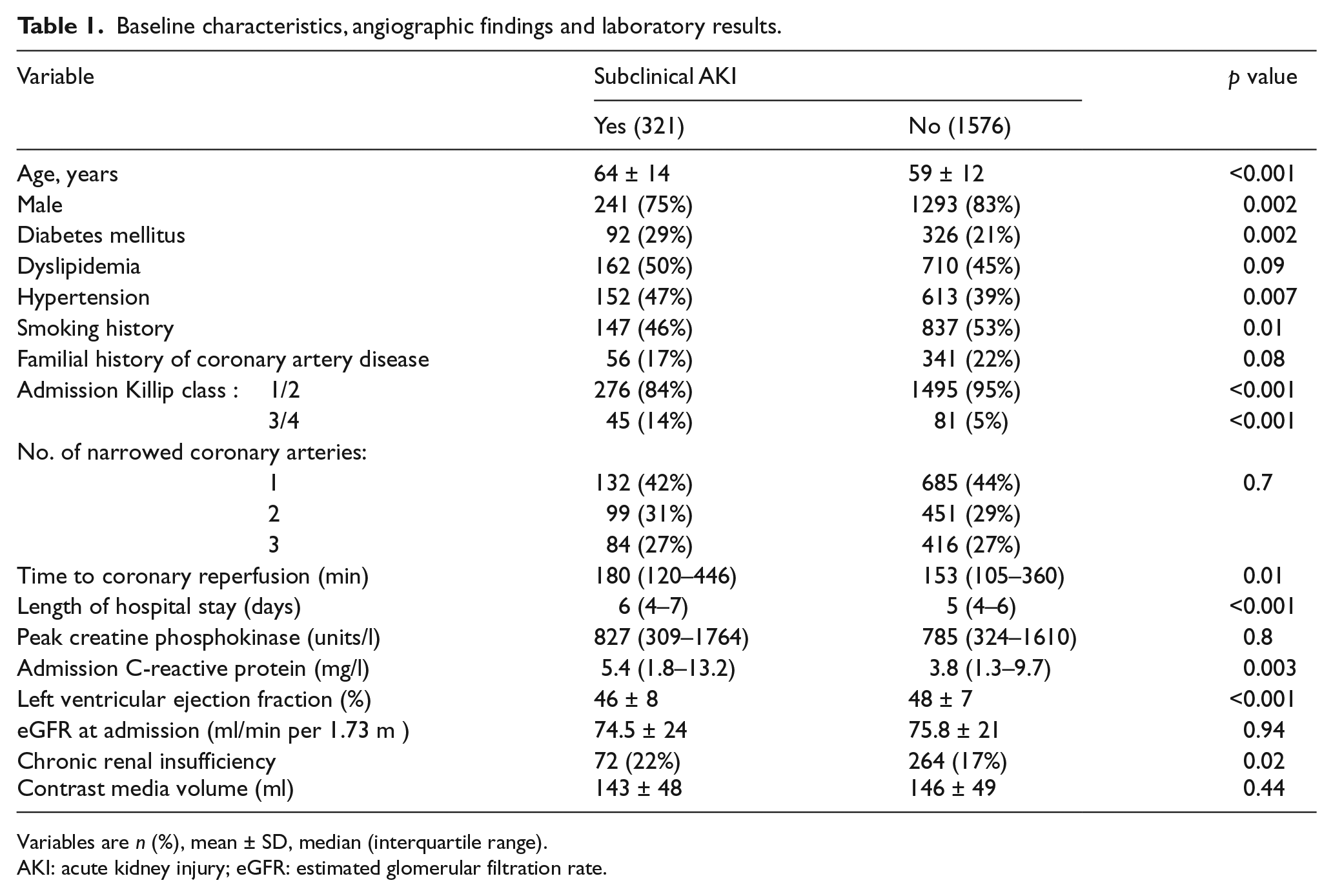
Variables are n (%), mean ± SD, median (interquartile range).
AKI: acute kidney injury; eGFR: estimated glomerular filtration rate.
Multivariate binary logistic regression model for predictors of subclinical acute kidney injury.
