
Abstract
Background:
Barriers in heart failure self-care contribute to heart failure hospitalizations, but geographic differences have not been well-studied. We aimed to compare self-care barriers in heart failure patients managed at tertiary centers in an Eastern (Singapore) versus a Western (USA) nation.
Methods:
Acute heart failure patients were prospectively assessed with a standardized instrument comprising of 47 distinct self-care barriers. The multi-equation generalized structural equation model was used to evaluate for geographic differences in barriers experienced, and association of barriers with outcomes.
Results:
Patient-related factors accounted for six out of 10 most prevalent self-care barriers among the 90 patients, with a median number of 11 barriers reported per patient. The Western patients reported a higher level of barriers when compared with their Eastern counterparts (median (interquartile range) 15 (9–24) versus 9 (4–16), p=0.001), after adjusting for demographics and co-morbidities. Many of these differences could be explained by geographic differences between the countries. There was no significant difference identified in all-cause mortality (19.4% versus 10.2%) and heart failure re-hospitalization (41.9% versus 45.8%) at six months between the groups.
Conclusions:
Self-care barriers are highly prevalent among acute heart failure patients, and differ substantially between East and West, but were not associated with geographic differences in outcomes.
Introduction
Heart failure (HF) is an important public health problem globally. Its natural course is characterized by chronic symptoms frequently interspersed with periodic exacerbations (acute decompensation) requiring emergent care and often hospitalization. Hospitalization marks a change in the natural history of the disease, with re-admission rates of 50% within the next six months, 1 and increased mortality in the year following hospitalization. 2
Inadequate self-care is increasingly recognized as an important contributor to HF hospitalizations. Self-care is a critical component of chronic HF management, and advocated as a method of improving outcomes from HF.3,4 HF self-care is a naturalistic decision-making process, involving behaviors to maintain physiological homeostasis (self-care maintenance) and responses to symptoms and signs (self-care management). 5 Prior studies evaluating HF self-care behaviors have established that self-care adherence is generally poor worldwide with notable distinctions between countries. Wide variations in non-compliance rates between countries are observed in multiple aspects of self-care such as weight monitoring (24% not monitoring in Australia versus 95% in Hong Kong), sodium restriction (18% not restricting dietary sodium in Netherlands versus 91% in Taiwan) and exercising (36% reported low rates of exercise in Germany versus 90% in Italy). 6 Similarly there are notable differences between countries with regards to self-care management and self-care confidence.6,7 Clearly, barriers to effective self-care exist with each patient experiencing multiple barriers at various levels (patient-, system- and environmental-levels).8,9 A systemic approach using human factors engineering models where barriers are viewed as products of a variety of patient, task, and environmental factors, may help us identify and better understand patients’ challenges (Figure 1).10,11 Geographic variations in self-care barriers are poorly characterized and may be due to differences in healthcare delivery, approaches to patient education and sociocultural factors.8,9,12 Understanding these differences is important for the development of region- and culture-specific effective approaches to improve self-care.
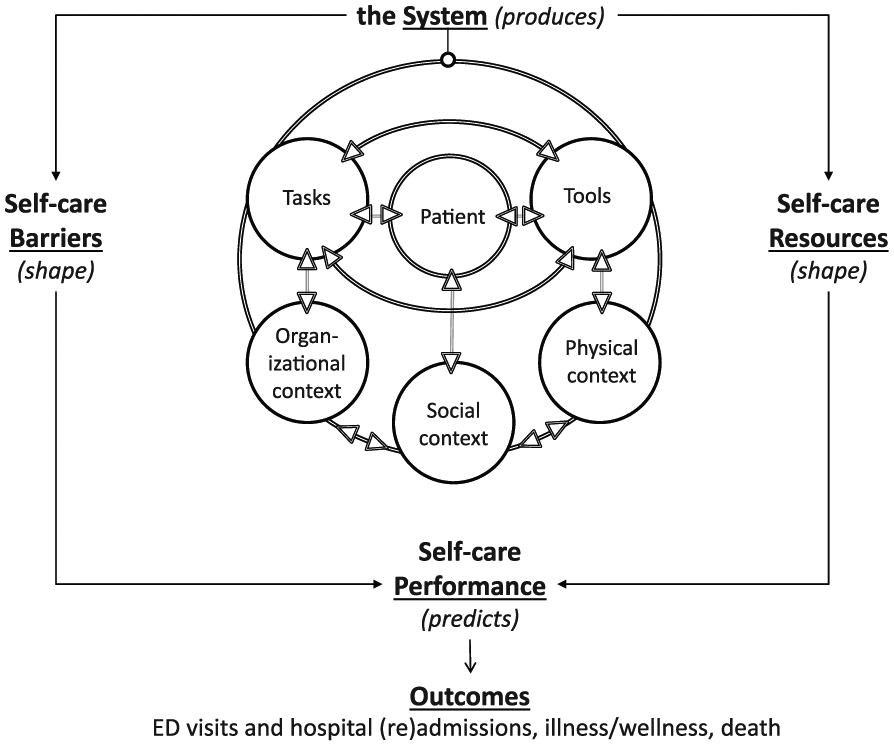
Sociotechnical systems of self-care barriers and resources. 13 Reproduced with permission from Annals of Emergency Medicine 2015; 66: 1–12, with permission from Elsevier 2015.
