
Abstract
Background
We aimed to externally validate an emergency department triage algorithm including five hierarchical clinical variables developed to identify chest pain patients at low risk of having an acute coronary syndrome justifying delayed rather than immediate evaluation.
Methods
In a single-centre cohort enrolling 29,269 consecutive patients presenting with chest pain, the performance of the algorithm was compared against the emergency department discharge diagnosis. In an international multicentre study enrolling 4069 patients, central adjudication by two independent cardiologists using all data derived from cardiac work-up including follow-up served as the reference. Triage towards ‘low-risk’ required absence of all five clinical ‘high-risk’ variables: history of coronary artery disease, diabetes, pressure-like chest pain, retrosternal chest pain and age above 40 years. Safety (sensitivity and negative predictive value (NPV)) and efficacy (percentage of patients classified as low risk) was tested in this initial proposal (Model A) and in two additional models: omitting age criteria (Model B) and allowing up to one (any) of the five high-risk variables (Model C).
Results
The prevalence of acute coronary syndrome was 9.4% in the single-centre and 28.4% in the multicentre study. The triage algorithm had very high sensitivity/NPV in both cohorts (99.4%/99.1% and 99.9%/99.1%, respectively), but very low efficacy (6.2% and 2.7%, respectively). Model B resulted in sensitivity/NPV of 97.5%/98.3% and 96.1%/89.4%, while efficacy increased to 14.2% and 10.4%, respectively. Model C resulted in sensitivity/NPV of 96.7%/98.6% and 95.2%/91.3%, with a further increase in efficacy to 23.1% and 15.5%, respectively.
Conclusion
A triage algorithm for the identification of low-risk chest pain patients exclusively based on simple clinical variables provided reasonable performance characteristics possibly justifying delayed rather than immediate evaluation in the emergency department.
Introduction
Chest pain is one of the most frequent causes of emergency department (ED) consultation worldwide and acute coronary syndrome (ACS) is the principal diagnosis to be ruled in or out in this scenario.1–3 Suspected ACS results in 5% to 10% of all ED consultations, generating more than 10 million ED attendances worldwide, with about four million patients ultimately hospitalized because of confirmed or suspected ACS as the cause of their symptoms.3,4 As EDs are frequently overcrowded, and ACS is a highly time-dependent disease, many efforts have been aimed at shortening the time between the arrival of a patient with symptoms consistent with ACS and the completion of the clinical evaluation.5–7 This was one of the main drivers that led to the creation of chest pain units (CPUs), specifically-dedicated physical spaces in the ED where such patients can undergo rapid and uniformly standardized evaluation. These units have gained increasing popularity since their creation in the early 1980s and are currently present in many EDs.2,8,9
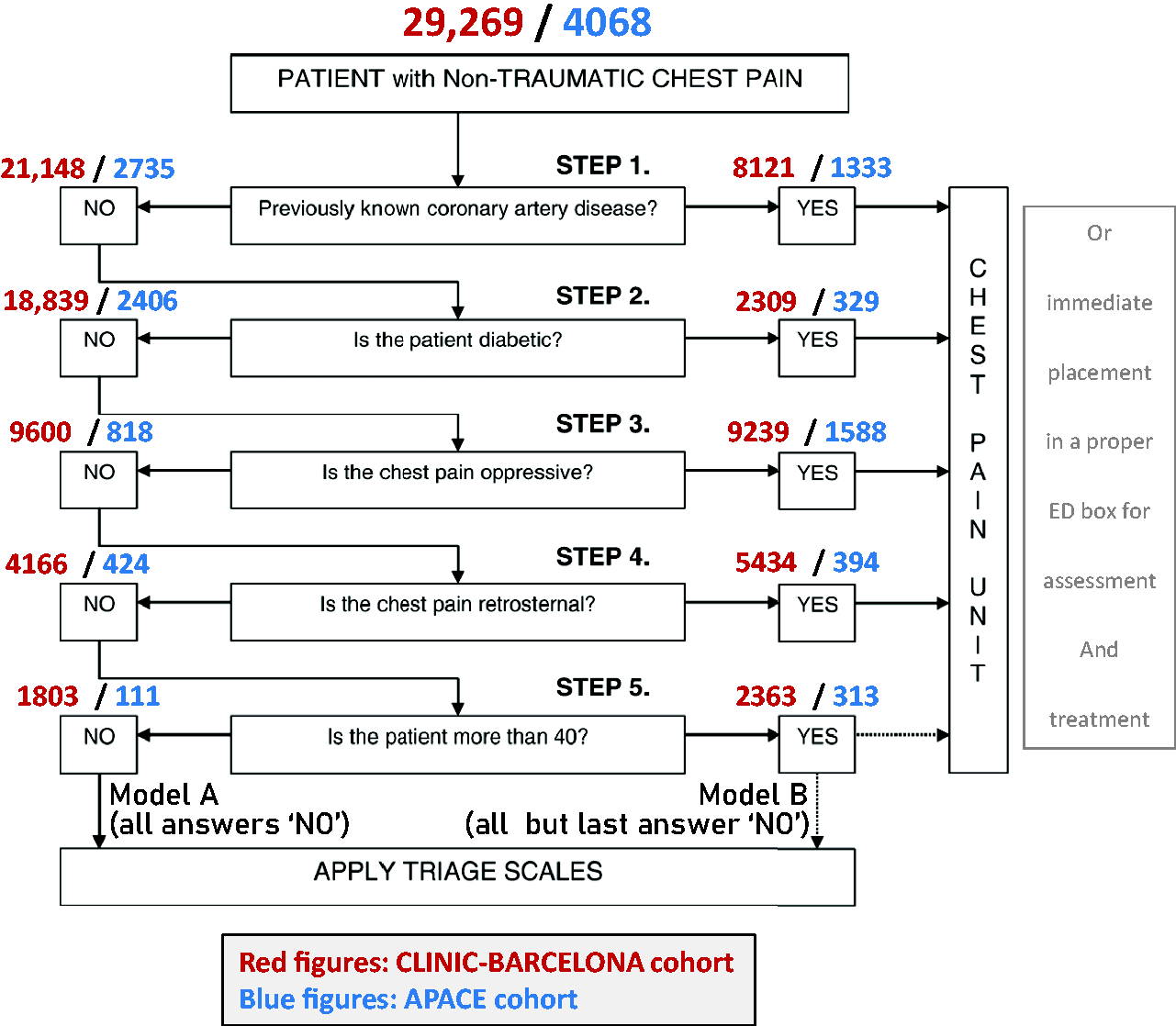
Implementation of CPUs has partially corrected the delay in providing immediate care to patients with suspected ACS. 1 However, a continuous increase rate of lower risk patients being referred to the ED has resulted in a progressive loss of sensitivity in the use of CPUs and has been associated with an increased number of patients with symptoms caused by diagnoses other than ACS. 10 One attempt to contribute towards solving the overcrowding in EDs and CPUs was the development of a triage algorithm based on five simple clinical variables easy to obtain at the triage level. 11 The aim of such a strategy was to identify chest pain patients with a low clinical risk for ACS, justifying a delayed rather than an immediate evaluation in the general ED or CPU, according to the infrastructure of the ED department. Triage towards ‘low-risk’ required absence of all five clinical ‘high-risk’ variables: history of coronary artery disease, diabetes, pressure-like chest pain, retrosternal chest pain and age above 40. The aim of this study was to externally validate an ED triage algorithm in two large cohorts, and to ascertain whether a modification in the algorithm could improve its performance.
