
Abstract
In patients admitted for acute myocardial infarction, the communication and transition from specialists to primary care physicians is often delayed, and the information imparted to subsequent healthcare providers (HCPs) may be sub-optimal. A French group of cardiologists, lipidologists and diabetologists decided to establish a consensus to optimize the discharge letter after hospitalization for acute myocardial infarction. The aim is to improve both the timeframe and the quality of the content transmitted to subsequent HCPs, including information regarding baseline assessment, procedures during hospitalization, residual risk, discharge treatments, therapeutic targets and follow-up recommendations in compliance with European Society of Cardiology guidelines. A consensus was obtained regarding a template discharge letter, to be released within two days after patient’s discharge, and containing the description of the patient’s history, risk factors, acute management, risk assessment, discharge treatments and follow-up pathway. Specifically for post acute MI patients, tailored details are necessary regarding the antithrombotic regimen, lipid-lowering and anti-diabetic treatments, including therapeutic targets. Lastly, the follow-up pathway needs to be precisely mentioned in the discharge letter. Additional information such as technical descriptions, imaging, and quality indicators may be provided separately. A template for a standardized discharge letter based on 8 major headings could be useful for implementation in routine practice and help to improve the quality and timing of information transmission between HCPs after acute MI.
Introduction
Poor communication and imperfect transfer of medical information between healthcare providers (HCPs) is a major issue when dealing with daily patient care. Difficulties in data transmission between hospitals and primary care physicians (PCPs) have been previously reported in terms of the timeliness, completeness and accuracy of the information1–3 and may adversely affect patients’ care.
Acute myocardial infarction (AMI) is a typical situation where patient information, healthcare knowledge, risk stratification, post discharge planning and improved communication between HCPs are essential, and might impact clinical outcomes. 4 Indeed, after AMI, patients enter into a chronic phase, but often remain at high residual risk of recurrent ischaemic events, even beyond the first year. 5 Therefore, information exchange among specialists and PCPs is of utmost importance, particularly between hospital cardiologists and PCPs at discharge. The discharge letter is therefore the cornerstone of communication and transition between specialists and PCPs, 6 but the timeliness with which the discharge letter is prepared and sent and the information it contains are often sub-optimal.
During hospitalization for AMI, in addition to revascularization, a range of specific treatments are implemented, including antiplatelet therapy (APT), lipid-lowering treatments (LLTs) and, in a subset of patients, antidiabetic or heart failure treatments. This makes the discharge letter crucial as compared with other medical situations, to ensure accurate transmission of information in the view of pursuing therapy appropriately and avoiding medication misadventures.
Against this background, a group of French clinicians came together to improve the quality of post-AMI communication and discuss the discharge document with the aim of reaching a consensus on a structured post-AMI discharge letter. This document, if implemented routinely, would help to improve timeliness and quality of the medical data communicated between HCPs in compliance with European Society of Cardiology (ESC) guidelines.7,8
Methods
Expert group
Based on a range of areas of expertise, and with a balanced geographical representation from across the country, four diabetologists and 28 cardiologists (of whom 22 are directly involved in the management of AMI in public or private hospitals) were invited to participate in the writing of this consensus discharge letter template. Although the group recognizes the importance of all information related to the patient’s characteristics, early management, risk stratification, secondary prevention treatments and structured follow-up, the goals of the consensus were specifically focused on determining the following:
The most convenient format and timeframe for sending the discharge letter.
The minimal content relating baseline characteristics, modalities of admission, acute management, risk assessment, discharge medications and strategies during follow-up, including structured care pathway and cardiac rehabilitation.
Specific part regarding antithrombotic, lipid-lowering and antidiabetic treatments at discharge.
Consensus
We used a three-step Delphi method to establish consensus. This method is an iterative process that uses systematic progression of repeated rounds to determine expert group consensus, when there is little or no definitive evidence and when opinion is important. The group also held discussions during live meetings and communicated at length by electronic means. During the meetings, various examples of discharge letters, corresponding to real-life examples from hospitalizations, were presented and critiqued. Additional presentations generated discussions about recent trials and guidelines for antithrombotic therapy (aspirin, P2Y12 inhibitors, oral anticoagulation when indicated), LLT (statins and ezetimibe) and antidiabetic agents (insulin, metformin, sulphonylureas, dipeptidyl peptidase 4 inhibitors, glucagon-like peptide-1 analogues and sodium glucose cotransporter SGLT1). Two questionnaires were prepared and circulated to obtain the opinion of all the members of the group, without the usual constraints related to physical presence at a meeting and bias induced by variations in speaking time. We considered that items with >70% agreement among the group should be mandatory in the discharge letter template; items with 50–70% agreement could be considered for inclusion; and items with <50% can be left at the physician’s discretion. To reach a consensus, we used the Delphi method; 9 after the second round, the document was fed back to participants for final agreement.
Results
The results of the second-round discussions are presented in Figures 1–5.
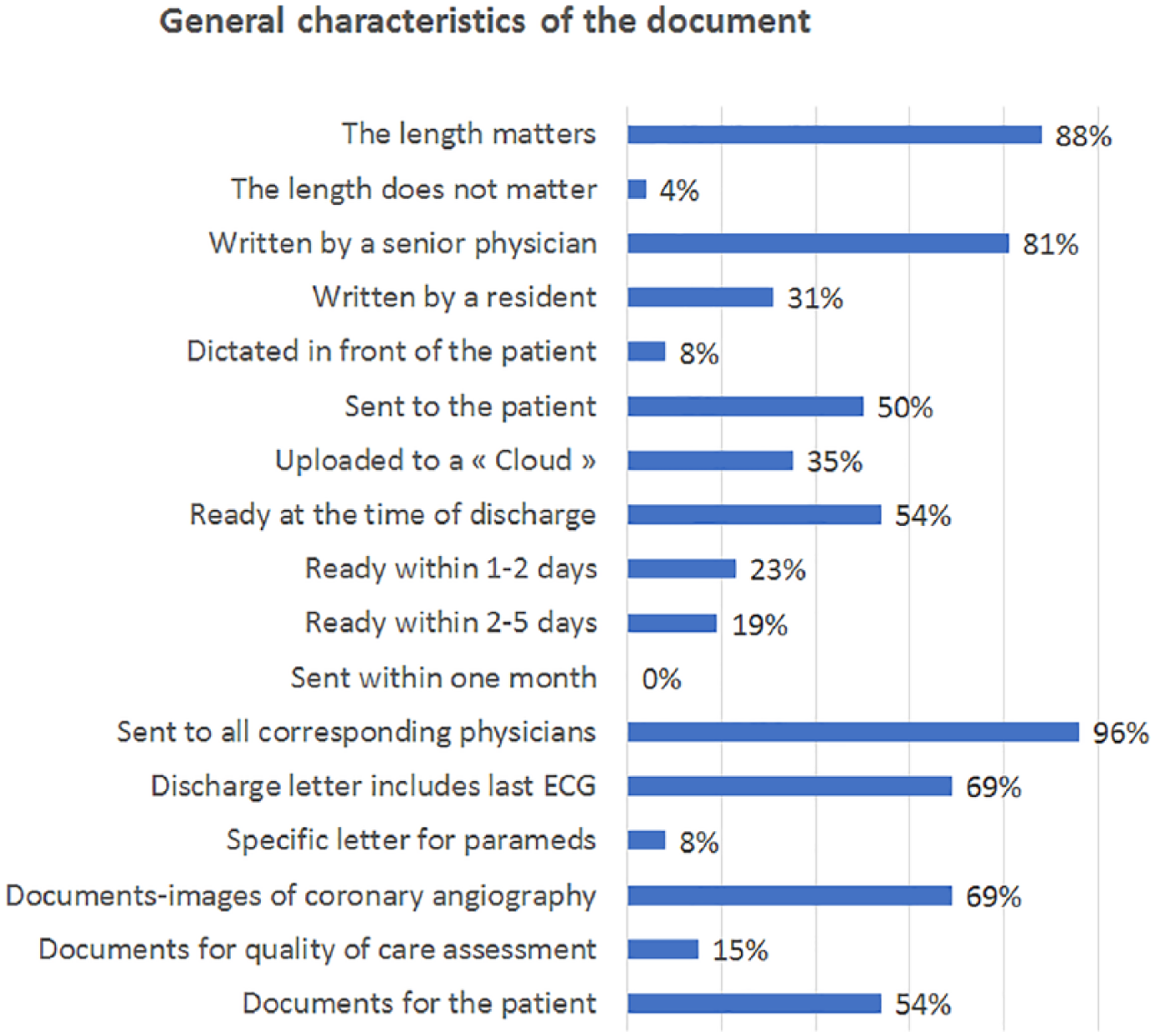
Results of the poll, format of the document.