Using a patient-centered, sociotechnical systems model of self-care barriers among patients with HF, 10 we aimed to compare self-care barriers self-reported by patients admitted for acute HF (AHF) in the USA and Singapore, representing Western and Eastern HF populations managed by contemporary international HF clinical guidelines. We hypothesized that self-care barriers would be highly prevalent, and there would be notable geographic differences in reporting of self-care barriers.
Methods
Subjects
Adult patients were recruited using convenience sampling between June 2013–December 2014. Inclusion criteria included having a primary diagnosis of and being treated for AHF by the emergency department (ED) provider, and enrollment within 24 hours of hospital presentation. Patients were excluded if they were unwilling or too sick to participate in the study. All enrollees provided written consent for this study. This study was reviewed and approved by the Vanderbilt University Medical Center (VUMC) Institutional Review Board and National Healthcare Group Institutional Review Board.
Setting
This study was performed contemporaneously in two tertiary centers, at VUMC (Nashville, Tennessee, USA) and National University Hospital (Singapore). Patients were interviewed in the ED (VUMC) or wards (National University Hospital). The ED at VUMC receives approximately 700 patients with AHF annually, and National University Hospital receives 800 AHF admissions annually.
Methods of measurement and data management
A semi-structured instrument containing open-ended questions and structured barrier items was administered to eligible patients (Supplementary Material). This instrument was developed in English and piloted in 31 patients presenting to VUMC ED, and has been previously described. 13 This was translated to Malay and Mandarin for use in Singapore.
The instrument contained two open-ended questions, one at the start of the interview inviting patients to describe self-care barriers and one at the conclusion of the interview about additional information which may have been missed initially. The introductory question was followed by 47 structured barrier items and optional follow-up probes inviting patients to elaborate on the specific nature of barriers they indicated experiencing. These barriers were labeled as challenges in the instrument and covered an array of sociotechnical factors (patient, tasks, tools, physical environment, social environment, and organizational context). Participants indicated for each barrier item whether it “often,” “sometimes,” or “never” “makes it harder to take care of myself.”
Instrument feasibility was evaluated through patient participation rates, instrument administration time, and item non-response. The severity of patients’ comorbid conditions was quantified with the Charlson Comorbidity Index and its 10-year probability of survival. 14 Patients were followed up for six months, and data on all-cause mortality and HF re-hospitalization were collected.
Interviews were conducted by physicians (cardiologists or attending emergency physicians), non-clinical researchers or clinical research coordinators. The instrument was administered verbally, and patients’ responses were recorded in writing by the researchers. Information on demographics, medical history and laboratory test results were obtained from medical records. Data obtained from instrument and medical records were entered into a secure Research Electronic Data Capture (REDCap) database. 15
Data analysis
For exploratory purposes, the data were presented as frequency (%), mean±standard deviation (SD) or median with interquartile range (IQR), depending on the nature of data. Preliminary analyses were performed with chi-square test, Mann-Whitney test and independent t-test. The total and median number of barriers reported as “never,” “sometimes,” and “often” experienced by patients, as well as the proportion of patients responding “never,” “sometimes,” and “often” to each barrier were computed. Patients’ responses were dichotomized into “never” and “ever” (combining “sometimes” and “often”); the totals, medians and proportions on the dichotomized responses were computed.
A generalized structural equation model (gSEM)13,16 was applied to compare between cultures (1: Eastern, 2: Western), occurrence of HF re-hospitalization and mortality in terms of barriers experienced. The computed sociotechnical factors (e.g. patient, tasks, environment, and context) were ascertained if they were loaded significantly on the underlying construct of overall barriers, while adjusting for the effects of gender (0: female, 1: male), employment status (0: not employed, 1: employed) and Charlson probability of survival. The effects of the overall barriers and the specific factors on the occurrence of HF re-hospitalization (1: yes, 0: no) and mortality (1: dead, 0: alive) were tested with logistic regression-, while considering the effects of gender, employment status and the Charlson probability. A robust procedure was implemented to enhance the precision of the analysis. Analyzed with Stata MP V14 (Stata Corporation, Texas, USA), all statistical analysis were conducted at 5% level of significance.
