
Abstract
Diuretic resistance is a powerful predictor of adverse outcome in acute heart failure (AHF), irrespectively of underlying glomerular filtration rate. Metrics of diuretic efficacy such as natriuresis, urine output, weight loss, net fluid balance, or fractional sodium excretion, differ in their risk for measurement error, convenience, and biological plausibility, which should be taken into account when interpreting their results. Loop diuretic resistance in AHF has multiple causes including altered drug pharmacokinetics, impaired renal perfusion and effective circulatory volume, neurohumoral activation, post-diuretic sodium retention, the braking phenomenon and functional as well as structural adaptations in the nephron. Ideally, these mechanisms should guide specific treatment decisions with the goal of achieving complete decongestion. Therefore, volume overload needs to be identified correctly to avoid poor diuretic response due to electrolyte depletion or dehydration. Next, renal perfusion should be optimised if possible and loop diuretics should be prescribed above their threshold dose. Addition of thiazide-type diuretics should be considered when a progressive decrease in loop diuretic efficacy is observed with prolonged use (i.e., the braking phenomenon). Furthermore, thiazide-type diuretics are a useful addition in patients with low glomerular filtration rate. However, they limit free water excretion and are relatively contraindicated in cases of hypotonic hyponatremia, where acetazolamide is the better option. Finally, ultrafiltration should be considered in patients with refractory diuretic resistance as persistent volume overload after decongestive treatment is associated with worse outcomes. Whether more upfront use of any of these individually tailored decongestion strategies is superior to monotherapy with loop diuretics remains to be shown by adequately powered randomised clinical trials.
Learning objectives
To understand the concept of diuretic resistance in acute heart failure with its different definitions
To be aware of the prognostic significance of diuretic resistance in acute heart failure
To understand the mechanisms of diuretic resistance in acute heart failure
To develop a tailored approach to handle diuretic resistance in acute heart failure
Key points
Diuretic resistance in acute heart failure is defined either descriptively as the persistence of congestion despite adequate decongestive treatment, or quantitatively as low natriuresis / urine output / net fluid loss / weight loss / fractional sodium excretion per diuretic dose administered.
Irrespectively of its definition, diuretic resistance in acute heart failure is consistently associated with poor outcomes and this remains true when adjusting for underlying glomerular filtration rate.
Diuretic resistance tracks poorly with changes in glomerular filtration rate during decongestive treatment, but is more frequent in case of (more severe) underlying chronic kidney disease.
Diuretic resistance has multiple causes in acute heart failure including altered drug pharmacokinetics, impaired renal perfusion and effective circulatory volume, neurohumoral activation, post-diuretic sodium retention, the braking phenomenon and functional as well as structural adaptations in the nephron.
True diuretic resistance should be discerned from poor diuretic response due to electrolyte depletion or dehydration
The treatment approach to diuretic resistance in acute heart failure is focused ideally on the underlying mechanistic cause implied.
Introduction
Signs and symptoms of volume overload are the predominant reason for hospital admission in acute heart failure (AHF). 1 Loop diuretics are nearly ubiquitously prescribed for this indication and are the only applied therapy in a majority of cases. 2 Response to loop diuretic therapy may be assessed in many ways, either qualitatively (i.e. disappearance of clinical congestion signs or normalisation of cardiac filling pressures) or quantitatively (i.e. natriuresis, urine output, net fluid loss or weight loss). Emerging evidence indicates that response to decongestive treatment in general and loop diuretics in particular may be an independent prognostic factor in AHF. 3 The frequently encountered clinical problem of diuretic resistance in AHF therefore merits attention, especially because an evidence-based approach is lacking and different treatment strategies have failed to demonstrate meaningful benefits in randomised clinical trials.4–6 This review aims to discuss the concept of diuretic resistance in AHF, with its different definitions and underlying mechanisms, to provide a better pathophysiological insight and suggest an integrated treatment approach.
The goal of decongestion in AHF
Over the past few decades, immense progress has been made in the pharmacological and device treatment of chronic heart failure with reduced ejection fraction. Indeed, there has been a dramatic reduction in all-cause mortality, from approximately 40% to 20% within 2 years after presentation. 7 Unfortunately, this progress stands in stark contrast to the lack of advancements made in AHF, in which large randomised clinical trials have repeatedly failed to show a reduction in either mortality or hospital readmissions despite various different treatment strategies.4–6,8–10 Because there is little high-quality evidence to guide management decisions in AHF, treatment often remains empirical and according to local practice. One very consistent finding however – both from real-world observational data and post hoc analysis of clinical trials – is that persistent congestion is associated with worse outcomes after AHF. Indeed, even when coming at the cost of worsening renal function, better decongestion is associated with improved hospital-free survival. 11 A reasonable treatment goal in AHF is thus to pursue complete decongestion while trying to avoid iatrogenic harm, in particular with respect to the kidneys. As intravenous loop diuretics are prescribed in the overwhelming majority of patients to achieve this goal, it makes sense to search for and validate metrics of their efficacy. 3
Loop diuretic efficacy: prognostic marker or causal factor in AHF?