Methods
Study design and setting
This was a secondary analysis of two large acute chest pain cohorts: the prospective observational single-centre CLINIC-BARCELONA cohort, which collects data of all consecutive patients attending to the CPU of the Hospital Clínic of Barcelona (Catalonia, Spain), and the prospective international multicentre Advantageous Predictors of Acute Coronary Syndromes Evaluation (APACE) cohort enrolling adult patients with acute chest discomfort in 12 centres in five European countries (ClinicalTrials.gov registry, number NCT00470587).
Selection of participants
For the CLINIC-BARCELONA cohort we used data from patients recruited between January 2008 and December 2017 (10 complete years). Details of the organizational characteristics of the CPU have been published elsewhere.10,12 Briefly, this CPU opened in 2002, and since 2006 data regarding clinical, electrocardiographic and exploratory findings recorded by emergency physicians at the time of patient presentation were entered into an electronic database. This database was specifically designed to provide a final medical report for suspected ACS patients after their ED care and to construct a codified database with all suspected ACS patients attended in the ED. In this CPU, all patients complaining of non-traumatic ACS symptoms undergo a complete assessment until a final diagnosis is achieved and a decision made to admit or discharge. Recruited patients included in the derivation 11 (year 2002) and validation 13 (years 2006–2007) previous studies, as well as patients in whom no final diagnosis was achieved in the CPU, were excluded.
Details of the design and conduct of the APACE cohort are published elsewhere.14–16 Briefly, adult patients presenting to the ED with symptoms suggestive of myocardial infarction (MI), such as any kind of acute chest discomfort and angina pectoris, were recruited. For this analysis, patients in whom the diagnosis remained unknown even after final adjudication and at least one elevated high-sensitivity cardiac troponin T (hs-cTnT) concentration, thereby possibly indicating MI, as well as patients included from Hospital Clínic of Barcelona (in order to eliminate duplications as they were already included in the CLINIC-BARCELONA cohort), were excluded.
To be considered in our analysis, cases in each cohort were required to have recorded the following data: the five clinical risk variables included in the algorithm (previous coronary artery disease, diabetes, pressure-like chest pain, retrosternal location of chest pain, and age) and the final diagnosis, which was classified as ACS/non-ACS (outcome variable).
Data collection
For every patient, data on demographics (age, sex), cardiovascular risk factors (hypertension, hypercholesterolaemia, diabetes, current smoking, family history of early ischaemic cardiomyopathy), cardiovascular comorbidities (myocardial infarction, percutaneous coronary intervention, heart failure, stroke, peripheral artery disease, and renal insufficiency), chronic treatments (antiaggregants, anticoagulants, renin–angiotensin system inhibitors, beta-blockers, diuretics, nitrates and calcium antagonists), chest pain characteristics, and vitals at ED arrival (systolic and diastolic blood pressure, and heart rate) were collected on an electronic database for the CLINIC-BARCELONA cohort and on specific case record forms for the APACE cohort. Routine interventions and management of patients was left to the discretion of the attending physician.
Outcome variables
The outcome variable was considered to be the final diagnosis of ACS (defined as unstable angina, non-ST elevation myocardial infarction, and ST elevation myocardial infarction) after ED care, as defined in the derivation study. In the CLINIC-BARCELONA cohort, the final diagnosis (ACS/non-ACS) was taken as reported by the attending emergency physicians in the electronic medical report, with no external adjudication or follow-up being performed beyond these clinical data, while in the APACE cohort the diagnosis was centrally adjudicated by two independent cardiologists (University Hospital Basel) using two sets of data: first, all available medical records obtained during clinical care including the 90 day follow-up information; second, study-specific assessments including detailed chest pain characteristics using 34 predefined criteria and serial hs-cTnT blood concentrations obtained from study samples. In situations of disagreement about the diagnosis, cases were reviewed and adjudicated in conjunction with a third cardiologist.
Ethical standards
For the CLINIC-BARCELONA cohort, use of the CPU database with personal patient data encoded to protect privacy was authorized by the Ethics Committee at the Hospital Clínic of Barcelona (Catalonia, Spain; protocol reference HCB/2019/0775). For the APACE cohort, the study was approved by the local Ethics Committees of each participating centre. Written informed consent was obtained from all patients.