Subclinical AKI and in-hospital outcomes
Patients developing subclinical AKI had a twofold increase in the rate of the composite end point of adverse in-hospital events (20.3% vs. 9.7%, p<0.001). Individual components of this end point (occurrence of heart failure, atrial fibrillation, need for mechanical ventilation and in-hospital mortality) were all significantly higher among patients with subclinical AKI (Figure 1). Patients having subclinical AKI also had longer hospitalization (6.3 ±1.4 vs. 5.2 ± 1.3 days, p<0.001).
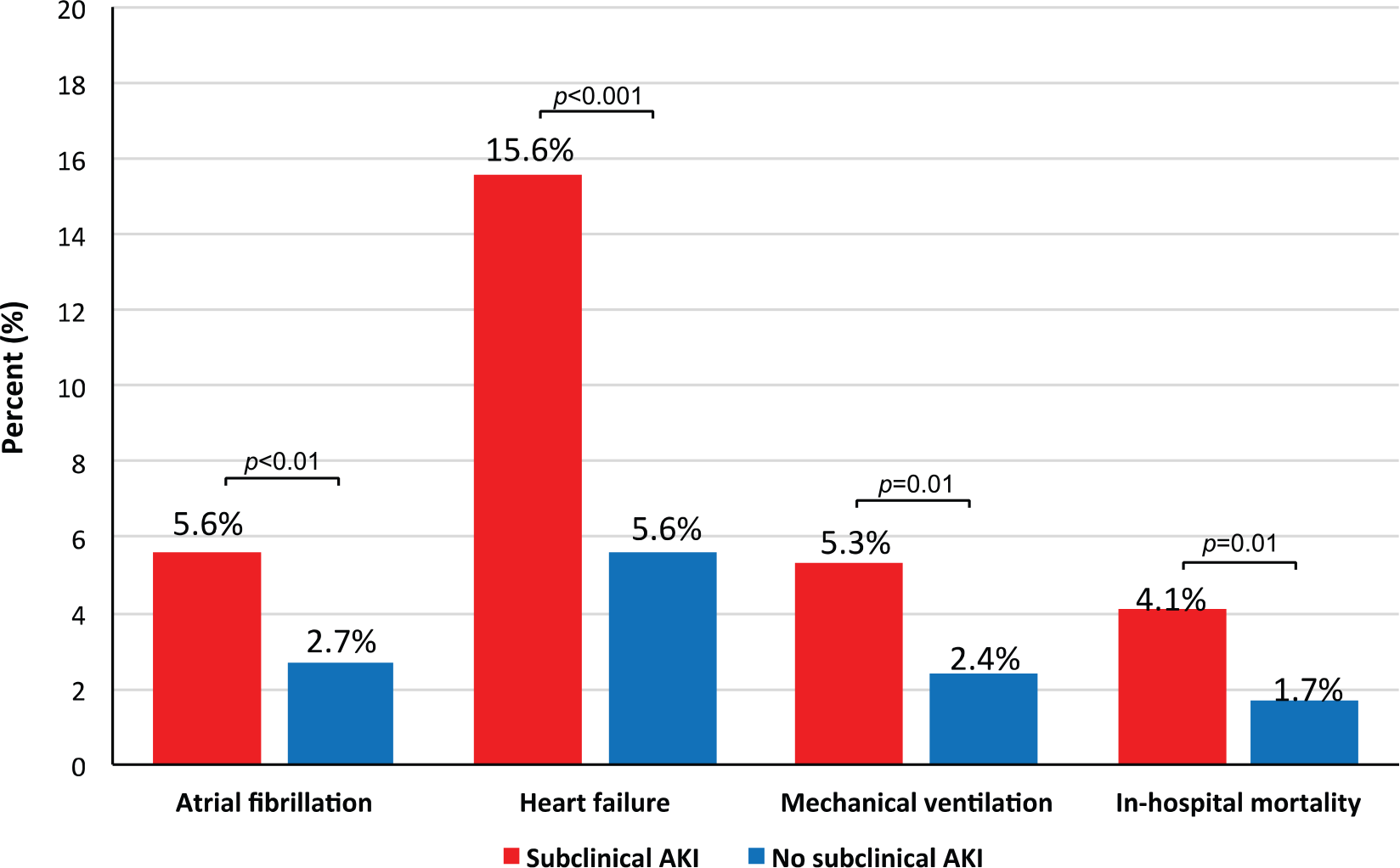
Rate of individual components of adverse in-hospital outcomes in patients with versus without subclinical acute kidney injury (AKI).
