
Abstract
Objectives
Herpes Zoster (HZ) is a common painful, debilitating condition caused by reactivation of the varicella-zoster virus. It is characterized by a painful skin eruption which is very complex to treat. Studies have reported that HZ negatively affects Quality of Life (QoL), but no large systematic review on this topic has been published to date. This systematic review aims to summarize the current data on patient-reported QoL amongst patients diagnosed with HZ.
Methods
We searched Medline, Embase, Cochrane Library, CINAHL, and PsycINFO. The primary outcome was the change in percent impairment of QoL compared to normative data. Secondary outcomes were meta-analyses comparing reported QoL to a control group or normative data.
Results
We assessed a total of 536 studies for inclusion. Thirteen studies were included in the systematic review and five studies in the meta-analyses. The total number of patients was 5472.
Conclusions
This systematic review and meta-analysis found lower reported QoL amongst patients diagnosed with acute herpes zoster compared to normative values. Our data show that acute herpes zoster significantly reduces the quality of life of the patients affected.
Introduction
Herpes zoster (HZ), also known as shingles, is a common painful and debilitating disease. 1 HZ is caused by the reactivation of the varicella-zoster virus (VZV), which as a primary infection, causes chickenpox. 2 After initial infection, the virus lies latent in the sensory ganglia and can from there be reactivated. 3 In developed countries, over 95% of the population are seropositive for VZV and are at risk of developing HZ. 3 The lifetime risk of developing HZ is between 25% and 30%. 4 The risk increases with older age to around 50% in those aged 80 years.4,5
Herpes zoster usually begins with prodromal symptoms such as fever, malaise, headache, and paresthesia, which precede the rash by a few hours and up to several days. 6 After the prodromal phase, HZ is characterized by a painful unilateral vesicular eruption of blisters in the skin, usually within a limited dermatomal distribution. 7 The predominant symptom of HZ is pain. 3 Due to its intense nature, many colorful descriptions exist. In Arabic, Hezam “innar” means belt of fire; in Hindi, Baoisayaa “daga” means big rash; in Norwegian, “Helvetesild” means Hell’s fire (also described as a bell of roses from Hell); and in Spanish, “Culebrilla” means small snake. 4
Treatment consists of both disease-limiting drugs such as antiviral medication and symptom-relieving medication such as analgesics. 8 Treatment is, however, complex, and many patients fail to find sufficient relief. HZ is in most cases self-limiting, but in a portion of patients, the pain becomes chronic is a syndrome called postherpetic neuralgia (PHN).9,10 To prevent the outbreak of HZ, several effective vaccines have been produced, but the degree of utilization of these vary substantially across countries.11,12
Over the last decades, studies have reported a negative impact on Quality of Life (QoL) from HZ. 13 Despite the large number of patients and the vast amount of published literature, no systematic review has previously been performed. Producing high-quality data on the subject of QoL in HZ is essential for understanding the impact of the disease on these patients and could aid health care professionals in treating these patients and authorities in prioritizing preventive measures, such as vaccines.
This systematic review and meta-analysis aim to summarize the current data on patient-reported quality of life amongst patients diagnosed with acute HZ.
Material and methods
We reported this systematic review following the PRISMA statement for systematic reviews. 14
Eligibility criteria
We included studies from peer-reviewed journals that examined the quality of life in patients suffering from HZ using patient-reported outcomes measures. Eligible criteria were as follows: Study design of cohorts or randomized controlled trials (RCT); use of QoL-PROMs reporting on QoL; studies had to report on baseline measurements of PROMs; have a control group, or use a validated PROM where normative data could be accessed. We excluded studies that reported solely on sleep quality as an indicator for QoL and studies on immuno-compromised patients or children.
Search strategy
On 19 April 2021, we conducted a systematic literature search in MEDLINE, EMBASE, Cochrane Library, CINAHL, and PsycINFO, identifying studies reporting on the quality of life in patients suffering from herpes zoster and postherpetic neuralgia. The search strategy consisted of three blocks: the construct of interest, population, and type of instrument. The search strategy was based on the search filter Patient-Reported Outcomes Measures (PROMs), developed by Oxford University and available through the COSMIN website (cosmin.nl). 15 A research librarian was involved in the search strategy. Supplemental Appendix 1 depicts the full search strategy. In addition to the formal search, we explored reference lists of included articles for possible additional studies, and one study was added. 16
Study selection and data extraction
Author MS and assistant PJ screened articles for inclusion using the Covidence software, 17 developed by the Cochrane Collaboration. Data extraction was done using a prespecified spreadsheet. We collected data on the details of the publication, authors, title, year of publication, type of study, aim, patient characteristics, PROM used, available control group or normative data, and HZ-definition used.
