
Abstract
Background:
The optimal anti-coagulation strategy for patients with non-ST-elevation myocardial infarction treated with percutaneous coronary intervention is unclear in contemporary clinical practice of radial access and potent P2Y12-inhibitors. The aim of this study was to investigate whether bivalirudin was superior to heparin monotherapy in patients with non-ST-elevation myocardial infarction without routine glycoprotein IIb/IIIa inhibitor use.
Methods:
In a large pre-specified subgroup of the multicentre, prospective, randomised, registry-based, open-label clinical VALIDATE-SWEDEHEART trial we randomised patients with non-ST-elevation myocardial infarction undergoing percutaneous coronary intervention, treated with ticagrelor or prasugrel, to bivalirudin or heparin monotherapy with no planned use of glycoprotein IIb/IIIa inhibitors during percutaneous coronary intervention. The primary endpoint was the rate of a composite of all-cause death, myocardial infarction or major bleeding within 180 days.
Results:
A total of 3001 patients with non-ST-elevation myocardial infarction, were enrolled. The primary endpoint occurred in 12.1% (182 of 1503) and 12.5% (187 of 1498) of patients in the bivalirudin and heparin groups, respectively (hazard ratio of bivalirudin compared to heparin treatment 0.96, 95% confidence interval 0.78–1.18, p=0.69). The results were consistent in all major subgroups. All-cause death occurred in 2.0% versus 1.7% (hazard ratio 1.15, 0.68–1.94, p=0.61), myocardial infarction in 2.3% versus 2.5% (hazard ratio 0.91, 0.58–1.45, p=0.70), major bleeding in 8.9% versus 9.1% (hazard ratio 0.97, 0.77–1.24, p=0.82) and definite stent thrombosis in 0.3% versus 0.2% (hazard ratio 1.33, 0.30–5.93, p=0.82).
Conclusion:
Bivalirudin as compared to heparin during percutaneous coronary intervention for non-ST-elevation myocardial infarction did not reduce the composite of all-cause death, myocardial infarction or major bleeding in non-ST-elevation myocardial infarction patients receiving current recommended treatments with modern P2Y12-inhibitors and predominantly radial access.
Introduction
Anti-coagulation therapy with heparin, fondaparinux, low molecular weight heparin (LMWH) or bivalirudin is typically used in conjunction with anti-platelet agents such as aspirin, P2Y12-inhibitors, or glycoprotein IIb/IIIa inhibitors (GPIs), in order to improve angiographic and clinical outcomes after percutaneous coronary intervention (PCI) for acute coronary syndromes (ACSs).1–6 The use of more potent P2Y12-inhibitors has further improved clinical outcomes in patients treated with PCI for ACS.7,8 Balancing the risk of thrombotic complications such as re-infarction and stent thrombosis against bleeding complications is important for long-term survival. In several trials bivalirudin has demonstrated lowered risk of bleeding compared to heparin with provisional GPIs in patients with ACS.1,6,9 However, these trials were performed prior to the routine use of radial access, potent P2Y12-inhibitors, or without assessing heparin monotherapy (without GPIs) as an alternative to bivalirudin during PCI in patients with ACS.
Non-ST-segment elevation myocardial infarction (NSTEMI) has poor long-term prognosis, is more common than ST-elevation myocardial infarction (STEMI), the patients are older, more frail and with more concomitant disease. No dedicated major trial comparing bivalirudin and heparin monotherapy, without planned GPIs, has included a large number of patients with NSTEMI undergoing PCI. In patients without elevated cardiac biomarkers, bivalirudin compared to heparin monotherapy in a relatively high dose (140 U/kg) was documented with a reduction in bleeding events, but no difference in major adverse cardiovascular events (MACEs) 10 Several studies have compared bivalirudin to heparin combined with GPIs in patients without STEMI undergoing PCI.2,6,9 In general, these studies demonstrated reduced bleeding complications with bivalirudin but no reduction in MACEs. In one of the largest bivalirudin trials on ACS, almost half of the patients had NSTEMI.11,12 This large subgroup had a similar reduction in bleeding events with bivalirudin as the total study population, but with no reduction in mortality or MACEs. However, more than one-quarter of the patients in the heparin group also received GPIs, which may have led to increased bleeding complications. In the recent ‘Bivalirudin versus heparin in NSTEMI and STEMI patients on modern antiplatelet therapy in the Swedish web-system for enhancement and development of evidence-based care in heart disease evaluated according to recommended therapies registry’ trial (VALIDATE-SWEDEHEART trial), in patients with STEMI or NSTEMI treated with potent P2Y12 inhibitors, we found no difference in MACEs or bleeding complications between bivalirudin and heparin monotherapy. 13
The aim of this pre-planned substudy was to investigate whether bivalirudin compared to heparin monotherapy without routine GPI use during PCI reduces the composite of all-cause death, myocardial infarction and major bleeding events in patients with NSTEMI in the VALIDATE-SWEDEHEART trial, treated with potent P2Y12-inhibitors and predominantly undergoing radial artery PCI.
