
Abstract
Background:
While coronary artery bypass grafting remains the standard treatment of complex multivessel coronary artery disease, the advent of peripheral ventricular assist devices has enhanced the safety of percutaneous coronary intervention. We therefore evaluated the safety in terms of inhospital outcome comparing protected high-risk percutaneous coronary intervention with the Impella 2.5 device and coronary artery bypass grafting in patients with complex multivessel coronary artery disease.
Methods:
This retrospective study included patients with complex multivessel coronary artery disease (SYNTAX score >22) undergoing either coronary artery bypass grafting before the implementation of a protected percutaneous coronary intervention programme with a peripheral ventricular assist device or protected percutaneous coronary intervention with the Impella 2.5 device following the start of the programme. The primary endpoint consisted of inhospital major adverse cardiac and cerebrovascular events. The combined secondary endpoint included peri and post-procedural adverse events.
Results:
A total of 54 patients (mean age 70.1±9.9 years, 92.6% men) were enrolled in the study with a mean SYNTAX score of 34.5±9.8. Twenty-six (48.1%) patients underwent protected percutaneous coronary intervention while 28 (51.9%) patients received coronary artery bypass grafting. The major adverse cardiac and cerebrovascular event rate was numerically higher in the coronary artery bypass grafting group (17.9 vs. 7.7%; P=0.43) but was not statistically significant. The combined secondary endpoint was not different between the groups; however, patients undergoing coronary artery bypass grafting experienced significantly more peri-procedural adverse events (28.6 vs. 3.8%; P<0.05).
Conclusion:
Patients with complex multivessel coronary artery disease undergoing protected percutaneous coronary intervention with the Impella 2.5 device experience similar intrahospital major adverse cardiac and cerebrovascular event rates when compared to coronary artery bypass grafting. Protected percutaneous coronary intervention represents a safe alternative to coronary artery bypass grafting in terms of inhospital adverse events.
Introduction
The revascularisation of patients with multivessel coronary artery disease (CAD) and multiple comorbidities presents a clinical challenge. While coronary artery bypass grafting (CABG) is still the standard of care for complex multivessel CAD represented by a high SYNTAX score, percutaneous coronary intervention (PCI) yields favourable results in less pronounced CAD.1–3 Besides individual anatomical considerations and technical feasibility, perioperative surgical risk in terms of comorbidities distinctively influences the choice of revascularisation strategy and may render heart surgery impossible altogether. 4 Currently, PCI is the most frequently applied method of revascularisation and is used in an increasing number of patients. 5 Interventional techniques and materials in PCI have advanced considerably over recent decades, allowing for the treatment of more complex forms of CAD combined with a marked decline of peri-procedural and long-term complications. 5 However, treatment of complex multivessel CAD by PCI still holds some insidious pitfalls. Complex treatments and manoeuvres including prolonged balloon inflation or stent implantation may impair adequate coronary blood flow leading to hypotension, insufficient cardiac perfusion and the development of cardiac shock or even cardiac arrest. 6 This translates into increased peri-procedural and intrahospital adverse events, especially for high-risk patients with complex CAD and multiple comorbidities. 6 The use of haemodynamic support by peripheral ventricular assist devices may improve the safety of high-risk procedures in this subset of patients. The Impella 2.5 (Abiomed, Danvers, MA, USA) resembles a coaxial miniaturised rotary blood pump that may support the left ventricle with up to 2.5 l/minute of blood flow into the ascending aorta and may secure cardiac and systemic perfusion.7–9 The feasibility and safety of the Impella 2.5 device were demonstrated in the PROTECT-I and the PROTECT-II trials.8,9 Protected PCI supported by the Impella 2.5 device improved event-free survival at 3 months follow-up when compared to the intra-aortic balloon pump (IABP). 9 These promising initial experiences could furthermore be successfully translated into the real world setting. 10
There are currently no data available comparing the inhospital outcome of patients with high perioperative risk undergoing complex revascularisation by protected PCI with Impella 2.5 support compared to CABG. Therefore, the purpose of the present study was to evaluate the inhospital outcomes of patients undergoing revascularisation of complex multivessel CAD before and following the implementation of a protected PCI programme using the Impella 2.5.
Materials and methods
Study design
The study was designed as an observational, retrospective single-centre study. A distinct ‘protected PCI programme’ using the Impella 2.5 was implemented in our tertiary care institution in October 2015. We consecutively included patients presenting with multivessel CAD and severely reduced left ventricular ejection function (LVEF) undergoing protected PCI supported by Impella 2.5 between November 2015 and November 2016.
This cohort was compared with consecutive patients with multivessel CAD and severely reduced LVEF undergoing CABG between October 2014 and October 2015 before the implementation of the ‘protected PCI programme’.