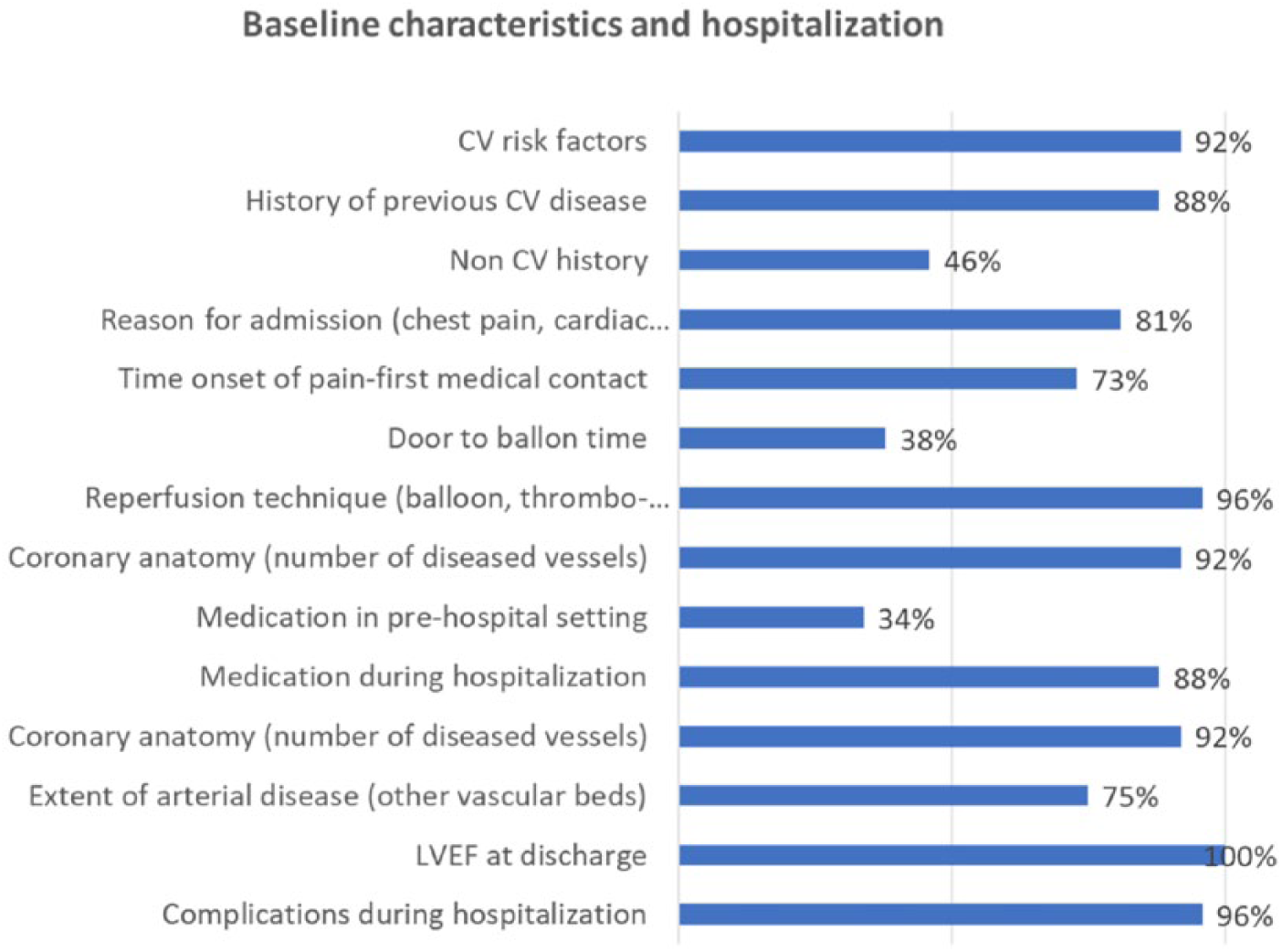
Results of the poll, baseline characteristics (demography, risk factors, history).
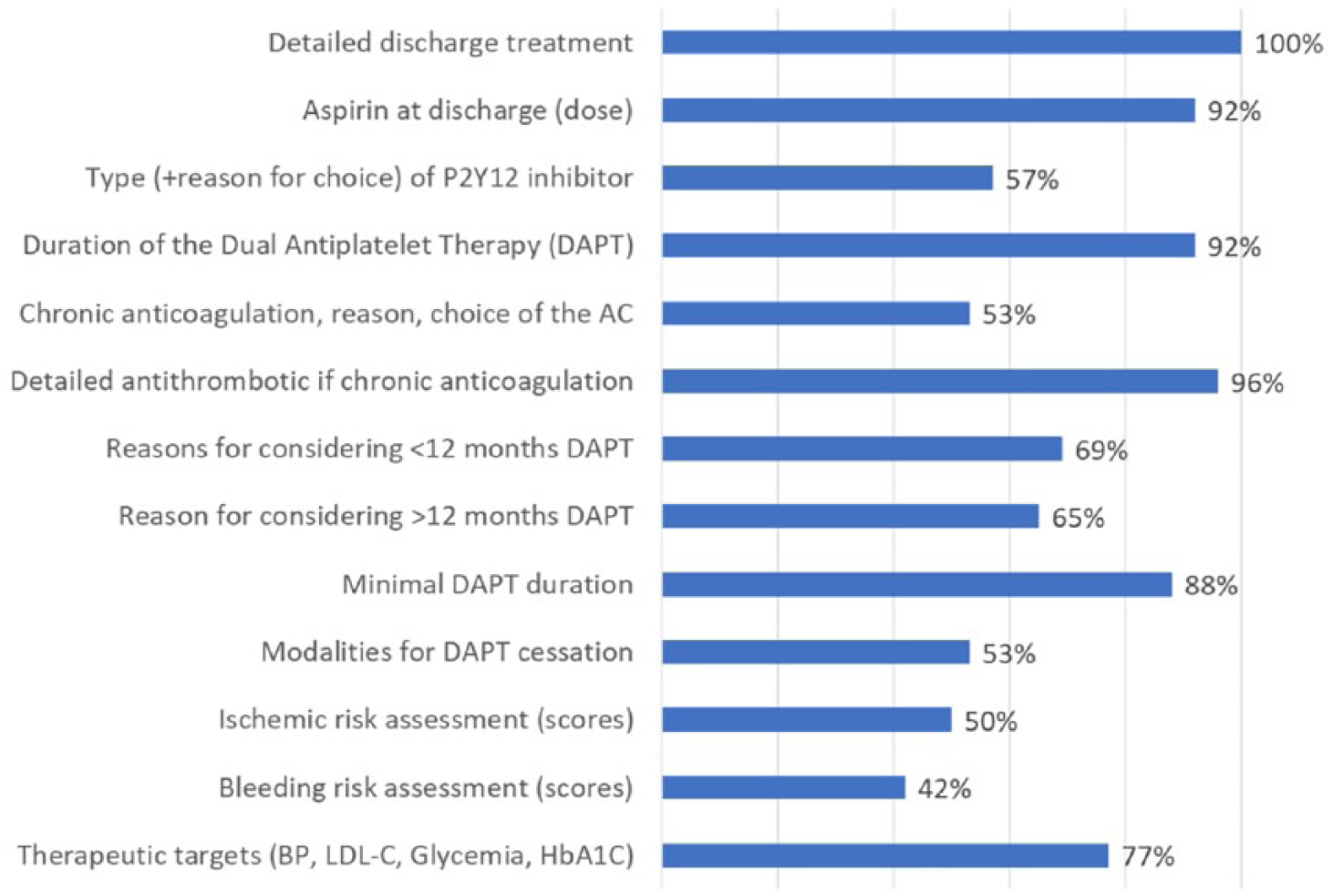
Results of the poll, anti-thrombotic treatment at discharge.