Methods
Study design
The VALIDATE-SWEDEHEART trial was a multicentre, prospective, randomised, controlled, clinical open-label trial. This registry-based randomised clinical trial (RRCT) utilised the platform of pre-existing high-quality health-care registries as case-report forms, for randomization, and for follow-up. 14
The trial was coordinated by Uppsala Clinical Research Centre (Uppsala, Sweden), where we managed the database and performed statistical analyses. An executive committee, with assistance from all investigators, was responsible for the design, conduct and reporting of the study. The funding agencies had no access to the study data and no role in design, implementation, or reporting. The trial was conducted in accordance with the Declaration of Helsinki and was approved by the ethical review board of Lund University, Sweden (2012/796) and by the Swedish Medical Products Agency (2012/120382). The trial is registered as www.clinicaltrialsregistry.eu: 2012-005260-10 and clinicaltrials.gov: NCT02311231. The authors vouch for the accuracy and completeness of the data and of all analyses, and for the fidelity of this report to the trial protocol. 13
Patients
Patients admitted to a participating hospital with a diagnosis of NSTEMI and planned for in-hospital PCI were eligible for inclusion according to previously defined inclusion and exclusion criteria. 14 Treatment with an oral loading dose of ticagrelor or prasugrel before PCI was mandatory. Pre-planned GPI use or GPI use before catheterization were contraindicated, however bail-out use of GPIs was allowed and recorded.
Study procedures
Patients with NSTEMI received guideline-recommended treatment with unfractionated heparin, LMWH or fondaparinux as per local practice while waiting for PCI. In the catheterization laboratory before angiography, an intra-arterial bolus of up to 3000 U heparin was allowed in order to prevent radial artery thrombosis. 15
After angiography, but prior to PCI, patients were randomised online through the Swedish angiography and angioplasty registry (SCAAR) to receive intravenous administration of bivalirudin (Angiox, The Medicines Company, USA) or intra-arterial administration of unfractionated heparin (Leo Pharma, Sweden) in an open-label fashion. Randomization followed a computer-generated list with 1:1 permuted block randomization stratified for STEMI/NSTEMI and hospital.
Bivalirudin was administered as an intravenous bolus of 0.75 mg/kg followed by an infusion of 1.75 mg/kg×h. Treatment was started as soon as PCI of the culprit lesion was intended. It was strongly recommended to continue bivalirudin infusion after PCI until the last opened vial had been administered. In patients randomised to receive heparin, a total dose of 70–100 U/kg was recommended.
Activated clotting time (ACT) measurement 10 min after initiation of heparin or bivalirudin treatment was strongly recommended. A bolus dose of the respective randomised treatment was recommended if ACT was <250 s (0.3 mg/kg bivalirudin or heparin dose at the physician’s discretion). P2Y12-inhibitor treatment was recommended for one year post-PCI in addition to aspirin 75–160 mg daily. 16 Written consent was obtained before angiography.
Endpoints and definitions
On endpoints and definitions see the main study publication. 13 The 180 day endpoint was chosen to demonstrate a possible separation of mortality events beyond 30 days.
Statistics
We hypothesised that bivalirudin would be superior to heparin in reducing the composite of all-cause death, MI or major bleeding events at 180 days. We anticipated a primary endpoint rate of 15.8% at 180 days in the heparin group for patients with NSTEMI. The trial was powered to detect a hazard ratio (HR) of 0.75 with 80% power in the NSTEMI group leading to planned recruitment of 3000 patients including compensation for deviations from treatment and attrition. Time-to-event endpoints are presented using Kaplan-Meier plots and treatment differences were assessed using the log-rank test and Cox regression. Time in hospital was compared using the Mann Whitney U-test and the Hodges-Lehmann estimator. Loss to follow-up was treated as censoring in event time analyses. A two-tailed p-value <0.05 was considered statistically significant.
The primary pre-planned subgroup analysis examined the primary endpoint and its components in the NSTEMI population. Subgroup analyses for the primary end point were pre-specified in the statistical analysis plan and in the previously published study design article. 14 Subgroup analyses were performed using a proportional hazards model with factors treatment, subgroup, and treatment-subgroup interaction.