Multivessel CAD was defined as: (a) the presence of greater than or equal to 75% luminal diameter stenosis in two or more major epicardial coronary arteries; or (b) the presence of greater or equal to 50% luminal diameter stenosis of the left main trunk (LMT). Severely reduced left ventricular function was defined as LVEF below 35% as evaluated by echocardiography.
Exclusion criteria were cardiogenic shock, defined as hypotension with systolic blood pressure less than 90 mmHg for more than 30 minutes or the need for supportive measures to maintain a systolic blood pressure above or equal to 90 mmHg and known contraindications for Impella 2.5 implantation.
Patient population
With the start of the ‘protected PCI programme’ in October 2015, two experienced interventional cardiologists assessed all patients in terms of patient-specific and lesion-specific properties that predict an increased peri-procedural risk according to the 2015 SCAI/ACC/HFSA/STS clinical expert consensus statement on the use of percutaneous mechanical circulatory support devices in cardiovascular care. 11 Patient-specific variables included increased age, reduced LVEF, symptoms of heart failure, diabetes mellitus, chronic kidney disease, prior myocardial infarction (MI) and peripheral arterial disease. Lesion-specific variables encompassed anatomical characteristics such as left main stenosis, bifurcation disease, ostial stenosis, heavily calcified lesions, chronic total occlusions and lesions that supply a large myocardial territory.
Consensus between the two interventional cardiologists was reached that the respective patient was suitable for protected PCI or CABG. The final decision on which revascularisation strategy to use was made by an interdisciplinary heart team consisting of an interventional cardiologist, a cardiac surgeon and a cardiac anaesthetist taking into consideration the individual patient’s preference.
All patients included into the study before the implementation of the ‘protected PCI programme’ who underwent CABG were also assessed using the same principals described above and would have also been potentially eligible for treatment with protected PCI. The screening and inclusion of patients before and after the start of the ‘protected PCI programme’ are illustrated in Figures 1 and 2.
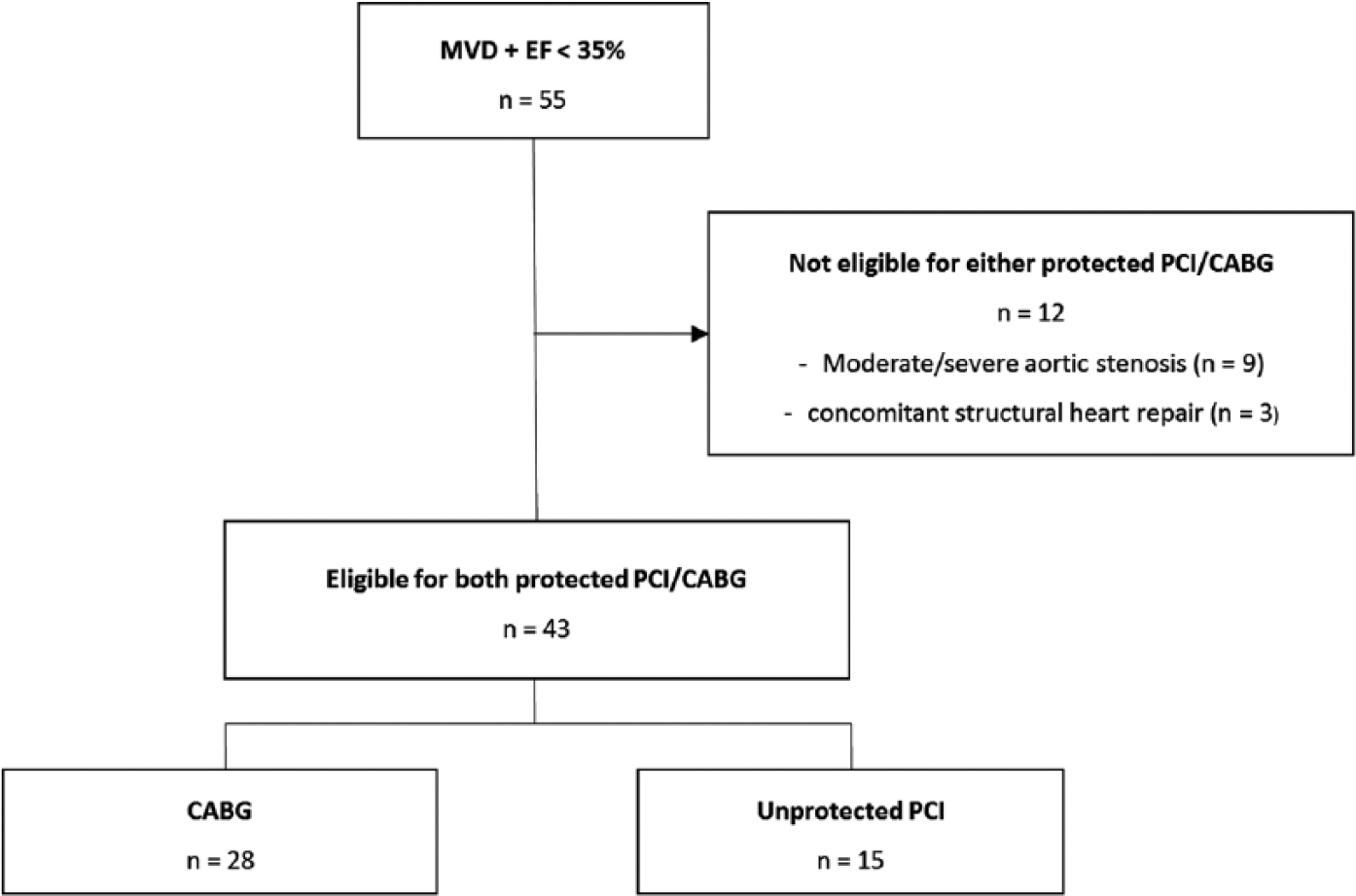
Screening and inclusion of patients before implementation of the peripheral ventricular assist device programme.