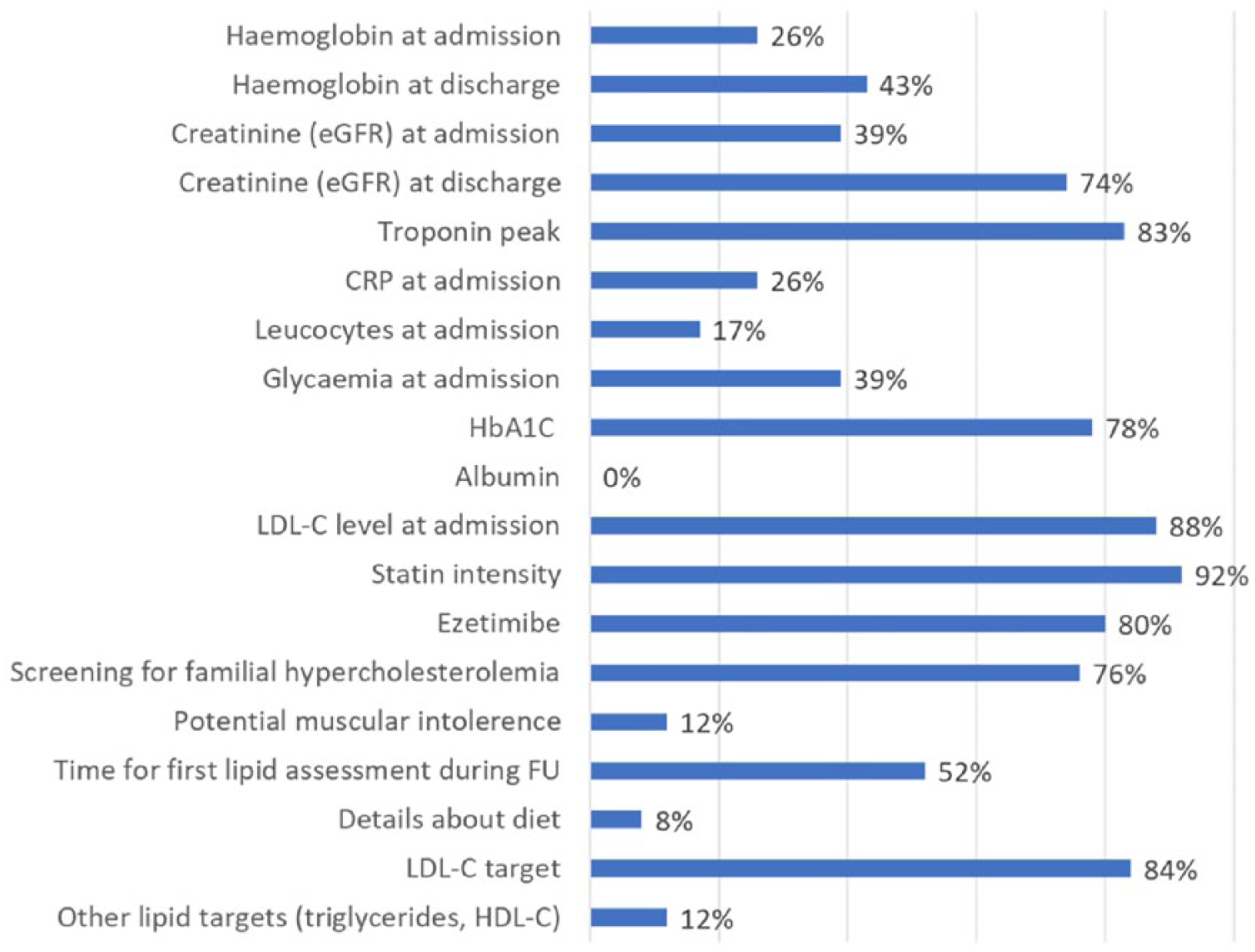
Results of the poll, lipid-lowering and antidiabetic treatments.
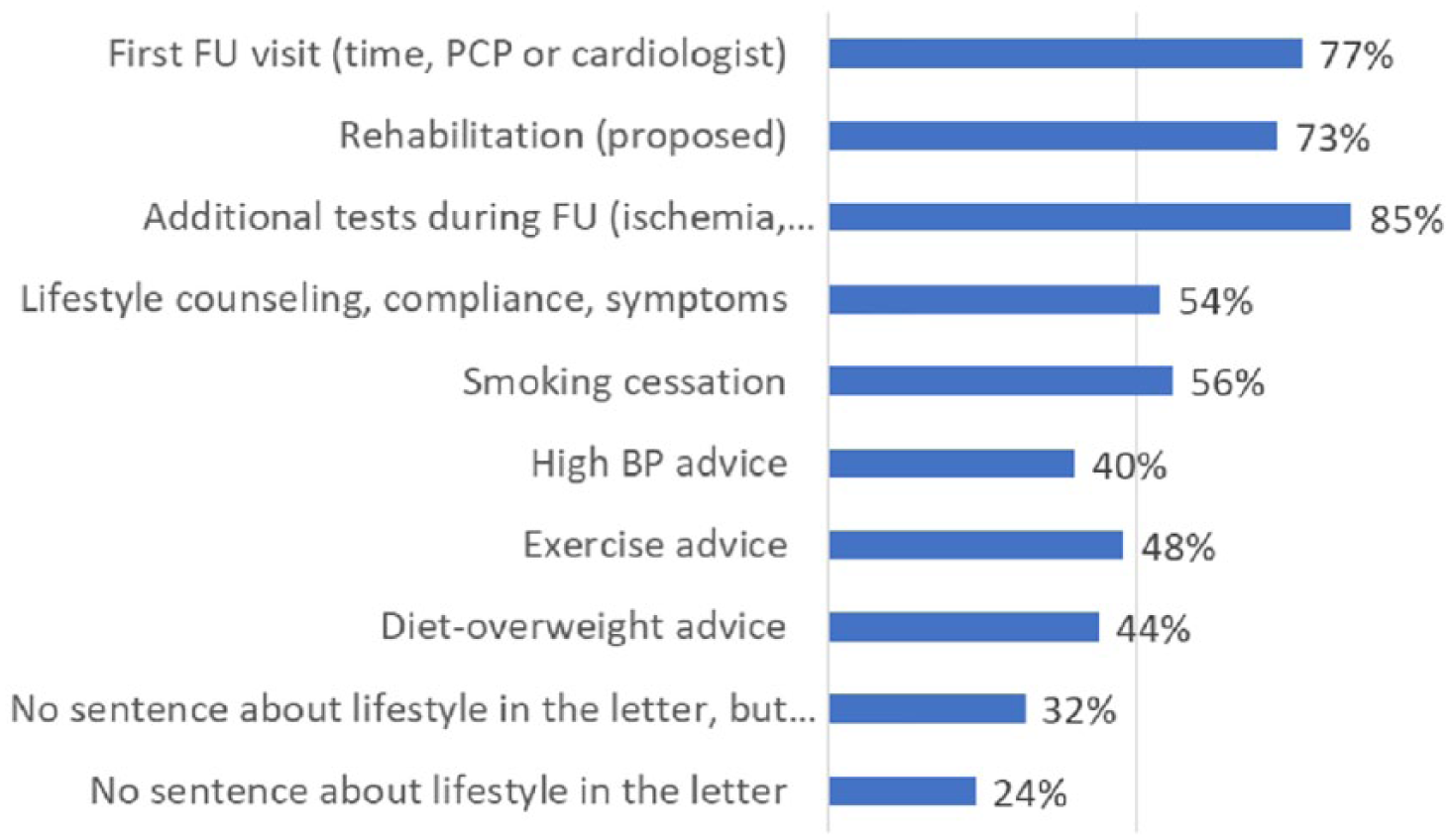
Results of the poll, structured pathway and follow-up.