Following inclusion of the first 1500 patients and again after 3000 patients in the entire VALIDATE-SWEDEHEART cohort, a data safety monitoring committee (DSMC) evaluated the trial progress as well as unblinded events for risk for trial subjects and recommended continuation of the study.
Results
Study population
Twenty-five out of Sweden’s 29 PCI centres participated in the trial. The trial enrolled 6006 patients, 3005 patients with STEMI and 3001 patients with NSTEMI, undergoing PCI between June 2014–September 2016. 13
All randomised NSTEMI patients, 1503 allocated to bivalirudin and 1498 allocated to heparin treatment, were followed according to the intention-to-treat principle. Baseline characteristics were well balanced between treatment groups (Table 1). Follow-up was complete in 99% of patients. Follow-up of mortality was 100%. 13
Baseline characteristics of treatment groups.
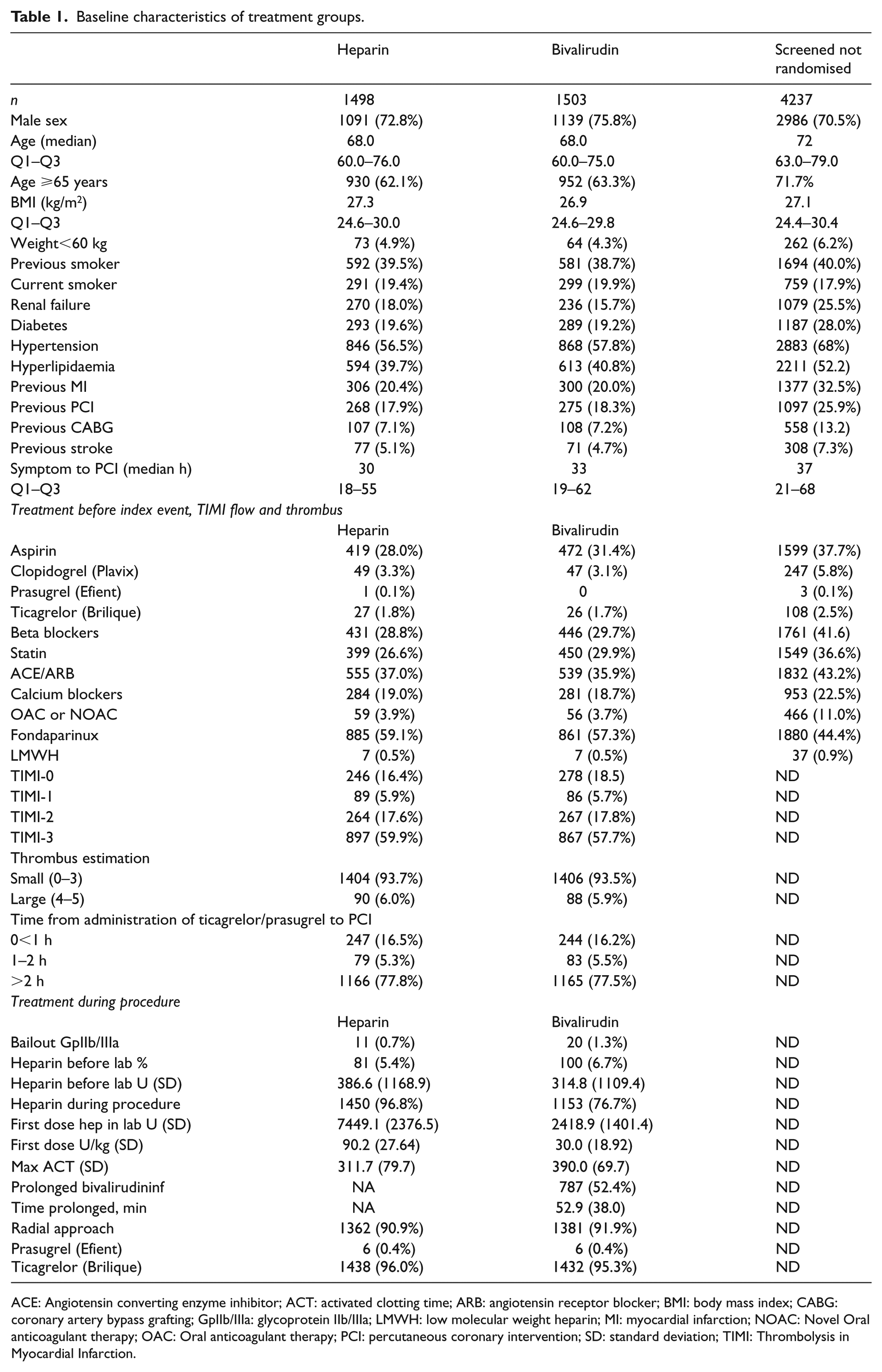
ACE: Angiotensin converting enzyme inhibitor; ACT: activated clotting time; ARB: angiotensin receptor blocker; BMI: body mass index; CABG: coronary artery bypass grafting; GpIIb/IIIa: glycoprotein IIb/IIIa; LMWH: low molecular weight heparin; MI: myocardial infarction; NOAC: Novel Oral anticoagulant therapy; OAC: Oral anticoagulant therapy; PCI: percutaneous coronary intervention; SD: standard deviation; TIMI: Thrombolysis in Myocardial Infarction.