The present study was carried out in strict compliance with the principles of the Declaration of Helsinki. The authors designed the study, gathered and analysed the data according to the STARD (Standards for the Reporting of Diagnostic Accuracy Studies) guidelines 17 for studies of diagnostic accuracy, vouch for the data and analysis, wrote the paper and decided to submit the manuscript.
Statistical analysis
Discrete variables were expressed as absolute values with percentages and continuous variables as medians with interquartile range. We ran the same analysis in parallel in the two cohorts (CLINIC-BARCELONA and APACE) as presented in the original paper that derived the initial algorithm. This included: a) an estimation of the adjusted odds ratio (OR) with 95% confidence interval (95% CI) in the multivariable model that included the five variables finally included in the algorithm; b) calculation of the area under the curve of the receiver-operating characteristic with the 95% CI using the ORs for these five variables obtained in our two validation cohorts; c) a detailed distribution of our patients through the algorithm; d) analysis of the performance of the algorithm in the two cohorts, including sensitivity, specificity, positive predictive value, negative predictive value (NPV), and positive and negative likelihood ratios; and e) estimation of efficacy, calculated as the percentage of patients that the algorithm rules out for immediate evaluation. The values obtained in this validation study were qualitatively compared with those obtained in the original derivation study.
Analysis of the safety and efficacy was performed for the two models proposed in the original derivation study: absence of clinical variables (i.e. answering ‘NO’ to all five questions, Model A) and in the presence of the last clinical variable (i.e. answering ‘NO’ to the first four questions and allowing the answer ‘YES’ or ‘NO’ to the age criterion, Model B). In addition, in order to try to improve the safety and efficacy of the algorithm, we repeated these analyses in a new different scenario, allowing the presence of up to one clinical variable, whichever of the five (Model C). We planned to only consider this additional proposal based on its simplicity, the easiness to ask the five questions during the triage interview (precluding the construction of more complicated strategies, as new hierarchical algorithms or decision trees) and because, at the end, this strategy constituted the most parsimonious approach to our secondary objective.
Statistical analyses were performed with SPSS software (24.0 version; IBM, New Castle, New York, USA), MedCalc (19 version, MedCalc Software, Belgium) and STATA software (version 15.1; Stata Corp, College Station, Texas, USA).
Results
Characteristics of study population
Overall, 33,337 patients met the entry criteria for this analysis, of which 29,269 were from CLINIC-BARCELONA and 4068 from the APACE cohorts (Figure 1). A total of 2749 (9.4%) patients had a final diagnosis of ACS in the CLINIC-BARCELONA cohort (340 STEMI, 1077 non-STEMI, 1332 unstable angina) in comparison with 1157 (28.4%) in the APACE cohort (154 ST-elevation MI (STEMI), 640 non-STEMI, 363 unstable angina). Patients’ clinical characteristics are presented in Table 1. Although both cohorts were predominantly male and had very similar median age (59 vs. 61 years, respectively), they differed extensively in many variables, reflecting the differences in patient recruitment strategies. For example, cardiovascular risk factors were more common in the APACE cohort, as were most of the cardiovascular comorbidities and chronic treatments.
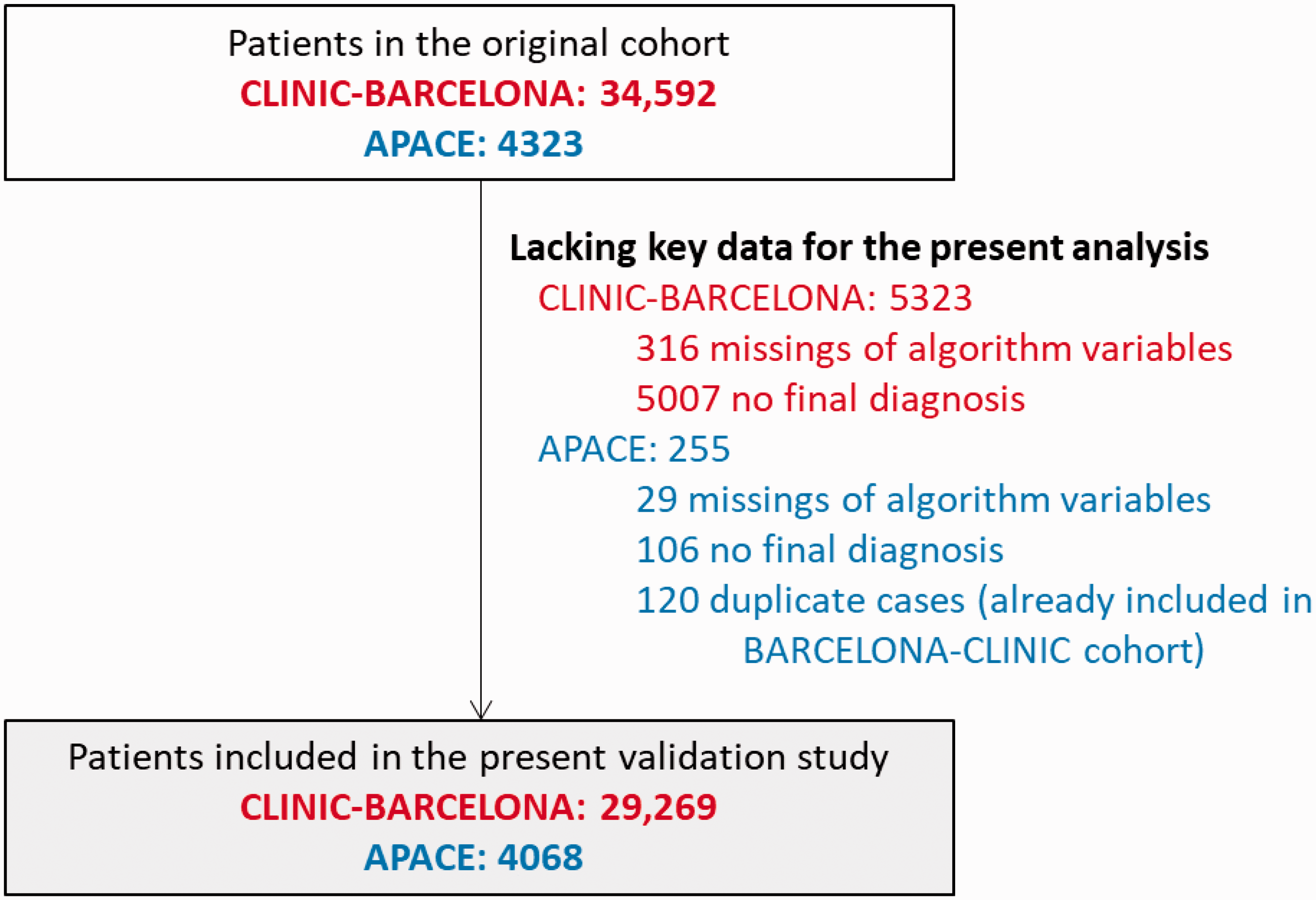
Flow chart for patient inclusion in the two cohorts in the present study.