Timeframe for sending and length of the discharge letter
Overall, 53% of the participants responded that the discharge letter should be ready and sent (or directly given to the patient) at discharge, while 85% agreed on a timeline within two days after discharge. A longer delay was considered unsuitable by our group and incompatible with optimal patient care. The majority of the group (88%) considered that the length of the letter should be ‘as short as possible’ (one or two pages) and 80% agreed that the letter should be written by a senior cardiologist or ‘under the supervision’ thereof.
Computer-based versus traditional
We observed discrepancies in the format of the discharge letter. Some physicians advocated a single document, limited to the main messages, to which could be appended, if necessary, additional material, such as technical reports from imaging or interventions, a copy of the coronary angiography (and percutaneous intervention, if any) (69%), a copy of the discharge electrocardiogram (69%) and documents for the patient’s information (54%). Other members of the group preferred to include all the information in a single document, in particular, by means of a computer-based document. No consensus was reached on the choice between traditional dictated letters, and self-generated and computer-generated documents. Indeed, in some centres, the discharge document is automatically generated using specific software on the basis of the information entered in their administrative, angiography, biology and clinical databases.
Structured versus non-structured
General agreement was reached on the use of a structured letter format. The following list details the essential content:
(a) Patient identification, cardiovascular risk factors and previous history;
(b) Reason for admission (symptoms) and final diagnosis;
(c) Invasive management including invasive strategy, coronary anatomy and revascularization;
(d) Risk assessment, including left ventricular ejection fraction;
(e) Main biological results;
(f) Medication at discharge;
(g) Therapeutic targets with specific details for the dual APT, LLT and antidiabetic treatments;
(h) Instructions for follow-up during the sub-acute and chronic phases.
Table 1 presents the eight headings of the structured discharge letter.
The eight headings of the structured discharge letter after acute myocardial infarction.
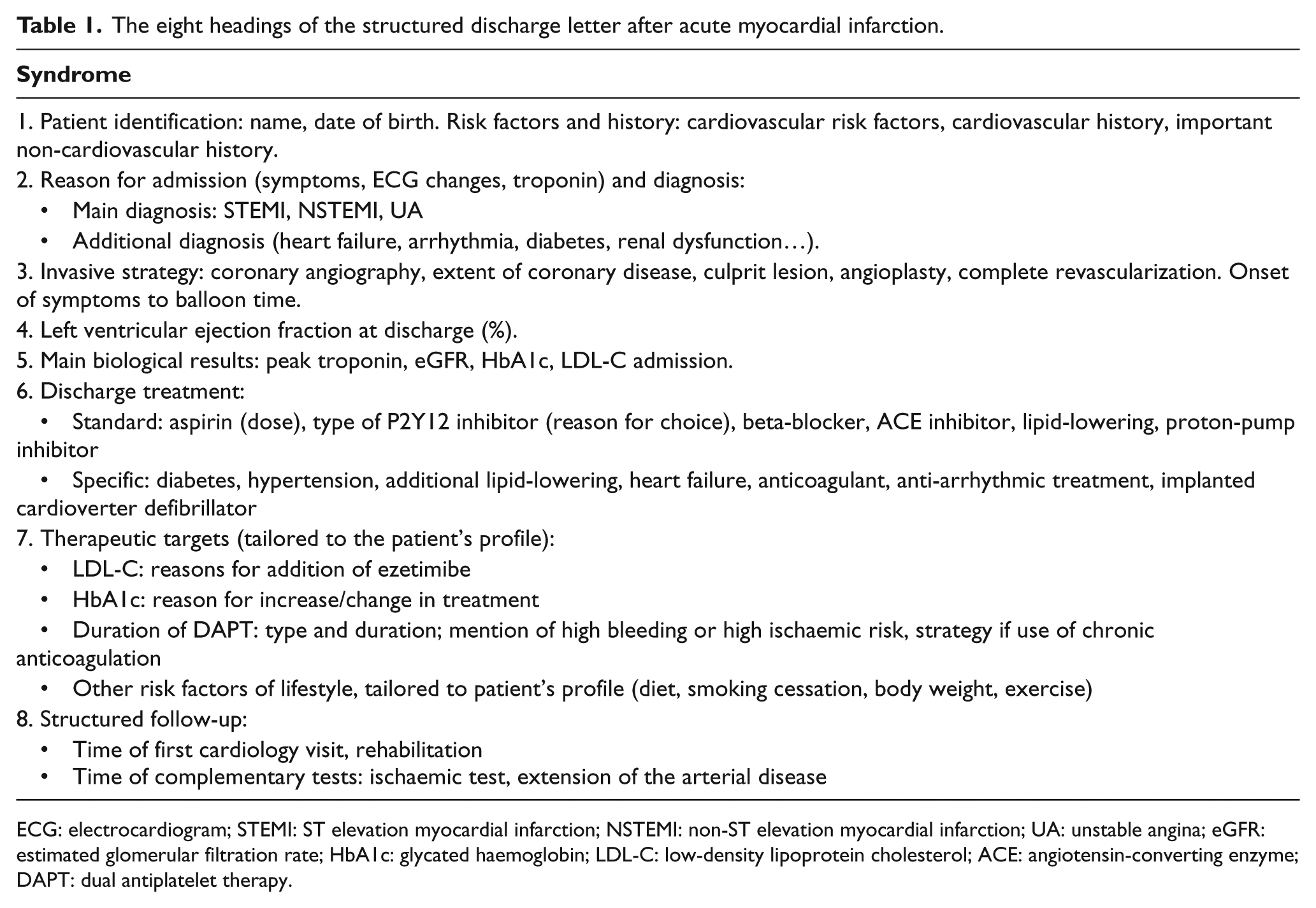
ECG: electrocardiogram; STEMI: ST elevation myocardial infarction; NSTEMI: non-ST elevation myocardial infarction; UA: unstable angina; eGFR: estimated glomerular filtration rate; HbA1c: glycated haemoglobin; LDL-C: low-density lipoprotein cholesterol; ACE: angiotensin-converting enzyme; DAPT: dual antiplatelet therapy.