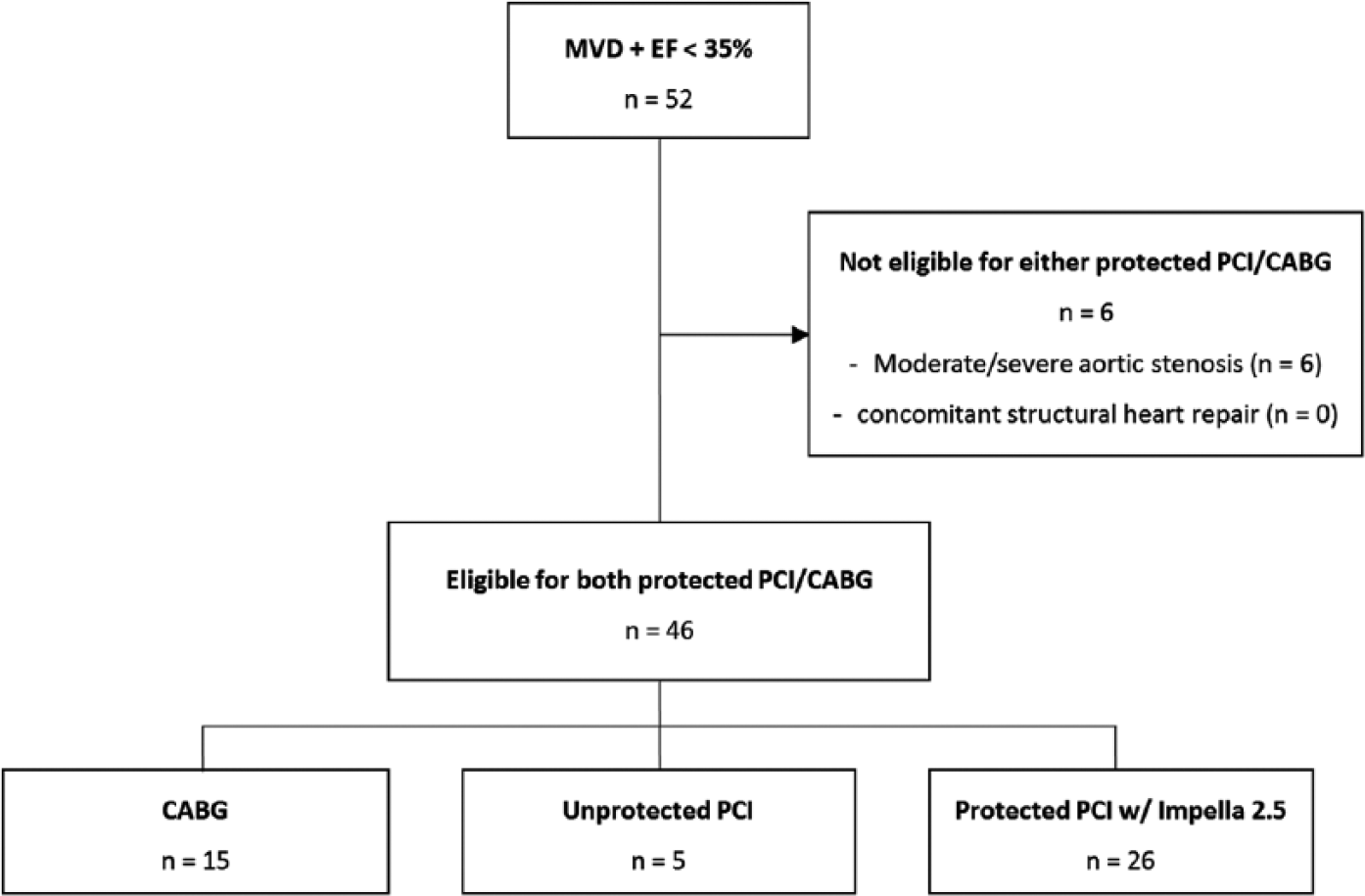
Screening and inclusion of patients after implementation of the peripheral ventricular assist device programme.