Working mechanism of loop diuretics
Loop diuretics inhibit the sodium–potassium–chloride cotransporter (NKCC2) at the luminal side of the renal tubules in the thick ascending limb of Henle’s loop, which accounts for approximately 25% of the total renal sodium reabsorption. 12 The primary pharmacodynamic effect of loop diuretics is therefore induction of natriuresis, chloruresis and kaliuresis. Yet, because they also impair the urinary concentration capacity of the kidneys dependent on the NKCC2, loop diuretics stimulate water loss as well as producing hypo to isotonic urine. 13
Loop diuretic efficacy
A very accurate metric for loop diuretic efficacy would be the sodium content of tubular fluid that exits Henle’s loop. To adjust for pharmacokinetics, one might subsequently correct for loop diuretic plasma levels. Of course, tubular fluid sampling is not achievable in patients with AHF and systemic assessment of loop diuretic plasma levels would be cumbersome. Therefore, alternative metrics have been proposed to assess loop diuretic efficacy in a more practical way. Although each has its strengths and limitations (Table 1), findings have been very consistent in demonstrating that poor loop diuretic efficacy – hence diuretic resistance – is associated with detrimental clinical outcomes (Table 2).
Strengths and weaknesses of different loop diuretic efficacy metrics.
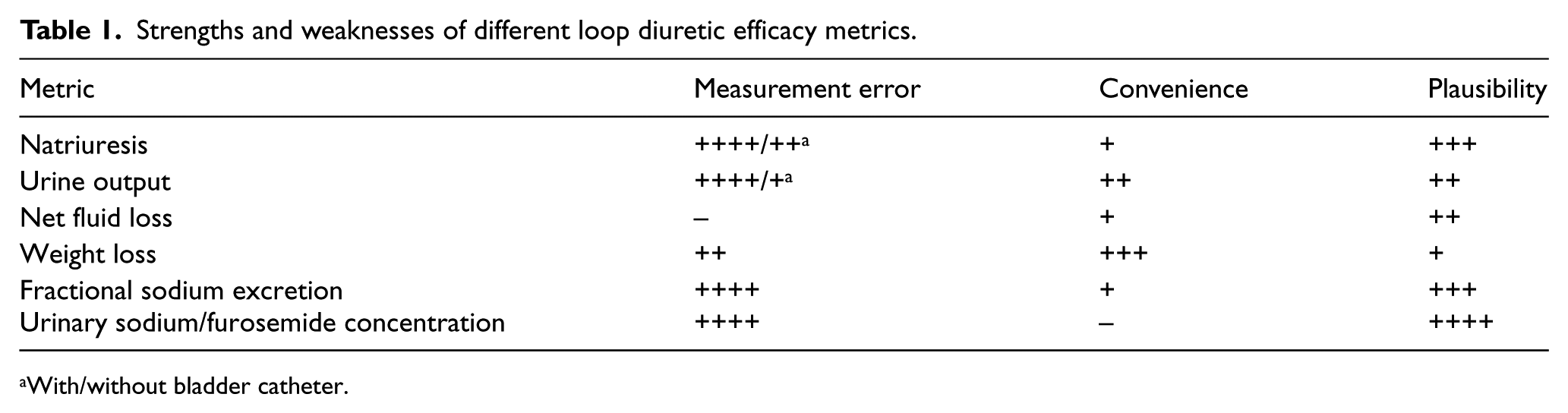
With/without bladder catheter.
Loop diuretic efficacy metrics and outcome.
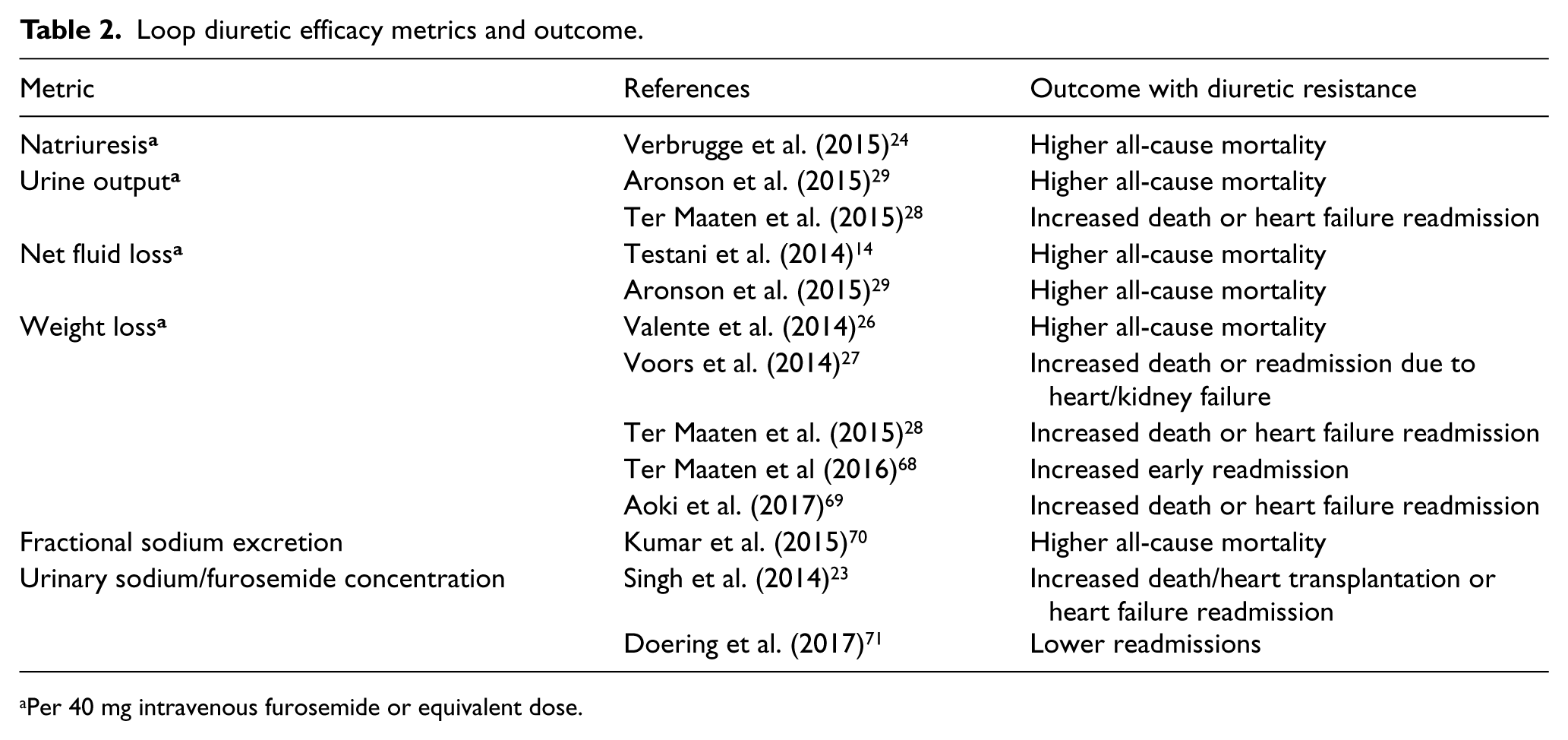
Per 40 mg intravenous furosemide or equivalent dose.
