
Abstract
Background
Cardiogenic shock is the leading cause of death in patients with acute myocardial infarction, with short-term mortality of approximately 50%. Whether diabetes mellitus and high blood glucose levels are associated with mortality in contemporary patients with acute myocardial infarction complicated by cardiogenic shock is inadequately described.
Purpose
To investigate if diabetes mellitus and high admission blood glucose were associated with 30-day mortality in a large, contemporary population with acute myocardial infarction complicated by cardiogenic shock.
Methods
Patients with acute myocardial infarction complicated by cardiogenic shock admitted at two tertiary centres in Denmark from 2010 to 2017 were individually identified through patient charts, resulting in the inclusion of 1716 cardiogenic shock patients. Glucose level at admission to the intensive care unit was available in 1302 patients.
Results
There was no significant difference in 30-day mortality between diabetes mellitus types I and II (63% vs. 62%, NS). Thirty-day mortality was significantly higher in diabetes patients compared to non-diabetes patients (62% vs. 50%, P < 0.001). Increasing admission glucose was associated with increasing 30-day mortality in a dose-dependent manner in diabetes mellitus (4–8 mmol/L, 41%; 8–12 mmol/L, 49%; 12–16 mmol/L, 63%; >16 mmol/L, 67%; P = 0.028) and non-diabetes patients (4–8 mmol/L, 32%; 8–12 mmol/L, 43%; 12–16 mmol/L, 57%; >16 mmol/l; 68%; P < 0.001).
Conclusion
Patients with acute myocardial infarction complicated by cardiogenic shock and concomitant diabetes mellitus type I or II had a significantly higher 30-day mortality in comparison to patients without diabetes mellitus, whereas no difference was found between diabetes mellitus types I and II. High glucose levels on admission to the intensive care unit were associated with increased 30-day mortality in diabetes mellitus and non-diabetes mellitus patients.
Introduction
Cardiogenic shock (CS) is a potentially fatal complication in patients with acute myocardial infarction (AMI), and CS is the leading cause of death among these patients.1–3 Despite modern treatment, the mortality of patients with acute myocardial infarction complicated by cardiogenic shock (AMICS) remains high.1,2,4 Recent data suggest that patients’ clinical presentations have changed over the past decade and that contemporary AMICS patients may present with more compromised haemodynamics. 4
Patients with AMI with concomitant diabetes mellitus (DM) have an increased risk of developing CS5,6 and there is evidence that the incidence of CS following AMI is increasing at the population level. 4 However, the association between DM and mortality in AMICS patients is studied to a lesser extent and, therefore, seems relevant to investigate. Furthermore, most previous research did not distinguish between DM types I and II. Stress hyperglycemia is a known phenomenon in critically ill patients considered to be largely caused by high hepatic glucose output, due to gluconeogenesis. 7 Results on whether glucose has a causal effect on adverse outcomes or is merely a marker of severe illness in various conditions have been divergent.7–9 An association between admission glucose levels and mortality in CS patients has previously been described, but the number of patients included in these studies has been relatively small.10–13
The aim of the present study was to investigate further whether DM and high blood glucose level on admission to the intensive care unit (ICU) was associated with all-cause 30-day mortality in contemporary patients with AMICS.
Methods
This study is a substudy from the RETROSHOCK cohort study. 4 The cohort consists of consecutive patients with AMICS admitted at two high-volume centres (Copenhagen University Hospital Rigshospitalet and Odense University Hospital) in Denmark during the period of 2010–2017. Combined, these two centres have an intake corresponding to two-thirds of the Danish population.
Patients with potential AMICS were extracted from the Danish National Patient Registry based on a screening algorithm identifying patients diagnosed with one or more of the following:
CS (International Classification of Disease, version 10 (ICD-10), R57.0). AMI as a primary or secondary diagnosis (ICD-10, I21.x) who either died in hospital and/or was admitted to the ICU and/or was treated with vasoactive drugs and/or treated with mechanical circulatory assist device. Out-of-hospital cardiac arrest (OHCA) as a primary or secondary diagnosis (ICD-10, I21.x) who either died in hospital and/or was admitted to the ICU and/or treated with vasoactive drugs and/or treated with mechanical assist device.
The Danish National Patient Registry links all in-hospital activities to a unique civil personal registration number (CPR) used in all contacts with the Danish healthcare system.14,15
Hereafter, medical records of each potential AMICS patient were individually evaluated to confirm the diagnosis of both AMI and CS. The diagnosis of AMI was made based on the universal definition of myocardial infarction,16–18 and the following criteria for CS, all of which had to be fulfilled simultaneously, were used:
Adult, aged 18 years or older; Persistent hypotension with systolic blood pressure of 90 mmHg or less for over 30 minutes and/or the use of vasoactive drugs; Signs of impaired organ perfusion (at least one of the following: altered mental status (excluding medical sedation), cold/clammy skin, oliguria, arterial lactate ≥2.5 mmol/L); Documented reduction in left and/or right ventricular function in the absence of hypovolemia, sepsis, anaphylaxis, pulmonary embolism, or primary valve dysfunction.