General content of the discharge information
Almost all participants agreed to include cardiovascular risk factors and cardiovascular (but not non-cardiovascular) history, as well as the reasons for admission and the main diagnosis. The type of reperfusion (only for ST-segment elevation myocardial infarction), invasive strategy and extent of coronary disease were also identified as key points to mention. Regarding reperfusion, only the onset of pain-to-balloon time was required, no other specific time delays (such as transportation or door-to-balloon) were deemed necessary. The technique of revascularization and in-hospital complications were also selected.
Biology
The only biological results selected for transmission were: peak troponin (confirmed by 88% of group members), creatinine (eGFR) at discharge (74%), glycated haemoglobin (HbA1c) (78%) and low-density lipoprotein cholesterol (LDL-C) at admission (88%).
Discharge treatments
All group members agreed that it is necessary to describe the discharge treatments in detail with the exact molecule names, doses and duration of therapy. Despite the presence of electronically generated prescriptions, this reminder of the treatment was deemed necessary. Depending on the patient’s profile, three key components of the discharge treatment require specific comment, namely dual APT, LLT and antidiabetic treatments.
Discharge antithrombotic therapy
Before the discussions about how to report antithrombotic therapies in the discharge letter, the following points were presented to the group to remind all members of the risks and benefits of dual APT, as well as the current guidelines regarding reduced or prolonged prescription according to the patient’s risk profile: 10
After an AMI, with or without percutaneous coronary intervention (PCI) based on the CURE study, dual APT is recommended for 12 months. CURE demonstrated a 20% reduction in major adverse cardiac events but was associated with an excess in bleedings, 11 justifying the exclusion of patients at high-bleeding risk from this recommendation.7,8,10
Studies with more potent P2Y12 inhibitors (prasugrel and ticagrelor) showed superiority over clopidogrel, but with further excess of bleeding.12,13
Similarly, other antithrombotic strategies post AMI, with a platelet thrombin receptor inhibitor 14 or with a low dose direct oral anticoagulant, 15 showed a reduction in ischaemic events after myocardial infarction (MI), but at the price of an excess in bleedings.
These findings led to debate about the need to reduce the duration of antithrombotic treatments <12 months in patients defined at ‘high bleeding risk’. Conversely, one year post AMI, some patients remain at high ischaemic risk, 5 and this risk can be reduced by extending the duration of dual APT16,17 or by a combination of aspirin and low dose rivaroxaban 18 beyond one year.
Given the trade-off between the reduction in ischaemic events and the increase in haemorrhagic complications, the choices of the type of antithrombotic regimen and of its duration need to be tailored to the patient’s individual profile. To this end, the ESC 10 proposes the use of scores, during acute hospitalization, to decide whether to reduce the duration of dual APT (to less than 12 months) in high bleeding risk patients (the PRECISE-DAPT score 19 ) or, after 12 months, to decide whether to prolong dual APT (DAPT score 20 ).
Of note, the DAPT score supposes that the patient has been treated with dual APT for 12 months without bleeding event, which theoretically precludes its use at discharge after an acute coronary syndrome (ACS). Conversely, variables related to the coronary anatomy and PCI technique might not be known by the physician who will subsequently decide about the prolongation or cessation of dual APT and are often better apprehended during the index hospitalization. Indeed, the DAPT score takes into account variables related to the coronary anatomy and PCI technique, such as the number of diseased vessels, or the diameter and type of stent used. It should be, however, highlighted that paclitaxel eluting stents are no longer implanted in most countries and this remains a limitation to the use of the DAPT score in daily practice.
According to the results of the poll, the discharge letter should report the following: the prescription of aspirin and a P2Y12 inhibitor, with the relevant doses and duration of therapy (>90%); the anticipated dual APT duration (87%), although only 58% of participants thought it necessary to give explanations for the choice of one P2Y12 inhibitor over another. Depending on the patient’s profile, the following should be given in the discharge letter:
The reason(s) for shortening the dual APT duration, including the results of the PRECISE-DAPT score (70%), should be given.
The reasons for prolonged dual APT duration (or use of low dose rivaroxaban) after 12 months, including clinical, anatomical characteristics and DAPT score (65%), should be given.
The precise description of the antithrombotic regimen during the first 12 months (96%) in the case of combined chronic oral anticoagulant therapy should be given, but the reason for anticoagulant drug selection (over another) is not required (50%).
Discharge LLTs
As for the antithrombotic treatment, the following rationale was presented before the discussions about LLT to remind the group of current recommendations:
After AMI, the prescription of LLT at discharge is systematic, using high intensity statins, initiated as soon as possible, and irrespective of baseline LDL-C level, with the addition of ezetimibe if required to reach the recommended therapeutic target.7,8,21,22
The recommended target for LDL-C is <1.8 mmol/L (70 mg/dL); or a reduction of >50% if baseline LDL-C is between 1.8 and 3.5 mmol/L (70 and 135 mg/dL).7,8,21,22
This strategy needs to be implemented during hospitalization, since prevention treatment should be optimized before discharge.21,22
Assessment of LDL-C is recommended 4–6 weeks after treatment initiation to verify tolerance, adherence and efficacy.21,22
In contrast to these strong-grade recommendations, registry studies consistently show that high-intensity statins are prescribed in only 50–60% of patients, and ezetimibe in <5% at discharge. In addition, LLT intensity is likely to be reduced during follow-up. 23 As a result, less than one-third of patients24–26 reach the recommended LDL-C target at 12 months after ACS,24–26 leaving huge potential for improvement in secondary prevention.
Among the reasons for limiting LLT intensity, statin intolerance (mainly muscular) is reported as a frequent side effect soon after statin initiation. 27 It is a frequent cause of statin interruption. In this case, despite the existence of clear algorithms for re-challenging LLT, 21 statins are often definitively discontinued. Even when LLT is well tolerated, statin non-compliance is a growing explanation for sub-optimal LLT, partially fuelled by ‘negative stories’ in the lay press. 28 In addition, concerns about the safety of low LDL-C values could explain de-escalation in LLT, despite studies demonstrating the safety and efficacy of very low LDL-C under statins, 29 or under a combination of statins and other drugs.30,31
According to the results of the poll, the discharge letter should report the following points:
The level of LDL-C at admission (or assessed fasting after day 1);
The type and dose of statin prescribed at discharge;
The additional prescription of ezetimibe. Optionally, the reason for the use of a combination therapy should be detailed. A strategy for LLT at discharge, using high-intensity statins and ezetimibe according to admission LDL-C, has previously been proposed by the same Consensus Group and remains valid; 32
If and why familial hypercholesterolaemia is suspected;
The date of lipid assessment to be performed during follow-up;
The LDL-C target (i.e. recap of the ESC recommendations; depending on the patient, target LDL-C <1.8 mmol/L (70 mg/dL); or a >50% decrease in admission value).
Conversely, the group deemed that it is not necessary to mention the following points systematically in the discharge letter:
Diet or smoking cessation recommendations given to the patient;
Modalities for the management of muscular intolerance, if any;
Information about lipid parameters other than LDL-C at admission.