Results
Characteristics of study sample
The study sample consisted of 90 (59 Eastern, 31 Western) patients with AHF (Table 1). Compared with their Western counterparts, the Eastern patients with AHF were more commonly male, with a greater proportion having received more than six years of formal education and employed at the time of interview. While more Eastern patients with AHF had diabetes mellitus and ischemic heart disease, the overall co-morbidity burden measured by Charlson Comorbidity Index and its estimated probability of survival was similar between groups. Left ventricular ejection fraction was also similar between groups.
Patient demographics and clinical characteristics.
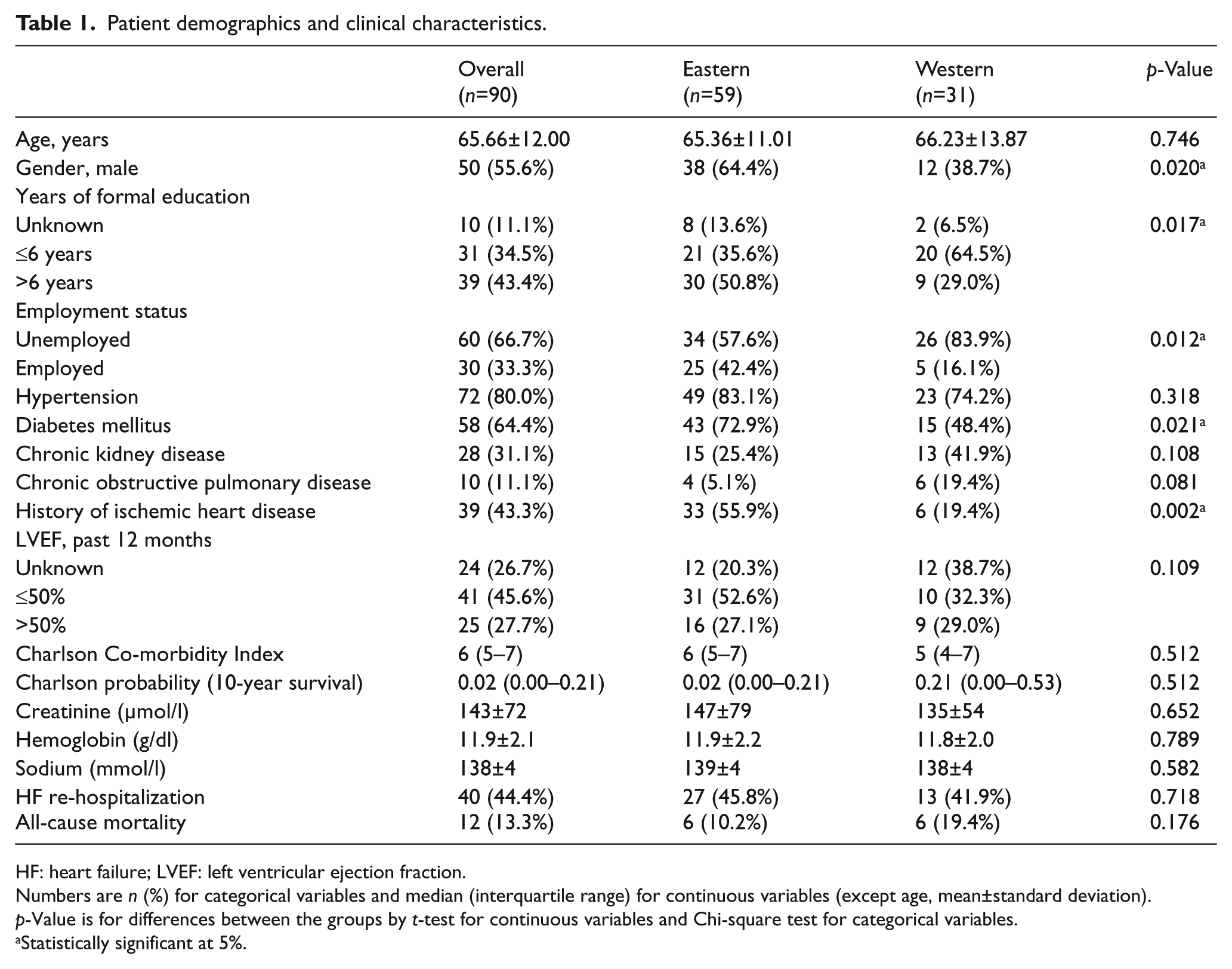
HF: heart failure; LVEF: left ventricular ejection fraction.
Numbers are n (%) for categorical variables and median (interquartile range) for continuous variables (except age, mean±standard deviation).
p-Value is for differences between the groups by t-test for continuous variables and Chi-square test for categorical variables.
Statistically significant at 5%.