In univariate analysis, subclinical AKI was independently associated with adverse in-hospital outcomes regardless of the presence of baseline CKD (Figure 2). Among patients having both CKD and subclinical AKI the incidence of adverse in-hospital outcomes was fivefold higher compared with patients without renal insufficiency and no subclinical AKI (37.5% vs. 7.7%). Subclinical AKI was independently associated with higher risk for adverse in-hospital events (odds ratio 1.92.6, 95% confidence interval: 1.23–2.97, p=0.004). Other factors associated with adverse in-hospital outcomes included left ventricular ejection fraction, C-reactive protein level and admission Killip class >2 (Table 3).
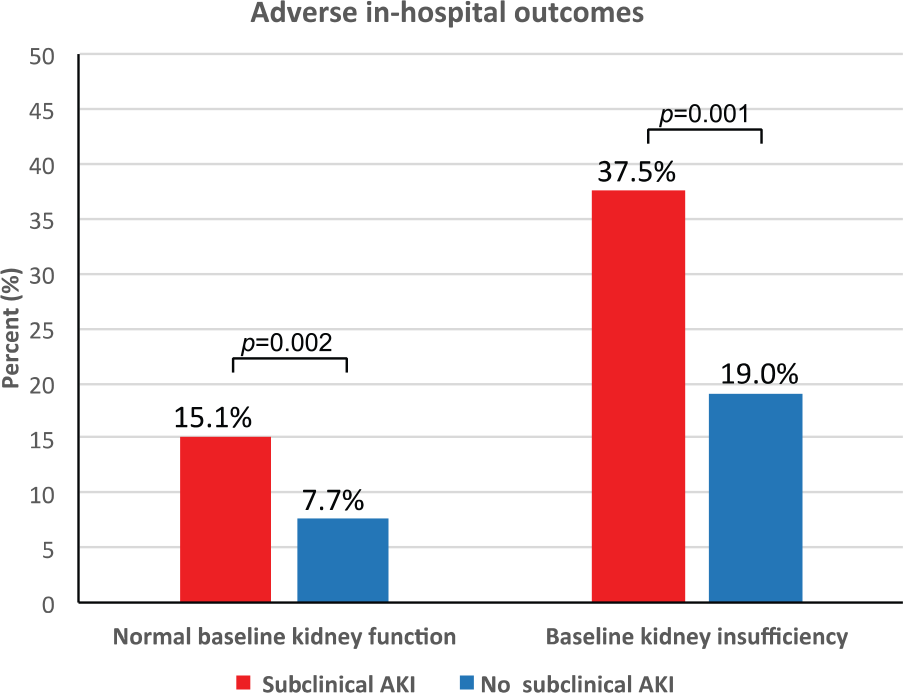
Rate of adverse in-hospital outcomes in patients with versus without subclinical acute kidney injury (AKI) according to baseline chronic kidney disease.
Multivariate binary logistic regression model for composite outcome of major in-hospital adverse events a .