This method has previously been described in detail. 4
Patients actively treated with antidiabetic drugs were registered as having DM and the distinction between DM types I and II was based on the diagnosis registered in patients’ medical records. Several clinical data were obtained from the medical charts of patients who met the criteria of AMICS. Data from invasive interventions were collected from Western Denmark Heart Registry (WDHR) 19 and Eastern Denmark Heart Registry (PATS). Revascularisation was defined as coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI). Data on pre-hospital management were obtained from emergency medical service records.
The blood glucose and lactate values were extracted from the intensive care unit databases PICIS (picis, Wakerfield, MA, USA) used at Odense University Hospital and ICCA (Philips, Amsterdam, Holland) used at Copenhagen University Hospital, Rigshospitalet. Admission blood glucose was, therefore, defined as the first measured glucose level in the ICU within a margin of 2 hours from admission to ICU. Glucose and lactate levels the day following admission to the ICU were taken 24 hours after admission also with a time margin of 2 hours. The primary outcome was all-cause 30-day mortality, and survival status at day 30 was available in all patients.
Statistics
Patients were divided into groups with and without DM and further stratified according to DM type (DMI or DMII) and admission blood glucose level. Dichotomous variables are presented as numbers and percentages and compared using a chi-square test. Continuous variables are either presented as mean and standard deviation or median and interquartile range (Q1; Q3), depending on whether data followed a normal distribution or not. Analysis of variance (ANOVA) or the Kruskal–Wallis test were used for comparison accordingly when comparing three groups. The two sample t-test and unpaired two sample Wilcoxon test was used when comparing two groups. Mortality was plotted according to the Kaplan–Meier approach, and differences between groups were assessed by log rank testing.
Logistic regression models were used to assess the association between DM and 30-day mortality. The assumption of linearity was tested in continuous variables and no significant interactions were found between DM and the remaining independent variables. The patients without diabetes were used as reference.
Thus, results are presented as odds ratios (ORs) and 95% confidence intervals (CIs). Demographics (age and sex) and potential confounders were added as covariates to the models. Glucose levels were divided into five groups in order to perform a comparison using Kaplan–Meier plots. The groups were made using predefined cut-off points according to previous research,11,20 and the hypoglycemic (<4 mmol/l) group was excluded (n = 18) to focus explicitly on the effect of high glucose levels.
All statistical analyses were performed using SAS Enterprise software (version 7.1. SAS Institute, Cary, NC, USA), R and R-studio (versions 3.6.0 and 1.2.1335, respectively) (Figure 1).
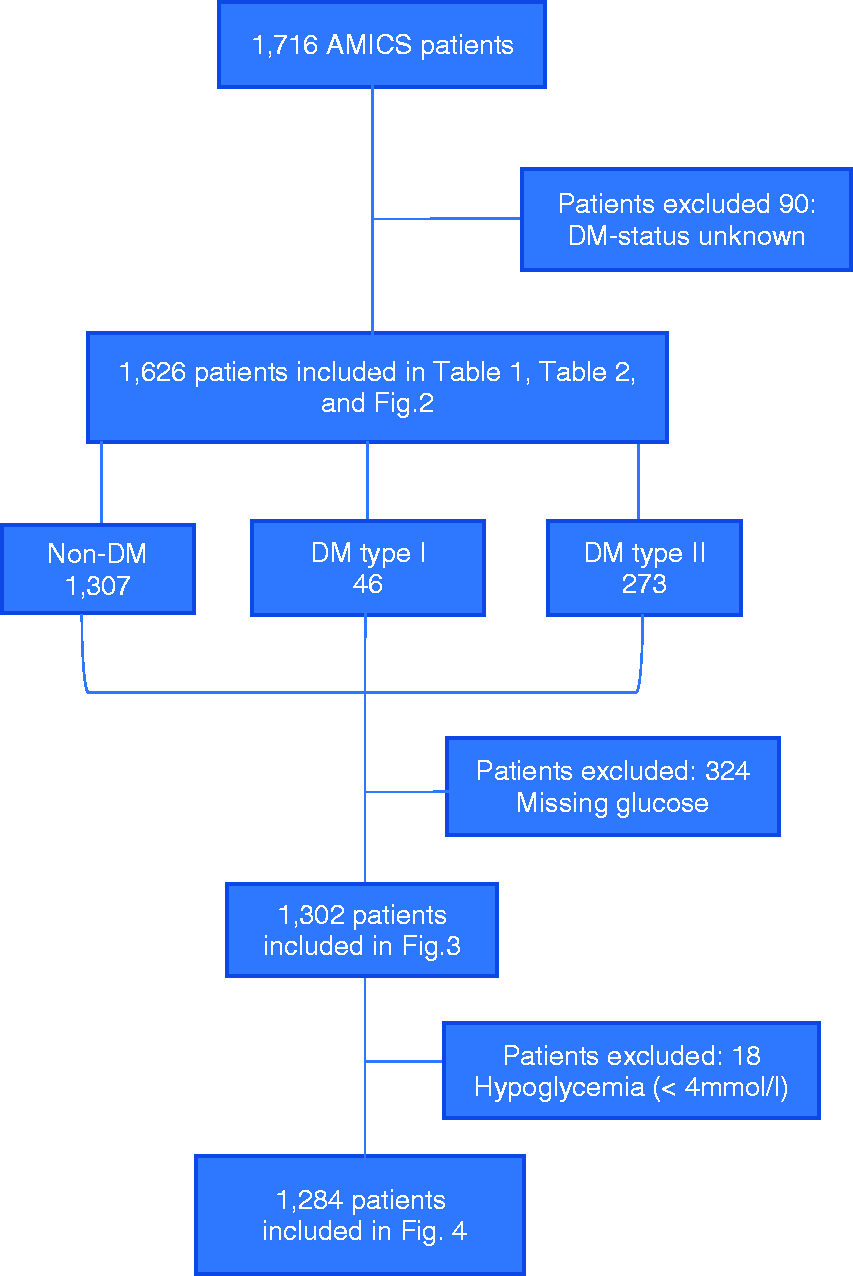
Flowchart showing exclusion process. AMICS: acute myocardial infarction complicated by cardiogenic shock.