Prevalence of HF self-care barriers
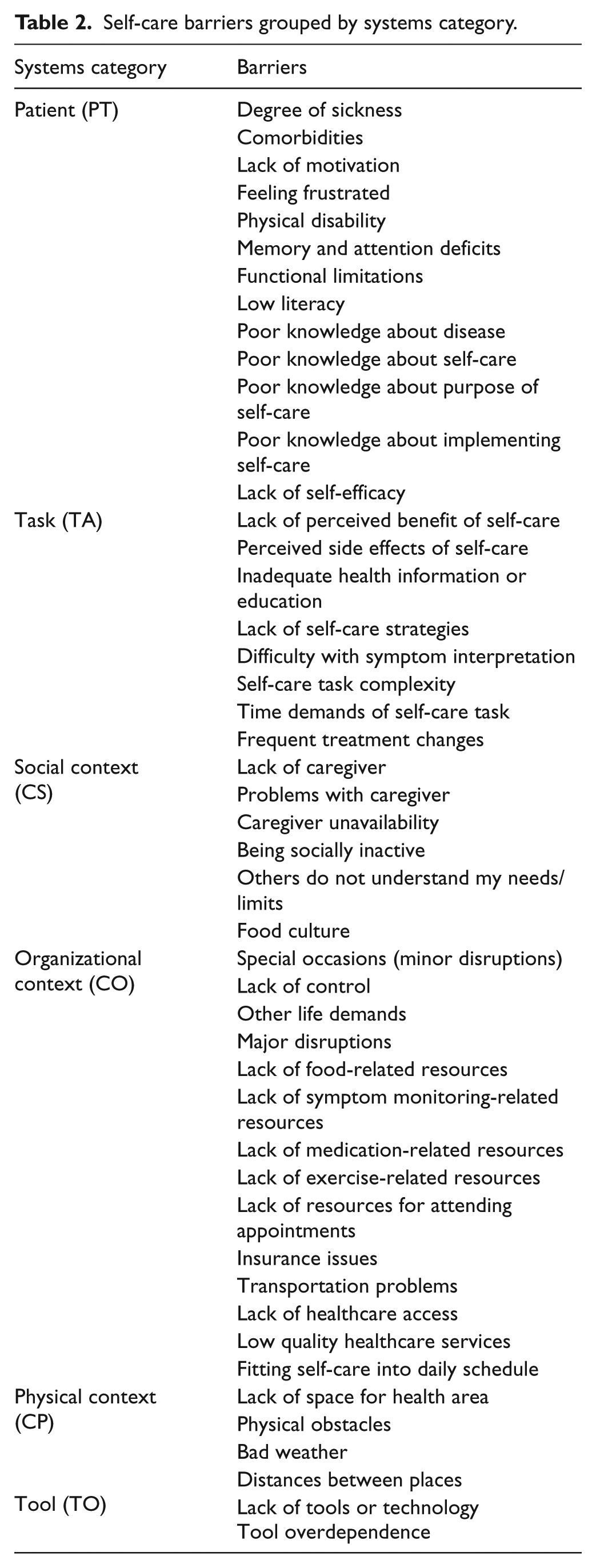
Among the identified self-care barriers (Table 2), 20 were reported as ever occurring in more than 25% of patients, with five of them present in more than 50% of patients. Patient factors accounted for six out of the 10 most prevalent barriers (Table 3). Apart from bad weather, the physical factors were infrequently perceived as barriers. Similarly, tool-related barriers were infrequently reported. There were no significant effects of gender, employment status, and disease severity identified for the factors of task and physical environment. However, patients who were employed had significantly fewer perceived patient barriers but more organizational context barriers.
Self-care barriers grouped by systems category.
Self-care barriers, in order of prevalence.