Among all patients, 7.8% received heparin (maximum 5000 U) in the bivalirudin arm before arriving in the catheterization laboratory versus 10.3% in the heparin arm. In the catheterization laboratory, 72.4% in the bivalirudin arm versus 99.7% in the heparin arm received heparin with a mean first heparin dose of 30.0 U/kg and 90.2 U/kg, respectively. The mean maximum ACT during PCI was 390 s and 311 s for the bivalirudin and heparin groups. In the bivalirudin group, 52.4% received prolonged study drug infusion for a mean of 53 min and none received an extra bolus because of low ACT. GPI-bailout was used in 1.3% and 0.7% in patients treated with bivalirudin and heparin, respectively (Table 1). The radial approach was used in 90.7% in the bivalirudin group and 89.7% in the heparin group.
Clinical outcomes
The primary endpoint at 180 days occurred in 12.1% (182 of 1502) and 12.5% (187 of 1498) of patients in the bivalirudin and heparin groups, respectively (HR of bivalirudin compared to heparin treatment 0.96, 95% confidence interval (CI) 0.78–1.18, p=0.69, Figure 1, Table 2). All cause death occurred in 2.0% versus 1.7% (HR 1.15, 0.68–1.94, p=0.61). Myocardial infarction occurred in 2.3% versus 2.5% (HR 0.91, 0.58–1.45, p=0.70). Major bleeding occurred in 8.9% versus 9.1% (HR 0.97, 0.77–1.24, p=0.82), definite stent thrombosis in 0.3% versus 0.2% (HR 1.33, 0.30–5.93, p=0.82). Stroke did not differ between groups (Table 2).
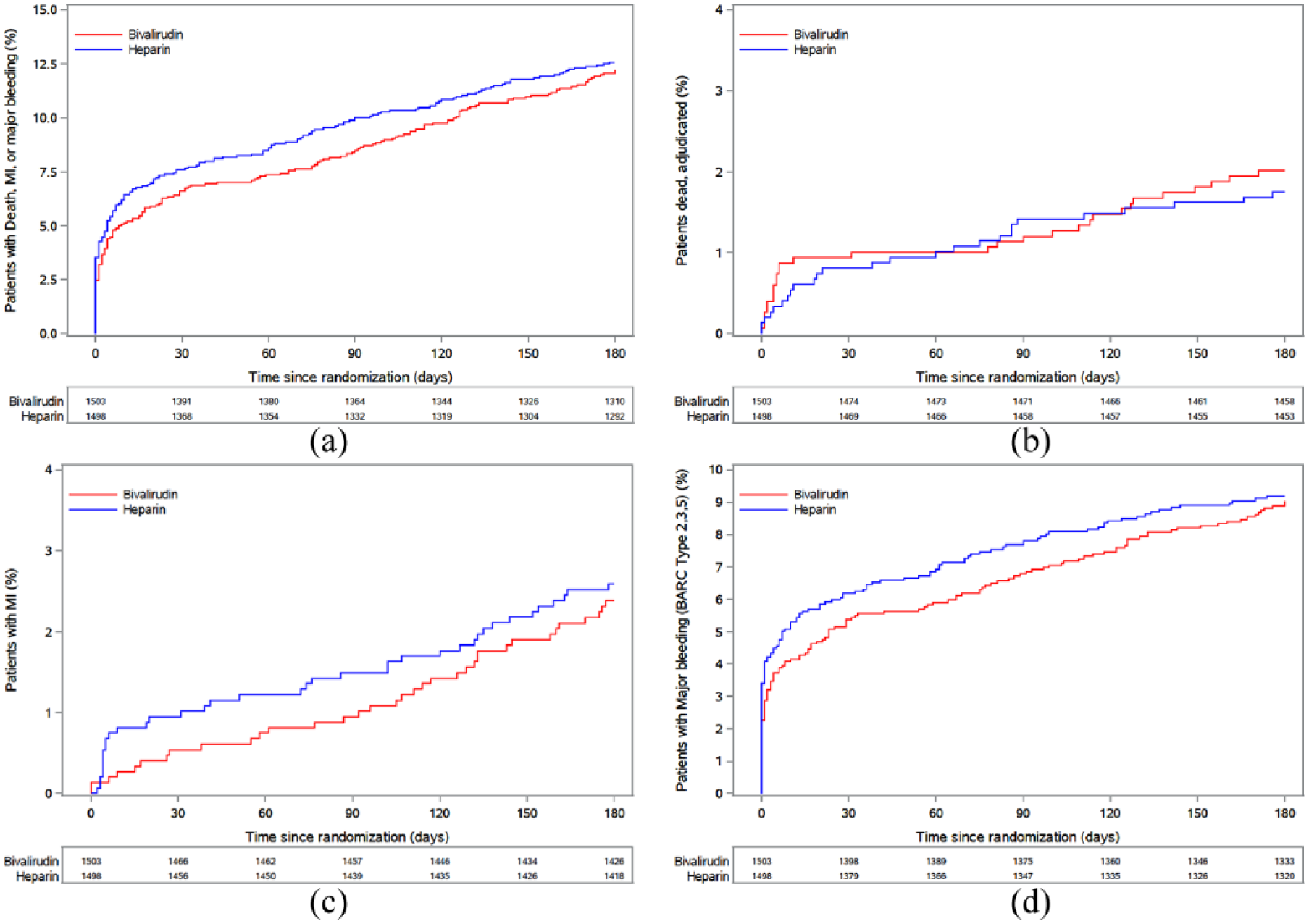