Results
A total of 1716 patients fulfilled the criteria of AMICS (Figure 1). In 90 (5%) patients DM status was unavailable; therefore, these patients were excluded. The 30-day mortality was higher among cases in which DM status was unavailable compared to patients with known DM status (79% vs. 52%; P < 0.001).
Of the remaining 1626 patients, 319 (20%) had DM, 46 (3%) type I DM and 273 (17%) type II DM. The percentage of patients with DM was stable during the entire period from 2010 to 2017 (range 15–23%, Pfor trend = 0.680). Comparisons between DM type I, DM type II and non-DM patients are shown in Table 1. When comparing all DM patients with non-DM patients the DM patients were slightly older (69 vs. 67, P = 0.014) and had more comorbidities including: ischaemic heart disease (43% vs. 25%, P < 0.001), previous AMI (26% vs. 12%, P < 0.001), hyperlipidaemia (62% vs. 28%, P < 0.001), hypertension (78% vs. 46%, P < 0.001) and peripheral artery disease (PAD) (19% vs. 6%, P < 0.001). They presented with higher median lactate (5.5 mmol/L vs. 4.10 mmol/L, P = 0.016) and glucose (13.7 mmol/L vs. 9.0 mmol/L, P < 0.001) levels, more often developed acute kidney injury (AKI) (56% vs. 39%, P < 0.001) and more frequently needed dialysis (34% vs. 23%, P < 0.001). Mean left ventricular ejection fraction (LVEF) was lower in the DM group (26 vs. 29, P = 0.001) and OHCA was less common among diabetes patients (31% vs. 45%, P < 0.001). There was no significant difference in the proportion of patients undergoing revascularisation between DM and non-DM (85% vs. 87%, P = 0.454). However, more patients with DM presented with multivessel disease (70% vs. 53%, P < 0.001) and more frequently needed multivessel intervention (22% vs. 14%, P = 0.004) (Table 2).
Patient characteristics.
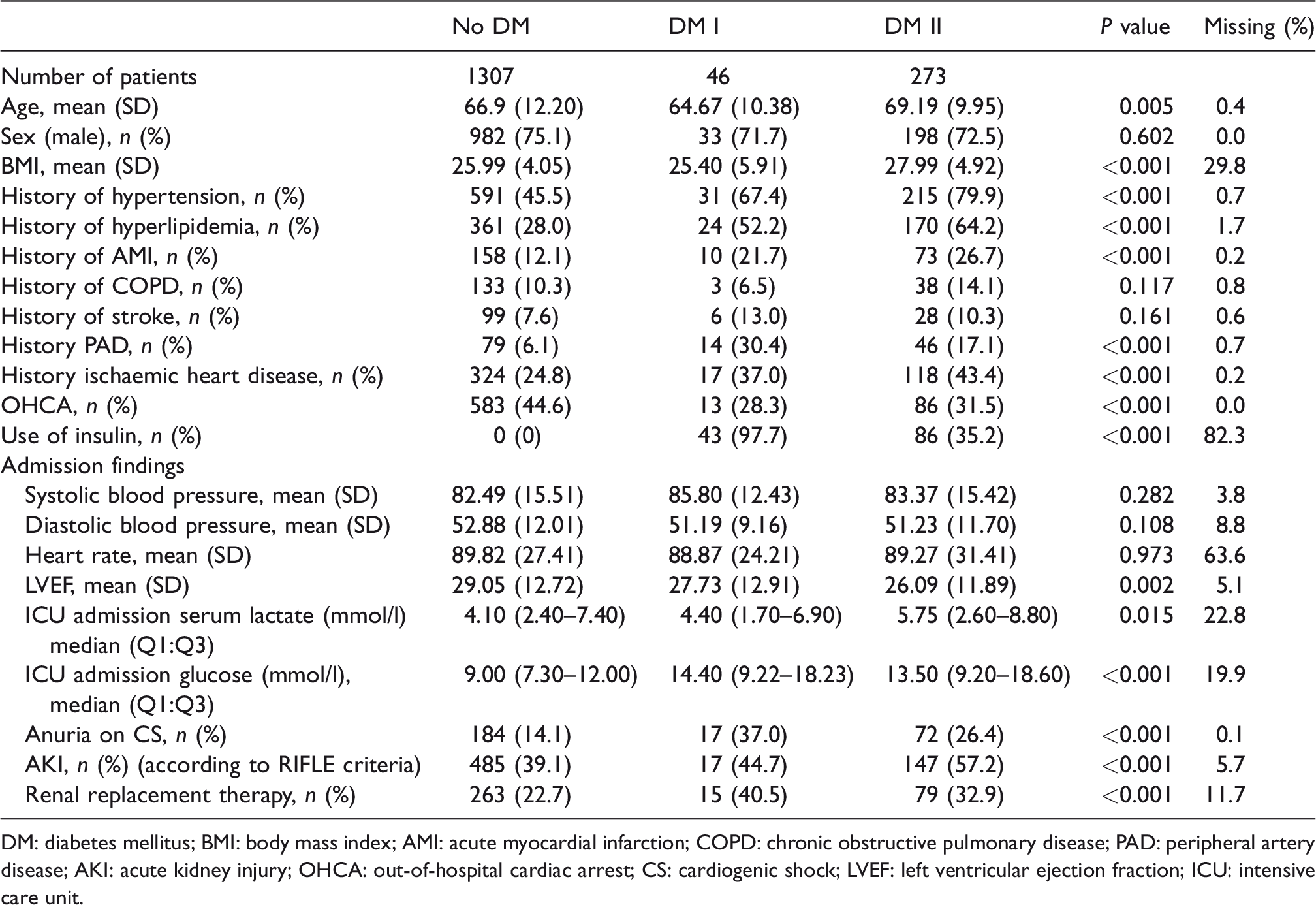
DM: diabetes mellitus; BMI: body mass index; AMI: acute myocardial infarction; COPD: chronic obstructive pulmonary disease; PAD: peripheral artery disease; AKI: acute kidney injury; OHCA: out-of-hospital cardiac arrest; CS: cardiogenic shock; LVEF: left ventricular ejection fraction; ICU: intensive care unit.