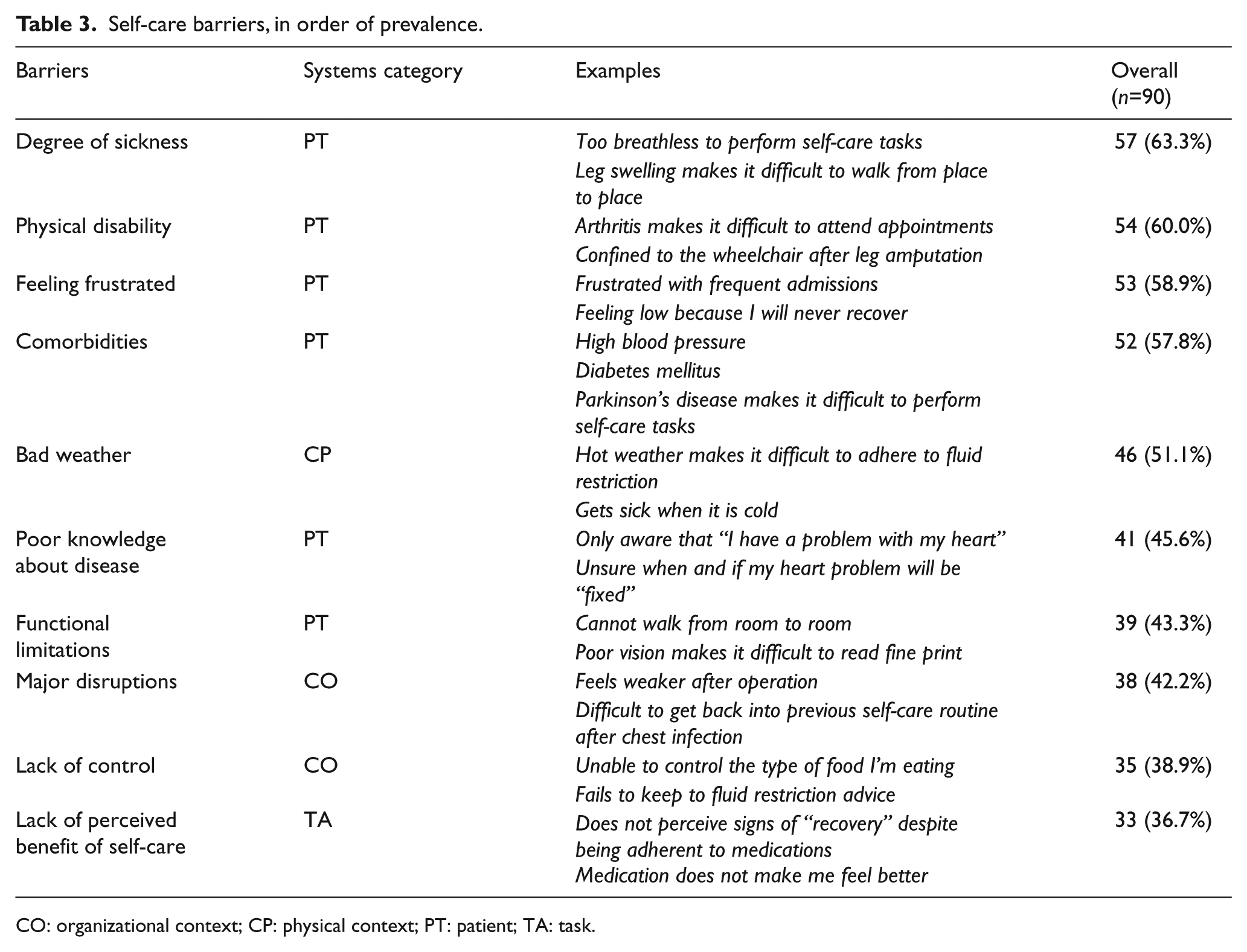
CO: organizational context; CP: physical context; PT: patient; TA: task.
The median number of barriers reported by the patients as ever being present was 11 (IQR 5–17) (Table 4). These multiple self-care barriers were sometimes related to one another i.e. clustered around a similar factor. The distribution of barriers varied among patients, with each patient presenting his or her unique barrier profile. The Western patients reported a significantly higher median number of barriers than their Eastern counterparts (median (IQR) of 15 (9–24) versus 9 (4–16), p=0.001). This was consistently seen across all barrier items with the exception of three items: no perceived benefit of self-care (task), weather (physical environment), and tool overdependence (tool). After adjusting for gender, employment status, and disease severity quantified by the Charlson Comorbidity Index, the difference in the perception of sociotechnical factors persisted between Western and Eastern patients, with the former reporting more barriers experienced.
Self-care barriers, East versus West.