(a) Kaplan-Meier curves showing cumulative probability of primary endpoint (death, myocardial infarction (MI) or major bleeding) during 180 days follow-up in non-ST-elevation myocardial infarction (NSTEMI) patients. (b) Kaplan-Meier curves showing cumulative probability of death during 180 days follow-up. (c) Kaplan-Meier curves showing cumulative probability of MI during 180 days follow-up. (d) Kaplan-Meier curves showing cumulative probability of major bleeding during 180 days follow-up.
Outcomes at 180 days in patients assigned to bivalirudin as compared with heparin.

BARC: Bleeding Academy Research Consortium; CV: cardiovascular; HR: hazard ratio; LAD: Left anterior descending artery; Lcx: Left Circumflex artery; MI: myocardial infarction; PCI: percutaneous coronary intervention; RCA: Right Coronary Artery; ST: stent thrombosis.
Including definitive ST.
Including definitive ST and probable ST.
The results in patients with NSTEMI were consistent across all pre-specified subgroups, including risk groups such as old age, chronic renal failure, diabetes mellitus and smokers (Figure 2).
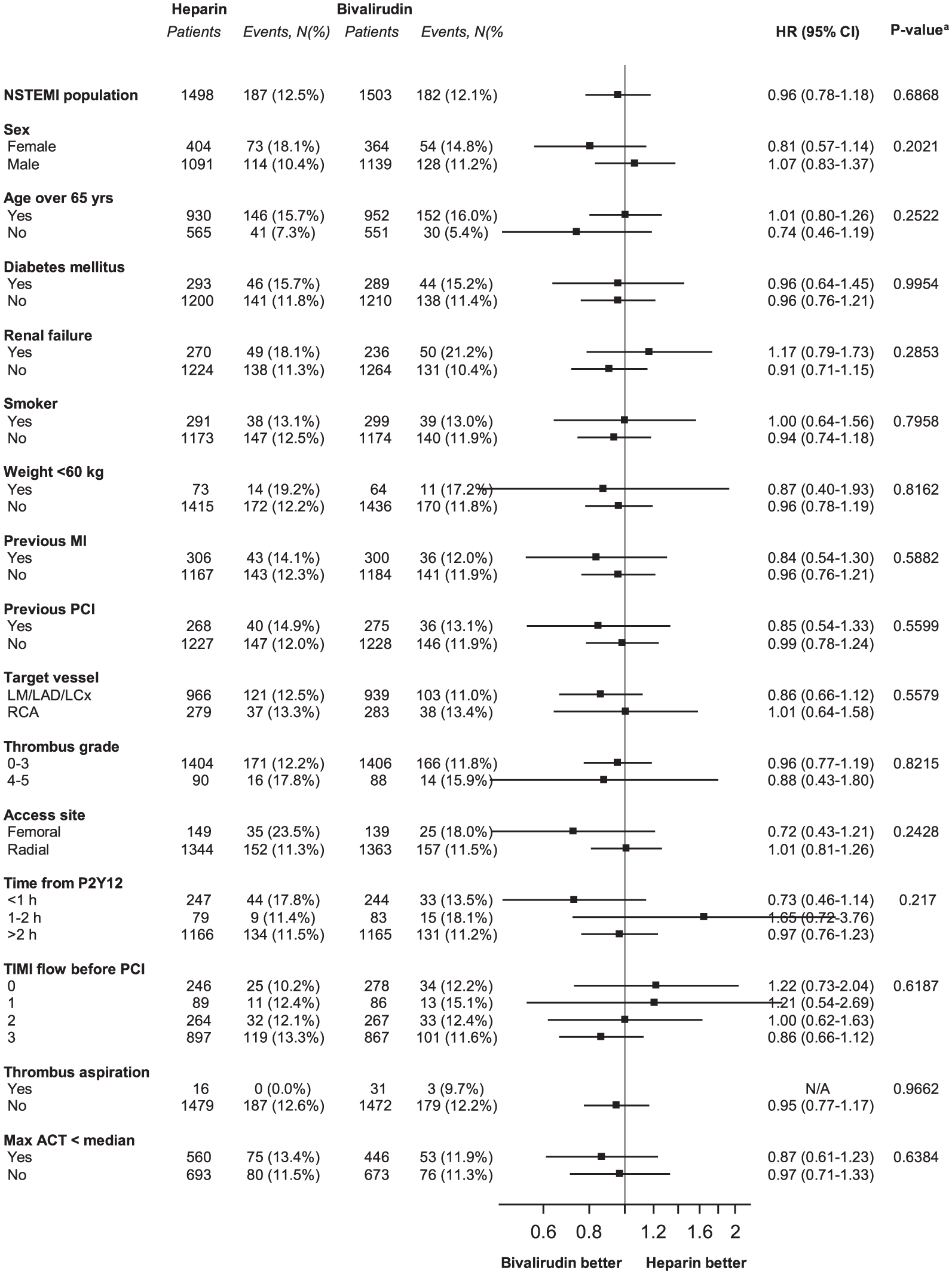
Forest plot of risk ratios for the primary endpoint (death, myocardial infarction (MI) or major bleeding) during 180 days follow-up according to pre-specified subgroups in non-ST-elevation myocardial infarction (NSTEMI) patients. Hazard ratios (HRs; black diamonds) and 95% confidence intervals (CIs; horizontal lines) are shown. ACT: activated clotting time; MI: myocardial infarction; PCI: percutaneous coronary intervention; TA: thrombus aspiration; TIMI: Thrombolysis in Myocardial Infarction.
There were no significant differences in any outcomes between the groups at 30 days post-PCI (Table 3).
Outcomes at 30 days in patients assigned to bivalirudin as compared with heparin.