Loop diuretic efficacy and prognosis in AHF
The exact mechanistic underpinning of the robust association between loop diuretic efficacy and prognosis in AHF is less obvious than at first sight. A logical explanation might be that AHF patients who present with loop diuretic resistance have a lower chance of achieving appropriate decongestion. Yet, similar congestion signs were reported in some cohorts at discharge in patients with versus without diuretic resistance and still there was a difference in outcomes. 14 Alternatively, loop diuretic efficacy might be interpreted as a renal stress test, indicating the reserve function of the kidneys to excrete sodium and water in analogy to the maximal aerobic capacity being reflective of the cardiac reserve during exercise. Finally, poor diuretic response might also indicate that volume overload is not present and sodium levels are possibly depleted.15,16 In the latter scenario, diuretic therapy is unlikely to target the underlying pathophysiological culprit of AHF and may be harmful instead. Although diuretic resistance is clearly a risk marker in AHF, it remains an open question whether interventions that increase loop diuretic efficacy also lead to improved outcomes in AHF. This would make it a causal factor and hence an attractive end-point in future clinical trials. The answer to this question may also depend on the metric being used to define loop diuretic efficacy.
Strengths and weaknesses of loop diuretic efficacy metrics
Measurement error
An important issue with all metrics of loop diuretic efficacy is measurement error. Urine output is prone to substantial collection error in the absence of a bladder catheter, and even a simple measurement of weight can be hard to reproduce when patients are frail and unable to stand alone. Net fluid balance is the most susceptible to measurement error as both fluid intake and output must be assessed simultaneously. Indeed, even in rigorously collected data from large randomised clinical trials, the correlation between metrics such as weight loss and net fluid balance is very poor. 17
Convenience/complexity
Some metrics of loop diuretic efficacy require more effort to measure (i.e. net fluid balance) or need laboratory analyses and/or calculations (i.e. natriuresis, fractional sodium excretion, urinary sodium/furosemide ratio). In addition, although urinary indices may contain interesting information, their interpretation is not straightforward during diuretic therapy and requires more study, specifically in the context of AHF. 15
Biological plausibility
An important limitation of urine output, weight loss and net fluid balance is that these metrics do not distinguish between dehydration and decongestion, the latter being the removal of water and sodium. This distinction is relevant to make as arginine vasopressin antagonists (i.e. vaptans) that induce pure water excretion without impact on natriuresis relieve clinical congestion signs but have no impact on long-term outcomes after AHF. 18 It is important to recognise that most AHF patients actually have normal to high serum osmolality, reflecting total body water in proportion to solute content.19,20 As extracellular volume is governed by sodium and not water homeostasis, natriuresis and fractional sodium excretion may better capture long-term effects of loop diuretic therapy on volume status. 12
Glomerular filtration rate versus loop diuretic efficacy