Diabetic status and treatments
Recent registries studies, such as EURO ASPIRE IV, have shown that the proportion of diabetic patients admitted for AMI is currently above 30%. 26 In addition, 3–5% of the patients without a history of diabetes have a HbA1c level >6.5% and can be considered as ‘newly diagnosed’ diabetics. When diabetic patients are already being treated, the HbA1c is often not at the target, justifying changes in the antidiabetic treatments. The clinical benefit of better glycaemic control is now clearly established in terms of micro- and macro-vascular complications, including all-cause mortality. According to European recommendations, in addition to lifestyle and diet, the use of metformin remains the first-line strategy when not contraindicated, but second- or third-line treatment can also be initiated, depending on the level of HbA1c and the patient’s characteristics. If insulin therapy is required, initiation or modification can be proposed, although it should be highlighted that many patients can be managed without insulin therapy. The following points were recalled:
Dipeptidyl peptidase 4 inhibitors are effective in HbA1c control, safe and well tolerated. 33
Glucagon-like peptide-1 receptor analogues are safe and effective in HbA1c control. Reductions in cardiovascular events 34 and mortality have been reported with liraglutide. 35
Sodium-glucose co-transporter-2 inhibitors are safe and effective. A reduction in cardiovascular events has been reported 36 and in cardiovascular mortality with empagliflozin. 37
Sulphonylureas are less attractive, since they expose the patient to a risk of hypoglycaemia. 38
Changes in treatments are driven by the HbA1c level, with different therapeutic targets applied according to the patient’s profile: 39
Target HbA1c between 6.5 and 7% (53 mmol/mol) in post MI patients;
Target HbA1c between 7% and 8% (64 mmol/mol) in patients with advanced cardiovascular disease, that is, patients with heart failure or triple vessel, left main or polyvascular disease or recent (< 6 months) stroke;
Target HbA1c up to 8% (64 mmol/mol) in patients with major chronic renal dysfunction (estimated glomerular filtration rate <30 ml/min);
Target HbA1c between 8% and 9% (75 mmol/mol) in elderly patients or patients considered as ‘frail’ or at risk of hypoglycaemia or dehydration.
The group recognized the importance of including the admission HbA1c value (78%), but not the admission glycaemia (39%). The importance of reporting HbA1c is irrespective of the patient’s status: in those without a history of diabetes, it supports the diagnosis of new-onset diabetes, and in those with known diabetes, it illustrates the quality of the treatment prior to admission.
The target HbA1c should also be reported in the discharge document, since different target values are applicable, depending on variables available during hospitalization and which may be more difficult to obtain during follow-up (for example, the extent of coronary disease). Supervision of a diabetologist for the treatment goals and adjustments during follow-up was strongly advocated.
Structured follow-up and rehabilitation
Apart from the time at which lipid testing should be performed (i.e. within 4–6 weeks after statin initiation or changes in LLT21,22), the ESC guidelines do not give clear recommendations for follow-up or for the date at which the first cardiological follow-up visit should occur. Conversely, participation in a rehabilitation programme is highly recommended, albeit without a clear definition of the duration and content of such rehabilitation programmes. Although most members of the group invite their patients to attend rehabilitation, and 73% said they would include this proposal in the discharge letter, it should be emphasized that, to date, there remains substantial variability in access to rehabilitation across regions in France. In some centres, rehabilitation is available and can be proposed in >70% of cases early after discharge, whereas in other centres, there are waiting lists and delays, discouraging patients from attending.
The need to plan the first follow-up visit by a cardiologist or by the PCP was recognized by 77% of the group. Participation in rehabilitation was considered as a structured pathway, including the first cardiological visit, but the timing of the first consultation with a cardiologist after AMI was dependent on local availability. In some centres, the first follow-up visit is performed by the referring PCP and the first cardiology consultation is only possible after 4–6 months. Nonetheless, all members concur that an early consultation with a cardiologist (i.e. at one month after discharge) would improve patient care.
The inclusion in the discharge letter of ‘general considerations’ or ‘automatically-generated sentences’ relating to lifestyle recommendation was a matter of some debate. Half of the participants argued that (1) this kind of advice should be given to the patients, not to the HCP; and (2) it adds unnecessary length to the document, whereas the content should be tailored to the patient’s profile. Therefore, our group did not consider that a reminder of lifestyle recommendations is essential for the discharge letter.
General documents for the patient’s information regarding atherosclerotic disease, risk factors, MI, primary and secondary prevention, lifestyle, measures to take in the case of symptoms cannot be considered a replacement for patient information and education, but are given as complementary material.
For 84% of the group, the need for additional tests (such as testing for residual ischaemia) or imaging (such as Duplex Ultrasound for the detection of the extent of arterial disease) is not systematic and needs to be explained in the letter when judged necessary.
Last, only 7% of the group considered that informing other HCPs about Quality of Care indicators is relevant, although 50% agreed that this information could be available in the patient’s chart.
An example of a standardized discharge letter containing all the mandatory information is given in Figure 6.
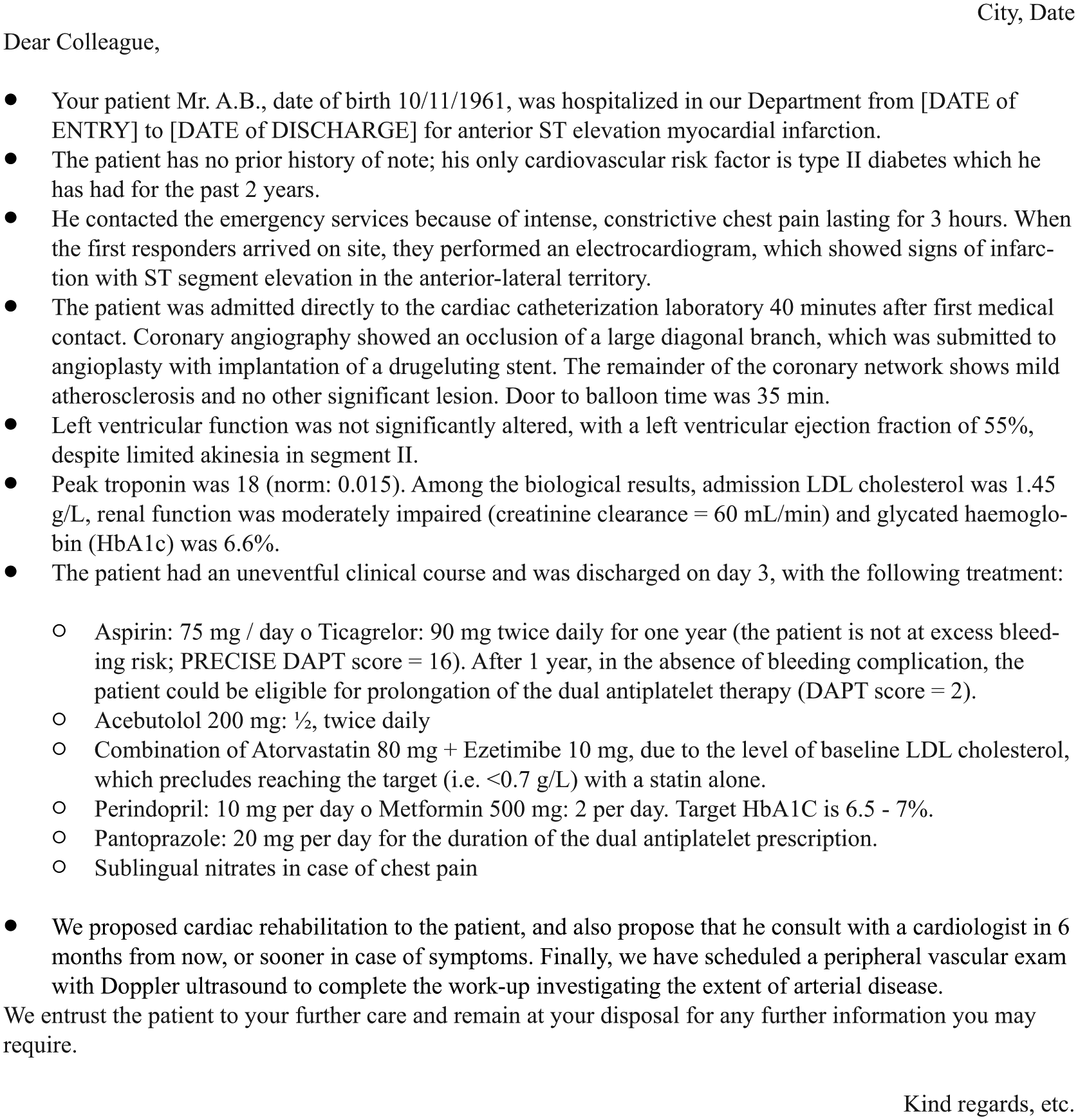
Example of discharge letter using of the eight-point template (for a patient admitted with ST elevation myocardial infarction and uncomplicated course).