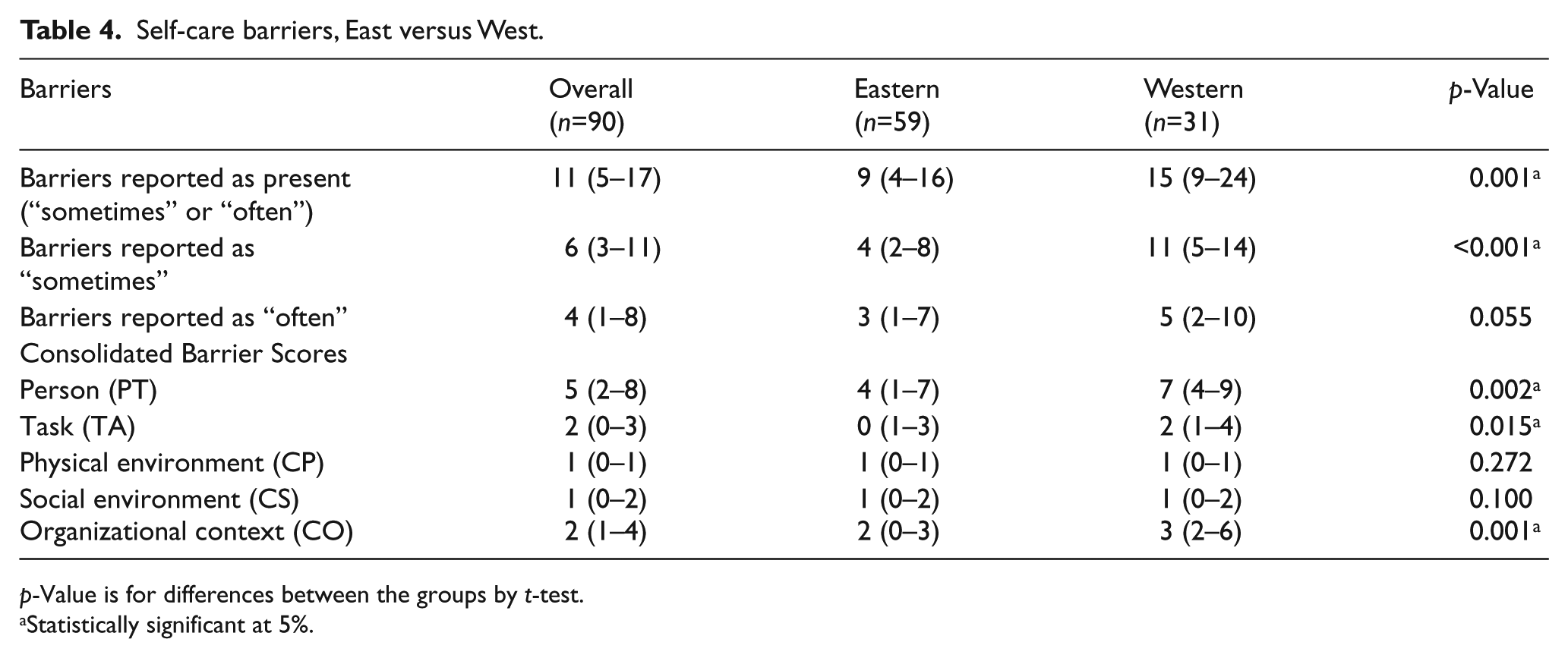
p-Value is for differences between the groups by t-test.
Statistically significant at 5%.
Feasibility of instrument administration
The majority of the patients approached were agreeable to participate, with less than 10% declining to be interviewed. Instrument administration took a median of 40 min, ranging from 20–90 min. The written copy of the instrument was infrequently used; almost all preferred the researcher to read aloud.
There were few items with no response. Notably, a majority of Eastern patients elected not to answer one (“Trouble doing the things I need to do for my health and fitting them all into my day”), which they felt was repetitive of a previous item (“Having a lot on my plate with day-to-day activities (work, taking care of others, church, etc.”). This item was subsequently removed from structural equation modeling.
Instrument assessment
Structured barrier items yielded significantly more information than open-ended questions, particularly amongst the Eastern patients. Only seven (12%) of Eastern and 13 (42%) of Western patients reported self-care barriers with the opening probe. Yet, all reported a number of barriers with the specific structured items. Similarly low response rates were seen with the closing probe. The responses usually re-emphasized a few more important barriers reported previously. A few cases yielded additional details about self-care barriers and self-care facilitators.
The sociotechnical factors of patient, physical environment, social environment, tasks, and organizational context were loaded positively and significantly on the underlying construct of barriers (Table 5). This suggests that, while the individual factors measured different aspects of barriers experienced, they were part of a unified measure or self-care barrier score.