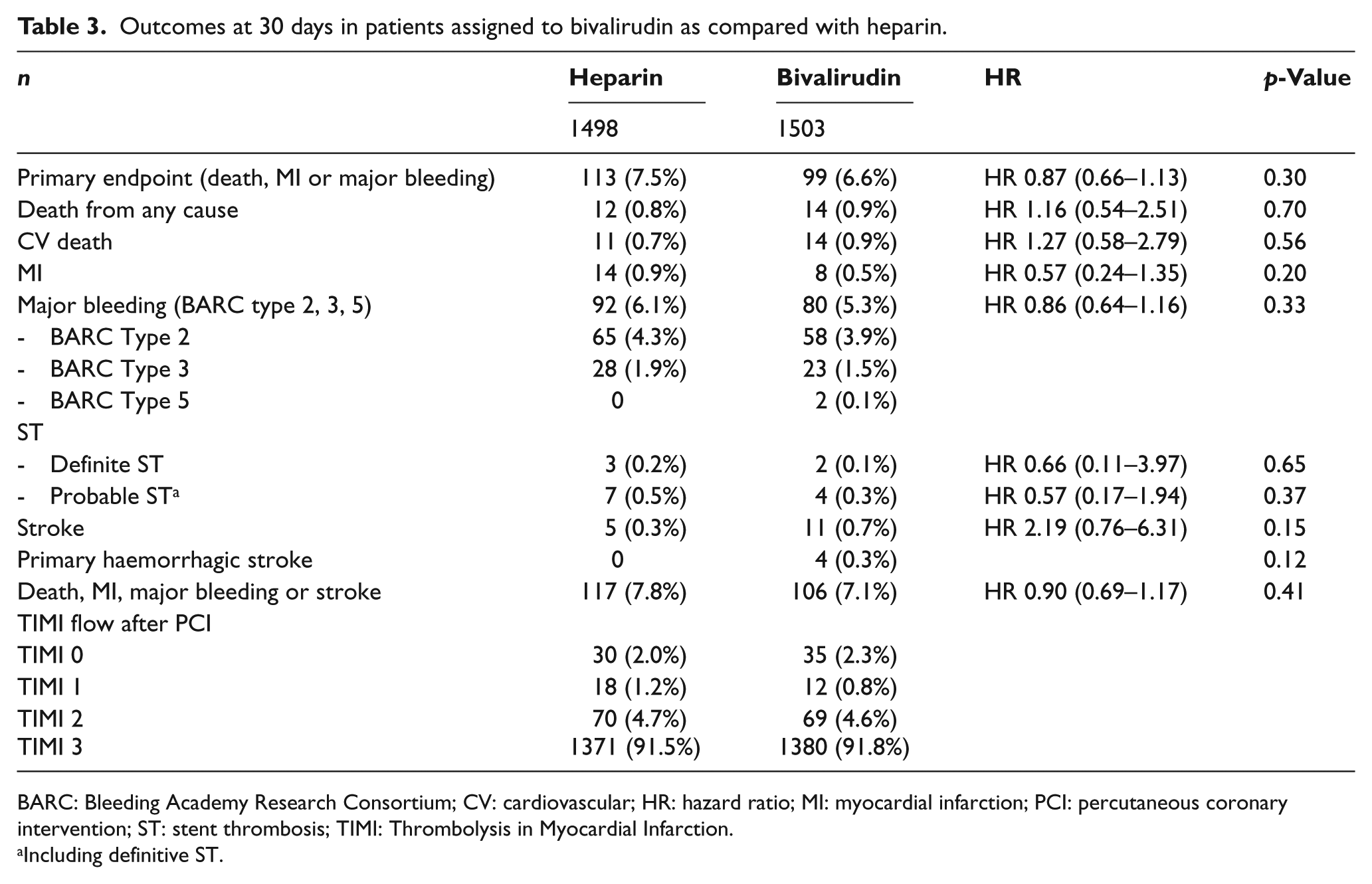
BARC: Bleeding Academy Research Consortium; CV: cardiovascular; HR: hazard ratio; MI: myocardial infarction; PCI: percutaneous coronary intervention; ST: stent thrombosis; TIMI: Thrombolysis in Myocardial Infarction.
Including definitive ST.
Patients with NSTEMI treated with PCI at the enrolling hospital during the study period that were screened but not randomised were older, were more likely to have diabetes mellitus, previous MI, previous coronary artery bypass grafting, previous stroke and more baseline medications (p<0.1 for all parameters in Table 1 except body mass index (BMI) and current smoker, when comparing screened not randomised patients with all randomised patients). Mortality after 180 days was lower in randomised patients (84/3001; 2.8%) compared to not randomised patients (210/4237; 5.0%).
Discussion
In this investigator-initiated RRCT substudy from the VALIDATE-SWEDEHEART trial, of the large subgroup of patients with NSTEMI treated with acute PCI, aspirin and potent P2Y12-inhibitors, anticoagulation with bivalirudin was not superior to heparin regarding the composite endpoint of all-cause death, MI or major bleeding at 180 days. There were no significant differences in any of the pre-specified secondary endpoints including the individual components of the primary outcome or stent thrombosis. The results were consistent in patients in all major patient subgroups, regardless of baseline clinical or angiographic characteristics.