Estimates of glomerular filtration rate (GFR) are widely used to assess renal function. GFR reflects the clearance function of the kidneys and therefore indicates well how toxic waste products are removed from the blood. In contrast, sodium and volume homeostasis is predominantly influenced by renal tubular function. 12 During decongestive treatment in AHF, only a modest correlation between worsening GFR and biomarkers of tubular injury has been found.21,22 This explains why loop diuretic efficacy tracks poorly with incident worsening renal function during decongestion and predicts outcomes in AHF irrespective of underlying GFR.14,23–25 That said, the frequency of diuretic resistance is clearly much higher with lower baseline GFR, when more advanced underlying chronic kidney disease is present.14,26–29 In conclusion, while GFR is an excellent marker for chronic kidney disease and hence a good risk marker for chronic heart failure when assessed in stable conditions, loop diuretic resistance performs better for prognostic stratification in AHF.14,30
Causes of loop diuretic resistance
Altered drug pharmacokinetics
Oral bioavailability
To exert their effects on the NKCC2 at the luminal side of the renal tubules, orally administered loop diuretics must first be absorbed from the gastrointestinal tract. Different pharmacological agents have shown substantial differences in oral bioavailability. While torasemide and bumetanide are almost completely absorbed (80-100%), furosemide demonstrates a highly variable oral bioavailability (10-100%), especially when intake is combined with food. 31 Food intake reduces the maximal plasma concentration of all loop diuretics by approximately 50%, but prolongs the time of their presence in the blood (Figure 1). As loop diuretic plasma levels need to exceed a critical threshold to induce natriuresis, food intake increases the risk of diuretic resistance, but in the case of diuretic efficacy effects are prolonged. In addition, in AHF with marked volume overload, especially when right heart failure is present, loop diuretic absorption may be impaired because of gut oedema and poor intestinal perfusion.32,33
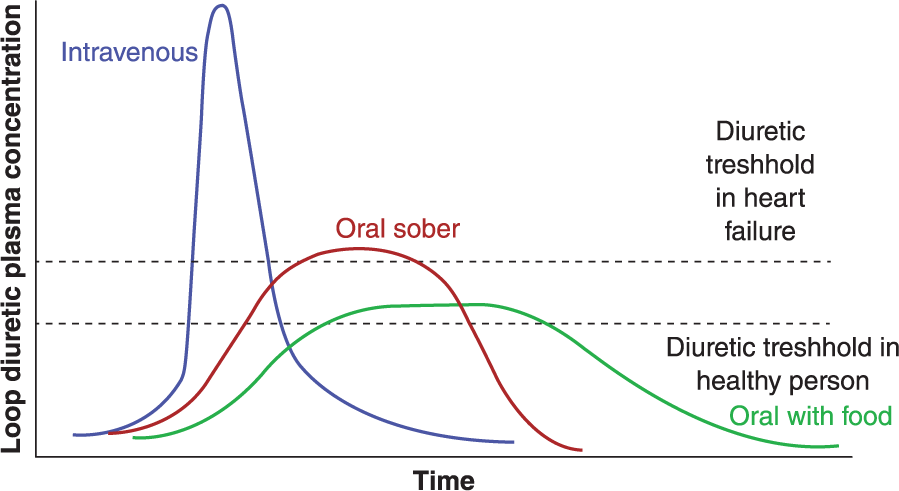
Loop diuretic pharmacokinetics.
Protein binding and tubular secretion of loop diuretics
Once absorbed, loop diuretics are more than 90% bound to plasma proteins. Therefore, the primary entrance of loop diuretics into the renal tubules is not through glomerular filtration, but rather through secretion by organic anion transporters and the multidrug resistance-associated protein 4 in the proximal tubules. 34 Uraemic anions compete with loop diuretic agents for proximal secretion, and the transport of both is inhibited by metabolic acidosis.35,36 This explains the shifted dose-response curve of loop diuretics in patients with chronic kidney disease (Figure 2). In addition, low plasma protein levels may decrease the amount of protein-bound loop diuretics offered to peritubular capillaries in the proximal renal tubules. Hence lower effective tubular concentrations of loop diuretics are reached for any given plasma level. Finally, significant proteinuria, as a result of glomerular or tubular damage, increases protein binding of loop diuretics in the renal tubular lumen, preventing their pharmacological action. 37
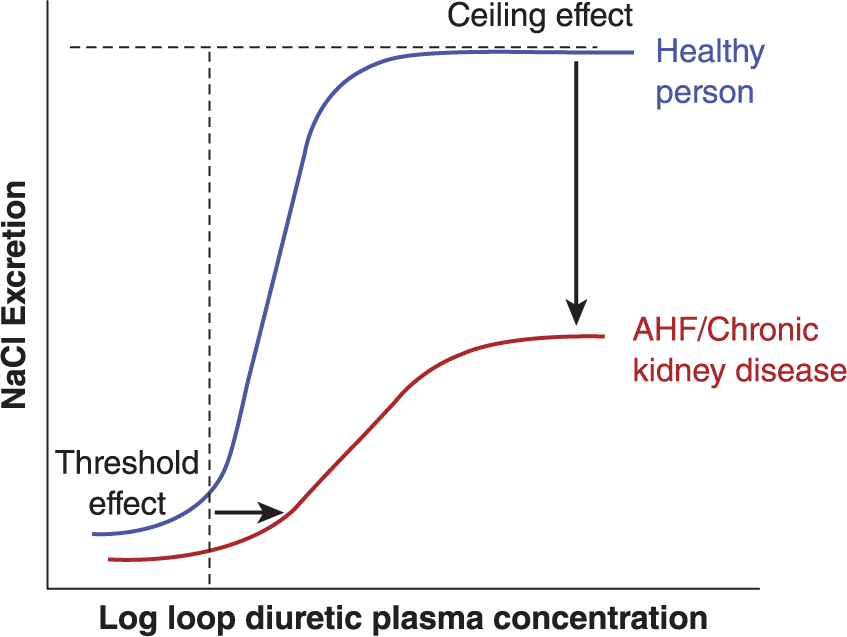
Loop diuretic dose–response curve.