Characteristics of patients with non-traumatic chest pain from the two cohorts evaluated in the present study.
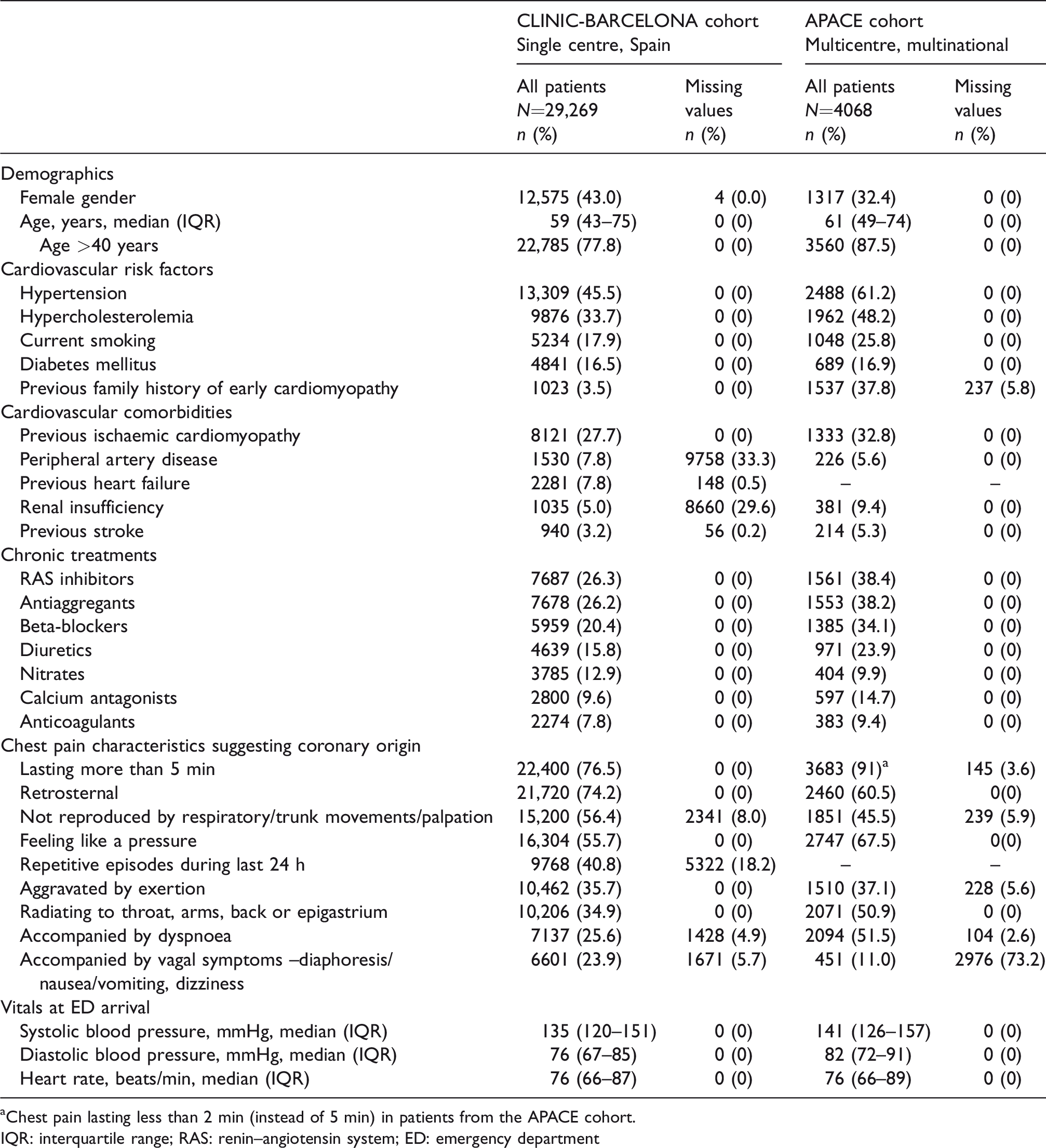
Chest pain lasting less than 2 min (instead of 5 min) in patients from the APACE cohort.
IQR: interquartile range; RAS: renin–angiotensin system; ED: emergency department
Main results
The effect size of the five clinical variables on the outcome (final diagnosis of ACS) is presented in Table 2. When all five variables were combined together in a single score, the c-statistic to rule out ACS was 0.76 (95% CI: 0.75–0.77) in the CLINIC-BARCELONA cohort and 0.72 (95% CI: 0.70–0.73) in the APACE cohort (Figure 2).
Adjusted odds ratios for the five variables included in the original derivation cohort that were included in the predictive triage model to rule out acute coronary syndrome during the triage interview obtained in the two cohorts used in the current validation study.