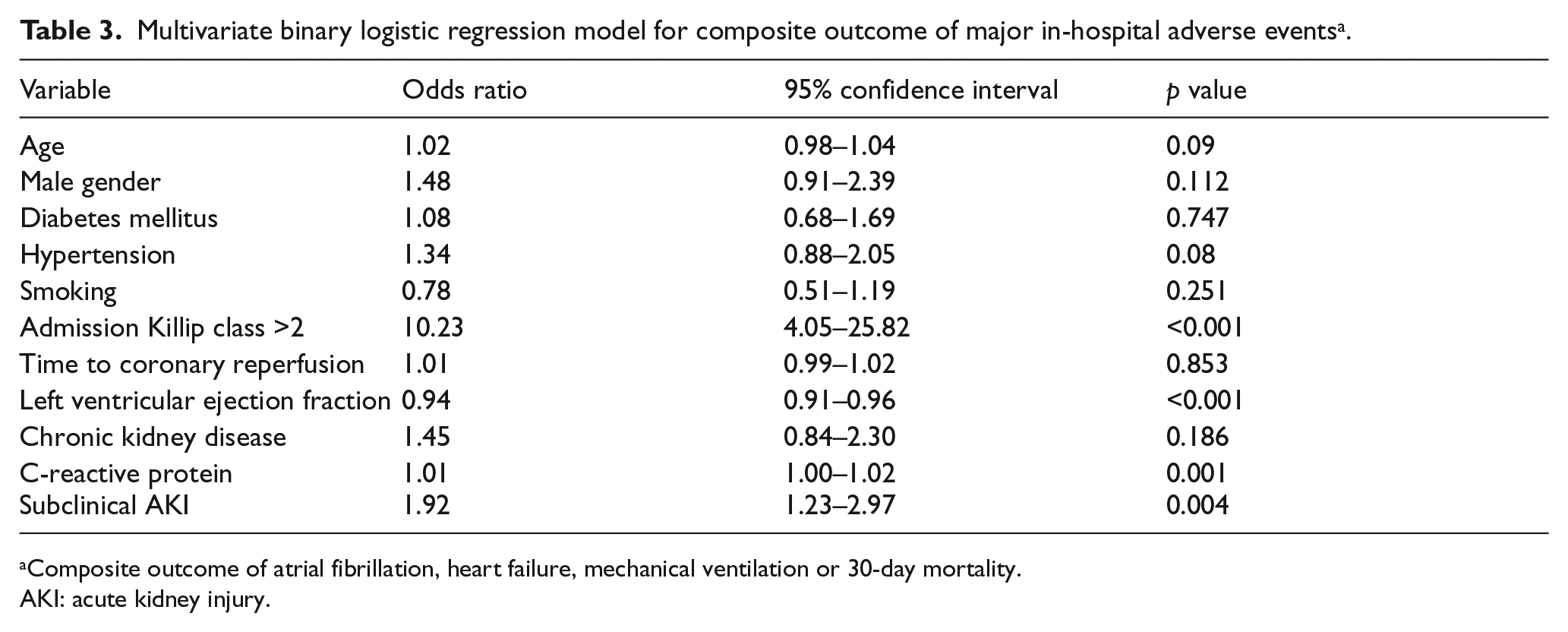
Composite outcome of atrial fibrillation, heart failure, mechanical ventilation or 30-day mortality.
AKI: acute kidney injury.
Discussion
Our study demonstrated that in a large population of STEMI patients treated with primary PCI, small, subclinical elevations of sCr, while not fulfilling the consensus criteria for AKI, were independently associated with a twofold increase in the risk for adverse in-hospital outcomes.
Worsening of renal function resulting in AKI is a frequent complication, known to be associated with adverse outcomes among STEMI patients undergoing primary PCI.1–6 Clinical AKI is diagnosed when renal damage and dysfunction reach a threshold sufficient to make sCr rise above 0.3 mg/dl within 48 h or when oliguria is present for over 6 h.8,9 However, such level of renal damage/dysfunction becomes evident only after the structure and function of nephrons that are part of the so-called renal functional reserve are affected. Because of a large renal reserve, up to 50% of kidney function may be lost before sCr rises. Furthermore, creatinine half-life is quite long and its variations over time are slow. The rise in sCr is a sign of a glomerular filtration alteration that has been ongoing for hours or days. In the case of a transient decrease in eGFR, sCr may never rise significantly and thus may not accurately depict kidney function until a new steady state has been achieved after eGFR has changed. Recent data suggested that even slight increase in sCr, under the critical value of 0.3 mg/dl, is associated with adverse outcomes.10,11
Lassnigg and colleagues found that small changes in postoperative sCr levels were associated with increased mortality following cardiac surgery. In their report, however, sCr level elevation was up to 0.5 mg/dl, beyond the consensus criteria used today. 15 Our findings are in accordance with a report by Tolpin and colleagues, who demonstrated that increase in sCr that did not meet current AKI criteria was independently associated with 30-day all-cause mortality in patients undergoing coronary artery bypass grafting. 16 In their report the effect was prominent mainly in patients without preexisting renal insufficiency, whereas in our report the effect of subclinical AKI was independent of baseline renal function.