The VALIDATE-SWEDEHEART trial was designed to investigate the clinical effect of a bivalirudin vs heparin monotherapy strategy without planned GPIs and optimising both treatment alternatives. To our knowledge this is the largest randomised trial comparing these strategies of anticoagulation without planned GPIs in patients with NSTEMI. In this trial, all patients were required to receive platelet inhibition with potent P2Y12 receptor inhibitors prior to randomization and PCI. Prolonged bivalirudin infusion was strongly recommended. A limited bolus of heparin (usually 3000 U), was given in the radial sheet at the start of PCI before randomization also in the bivalirudin group to avoid radial thrombosis. 15 The rationale for the early potent P2Y12-inhibitor strategy emanated from studies indicating faster onset of platelet inhibition 17 and lower risks of stent thrombosis and early re-infarction with early or intravenous administration of P2Y12-inhibitors.18–20 Finally, previous post-hoc analyses indicated that a prolonged infusion of high-dose bivalirudin might prevent early stent thrombosis.11,21 In our study, 77% of patients received treatment with a small bolus dose of heparin during the procedure before randomization in the bivalirudin group, 78% received potent P2Y12-inhibitors more than two hours before PCI, and 52% of patients received prolonged high-dose bivalirudin for an average of 53 min, factors that might have contributed to the overall low event rates and the lack of significant differences between the randomised anticoagulation strategies concerning ischaemic events. Similarly, 30 day and 180 days rates of stent thrombosis were also low (0.1 vs 0.2% and 0.3 vs 0.2% for bivalirudin vs heparin groups).