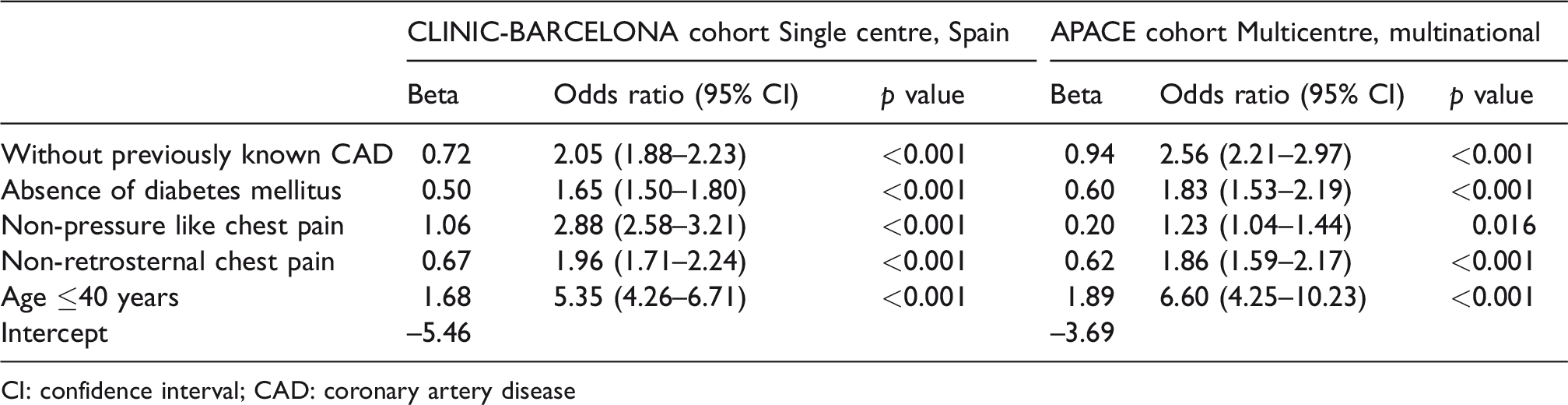
CI: confidence interval; CAD: coronary artery disease
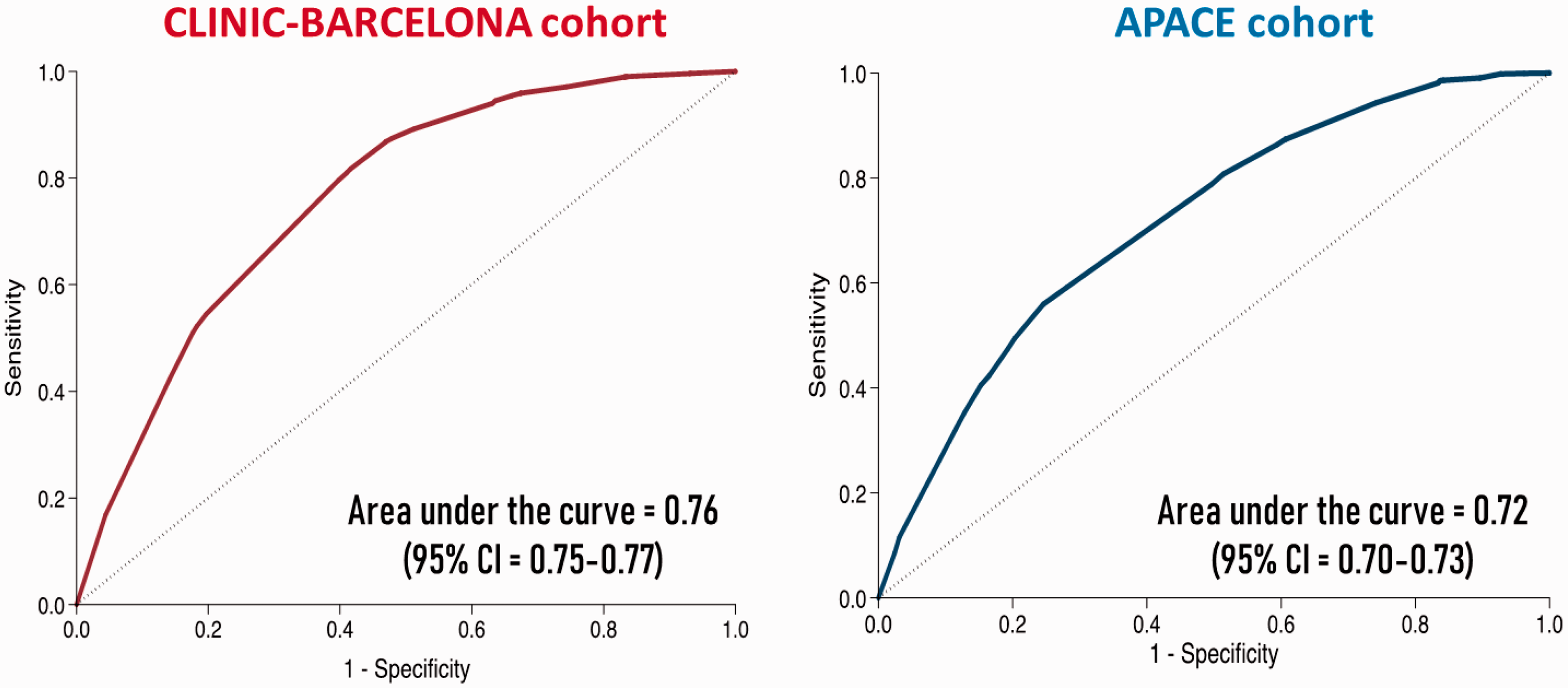
The receiver-operating characteristic curves of the predictive triage model obtained with the two cohorts in the present study.