While patients having diabetes were more likely to have subclinical AKI, diabetes was not independently associated with this finding.
Although our study was not designed to delineate the pathophysiologic mechanisms, we hypothesize that an increase in sCr levels may indicate a state of global tissue hypoperfusion. Recent data suggest that among STEMI patients, hemodynamic confounders related to the acuity of presentation can increase the risk for AKI via enhanced susceptibility to both contrast induced AKI and direct damage related to renal hypoperfusion. 6 Patients with subclinical AKI had longer symptom duration, higher C-reactive protein level and lower left ventricular ejection fraction, all previously shown to be associated with increased risk for AKI in STEMI patients.17–19
Our findings bear some important clinical implications. At the present time small subclinical changes in sCr following primary PCI are often neglected. Given our findings, a slight change in sCr (0.1–0.3 mg/dl) after STEMI and primary PCI may be used to identify a group of patients with early stages of organ dysfunction or tissue hypoperfusion. Our current findings therefore may highlight the importance of further investigation of sCr as a sensitive and early marker to be used in outcome management in this patient population. In a recent Acute Dialysis Quality Initiative consensus, a new perspective has been suggested for the diagnosis of AKI (or kidney attack), including a new category of kidney disorders defined by positivity of damage biomarkers and negativity of sCr or urine output criteria. 20 Similarly, the entity of subclinical AKI has recently been described characterizing those patients who display a slight increase in sCr under the critical value of 0.3 mg/dl so far utilized as the biochemical threshold to diagnose AKI. 11 As sCr is considered to be a relatively late biomarker for AKI, several novel biomarkers have been recently developed to improve the sensitivity and specificity of the early diagnosis of AKI.21–24 Neutrophil gelatinase-associated lipocalin, kidney injury molecule 1 and interleukin 18 are all novel biomarkers shown to improve ability to diagnose early renal tubular damage within hours of the initial kidney insult, and indicate renal structural damage, prior to functional loss, manifested by sCr elevation. The condition in which a tubular damage biomarker is positive, even in the absence of a rise in sCr (subclinical AKI), may become sufficient to trigger interventions and protective strategies for the kidney.
There is currently no effective prophylactic regimen available to prevent contrast-induced AKI. 25 Remote ischemic preconditioning (rIPC), defined as transient brief episodes of ischemia at a remote site before a subsequent prolonged ischemia/reperfusion injury of the target organ, is an adaptational response that protects against ischemic and reperfusion insult. Several studies demonstrated the tissue-protective effects of rIPC in various target organs, including the kidneys.26,27 In this regard, rIPC may offer a novel noninvasive and virtually cost-free treatment strategy for decreasing AKI incidence
We acknowledge several important limitations of our study. This was a single center retrospective and non-randomized observational study, and while an association was found between small rises in sCr and adverse outcomes, no causal relationship can be established. Patients having subclinical AKI were older, having more co-morbidities, lower left ventricular ejection fraction and higher C-reactive protein reflecting higher risk, which might have resulted in adverse in-hospital outcomes, and thus subclinical AKI may be a surrogate of characteristics of poor outcome. While we attempted to adjust for these confounding factors using the multivariate regression model, there might be several confounders not adjusted for which could have influenced results. The sCr levels were measured up to 72 h following hospital admission. As the change in sCr can lag beyond this period due to delayed effects of contrast material and drugs, worsening of renal function might have occurred following hospital discharge in some patients, the true incidence of subclinical AKI described in our study may have been underestimated. As data regarding medication throughout hospitalization, including the concomitant use of beta blockers, renin/angiotensin blockers and diuretics throughout hospitalization, were not present in many patients, their effect on AKI development, early left ventricular remodeling as well as clinical events, could not be assessed. In addition, no information was present on whether patients were submitted to single- or multi-vessel PCI procedure in a single or more than one procedure, thus omitting the possibility to observe their relation to renal function and clinical events.
Conclusions
Our results suggest that irrespective of sCr utility as a marker for acute changes in renal function, small subclinical increase may serve as a significant biomarker for adverse outcomes in STEMI patients undergoing primary PCI.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.