Impaired renal perfusion and effective circulatory volume
In AHF, volume overload is often present outside the vascular compartment (i.e. interstitial oedema, ascites and pleural effusion) or pooled in systemic capacitance veins (mostly in the splanchnic circulation). 33 However, the kidneys are only able to regulate the effective circulatory volume. In normal circumstances, the plasma refill rate is approximately 3–4 mL/kg per hour, which explains how clinical congestion signs may disappear over time with diuretic therapy. Yet situations may occur in which renal perfusion is severely compromised and fluid cannot be recruited. Obviously, in case of low-output heart failure or cardiogenic shock, diuretic agents are ineffective and renal perfusion must first be restored. Furthermore, excessive abdominal congestion is associated with increased intra-abdominal pressure and poor renal perfusion that can be reversed by ultrafiltration or mechanical removal of ascites.38,39 Finally, evidence is accumulating that chronic sodium overload induces structural changes in the glycosaminoglycan content of the interstitial compartment that may promote oedema formation and impair the plasma refill rate.40,41
Neurohumoral activation, post-diuretic sodium retention and the braking phenomenon
Post-diuretic sodium retention
Loop diuretics directly stimulate renin release in the afferent arteriole, which is triggered by inhibited chloride transport via the NKCC2 in macula densa cells lining the renal tubular lumen at the end of Henle’s loop. 12 Indeed, low chloride concentrations inside macula densa cells depolarise their cell membrane, leading to paracrine signalling towards the nearby afferent arteriole where renin is ready to be released. With the renin-angiotensin–aldosterone system already potently activated in heart failure, this further contributes to sodium avidity in between moments of diuretic administration. This is especially relevant for furosemide and bumetanide that have a relatively short half-life (1-3 hours) in comparison with torasemide (approximately 6 hours). Post-diuretic sodium retention implies that when sodium intake is high, it can match or even exceed the loss achieved with intermittent loop diuretic administration (Figure 3). 42 Interestingly, although plasma renin activity increases acutely with appropriate decongestion, such a rise does not seem to translate into worse outcomes. 43 In contrast, neurohumoral activation accompanied by poor diuretic efficacy or persistent volume overload – hence diuretic resistance – clearly does.24,43
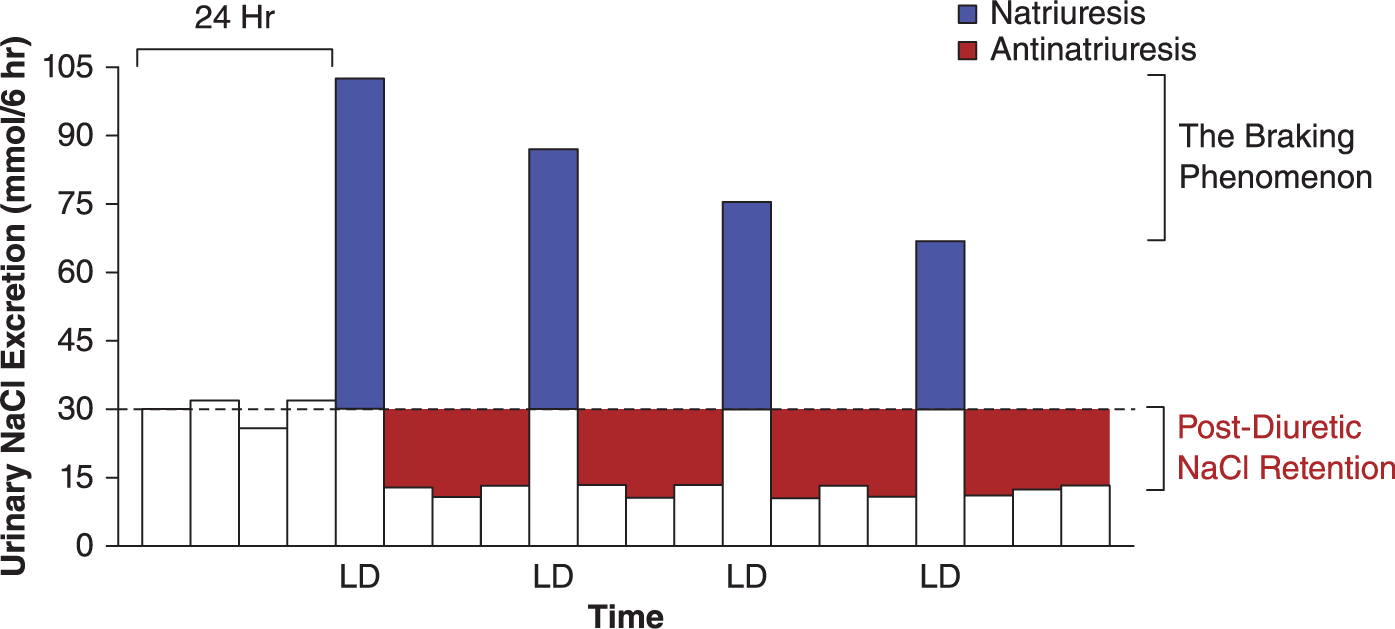
Post-diuretic sodium retention and the braking phenomenon.
The braking phenomenon
It is well known that with repeated administration of the same dose of loop diuretics, natriuresis decreases over time (Figure 3). This may indicate decreasing extracellular volume overload and removal of excess sodium with appropriate decongestion. 15 However, neurohumoral activation of the sympathetic nerve and renin–angiotensin–aldosterone system as well as structural and functional adaptations in the nephron may lead to an excessive braking phenomenon despite persistent volume overload.