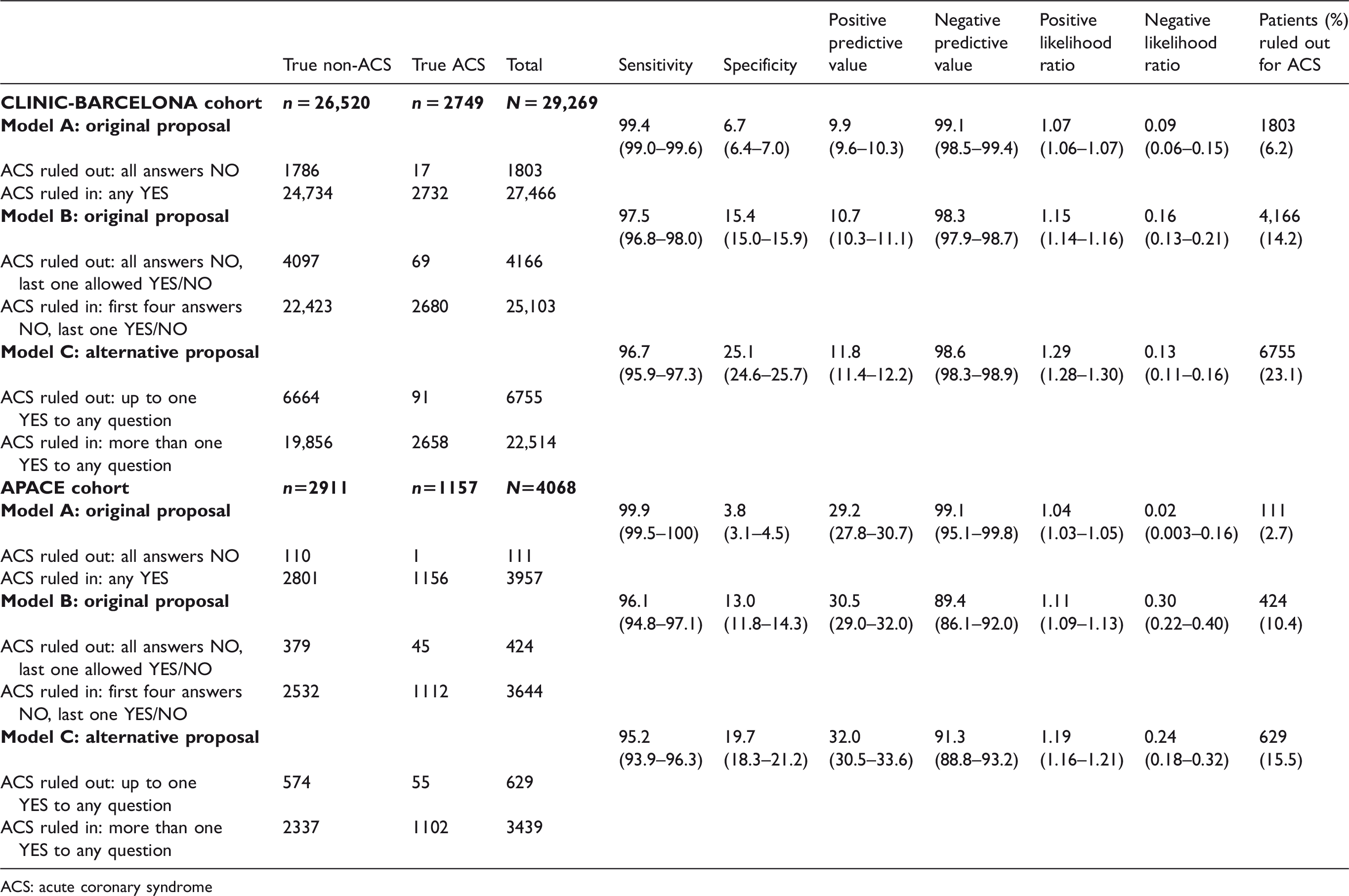
The flow of our patients through the triage algorithm is depicted in Figure 3. As a result of the distribution, the safety of the algorithm to rule out ACS when all five clinical variables were absent (original Model A) was very good, with a sensitivity of 99.4% (95% CI: 99.0–99.6) and 99.9% (95% CI: 99.5–100) for the CLINIC-BARCELONA and APACE cohorts, respectively, and a NPV of 99.1% (95% CI: 98.5–99.4) and 99.1% (95% CI: 95.1–99.8), respectively. However, efficacy was very low, excluding only 6.2% and 2.7%, respectively, of patients from CPU admission (Table 3). Omission of the last clinical variable (age criterion, Model B) resulted in a sensitivity and NPV of 97.5% (95% CI: 96.8–98.0) and 98.3% (95% CI: 97.9–98.7), respectively in the CLINIC-BARCELONA cohort, and 96.1% (95% CI: 94.8–97.1) and 89.4% (95% CI: 86.1–92.0), respectively in the APACE cohort. Efficacy increased to 14.2% and 10.4% in the CLINIC-BARCELONA and APACE cohorts, respectively (Table 3).
Detailed description of the ruling out process at each step of the triage flowchart for the patients from the two cohorts included in the present study.
Patient distribution following the algorithm application according to the two originally proposed models (A and B) for ruling out acute coronary syndrome proposed by the derivation study and according to the new alternative models (C) proposed in the present study in the two validation cohorts evaluated in the present study.
ACS: acute coronary syndrome
The exploration of the alternative Model C allowing the presence of one clinical high-risk variable (i.e. irrespective of the hierarchical position occupied by the variable in the algorithm) provided a sensitivity of 96.7% (95% CI: 95.9–97.3), a NPV of 98.6% (95% CI: 98.3–98.9) and an efficacy of 23.1% in the CLINIC-BARCELONA cohort. Lower sensitivity and NPV were obtained using this alternative model in the APACE cohort, with an efficacy of 15.5% in ruling out patients to be seen in the CPU (Table 3).
Details of the type of ACS in the false negative patients resulting from the application of the original algorithm and the alternative model are presented in Table 4.