Protected PCI with Impella 2.5 left ventricular support
PCI was performed according to current societal guidelines and at the discretion of the treating interventional cardiologist. 12 Transthoracic echocardiography was conducted prior to the implantation of the Impella 2.5 to rule out relevant aortic valve pathologies and left ventricular thrombi. Placement of the Impella 2.5 was carried out according to the manufacturer’s instructions before the start of the PCI. A pre-close technique was used to facilitate sheath removal by insertion of two 6 F Perclose Proglide (Abbott Vascular Santa Clara, CA, USA) devices prior to placing the vascular sheath. The device was left in place for a maximum of 24 hours after the intervention and provided up to 2.5 l/minute of haemodynamic support.
Coronary artery bypass grafting
CABG surgery was performed according to the 2011 ACCF/AHA guidelines for coronary artery bypass graft surgery at the discretion of the treating cardiac surgeon. 13
Primary and secondary endpoints
The primary endpoint of this study was defined as the occurrence of major adverse cardiac and cerebrovascular events (MACCEs) including all-cause mortality, MI, repeat target vessel revascularisation (TVR; both re-CABG or re-PCI) and stroke during inhospital follow-up.
MI included both spontaneous (>72 hours after procedure) and post-procedure (<72 hours after procedure) MI. Spontaneous MI was defined according to the third universal definition as elevation of cardiac biomarkers (either troponin or creatine kinase myocardial type (CK-MB)) above the 99th percentile upper reference limit used by the local laboratory. 14 Post-procedure MI was defined as elevation of cardiac biomarkers (either troponin or CK-MB) above five times the 99th percentile upper reference limit. In both cases, laboratory changes must occur in combination with ischaemic symptoms or the development of pathologic Q-waves or ST segment changes in at least two contiguous leads on electrocardiography.
TVR was defined as repeat revascularisation that involved the target lesion or target vessel. Stroke was defined as permanent (longer than 24 hours), focal or global neurological deficits ascertained by a standard neurological examination and evidence of infarction on an imaging study.
The secondary endpoint was defined as a composite of peri and post-procedural inhospital adverse events. Peri-procedural adverse events must occur during the intervention or within the first 24 hours after it and contained cardiac arrhythmia, the need of an additional peripheral ventricular assist device (pVAD) as well as dissection of a coronary artery or aorta. Cardiac arrhythmia was defined as a sustained ventricular tachycardia, ventricular fibrillation or atrial fibrillation (AF) requiring cardioversion or cardiopulmonary resuscitation. Adverse events were considered post-procedural if they occurred more than 24 hours post-intervention. Post-procedural complications included cardiac arrhythmia, acute renal injury or failure, cardiac or vascular operation, pulmonary oedema, pericardial effusion (PE), post-procedural delirium and hospital-acquired pneumonia. Peri and post-procedural transfusion of packed red blood was also assessed per unit; however, the results did not count towards the secondary endpoint. Acute renal injury or failure was defined according to the Acute Kidney Injury Network as a rise in serum creatinine greater than two to three times and urine excretion less than 0.5 ml/kg/h over a period of more than 12 hours (kidney injury) or a rise in serum creatinine more than three times and urine excretion of less than 0.3 ml/kg/h for more than 24 hours or anuria for more than 12 hours (kidney failure). 15
Cardiac or vascular operation was defined as a post-procedural adverse event if there was a need for cardiac or thoracic operation, abdominal vascular operation or vascular operation for limb ischaemia or a need for surgery of the vascular access site. Post-procedural delirium was defined as acutely altered fluctuating mental status with features of inattention and an altered level of consciousness with the need for pharmacological therapy.
The study was carried out according to the principles of the Declaration of Helsinki and was approved by the medical ethics commission II of the Faculty of Medicine Mannheim, University of Heidelberg, Germany. The need for informed consent was waived due to the retrospective design of the study.
Statistical analysis
Statistical analysis was performed using SAS (version 9.04; SAS Institute Inc., Cary, NC, USA). Data are presented as means±standard deviation for continuous variables with a normal distribution, median with interquartile range for continuous variables with a non-normal distribution, and as frequency for categorical variables. The Kolmogorov–Smirnov test was used to assess normal distribution. Student’s t-test and the Mann–Whitney U-test were used to compare continuous variables with normal and non-normal distributions, respectively. The chi-squared test or Fisher’s exact test were used to compare categorical variables. A two-tailed P value of less than 0.05 was considered statistically significant in all tests.