Procedural characteristics.
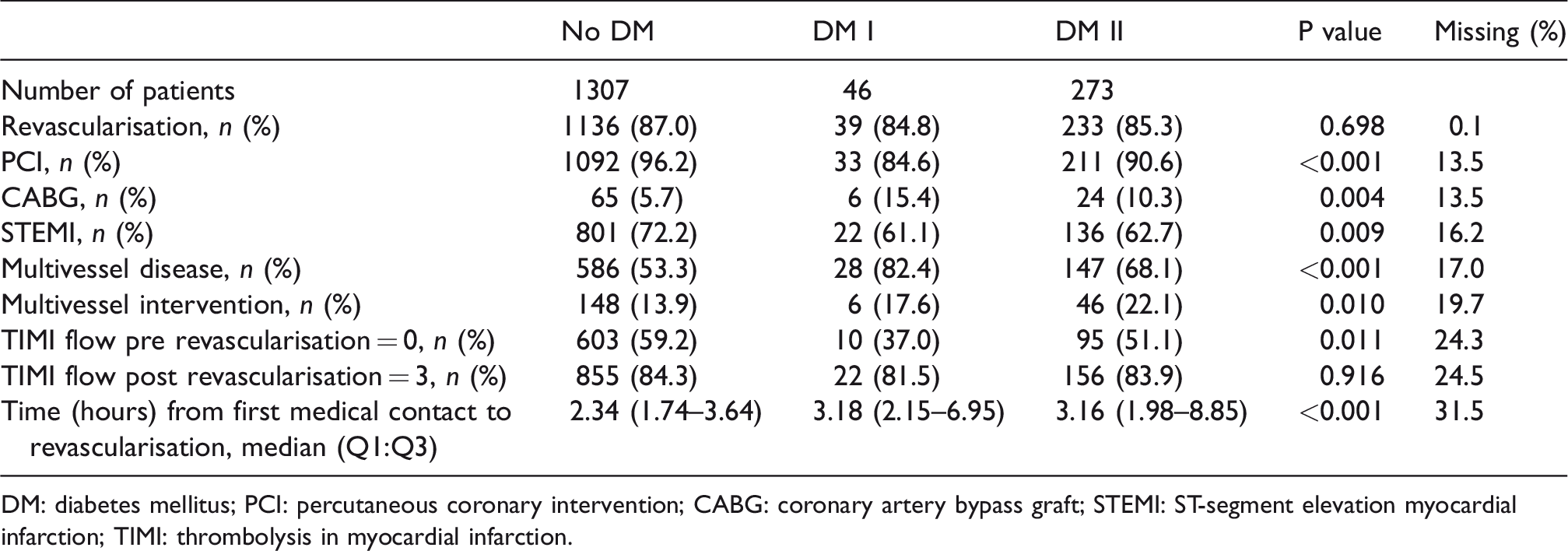
DM: diabetes mellitus; PCI: percutaneous coronary intervention; CABG: coronary artery bypass graft; STEMI: ST-segment elevation myocardial infarction; TIMI: thrombolysis in myocardial infarction.
Patients with DM had significantly higher 30-day mortality versus patients without DM (62% vs. 50%, P < 0.001), but no difference was found between DM types I and II (63% vs. 62%, P = NS) (Figure 2).