Details of the final diagnosis of false negative cases (patients who would not be triaged to a chest pain unit according to the proposed algorithm).
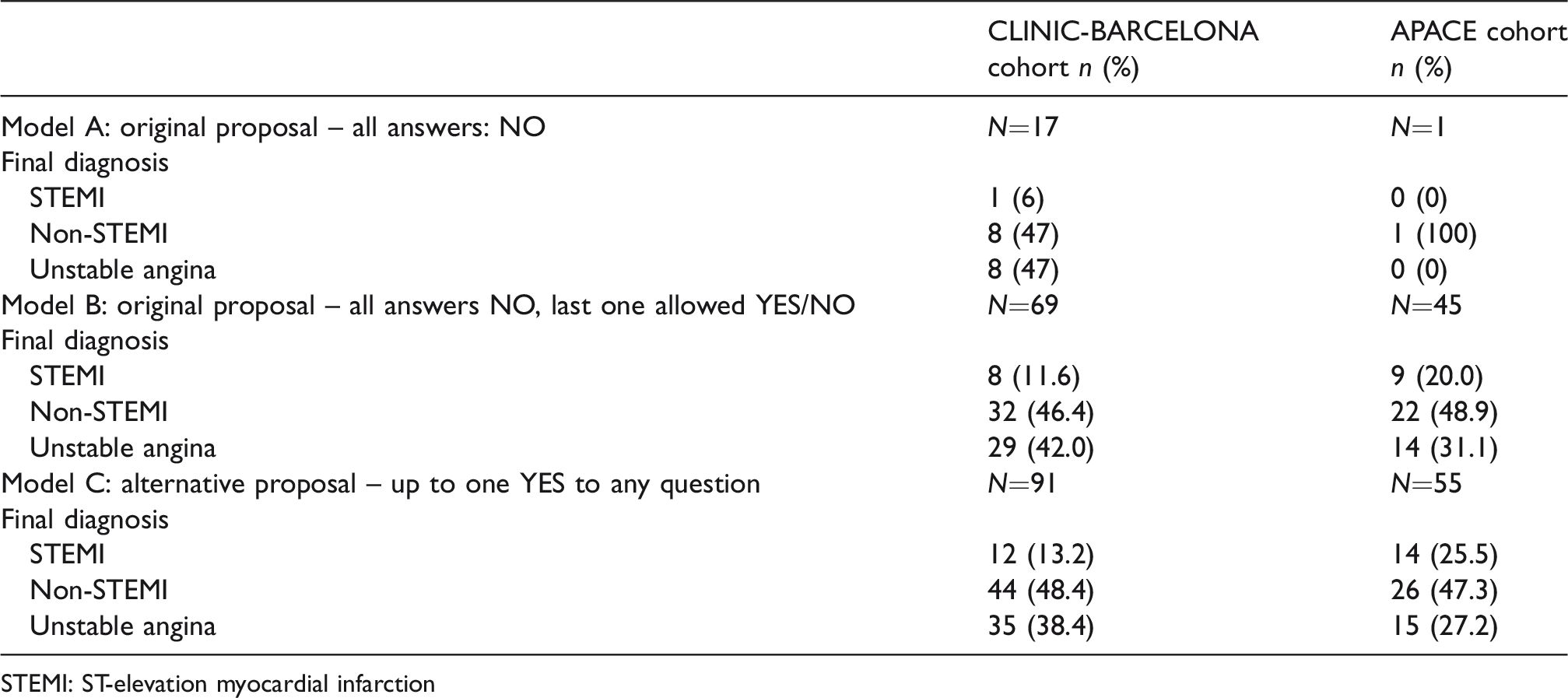
STEMI: ST-elevation myocardial infarction
Discussion
Our study aimed to validate a previously derived algorithm to detect chest pain patients at very low risk of having an ACS during the ED triage process. The main goal of this triage algorithm is to identify low-risk patients for whom a delayed rather than an immediate evaluation would be justified. The potential utility of such a strategy could be far reaching, as every ED patient is initially triaged to determine the priority of care and the five clinical variables included in the algorithm are easily obtainable by nurses. Our results, obtained in two independent cohorts, are consistent and show three major findings.
First, safety of the original model was very high in both CLINIC-BARCELONA and APACE cohorts (sensitivity of 99.4% and 99.9% and NPV of 99.1% and 99.1%, respectively), but efficacy was very low with only 6.2% and 2.7% of patients identified as ‘low-risk’, respectively. This efficacy contrasts with the 12% reported in the initial derivation study, 11 but is close to the 5.2% reported in the first validation study. 13 Such a low efficacy (at most one in 20 chest pain patients would be classified as ‘low-risk’) substantially questions the clinical relevance of this triage algorithm as initially proposed. Second, the original alternative modification proposed by authors in the original derivation study omitting age below 40 years as a criterion (Model B) resulted in a greater efficacy (14.2% and 10.4%, respectively), albeit a decrease in safety (sensitivity of 97.5% and 96.1% and NPV of 98.3% and 89.4%, respectively). Again, efficacy was substantially lower than the 25.4% and 24.3% reported in the initial derivation and validation studies, respectively. Third, the alternative modification proposed herein allowing 1/5 high-risk criteria (Model C) resulted in a sensitivity of 96.7% and 95.2% and a NPV of 98.6% and 91.3%, while increasing efficacy to 23.1% and 15.5%, respectively. These performance characteristics were comparable to that reported previously for the original modification.
It is hard to define the minimally clinically acceptable NPV for such a triage algorithm. In a survey answered by more than 1000 US emergency physicians that were asked about the acceptable risk of major adverse cardiac event in patients with chest pain soon after discharge from the ED, a miss rate of more than 2% was uniformly considered unacceptable, and almost half of the clinicians accepted a miss rate of up to 1% at maximum. 18 However, this is for patients discharged from the ED, a strategy that is not applicable here. This is because the result of the triage flowchart application is not to discharge patients, but to identify low-risk chest pain patients in whom a delayed evaluation (performed in the CPU or the ED) could be justified, hence lower sensitivity and NPV could be justified, as the main unwanted result of a too flexible strategy would be a potential increment in the elapsed time until the final diagnosis achievement.