Generalized structural equation modeling of the self-care barriers in heart failure patients and all-cause mortality. a
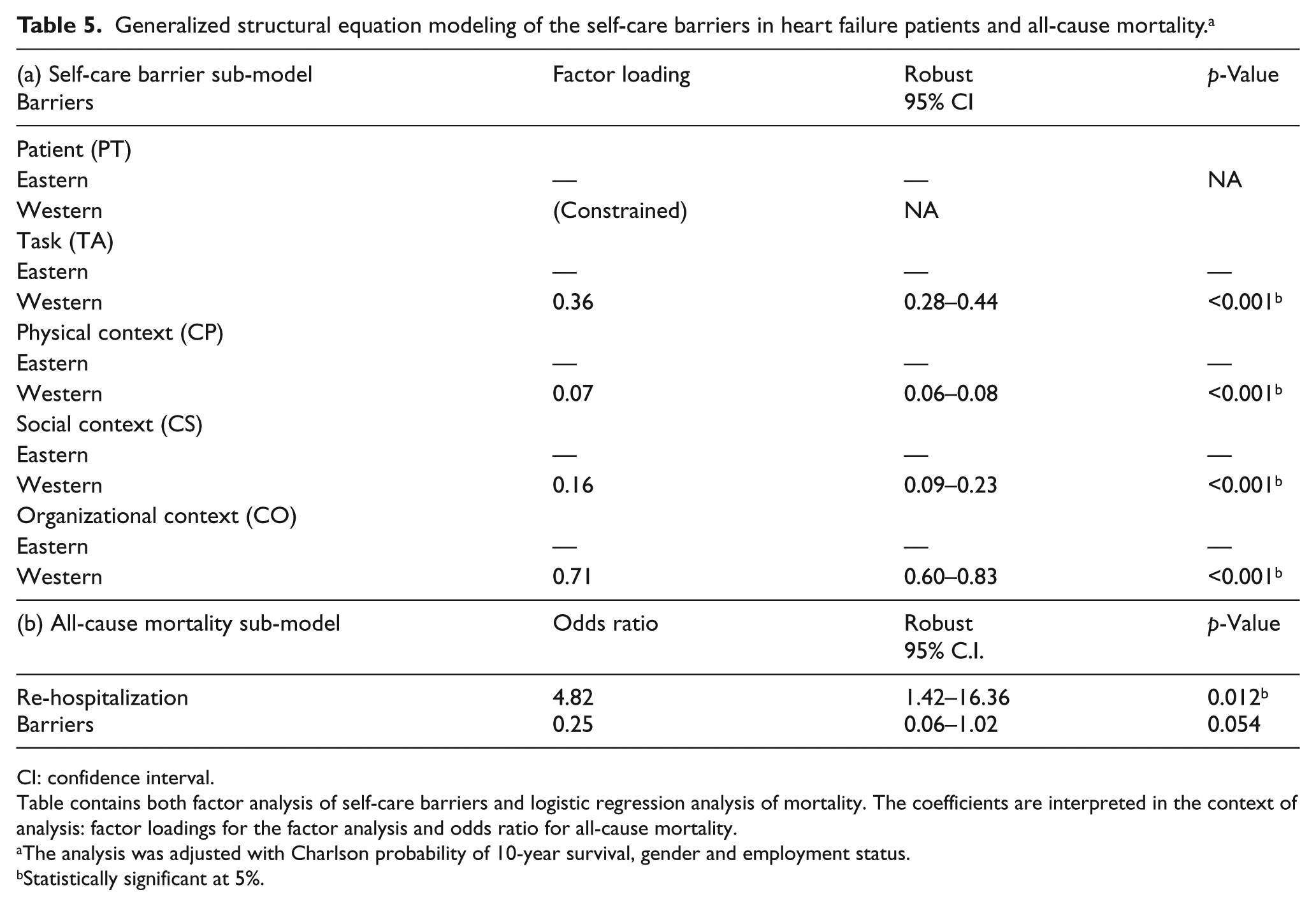
CI: confidence interval.
Table contains both factor analysis of self-care barriers and logistic regression analysis of mortality. The coefficients are interpreted in the context of analysis: factor loadings for the factor analysis and odds ratio for all-cause mortality.
The analysis was adjusted with Charlson probability of 10-year survival, gender and employment status.
Statistically significant at 5%.
Association with all-cause mortality and HF re-hospitalization
There were 27 (45.8%) Eastern patients and 13 (41.9%) Western patients who experienced re-hospitalization within six months (p=0.718). There were 12 deaths (six each in the two groups) and no East–West difference was established (p=0.176). While patients who had been re-hospitalized were facing a higher odds of death (AOR)=4.82; p=0.012), the barrier construct was not significant in explaining the sequential events of re-hospitalization and death according to the gSEM (Table 5). However, a further analysis suggested that patients who experienced more barriers in the physical environment (AOR=1.37; p<0.001) and the social environment (AOR=1.27; p=0.001) were more likely to suffer from re-hospitalization. None of the individual barriers scores was significantly associated with death.
Discussion
Using a semi-structured instrument in this cross-cultural study of 90 patients with AHF, we found self-care barriers were prevalent and varied between patients. The sources of barriers were predominantly related to patient, organizational context, self-care tasks, and physical environment, with less contribution from social context and tools and technologies. Western patients perceived a significantly higher level of barriers compared to Eastern patients, even after accounting for demographics, education and comorbidities. There was no East–West difference in all-cause mortality or HF hospitalization over six months despite the difference in barrier perception.
Prior qualitative studies evaluating factors impacting HF self-care found a myriad of barriers hindering self-care; 9 these barriers were present regardless of country. Similarly, a recent study identified some of these barriers as reasons for HF readmissions: psychosocial factors, sub-optimal self-care, inadequate access to and quality of professional support, severity of symptoms, and physiologic progression of disease. 17 HF readmissions are multi-faceted and the perspectives of patients and caregivers can differ from those of healthcare providers. 18 Our study is consistent with these studies, and further extended the findings by providing information on prevalence of barriers and geographical comparison.