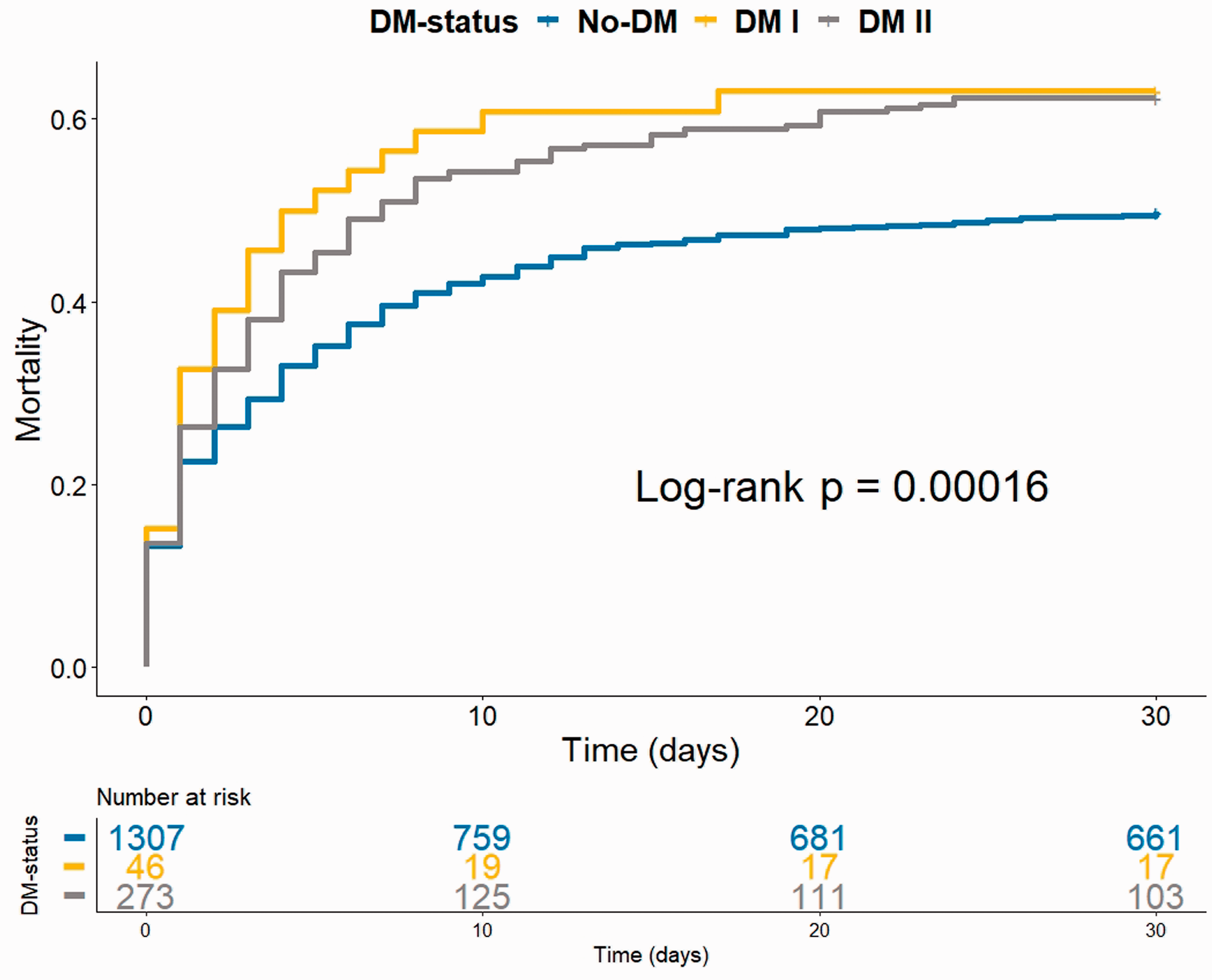
Mortality in AMICS patients stratified by DM status. AMICS: acute myocardial infarction complicated by cardiogenic shock; DM: diabetes mellitus.
The unadjusted OR for 30-day mortality comparing DM with non-DM patients was 1.67 (95% CI 1.30–2.15; P < 0.001).
In a logistic regression analysis adjusted for DM, sex and age (Table 3), DM was significantly associated with 30-day mortality with an OR of 1.58 (95% CI 1.22–2.05; P = 0.0006). When further adjusting for previous AMI, Hyperlipidemia, hypertension, PAD, multivessel coronary disease, ischaemic heart disease, OHCA and the level of lactate (Table 3) DM was still significantly associated with 30-day mortality with an OR of 1.46 (95% CI 1.01–2.11; P = 0.0427). The non-DM patients were used as reference.
Multiple logistic regression showing the association between diabetes and 30-day mortality in AMICS patients.
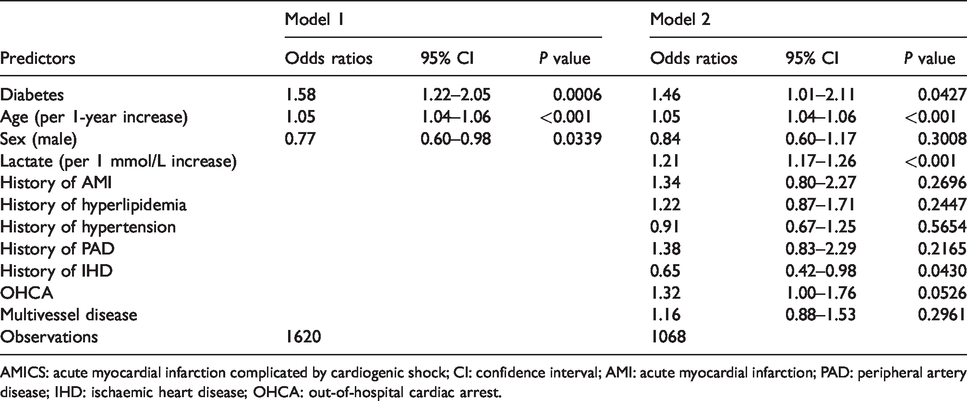
AMICS: acute myocardial infarction complicated by cardiogenic shock; CI: confidence interval; AMI: acute myocardial infarction; PAD: peripheral artery disease; IHD: ischaemic heart disease; OHCA: out-of-hospital cardiac arrest.