Results
Baseline characteristics
A total of 54 patients (70.1±9.9 years, 92.6% men) were included in the study. Of these, 26 patients (48.1%) were revascularised using protected PCI while 28 patients (51.9%) received CABG. The mean SYNTAX score of all patients included in the study was 34.5±9.8 documenting severe CAD with no difference between the two groups (P=0.76). The EuroSCORE II was 4.4% and was also similar between both groups (P=0.49).
Cardiovascular risk factors were distributed evenly between the two groups. Patients undergoing PCI, however, had significantly more ST-segment elevation myocardial infarction (STEMI) as a main diagnosis (15.4 vs. 0.0%; P<0.05) combined with a lower incidence of stable CAD as an indication for revascularisation (15.4 vs. 50.0%; P<0.01). In terms of cardiovascular history, prior CAD was more prevalent in patients who underwent protected PCI (61.5 vs. 28.6%; P<0.05) combined with a higher incidence of prior CABG (19.2 vs. 0.0%; P<0.05). The mean number of coronary segments involved was significantly higher in patients treated with protected PCI compared to CABG (7.0±2.5 vs. 4.4±2.2 segments; P<0.001). The mean number of vessels involved per patient was similar in both groups (P=0.56) but differed concerning the individual involved major coronary vessels. Significant LMT stenosis was less prevalent in the protected PCI group (53.8 vs. 89.3%; P<0.01) while significant left anterior descending (LAD) artery stenosis was more often found in the protected PCI group (92.3 vs. 71.4%; P<0.05) together with significant left circumflex artery stenosis (96.2 vs. 75.0%; P<0.05). There were no significant differences concerning the New York Heart Association classification on admission and the number of patients presenting with angina pectoris CCS III or higher between both groups (all P>0.05). All baseline characteristics are shown in Table 1.
Demographic data, medical history, angiographic data and risk classification of patients with multivessel CAD who underwent protected PCI or CABG.
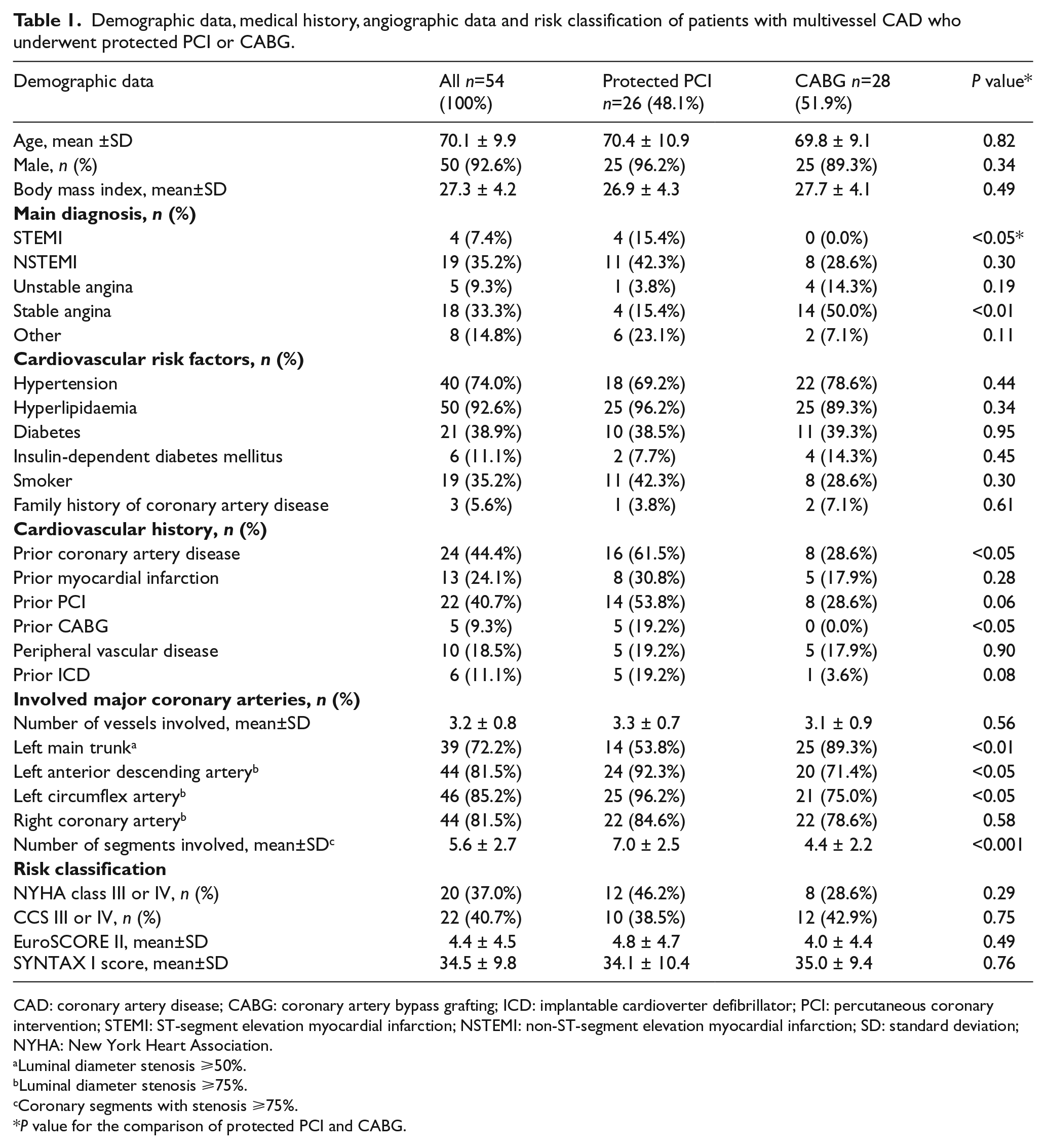
CAD: coronary artery disease; CABG: coronary artery bypass grafting; ICD: implantable cardioverter defibrillator; PCI: percutaneous coronary intervention; STEMI: ST-segment elevation myocardial infarction; NSTEMI: non-ST-segment elevation myocardial infarction; SD: standard deviation; NYHA: New York Heart Association.