It is important to point out that among both cohorts, sensitivity for each model did not differ (as observed by the overlapping of CIs). However, NPV was lower (except for Model A) in the APACE cohort in comparison with the CLINIC-BARCELONA cohort. The difference in prevalence for ACS between cohorts explains this finding, as the CLINIC-BARCELONA cohort showed a prevalence of 9.4% in contrast to the 28.4% of the APACE cohort. Interestingly, Model A is not clinically useful due to the unsatisfactory efficacy found in the derivation 11 and validation 13 studies as well as in the current study. The higher and clinically acceptable efficacy exhibited in previous studies by Model B has not been demonstrated in our two contemporary, larger, cohorts. However, we believe that the alternative modification proposed in the present study (Model C) provides reasonable safety and efficacy to allow its use in several ED clinical scenarios.
To date, many efforts have been made to derive chest pain risk stratification tools to help physicians make safer decisions, but nearly all of them include electrocardiogram recording and blood sampling for cardiac troponin T/I. Currently, the most extended approach is based on sequential cardiac troponin T/I sampling and proper interpretation of the absolute troponin values (single sample) as well as the kinetic of cardiac troponin T/I changes between the two time points (two samples). Indeed, the 0/3-h algorithm and the 0/1-h algorithm are recommended with a class I recommendation in current clinical practice guidelines. 5 The real impact of applying this triage flowchart in real world EDs, especially with the alternative model (Model C) proposed herein, on improving timing and outcomes of patients with ACS has not been tested in the present study and should be ascertained in the future.
The present study should be interpreted in the context of its limitations. First, the CLINIC-BARCELONA cohort comes from the same centre that derived the algorithm. However, cases included in the initial derivation (run in 2002) and validation (2005–2006) studies were not included in the current validation study (run between 2008 and 2017); accordingly, the latter has to be considered an adequate validation cohort (more contemporary and larger than the previously ones) for the purposes of the present study. Second, the final diagnosis of the patients from the CLINIC-BARCELONA cohort was based exclusively on the discharge report from the CPU, and there was no external adjudication or subsequent follow-up period. Therefore, it is possible that there was a small percentage of error in these diagnoses. Third, two out of the five questions included in the flowchart are subjectively described by patients (chest pain location and characteristics). Despite this potential weakness, since 1985, these variables not only have repeatedly been included in studies assessing patients with chest pain, but also have been found to be significant in diagnosing MI.19,20 Therefore, most nurses and physicians have learned how to reliably interrogate patients with respect to this issue, thus reducing the individual variability. Fourth, as the main reason for patient inclusion to validation cohorts was the presence of chest pain as main clinical complaint, some populations (such as women, patients with diabetes or coronary artery bypass grafting and elders, who typically exhibit fewer classical symptoms and even absence of chest pain)21,22 can be underrepresented in our analysis. Finally, our cohorts are mainly constituted by White Caucasians, and transposition of our results to populations with other race predominance has to be cautious, as chest pain characteristics may vary among different races. 23
In summary, a triage algorithm for the identification of low-risk chest pain patients exclusively based on simple clinical variables provided reasonable performance characteristics possibly justifying delayed rather than immediate evaluation in the ED.
Footnotes
Acknowledgement
ÒM and PL-A contributed equally to this manuscript and should be considered as first author.
Conflict of interest
We disclose that ÒM received competitive grants from the Instituto de Salud Carlos III supported with funds from the Spanish Ministry of Health and FEDER (PI15/01019, PI15/00773, PI18/00393, PI18/00456), Catalonia Government (SGR 2009/1385, 2014/0313, 2017/1424), and the Fundació La Marató de TV3 (2015/2510); GM-N is granted for research by Hospital Clínic of Barcelona, Catalonia, Spain; JB received research grants from the University Hospital of Basel, the Division of Internal Medicine, the University of Basel, the Swiss Academy of Medical Sciences and the Gottfried and Julia Bangerter-Rhyner Foundation, as well as speaker/consulting honoraria from Siemens, Roche Diagnostics, and Ortho Clinical Diagnostics outside of the submitted work; TN received speaker/consulting honoraria from Beckman Coulter, Orion Pharma, Bayer and Ortho Clinical Diagnostics; WFP has received Research Grants from Abbott, Boehringer Ingelheim, Braincheck, CSL Behring, Daiichi-Sankyo, Immunarray, Janssen, Ortho Clinical Diagnostics, Portola, Relypsa, and Roche; served as a consultant for Abbott, Astra-Zeneca, Bayer, Beckman, Boehrhinger-Ingelheim, Ischemia Care, Dx, Immunarray, Instrument Labs, Janssen, Nabriva, Ortho Clinical Diagnostics, Relypsa, Roche, Quidel, Salix, and Siemens; provided expert testimony for Johnson and Johnson; and claims stock/ownership Interests in AseptiScope Inc., Brainbox Inc, Comprehensive Research Associates LLC, Emergencies in Medicine LLC, and Ischemia DX LLC; CM has received research support from the Swiss National Science Foundation, the Swiss Heart Foundation, the KTI, the Stiftung für kardiovaskuläre Forschung Basel; Abbott, Alere, Astra Zeneca, Beckman Coulter, Biomerieux, Brahms, Roche, Siemens, Singulex, Sphingotec, and the Department of Internal Medicine, University Hospital Basel, as well as speaker honoraria/consulting honoraria from Abbott, Alere, Astra Zeneca, Biomerieux, BoehringerIngelheim, BMS, Brahms, Cardiorentis, Novartis, Roche, Siemens, and Singulex. All other authors declare that they have no conflict of interest with this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.