Blood glucose levels
A total of 1302 patients were admitted to the ICU and had their blood glucose measured within 2 hours. Overall, the association between blood glucose levels on ICU admission and 30-day mortality was U-shaped in the sense that a small proportion of patients (n = 18) with hypoglycemia (<4 mmol/L) had the highest mortality of 72%, normoglycemia (4–8 mmol/L) the lowest of 33%, and thereafter mortality increased with increasing blood glucose levels (Figure 3).
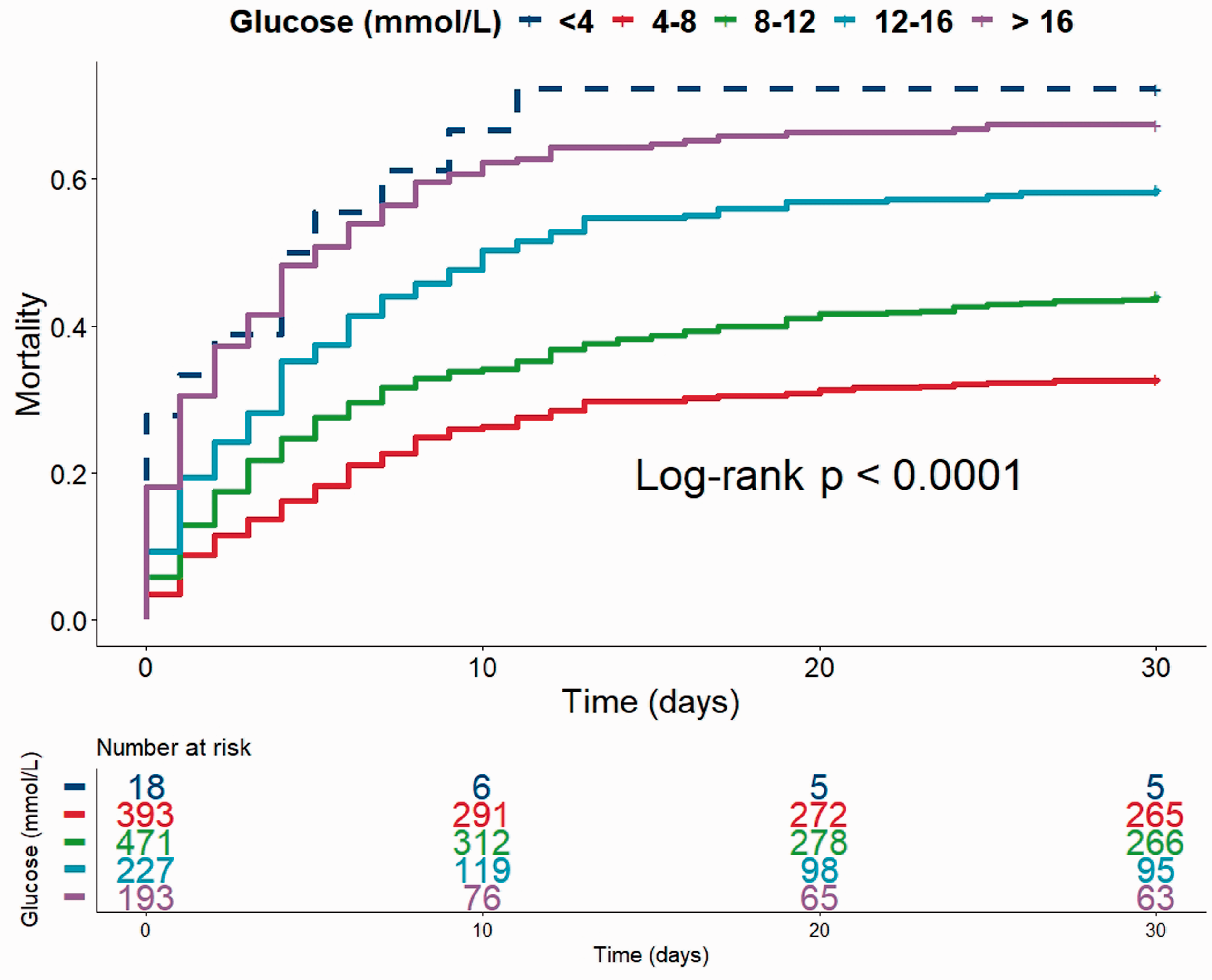
Mortality in AMICS patients stratified by glucose level at admission to the ICU. AMICS: acute myocardial infarction complicated by cardiogenic shock; ICU: intensive care unit.