Discussion
Sub-optimal discharge letters are part of the deficit in communication between specialists and PCPs, 6 in terms of both the content 2 and the timeframe of delivery. 1 Attempts to improve the quality of the information transferred between HCPs have long been under way, with various consecutive propositions, starting with a ‘problem list’ that was found to improve communication between specialists and PCPs. 40 The ‘problem list’ evolved into the ‘structured letter’, by adding a list of management proposals, 41 and subsequently matured into a ‘structured discharge document’, which includes diagnosis, stage of the disease, current problems, treatment objectives, prognosis, patient information and follow-up.42,43 Last, the use of computer-based documents is potentially the ultimate solution to avoid incorrect content and lack of standardization and to ensure timely availability.
Based on these observations, national authorities and various jurisdictions have developed ‘official’ datasets for discharge summaries, including promoting the use of a template or an electronic format, as for example in Northern Ireland, 44 Canada, 45 the United States, 46 France,47,48 Scotland, 49 Ireland 50 and the UK. 51 All these groups have finally proposed structured documents with a list of headings to be included in the clinical discharge report. It is unclear how these documents are used in routine practice, but in France, initial discussions among the present Consensus Group revealed that the discharge template proposed by the French National Health Authority (Haute Autorité de Santé (HAS)) is not widely used in daily practice. 47
Although compliance with the HAS recommendations was not a pre-requisite, the French Consensus document satisfies most of the requirements for an ‘official’, high-quality discharge document. The timeframe of delivery was identified as a major deficiency in the transmission as early as 1984, 6 and is still an issue in practice, since it has been shown that the discharge letters do not arrive within one week in 47%, 2 or arrive after 1–106 days in clinical studies. 52 In France, between 2008 and 2011, the proportion of discharge letters delivered in less than eight days increased from 26% to 48%, but content was considered suboptimal in 55%. 47
The members of the group declared that shortening this delivery delay was not only necessary, but mandatory, possible and desirable. The Consensus document is structured and accompanied by a template. The advantage of a specific structured discharge letter over a traditional document is that a standardized discharge letter requires a shorter transcription time 53 yet still improves medical communication between HCPs40,41 and is preferred by PCPs. 42 Given the variations in practice observed in our group, we considered that the final format could be left at the physician’s discretion, focusing on the timeframe of delivery and the medical content. The list of headings in the consensus document proposed here includes most of the points considered to be mandatory for a high-quality discharge document, particularly those recommended by the authorities, but also more specific points, such as for emergency departments 43 or after AMI.54,55 Compared with available ‘official’ documents, the template proposed here by the French Consensus Group is patient-directed and specific to the AMI setting. Indeed, four specific points are added, where transmission of information and advice is particularly important because they depend on patient characteristics, explain the discharge treatment and require further action during follow-up, namely: antithrombotic therapy, LLT, antidiabetic treatment and a specific post-AMI follow-up pathway.
One surprising result was the group’s decision to omit lifestyle recommendations from the document. This should not be interpreted as a denial of the importance of diet, smoking cessation, physical exercise and weight control on the part of the group. Rather, we considered that the main aim of the document was to provide other corresponding physicians with information specific to an individual patient. To this end, general statements that apply to everyone can be left out, unless the physician writing the report feels it necessary to insist on this point. In this case, it can be included under heading 7 of the proposed letter, in the sub-section ‘Other risk factors’. We also sought to reduce the length and time to delivery of the document by limiting the information to patient-specific details, without generalities. Additionally, the group considered that the document is mainly directed at physicians, who are aware of the importance of lifestyle counselling. Finally, the group was in favour of providing patient-specific documents at discharge; this can be implemented at the discretion of each physician.
Currently, there is no standard dual APT type and duration but, rather, dual APT is individualized according to the balance between thrombotic and bleeding risks in a given patient. Even using available scores, these risk estimations are complex and cumbersome to use, and require clinical, biological, anatomical and procedural variables that are often difficult to retrieve after hospitalization. Thus, our group decided to detail the prescription with recommendations for the duration. However, the group also emphasizes the need for a precise description of the coronary anatomy, in order to help cardiologists and PCPs adapt the duration of dual APT during follow-up. Ideally, in addition to the report, a copy of the coronary angiogram should be given to the patient.
Regarding the LLT, the prescription of high-intensity statins after AMI is far from ideal; de-escalation of treatment often occurs during follow-up and, as a result, the proportion of patients who are not at target LDL-C is above 50%, as shown in recent registries.24–26,56 Recalling the therapeutic targets recommended by guidelines may improve prescription rates at discharge, and increase maintenance and adherence during follow-up. 57 Additionally, explanations about the importance of LLT, efficacy, tolerance and compliance also have an educational value, not only for the patient, but also for the PCP.
Considering that 30–35% of the patients admitted for AMI are diabetics, the routine assessment of HbA1c during hospitalization provides an opportunity to evaluate the efficacy of treatment in diabetic patients and to detect new-onset diabetes. Given the currently available antidiabetic drugs and their impact on clinical outcomes, the selection of the best treatment has become important, but more complex. The discharge document proposes to detail the strategies according to the patient’s condition, therapeutic targets and specific follow-up pathway. Additionally, this discharge information might promote improved collaboration between cardiologists and diabetologists.
With the progressive reduction in the length of stay for AMI, there is a growing need for structured pathways for follow-up, but this remains a challenge in secondary prevention. 4 The group proposes to highlight the importance of rehabilitation and to add, in the discharge document, the time at which the first follow-up visit (by cardiologist or by the PCP) should be performed, as well as proposing systematic detection of peripheral vascular extension. If necessary, the time of the first ischaemic test or angiographic control should be included in the discharge document. As complementary information, material to be given to the patient or sent to the PCP is proposed, but not mandatory. At the discretion of the centre, a copy of the discharge letter or imaging documents (echocardiography or coronary angiography) may be added to the general documents. Easy-to-understand patient information in the form of flyers or booklets could be included, addressing such topics as arterial disease and MI, the potential progression of the disease, and the symptoms and actions in the case of adverse event as well as potential side effects of the prescribed drugs.