Luminal diameter stenosis ⩾50%.
Luminal diameter stenosis ⩾75%.
Coronary segments with stenosis ⩾75%.
P value for the comparison of protected PCI and CABG.
Procedural characteristics
In the protected PCI group (n=26), a total of 120 stents were implanted with a mean diameter of 2.8±0.4 mm. The mean number of stents per patient was 4.6±2.2 with a mean total stent length of 113.1±61.3 mm. One patient (3.8%) received sirolimus-eluting stents, while all other patients received everolimus-eluting stents (96.2%).
In the CABG group (n=28), a mean of 2.2±0.4 grafts per patient were used. The mean number of arterial grafts per patient was 1.2±0.4 and the mean number of venous grafts was 1.0±0.6. All patients received a left internal mammary artery to LAD graft (100.0%) and two patients had an off-pump coronary bypass procedure (7.1%). The procedural characteristics for both groups are shown in Table 2.
Procedural characteristics of patients undergoing PCI or CABG.

Unless otherwise specified, data are means±standard deviation.
CABG: coronary artery bypass grafting; LAD: left anterior descending artery; LIMA: left internal mammary artery; PCI: percutaneous coronary intervention.
Primary endpoint
The duration of hospital stay was significantly longer in the CABG group compared to the protected PCI group (16.1 vs. 8.8 days; P<0.0.5). The primary endpoint of MACCEs occurred more often in the CABG group but did not show a statistical significance (17.9 vs. 7.7%; P=0.43). All-cause mortality was similar in both groups with two cases each (protected PCI 7.7% vs. CABG 7.1%; P=0.94). In the CABG group, there was one case of MI (3.6 vs. 0.0%; P=0.33), one case of repeat revascularisation (3.6 vs. 0.0%; P=0.33) and one case of stroke (3.6 vs. 0.0%; P=0.33).
Secondary endpoint (peri and post-procedural)
The secondary endpoint of minor inhospital adverse events occurred more often in the CABG group but remained without statistical significance (85.7 vs. 46.2%; P=0.21). When stratified for peri and post-procedural adverse events, there were more peri-procedural adverse events in the CABG group (28.6 vs. 3.8%; P<0.05). This was mainly driven by a tendency towards more cardiac arrhythmias in the CABG group (17.9 vs. 3.8%; P=0.10). The rate of post-procedural adverse events was similar between the groups (57.1 vs. 42.3%; P=0.61). However, PE occurred more often in the CABG group (10.7 vs. 0.0%; P=0.08). In addition, the inhospital need for transfusion differed significantly between both groups (0.0 vs. 67.9%; P<0.001), with a higher need for transfusion in CABG patients both peri and post-procedural. The adverse event and MACCE rate are shown in Table 3.
Major adverse cardiac and cerebrovascular events and inhospital adverse events of patients undergoing PCI or CABG.