The main component of the primary composite outcome in the trial was bleeding, which constituted a dominant part of the composite outcome. Two-thirds of all bleedings were of moderate severity according to the Bleeding Academy Research Consortium (BARC) classification (BARC=2), and one-third were severe (BARC⩾3). Severe bleedings events thereby amounted to as many events in the trial as MIs and deaths combined. As only severe bleedings, defined as BARC⩾3, have the same consequences on mortality as MI, 22 the possibility of detecting any effect on mortality by the previously observed lower bleeding rate with bivalirudin was small. The low and similar mortality in both arms was therefore probably due to low rates of both MI and bleeding. Although both non-fatal events (MI and bleedings) were numerically lower in the bivalirudin arm of the trial at 30 days, the absolute risk reduction was low and did not achieve statistical significance. Furthermore, the trends were largely nullified at 180 days and all-cause mortality showed no trend whatsoever for any advantage of bivalirudin over heparin at either 30 or 180 days. These findings are in contrast with most previous trials showing a reduction in bleeding events with bivalirudin.6,9–11 The use of the recommended radial approach in 90% of patients and the low use of GPIs in the heparin arm may have contributed to the very low rate of severe bleeding complications in both arms despite an average age of 68 years which is among the highest of recent major ACS trials.1–6
The primary composite endpoint results were similar without any significant interactions within any predefined subgroup. In the main trial including patients with STEMI and NSTEMI, there was a trend towards a better effect of bivalirudin compared to heparin in females. 13 However, this was not seen in this study of patients with NSTEMI.
We utilised national quality registries as online platforms for randomization, as case-report forms for collection of baseline and procedural data, and for mortality follow-up. The registry-based approach was combined with event-tracking by telephone calls and adjudication of suspected events by a blinded independent clinical endpoint committee, resulting in a hybrid RRCT. 14 This design facilitated the identification and randomization of a large proportion of all eligible patients, which in turn reduced the number of sites necessary for enrolment and costs compared to a conventional randomised clinical trial. Furthermore, this design allowed follow-up of all eligible patients that were not enrolled in the study.23–25 The simplified registry-based randomization process and broad inclusion criteria resulted in a trial population that may better represent a real-world population than many conventional randomised trials. The RRCT design most likely also explains why we, in this trial, managed to include an older population, 68 years, 3–6 years older than previous bivalirudin trials. Still, the not-randomised population was even older, 72 years, with more concomitant disease.
Limitations of the VALIDATE NSTEMI trial should be noted. First, the treating physician was aware of the group to which each patient had been assigned, and that physician entered the angiographic variables into the registry; therefore, these variables were susceptible to bias. Second, a comparison of the clinical characteristics and outcomes between the patients who underwent randomization and those who did not indicates that the two cohorts differed significantly in a number of respects, such as age, comorbidities and, most notably, in mortality. In many cases, these differences reflect the exclusion from the trial of patients who were ineligible because they were unable to provide oral consent. Even when a trial uses a population-based registry for enrolment, the trial participants cannot be fully representative of the complete range of patients.
In conclusion, in the VALIDATE-SWEDEHEART RRCT trial comparing bivalirudin with heparin in the large subgroup of patients presenting with NSTEMI and treated with PCI using a radial approach and high-intensity platelet inhibition, there were no significant differences between bivalirudin and heparin treatment with respect to mortality, re-infarction or major bleeding events during 180 days of follow-up.
Footnotes
Acknowledgements
The authors wish to thank the patients and the staff at all centres participating in the VALIDATE-SWEDEHEART collaboration for their commitment to this study. They thank Ylva Lindman, Anna Stendahl, Frida Kåver and Solveig Wennerholm for excellent study management. The DSMC consisted of Gorm B Jensen, Lars Köber and Gunnar Gislason. Editorial assistance was provided by Vendela Roos, Uppsala Clinical Research Centre, Uppsala, Sweden.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
The study was supported by the Swedish Heart and Lung Foundation, by the Swedish Research Council, by unrestricted grants from AstraZeneca and the Medicines Company, and by the Swedish Foundation for Strategic Research (as part of the TOTAL-AMI project). The design and conduct of this study, all study analyses, and the final contents, drafting and editing of all emanating scientific publications are the sole responsibilities of the authors.