Limitations
As for all consensus groups, our group is not necessarily representative of the whole population of French physicians. Nonetheless, all the members of this group have practical clinical experience in caring for AMI patients, prescribing secondary prevention therapy and providing medical information to general practitioners and cardiologists. This discharge document applies only to patients admitted for AMI with an uncomplicated in-hospital course, and corresponds to the minimum amount of information that should be transmitted. Consequently, this discharge document must be differentiated from a discharge report, such as the detailed report about coronary angiography-revascularization, where detailed information is provided.
Conclusions
These discussions regarding the format, timeliness and content of the discharge letter after AMI highlight an important unmet need in the communication between hospital cardiologists and PCPs. The French Consensus Group considers that both timeliness and medical content could be improved using a structured discharge document, containing the most important headings. A short letter, delivered within two days (and ideally, on the day of discharge), and containing eight headings including, in addition to medical history, management, risk assessment, biology and discharge treatments, specific details and explanations about the antithrombotics, LDL lowering and antidiabetic treatments, and concerning the follow-up pathway, is considered to be an attainable goal.
Footnotes
Appendix 1. Full list of the members of the consensus group,with affiliations
Christophe Bauters, MD, Centre Hospitalier Régional et Universitaire de Lille, Lille and INSERM U744, Institut Pasteur de Lille, Université de Lille 2, and Faculté de Médecine de Lille, Lille; Cyrille Bergerot, MD, Centre d’Investigation Clinique de Lyon (CIC) et Service d’Explorations Fonctionnelles Cardiovasculaires, Groupement Hospitalier Est, Lyon, and INSERM UMR-1060, CarMeN Laboratory, Université Claude Bernard Lyon 1, Lyon; Farzin Beygui, MD, Service de Cardiologie, Centre Hospitalier Universitaire de Caen, Caen; Franck Boccara, MD, Cardiologie, CHU St Antoine, INSERM 938, UPMC, Paris; Eric Bonnefoy, MD, Hôpital cardiologique Louis Pradel, Lyon, France Université Lyon 1, Lyon; Eric Bruckert, MD, Endocrinologie métabolisme et prevention cardiovasculaire, Institut E3M et IHU cardiométabolique (ICAN), AP-HP, Groupe hospitalier Pitié-Salpétrière, 83 boulevard de l’Hôpital, 75013 Paris; Guillaume Cayla, MD, PhD, Cardiology department, CHU Nimes, University of Montpellier, Place Pr Debré, 30029 Nimes Cedex; Jean-Philippe Collet, MD, Université Pierre et Marie Curie (UPMC-Paris 06), Institut de Cardiologie, Pitié-Salpêtrière Hospital (AP-HP), ACTION Group, Paris; Pierre Coste, MD, Hôpital cardiologique du Haut Levêque, Pessac, France Université Bordeaux Segalen, Bordeaux; Vincent Descotes-Genon, MD, Fédération de Cardiologie, Centre Hospitalier Métropole Savoie, Chambéry; Gregory Ducrocq, MD, PhD, Cardiology Department, Bichat Hospital, 46 rue Henri Huchard, 75018 Paris; Meyer Elbaz, MD, Service de Cardiologie B, CHU Rangueil, TSA 50032, 31059 Toulouse; Michel Farnier, MD, Point Médical, Rond-Point de la Nation, 21000 Dijon; Emile Ferrari, MD, PhD, Department of Cardiology, University Hospital Nice, 30 Av de la voie Romaine, 06001 Nice; Dominique Guedj, MD, 118 Rue de la Pompe, 75116 Paris; Laszlo Levai, MD, Cardiologie, Cardiologie interventionnelle et LECV, Hôpitaux Civils de Colmar, 39 Ave de la Liberté, 68000 Colmar; Jacques Mansourati, MD, Department of Cardiology, Hôpital de La Cavale Blanche, University Hospital of Brest, 29609 Brest Cedex, and EA4324, University of Western Brittany, Brest; Nicolas Mansencal, MD, PhD, Department of Cardiology, Université de Versailles-Saint Quentin (UVSQ), Ambroise Paré Hospital, Assistance Publique-Hôpitaux de Paris (AP-HP), Centre de Référence des Maladies Cardiaques Héréditaires, INSERM U1018, Team 5, CESP, 9 Avenue Charles de Gaulle, 92100 Boulogne-Billancourt; Nicolas Meneveau, MD, PhD, Department of Cardiology, EA3920, University Hospital Jean Minjoz, Boulevard Fleming, 25000 Besancon; Christophe Meune, MD, PhD, Department of Cardiology, Avicenne University hospital Avicenne, Paris XIII University, INSERM UMR 942, Rue de Stalingrad, 93000 Bobigny; Olivier Morel, MD, Department of Cardiology, University Hospitals of Strasbourg, Nouvel Hospital Civil, Strasbourg; Patrick Ohlmann, MD, Department of Cardiology, University Hospitals of Strasbourg, Nouvel Hospital Civil, Strasbourg; Francois Paillard, MD, Department of Cardiology, University Hospital Pontchaillou, 2 rue Henri Le Guilloux, 35033 Rennes; Christophe Piot, MD, Clinique du Millénaire, 220 Boulevard Pénélope, 34000 Montpellier; Vincent Probst, L’institut du thorax, Service de cardiologie du CHU de Nantes et U1087, Bd Jacques Monod, 44093 Nantes cedex 01; Etienne Puymirat, MD, PhD, Assistance Publique-Hôpitaux de Paris (AP-HP), Hôpital Européen Georges Pompidou (HEGP), Department of Cardiology, 20 Rue Leblanc, 75015 Paris, and Université Paris-Descartes, Paris; Gilles Rioufol, MD, PhD, Hospices Civils de Lyon, Lyon; François Roubille, MD, PhD, Unité de soins intensifs cardiologiques-Intensive care unit, Cardiology Department, 191 avenue du Doyen Gaston Giraud, 34090 Montpellier, and PhyMedExp, University of Montpellier, INSERM U1046, CNRS UMR 9214,34295 Montpellier cedex 5; Pierre Sabouret, ME, Heart Institute, Pitié-SalpétrièreHospital, 47–83 Bd de l’Hôpital, 75013 Paris; Emmanuel Teiger, MD, Department of Cardiology, University Hospital Henri Mondor, Assistance Publique Hôpitaux de Paris (AP-HP), 51 Avenue du Maréchal de Lattre de Tassigny, 94010 Créteil, and Université Paris-Est Créteil, Créteil, France.
Conflict of interest
DA declares or lecture fees Astra-Zeneca, MSD, Pfizer. GL has received fees for lectures or consulting from Amgen, Sanofi, NovartisAstraZeneca, Bayer, BMS, Biopharma, Bristol-Myers Squibb, Boehringer-Ingelheim, Daiichi Sankyo, Eli Lilly, MSD Schering, Pfizer, Sanofi, Servier, and The Medicines Company. FS has received support from/participated in speaker’s bureau for Amgen, Merck, Pfizer, EliLilly, Daiichi-Sankyo and Sanofi. He has received honoraria from Amgen, Merck, Pfizer, EliLilly, Daiichi-Sankyo, BMS and Sanofi. He has received study honoraria as representative of a research association from Amgen, MSD, Sanofi, Pfizer and BMS. MK has received support from/participated in speaker’s bureau for Amgen, Merck and Sanofi. He has received honoraria from Amgen, Merck, Pfizer, AstraZeneca and Sanofi. He has received study honoraria as representative of a research association from Amgen, MSD, Sanofi and Novo Nordisk. JF reports speaker fees from Amgen, MSD, Sanofi and Servier. LB reports unrestricted grants for research from Boston Scientific, Medtronic, Abbott, Biotronik, speaker fees and consulting with Astra-Zeneca and MSD. No other author has any conflict of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.