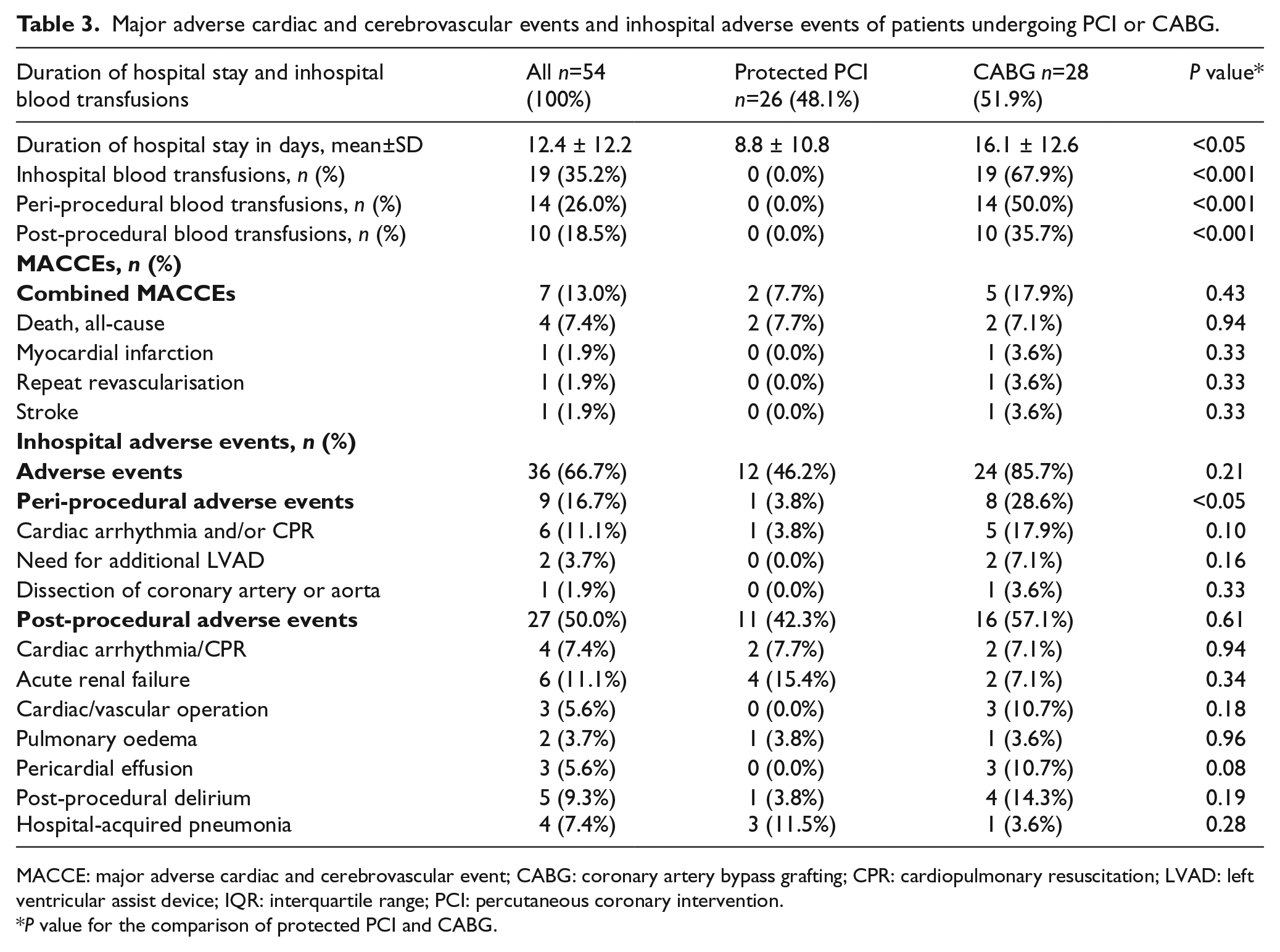
MACCE: major adverse cardiac and cerebrovascular event; CABG: coronary artery bypass grafting; CPR: cardiopulmonary resuscitation; LVAD: left ventricular assist device; IQR: interquartile range; PCI: percutaneous coronary intervention.
P value for the comparison of protected PCI and CABG.
Discussion
Balancing procedural risks and potential benefits of CABG against PCI in patients with complex multivessel CAD presents a challenge. Driven by the demographic development, predicted mortality risk among patients referred for CAGB as markedly increased during the past few decades. 16 Patients with a severely reduced LVEF undergoing CABG have a significantly increased mortality when compared to patients with normal LVEF. 17 Although this does not translate into decreased LVEF as an independent risk predictor for inhospital mortality in most studies, a combination of risk factors usually correlates with perioperative adverse events. 18 Furthermore, the characterisation of complexity of CAD reflected by the SYNTAX score provides an important tool for risk stratification, as a high SYNTAX score correlates with increased mortality in patients with left ventricular dysfunction. 19 Depressed left ventricular function is also a risk factor for increased 30-day mortality after CABG. 20 This emphasises the necessity of meticulous patient selection for either revascularisation strategy to reduce inhospital mortality and adverse events.