Structural and functional nephron adaptations causing diuretic resistance
Distal nephron hypertrophy
Loop diuretics increase the sodium and chloride load delivered to the distal nephron. Over time, this exposure causes intrinsic renal adaptations that impair natriuretic efficacy (i.e. distal tubular hypertrophy and increased local aldosterone secretion) and are mediated by the thiazide-sensitive sodium-chloride symporter and sodium-independent chloride/iodide transporter or pendrin.44,45
Increased proximal tubular sodium reabsorption
For loop diuretics to be effective, enough substrate must be available to the NKCC2. In other words, enough sodium, potassium and chloride should pass through the tubular lumen at the level of the thick ascending limb of Henle’s loop. As explained above, adequate renal perfusion is a prerequisite to produce ultrafiltrate passing through the renal tubular lumen and maintain a normal GFR. Importantly, renal autoregulation mechanisms aim to preserve GFR initially, even when renal blood flow is already substantially depressed. 12 This can be explained by a higher fraction of plasma being filtered through the renal glomeruli when renal blood flow is lower. The result is thicker blood with a higher oncotic pressure entering the peritubular capillaries through the efferent arteriole. In turn, this stimulates isotonic reabsorption in the proximal renal tubules and may lead to substantially increased proximal tubular sodium reabsorption. 12 The consequence is that less sodium (and chloride) is offered to the more distal nephron and Henle’s loop, impairing loop diuretic efficacy. 12
Management approach to (loop) diuretic resistance in AHF
As the mechanisms of loop diuretic resistance in AHF are multifactorial, we propose an integrated management approach (Figure 4). It should be emphasised though, because of the lack of high-quality evidence from randomised clinical trials, such recommendations rely heavily on pathophysiological insights and observational data.
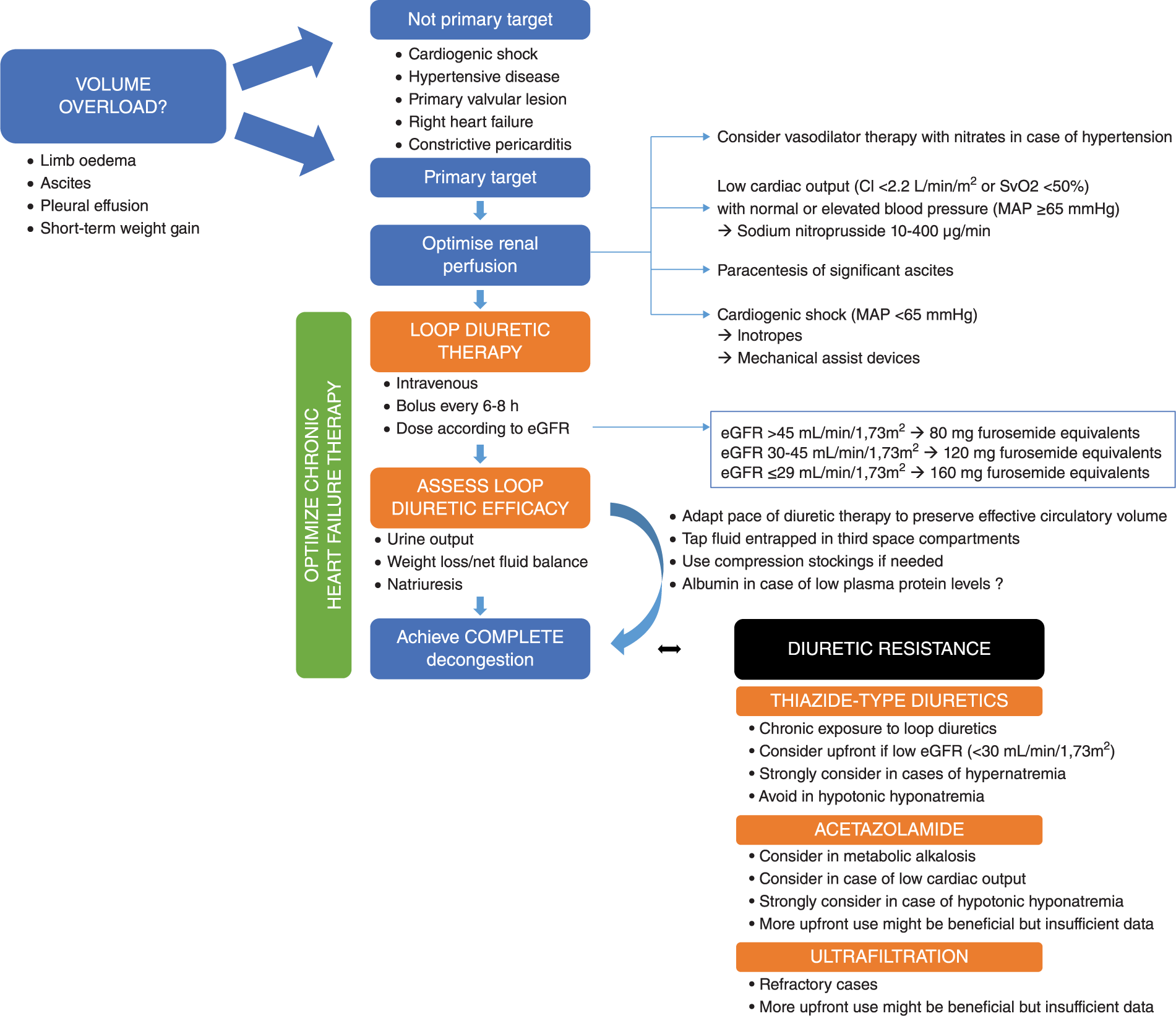
Integrated management approach to treat volume overload and loop diuretic resistance in acute heart failure.