Up to 50% of HF readmissions are thought to be preventable, through adequate self-care behavior.19,20 However, the adequacy of self-care behavior and barriers to effective self-care are rarely explored when patients are admitted. 17 Furthermore, patients are discharged from the hospital (including the ED) once they are deemed physiologically stable, often without consideration for non-clinical factors. 4 The various behavioral and psychosocial barriers plaguing these patients variably impact the adequacy of self-care and put them at high risk of early readmission. 21 The first step in addressing these barriers is early identification through a focused yet comprehensive instrument. Our data suggests that patients have variable barrier profiles; timely identification allows us to direct or develop relevant resources to address the patients’ individualized needs. 22
In our study, patients who were employed reported significantly fewer patient-related barriers, and more organizational barriers. This is not unexpected as employment is a reflection of age and education, thus explaining the fewer patient-related barriers. Patients who are employed need to juggle work commitments with chronic disease care, leading to more organizational-related barriers. The Western patients reported a significantly higher median number of barriers compared to Eastern patients. Furthermore, with the exception of five barriers, the barrier items were more often present amongst the Western patients. Some of these differences can be explained by the geographical differences between the countries. Singapore is a small, heavily-urbanized island city-state where the highest point is 164 m. Nashville is located in the Central Basin, surrounded by the Highland Rim, a region of hills, valleys and farmland. It is therefore unsurprising that few Eastern patients reported physical obstacles as a barrier, whereas more than one-third of Western patients reported physical obstacles as a barrier to self-care. Though not statistically significant, a lower proportion of Western patients perceived weather as a barrier compared to Eastern patients. Singapore is a tropical country, and its hot and humid weather makes it difficult for HF patients to adhere to fluid restriction. Cultural factors may account for some of the discrepancies in barriers across these two countries. Familism, which refers to strong feelings of belonging, responsibility and concern for one’s family, is an important cultural value in Eastern society. 23 The high level of family support and the tendency for Eastern patients to leave their health (and care of chronic diseases) in the hands of family members24,25 may explain their perception of fewer barriers to self-care.
Barriers were self-reported, and there was no correlation made with actual level of self-care or objectively assessed barriers. Eastern patients, particularly the older ones, tend to hold members of the medical team in high regard. It is conceivable that there may have been under-reporting of barriers by the Eastern patients, eager to please the medical team by “saying the right thing”. Indeed, more than 85% of Eastern patients in this study reported the desire to please doctors and nurses as a facilitator of HF self-care as compared to 58% of Western patients.
The event rates we observed are consistent with previous investigations.26–28 Although there was a significant East–West difference in the perception of self-care barriers, this did not translate into differences in outcomes. There are a few explanations for this. Our numbers may be too small to detect differences in outcomes. Indeed, this was designed as a descriptive study and was not adequately powered to detect differences in outcomes. While the presence of self-care barriers is likely to adversely affect HF self-care, the converse is not necessarily true. Patients who reported a lower number of HF self-care barriers may not have been practicing effective HF self-care. The finding that barriers in the physical and social environments are associated with HF re-hospitalization is noteworthy, indicating the importance of knowing the type of barriers present, not only their total count. To our knowledge, this has not been reported before and deserves further evaluation in a larger study.
While our study undertook a novel comparison of self-care barriers, it was limited by the small sample size and the participation of one hospital per country with a distribution imbalance between hospitals, limiting the ability to generalize our results. Patients who were excluded may be different in terms of demographics, clinical characteristics, and barriers experienced. Our high participation rate of 90% may ameliorate but would not eliminate this selection bias. It remains plausible that our participants may not have accurately reported the barriers, especially those which were too sensitive to report in front of caregivers or healthcare providers. The instrument was translated into Malay and Mandarin for use in Singapore, without prior rigorous validation. The translated versions may not have achieved semantic, conceptual, and normative equivalence, potentially impacting the internal validity of our findings. Lastly, knowledge of patients’ level of self-care and how that related to the barriers they reported would have been of great interest but was not available in this study.
Conclusion
Self-care barriers are highly prevalent among admitted patients with AHF, and differ substantially between East and West, but were not associated with geographic differences in six-month mortality and re-hospitalization.
Footnotes
Author contribution
RJH, ABS, SC, SLL, and CSPL conceived and designed the study. RJH obtained research funding. SC, KFM, SLL, KYL, and AC supervised enrollment and data collection activities. SPC conducted and reported the analysis. SLL and CSPL drafted the manuscript. All authors contributed to the manuscript and approved of the final version to be submitted.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This project utilized grant support from UL1 TR000445 National Center for Advancing Translational Sciences (NCATS) / National Institutes of Health (NIH) and K01 AG044439 National Institute on Aging (NIA) / National Institutes of Health (NIH). The opinions expressed are not those of NCATS or the NIH.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.