Twenty-two per cent of patients with multivessel CAD are deemed ineligible for CABG, either because of clinical considerations or patient preference. The ‘label’ of documented surgical ineligibility itself increases the risk of inhospital and long-term mortality. 21 To reduce inhospital mortality in this cohort, protected PCI may resemble a valuable alternative. Protected PCI has initially proved to be feasible in patients with complex multivessel CAD and severely reduced LVEF, with a MACCE rate of 20.0% in a cohort of 20 patients. 8 The Europella Registry, one of the biggest registries of Impella 2.5 use in protected PCI, has further demonstrated the safety and feasibility of the protected PCI approach with the Impella 2.5 device in a cohort of 144 patients in a real-world setting. 22 The primary endpoint, a combination of death, MI, stroke, urgent CABG and bleeding, occurred in 12.4% of patients of whom 48.6% presented with a severely depressed LVEF (ejection fraction <30.0%). Furthermore, a trend towards fewer MACCEs has been shown after 3 months in patients undergoing high-risk PCI when directly compared to IABP (40.6% in the Impella group vs. 49.3% in the IABP group; P=0.066). 9
Our study compared a reference cohort with complex CAD and depressed LVEF before the implementation of a protected PCI programme (thus undergoing CABG) and after implementation (thus undergoing high-risk PCI with Impella 2.5).
Our results demonstrate that protected PCI with Impella 2.5 support in high-risk patients reflected by a high SYNTAX score and markedly depressed left ventricular function yields comparable results to patients undergoing CABG in terms of inhospital MACCEs. With a MACCE rate of only 7.7% in the Impella group, our results showed improvement when compared to the above-mentioned trials. However, we reported inhospital MACCEs and not 30-day events. Furthermore, peri-procedural adverse events occurred less frequently in the Impella group together with a reduced necessity for blood transfusion.
The higher incidence of peri-procedural adverse events in the CABG group was driven by a strong tendency towards more cardiac arrhythmias. AF occurs in 15.0–40.0% of patients after CAGB while ventricular arrhythmias occur only in 0.4–1.4%. 23 In patients undergoing primary PCI, ventricular arrhythmia was reported in 4.3% of patients, while data on patients developing AF after PCI are not readily available. 24 However, both types of arrhythmia have a negative impact on prognosis. 25 Our data therefore are comparable to those of previous studies, with a higher incidence of arrhythmias both supraventricular and ventricular in patients undergoing CABG.
Although the overall frequency of post-procedural adverse events was similar in both groups, there was a tendency towards more patients with PE in the CABG group. PE is a common finding after cardiac surgery occurring in up to 64.0% of patients and is more often associated with CABG than with other types of surgery. 26 Although PE resolves without further therapeutic intervention in most cases, 1.9% of patients experience cardiac tamponade. PE may also occur after PCI mostly caused by coronary artery perforation; however, there was no such case in our study.
While blood transfusions are seldom required after PCI, the use of blood transfusion after CABG is highly variable between hospitals and ranges from 7.8% to 92.8%. 27 Dismal effects including stroke and increased early mortality have been linked to peri and post-procedural transfusion of red blood cells.28,29 Probably as a result of our small cohort size, the greater necessity for transfusions in the CABG group did not impact the overall MACCE rate.
Although boundaries regarding the eligibility for PCI treatment in indications formerly reserved for CABG seem to expand, as demonstrated in the recent EXCEL trial, it needs to be shown whether long-term results of protected PCI can compare to those of CABG. 30 In addition, pVADs in general and the Impella platform in particular evolve at a rapid pace. The haemodynamic support of up to 3.5 l/minute provided by the Impella cardiac power may further improve the efficacy and safety of the protected PCI approach. A recent publication reporting outcomes of patients with unprotected left main trunk undergoing protected PCI with Impella 2.5 and Impella cardiac power showed inhospital mortality as low as 1.57% and a 30-day MACCE rate of only 2.36%. 31 This highlights the need for additional studies focusing on the potential improvement of outcomes with the implementation of newer devices
Limitations
The present study is mainly limited due to the relatively small study cohort and the retrospective design without randomisation. The study combined inclusion periods before and after the implementation of our protected PCI programme. Considering the inherent differences between both groups in terms of the main diagnosis, cardiovascular risk factors and coronary morphology, a selection bias that may have affected the results of the study cannot be excluded. Second, the study was focused on peri and post-procedural complications and inhospital outcomes, while a longer clinical follow-up is pending. This short follow-up is likely to affect the CABG group negatively in terms of the primary endpoint, as patients with a high SYNTAX score undergoing CABG usually have a better long-term outcome when compared to PCI.
Conclusions
This is one of the first studies to compare inhospital outcomes of Impella 2.5-supported high-risk PCI versus CABG in the setting of complex multivessel CAD. Our data suggest that protected high-risk PCI with Impella 2.5 is safe, with similar MACCE rates when compared to CABG. Nonetheless, larger randomised controlled multicentre trials also providing long-term results are needed to confirm these findings.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.