Is volume overload the target culprit?
When considering (loop) diuretic therapy in AHF, one should never forget the primary aim of this therapy, which is creating a net negative sodium balance to reduce extracellular volume and hence relief signs and symptoms of congestion. Yet, in some presentations of AHF, volume overload may not be the target culprit. For example, cardiogenic shock due to an acute coronary syndrome or fulminant myocarditis may even require carefully administered fluids with the purpose of haemodynamic stabilisation, despite the presence of significant pulmonary oedema. Furthermore, flash pulmonary oedema due to a hypertensive crisis or severe mitral valve regurgitation is caused by volume misdistribution rather than volume overload per se and might be addressed better with vasodilator therapy or valve intervention, respectively. 46 In other phenotypes such as primary right heart failure or constrictive pericarditis, some degree of volume overload may be necessary to maintain adequate preload and is not the primary target of therapy. Main indicators of volume overload are limb oedema, ascites, pleural effusion, or significant weight gain over a short-term period. In contrast, jugular venous distension, orthopnoea, bendopnoea and pulmonary oedema are less specific as they reflect increased cardiac filling pressures, but not necessarily volume overload.
Are the kidneys adequately perfused?
If volume overload is present and deemed to be the target culprit in AHF, there is a clear indication for diuretic therapy. However, for diuretic therapy to be successful, renal perfusion must be adequate. Renal blood flow depends on mean arterial pressure, central venous pressure and intrarenal vascular resistance. Arterial hypotension during decongestive therapy is strongly associated with worsening renal function and should be avoided when possible. 47 Furthermore, lowering central venous pressure through administration of vasodilator therapy may lower the need for diuretics in AHF. 48 Specifically in the case of low cardiac output with normal or elevated arterial blood pressure (i.e. high systemic vascular resistance), intravenous sodium nitroprusside improves organ perfusion and hence renal blood flow. 49 Significant ascites in the setting of AHF is usually associated with increased intra-abdominal pressure, which impairs renal perfusion and may be alleviated by paracentesis. 39 Finally, when arterial blood pressure is low due to cardiogenic shock, inotropes and/or mechanical assist devices should be considered.
Consider loop diuretic pharmacokinetics
When a patient is admitted to the hospital with marked volume overload, intravenous administration of loop diuretics may be preferred over oral intake to overcome concerns about gastrointestinal reabsorption and oral bioavailability. There is no difference between bolus versus continuous administration with respect to successful decongestion, but the latter is associated with more pronounced neurohumoral activation.9,50,51 The benefit of the continuous administration of loop diuretics is that post-diuretic sodium retention does not occur, yet this can also easily be overcome by repeating loop diuretic bolus administration at 6-8 hour intervals if the patient is still volume overloaded. In addition, it is easy to adjust the pace of decongestion with bolus therapy when the plasma refill rate is impaired. Finally, it is crucially important to adjust the dose of loop diuretics according to the GFR and plasma protein levels (Figure 2).
Assess loop diuretic efficacy to recognise loop diuretic resistance early
When administering loop diuretics, it is important to assess the response to therapy and recognise diuretic resistance early to intervene. In most patients, urine output and weight loss suffice to evaluate loop diuretic efficacy. However, in patients with or at high risk of cardiorenal syndrome, following natriuresis may offer a better perspective on decongestion success. 15 The goal of diuretic treatment should be to continue until clinical signs and symptoms of volume overload have completely disappeared and cardiac filling pressures have normalised.
Continuously assess the effective circulatory volume
When clinical signs and symptoms of volume overload persist despite rapidly decreasing loop diuretic efficacy, one should consider that the effective circulatory volume is decreased. This might be further supported by deteriorating GFR or very low cardiac filling pressures. A simple treatment response might be just to slow down the pace of diuretic administration and allow more time for plasma refilling. Sometimes there might be fluid entrapment in third space compartments which can be tapped (e.g. ascites or pleural effusion). Alternatively, the plasma refill rate may be severely compromised because of low plasma oncotic pressure, vascular leak, or alterations in the interstitial matrix.40,41 Compression stockings should be considered in such cases. Intravenous albumin administration just before diuretic therapy is effective to recruit peripheral oedema, especially when plasma levels are low, but is expensive and has not been shown to improve outcomes in AHF.