After excluding patients with glucose levels less than 4 mmol/L and stratifying by DM status (Figure 4) there was still a significant association between the level of glucose and 30-day mortality in both groups. An elevated ICU admission blood glucose level was associated with increased mortality in a dose-dependent manner in DM (4–8 mmol/L, 41%; 8–12 mmol/L, 49%; 12–16 mmol/L, 63%; >16 mmol/L, 67%; P = 0.028) and non-DM patients (4–8 mmol/L, 32%; 8–12 mmol/L, 43%; 12–16 mmol/L, 57%; >16 mmol/L, 68%; P < 0.001).
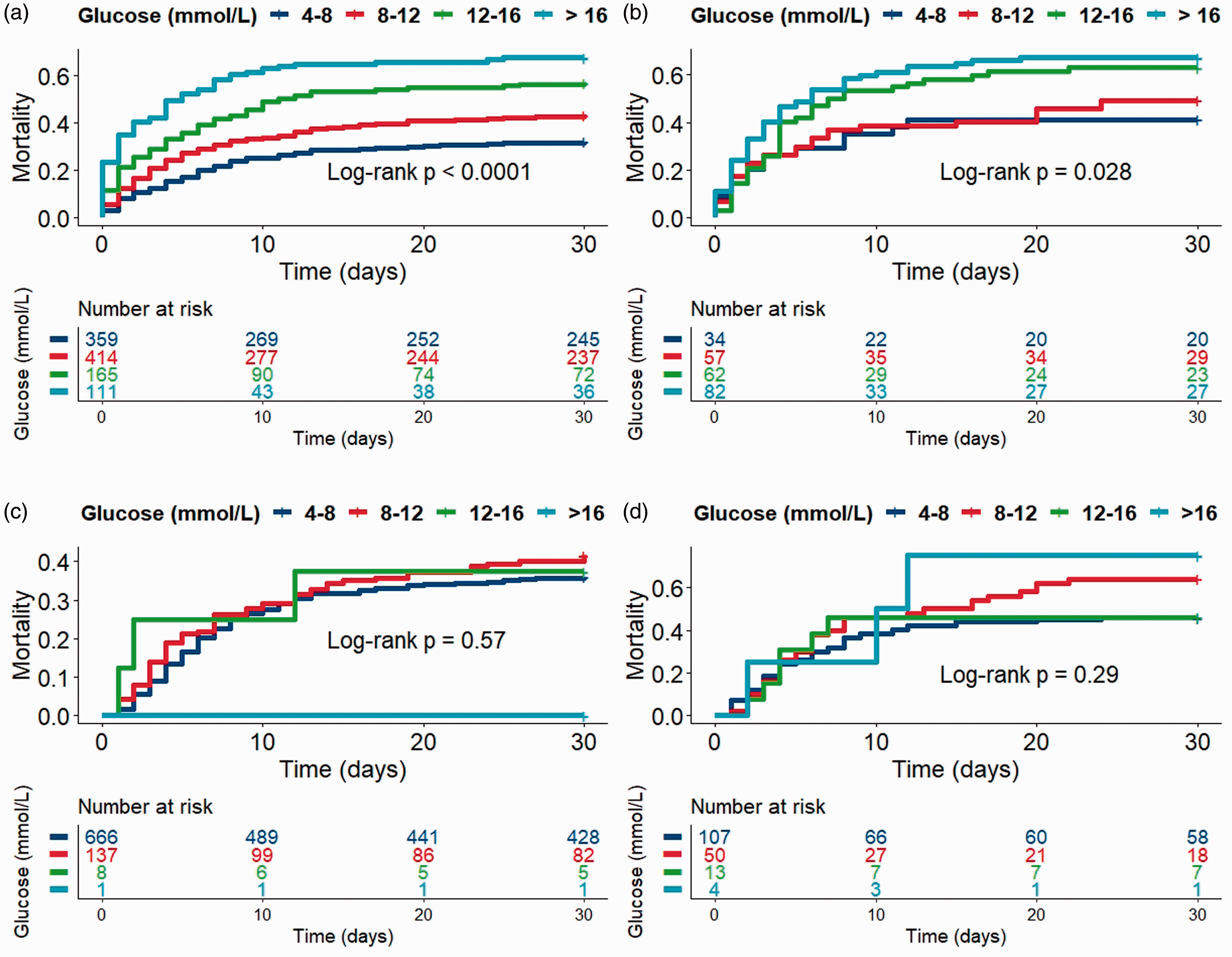
AMICS patients stratified by DM status and glucose level at admission to the ICU and 24 hours later. (a) Non-DM patients at admission; (b) DM patients at admission; (c) non DM-patients 24 hours after admission; (d) DM-patients 24 hours after admission.
Twenty-four hours after admission, the association between increasing glucose levels and 30-day mortality was lost in both the DM group and the non-DM group (Figure 4, non-DM P = 0.57; DM P = 0.29). Similar results were obtained when dividing glucose levels into quartiles (data not shown). Patients dying within 24 hours of admission to the ICU (n = 98) had significantly higher median admission blood glucose levels than those surviving beyond 24 hours (12.7 mmol/l Q1:Q3 (9.4–20.8) vs. 9.4 mmol/l Q1:Q3 (7.5–13); P < 0.001).
Discussion
The present study is based on a large cohort of patients with individually evaluated medical records to validate the diagnoses of AMICS. Patients with DM had significantly higher 30-day mortality in comparison to patients without, but no difference was found between DM types I and II. After adjusting for age, sex, level of lactate, comorbidities and cardiovascular risk factors DM was still significantly associated with 30-day mortality. Elevated blood glucose levels at admission to the ICU were associated with increased mortality irrespective of DM status.