Optimise chronic heart failure therapy in the case of reduced ejection fraction
Although pharmacological therapies in AHF have not been demonstrated to reduce all-cause mortality or heart failure readmissions in the long term, a hospital admission should always be considered as an opportunity to improve chronic heart failure therapy. 52 The neurohumoral system is both an important treatment target in heart failure with reduced ejection fraction and mechanistically implied in the occurrence of (loop) diuretic resistance. Indeed, it has been well established that renin-angiotensin-aldosterone system blockers decrease the need for diuretics in congestive heart failure, especially in the long term.53,54
Thiazide-type diuretics
Thiazide-type diuretics are the most frequently considered therapy in the case of loop diuretic resistance in AHF. They are effective mainly when the cause of diuretic resistance is distal tubular hypertrophy because of prolonged exposure to loop diuretics. 44 Alternatively, adding a thiazide-type diuretic up front is useful in the case of a low GFR to boost the fractional sodium excretion and ensure adequate natriuresis. 55 A drawback of thiazide-type diuretics is that they limit free water excretion or the urinary dilution capacity of the kidneys and therefore they should be avoided in hypotonic hyponatremia. 56 Most clinical evidence to support the use of thiazide-type together with loop diuretics in AHF comes from small observational studies. Those indicate a probable class effect and a 75-90% response rate in patients with loop diuretic resistence. 57 In addition, some intriguing data from the stepwise pharmacological care arm in the Cardiorenal Rescue Study in Acute Decompensated Heart Failure (CARRESS-HF) suggest that the combination of a diuretic efficacy-guided approach with step-up of thiazide-based therapy provides effective diuresis without compromising GFR, even when directly compared to an aggressive ultrafiltration approach. 58
Acetazolamide
Acetazolamide is an old and largely forgotten diuretic, which is still in use for the treatment of mountain disease and obstructive sleep apnoea syndrome. As a carbonic anhydrase inhibitor, it blocks sodium bicarbonate reabsorption in the proximal tubules. 12 Consequently, it improves sodium delivery to the NKCC2 hence boosting loop diuretic efficacy. One observational study in patients with AHF and marked volume overload found that the addition of acetazolamide improved loop diuretic efficacy with approximately 100 mmol sodium excreted per 40 mg of furosemide-equivalent dose. 24 Furthermore, acetazolamide also improves thiazide-type diuretic efficacy, as it potently downregulates pendrin expression in the distal nephron. 59 Pendrin, also known as the sodium-independent chloride/iodide transporter, compensates for sodium and chloride loss in the distal convoluted tubules and might be an unrecognised source of diuretic resistance.45,60 While the diuretic and natriuretic capacity of acetazolamide is poor on its own, it might well be a very efficient booster of diuretic efficacy in combination diuretic therapy.59,61 This concept is further supported by one small randomised trial including 24 patients with volume overload refractory to loop diuretic therapy. 62 All these patients demonstrated a greatly reduced fractional sodium excretion, which was easily overcome by the addition of acetazolamide. At the moment, there are insufficient data to recommend add-on or even up-front therapy with acetazolamide in addition to loop diuretics. Intriguingly, however, sodium-glucose transporter 2 inhibitors that also block sodium transport in the proximal renal tubules greatly increase loop diuretic efficacy and are among the most promising drugs under investigation in chronic heart failure. 63
Ultrafiltration
As loop diuretic therapy results in the production of hypotonic urine, while ultrafiltration removes isotonic plasma and hence more sodium for the same amount of water, it has been hypothesised that the latter might be a superior decongestion strategy. 64 Indeed, in the Ultrafiltration versus Intravenous Diuretics for Patients Hospitalized for Acute Decompensated Heart Failure (UNLOAD) study, which included 200 patients with AHF and clear signs of volume overload, ultrafiltration outperformed loop diuretics, producing greater weight and fluid loss. 65 Moreover, the 90-day readmission rate was also significantly lower in the ultrafiltration compared to loop diuretic group, presumably due to more effective decongestion. 65 These findings are somewhat in contradiction to the results of the much larger CARRESS-HF study(n=2033), which found no better decongestion – and hence no better clinical outcome – with ultrafiltration compared to pharmacological care with strong emphasis on combinational treatment. 4 Moreover, catheter-related adverse events and bleeding complications were more frequent in the ultrafiltration group. In addition, GFR improved significantly more with pharmacological care after 60 days. 4 In light of these results, we would recommend optimising pharmacological therapy first, with ultrafiltration reserved as bail-out in cases of refractory congestion. Nevertheless, it should be noted that such patients generally have a very poor prognosis. 66 One important point of criticism to CARRESS-HF might be, however, that the pharmacological care arm allowed decongestive treatment to be titrated very carefully on an individual base, according to diuretic efficacy. In contrast, the ultrafiltration rate was pre-set at a constant rate of 200 mL per hour, which was only changed for technical reasons or clinical requirements, as assessed by the treating physician. This has potentially put patients in the ultrafiltration arm at greater risk of intravascular volume depletion and hypotensive episodes, which might have been associated with more harmful neurohumoral activation. The Aquapheresis Versus Intravenous Diuretics and Hospitalization for Heart Failure (AVOID–HF) trial could have filled this important gap in the evidence. 67 Regrettably, the sponsor of this trial unilaterally decided to terminate the study after only 27% of the intended study population was recruited, despite the absence of any futility or safety concerns, rendering the trial severely underpowered. For this reason, results should be interpreted very cautiously, but the estimated days to a first heart failure event were in favour of the adjustable ultrafiltration group versus the adjustable loop diuretics group (62 versus 34 days; P value 0.106). Therefore, individually titrated ultrafiltration therapy may still have a role to play in the treatment of cardiorenal syndrome, yet more evidence is needed.
Conclusions
Loop diuretic resistance is a frequently encountered problem in AHF and portends poor prognosis. It is therefore important for the clinician to assess loop diuretic efficacy in AHF patients, when providing decongestive treatment. Different metrics for loop diuretic resistance have all been consistently associated with adverse clinical outcomes. Yet it remains an open question whether therapies that boost diuretic efficacy or prevent diuretic resistance improve prognosis in AHF. The mechanisms of loop diuretic resistance in AHF are multifactorial and require an integrated approach.
Footnotes
Conflict of interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.