Among the 1626 consecutive AMICS patients, 20% were actively treated with antidiabetic medication prior to admission. This rate is similar to or lower than previous cohorts including AMI and CS patients (range 17–43%).5,6,21–23
The results of the present study are consistent with a large registry-based study from 2018 including 1,332,530 patients with AMI, of which 72,765 were complicated by CS. The study showed that patients with AMI and DM were more likely to develop CS and that AMICS patients with DM had an increased risk of mortality after adjusting for comorbidity and cardiovascular risk factors. 6 Our findings demonstrate a more significant association between DM and 30-day mortality than reports from the Shock Trial Registry and PL-ASC registry in the setting of CS. These reports showed a weakened and only borderline significant association between DM and short-term mortality after adjusting for the worse cardiovascular profile of DM patients. Unlike the current study these reports did not include lactate in their prognostic models, which probably would have further weakened the association between DM and mortality.22,24
It has been shown that early revascularisation can improve survival in patients with AMICS, 25 but neither in the present study nor in a recent registry-based study could this explain the difference in mortality between DM and non-DM patients. 6
However, more DM patients presented with multivessel disease and more frequently needed multivessel intervention, indicating a higher atherosclerotic burden, which could play a role in the increased 30-day mortality.
Stress hyperglycemia is caused by the interactions of hormones such as catecholamines, growth hormone and cortisol. This ultimately leads to increased hepatic gluconeogenesis and insulin resistance. 7
Our results demonstrate an association between elevated admission glucose and increased mortality in both DM and non-DM patients. This is consistent with findings of previous studies including patients with AMI and AMICS.10,26–29 However, some reported a more distinct effect of glucose on mortality in non-DM patients in comparison to DM patients.26,27,29 In addition, a registry-based study including patients with ST-segment elevation myocardial infarction (STEMI) complicated by CS found increasing glucose levels to be significantly associated with mortality exclusively in non-DM patients. 13
Critically ill patients, not limited to CS, are often defined as patients admitted to the ICU. Whether hyperglycemia in these patients should be treated and to what extent glucose should be lowered have previously been investigated but with diverging results.8,30–32
An earlier review suggested that mainly the non-DM critically ill patients are likely to benefit from intensive insulin therapy to lower mortality and argued that patients with DM may have built up a physiological tolerance for the adverse effects of hyperglycemia, 31 possibly caused by a pre-existing chronic state of hyperglycemia. 7
However, a decrease in mortality, in both DM and non-DM due to insulin treatment was shown in post-surgical mechanically-ventilated patients. 32
The study suggested that hyperglycemia could be dangerous due to a deleterious effect on macrophages and neutrophils and reported a linear increase in the risk of polyneuropathy with increasing glucose levels. 32 Still, it should be considered that insulin therapy may have additional beneficial effects other than glycemic control. This includes a positive ionotropic effect on the heart, 33 and animal models have demonstrated an anti-apoptotic effect on the myocytes in the setting of ischaemia. 34
A large randomised multicentre study with 6104 critically ill patients showed that intensive glucose control increased mortality compared with less stringent glucose management, 30 and that hypoglycemia was more common in the group of patients receiving intensive insulin therapy. A review suggested that stress hyperglycemia is a protective response that increases survival in the critically ill, and that the benefits from acute treatment of increased glucose levels lack biological plausibility. 8
The present study showed that the association between admission glucose and mortality is lost already the day following ICU admission. This may be explained by several factors. First, the patients who died within the first 24 hours had significantly higher median glucose levels. Second, patients with high admission blood glucose levels received medical treatment to lower their levels. As a result, only a limited number of patients had persistent hyperglycemia 24 hours after ICU admission.
Strengths and limitations
A strength of the present study is the vast number of patients with AMICS, all of which obtained individual validation of both the AMI and CS diagnoses. Furthermore, we distinguished between DM type I and DM type II, and included the level of lactate in the prognostic modelling; however, some limitations must be taken into consideration. One plausible limitation is that there may have been patients with undetected DM in the non-DM group. However, any misclassification would most likely have diminished rather than enhanced the association between DM and mortality. In addition, diabetic status was unavailable in 90 patients due to a general lack of information on comorbidity in these patients. Furthermore, we did not take into consideration the duration of DM, and haemoglobin A1c (HbA1c) levels were not routinely measured, which could have provided valuable information on baseline glucose levels in DM patients prior to the development of CS. As admission glucose was defined as admission to the ICU it is possible that some patients received treatment to lower their levels prior to ICU admission.
Future direction
The characteristics as well as treatment of CS patients have continuously evolved in the past decade, with CS patients having more compromised haemodynamics and being more critically ill in recent years.4,35 The findings of the current study consequently suggest the prognostic importance of DM, irrespective of type, and glucose levels among contemporary patients with AMICS.
In conclusion, patients with AMICS and concomitant DM types I or II had significantly higher 30-day mortality in comparison to patients without DM, whereas no difference was found between DM types I and II. High blood glucose levels on admission to the ICU were associated with increased 30-day mortality in DM and non-DM patients.
Footnotes
Conflict of interest
The author(s) declare that there are no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the ‘Lundbeck Foundation’ (grant number R186-2015-2132).