Methodological quality assessment and risk of bias
The quality and risk of bias in the included studies were evaluated using the Newcastle–Ottawa Quality Assessment Scale (NOS) for cohort studies and the Risk of Bias tool for Randomized Trials (ROB 2.0).18,19 We evaluated the quality of evidence from the different QoL measures using the Grading of Recommendations, Assessment, Development, and Evaluations system (GRADE). 20 The GRADE system evaluates the studies and ranks them in one of four levels of evidence: very low, low, moderate, and high.
Effect measures and synthesis methods
All results collected from PROMs were registered as mean and standard deviation when possible. If only median and ranges were available, these were collected and recalculated to means and standard deviations according to the algorithm published by Hozo et al. 21 For all results, we identified normative data or data from a representative control group. The QoL reported from the HZ group was compared to the control data/normative data and a percentage of impairment compared to normal QoL was calculated. If more than four studies reported on the same PROM, we performed a meta-analysis. We used the Review Manager Software (RevMan) for all meta-analyses. 22
Results
Study selection and characteristics
Our literature search retrieved a total of 532 studies, of which 13 studies met the eligibility criteria13,23–33 (Figure 1). The additional reference list search added four additional studies. For three studies, we could not find any normative reference data, and these were therefore excluded.29,34,35 Prisma flowchart depicting the flow of studies in the article screening process.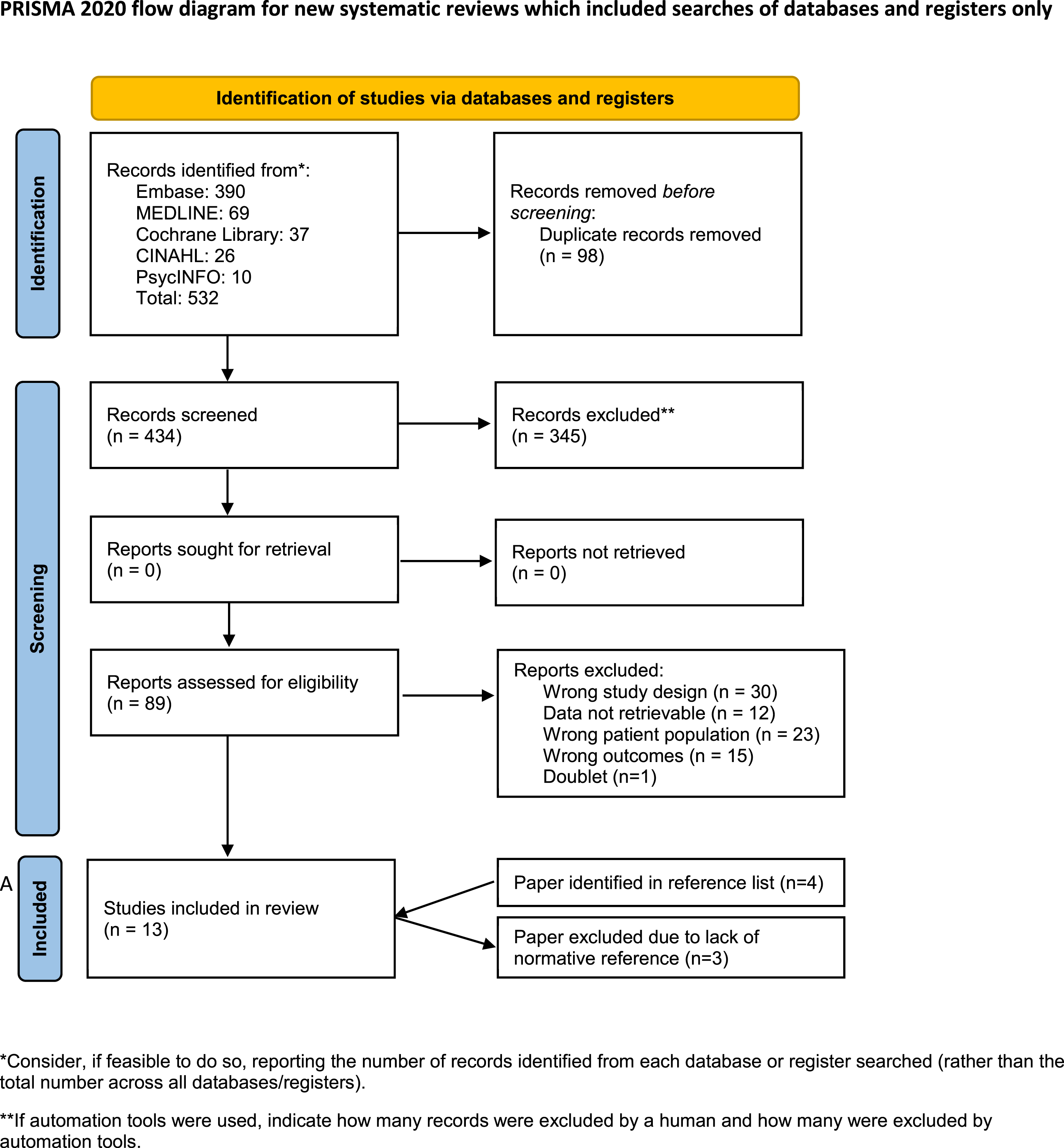
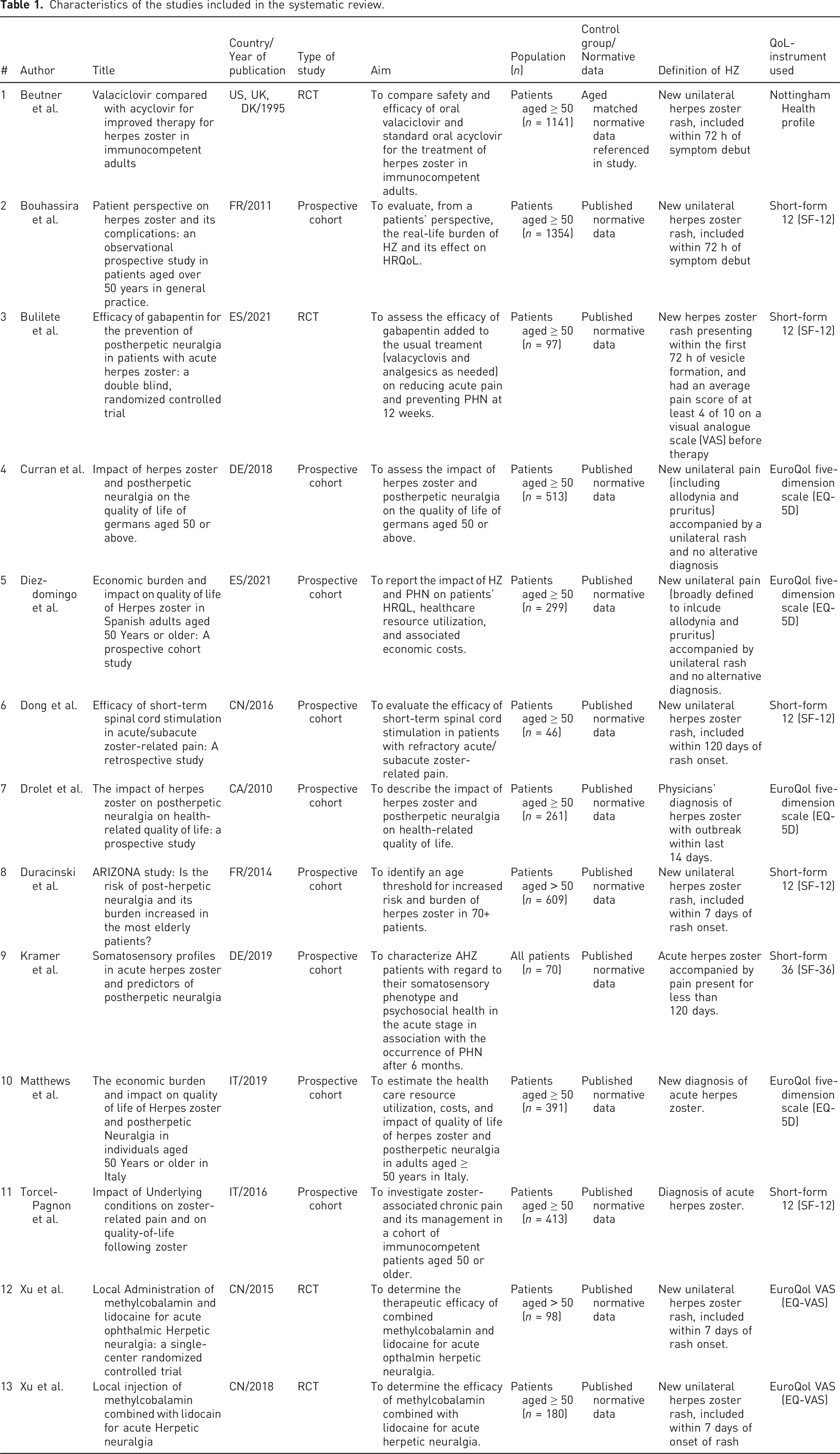
Characteristics of the studies included in the systematic review.
Results of included studies
Results of the studies included in the systematic review.
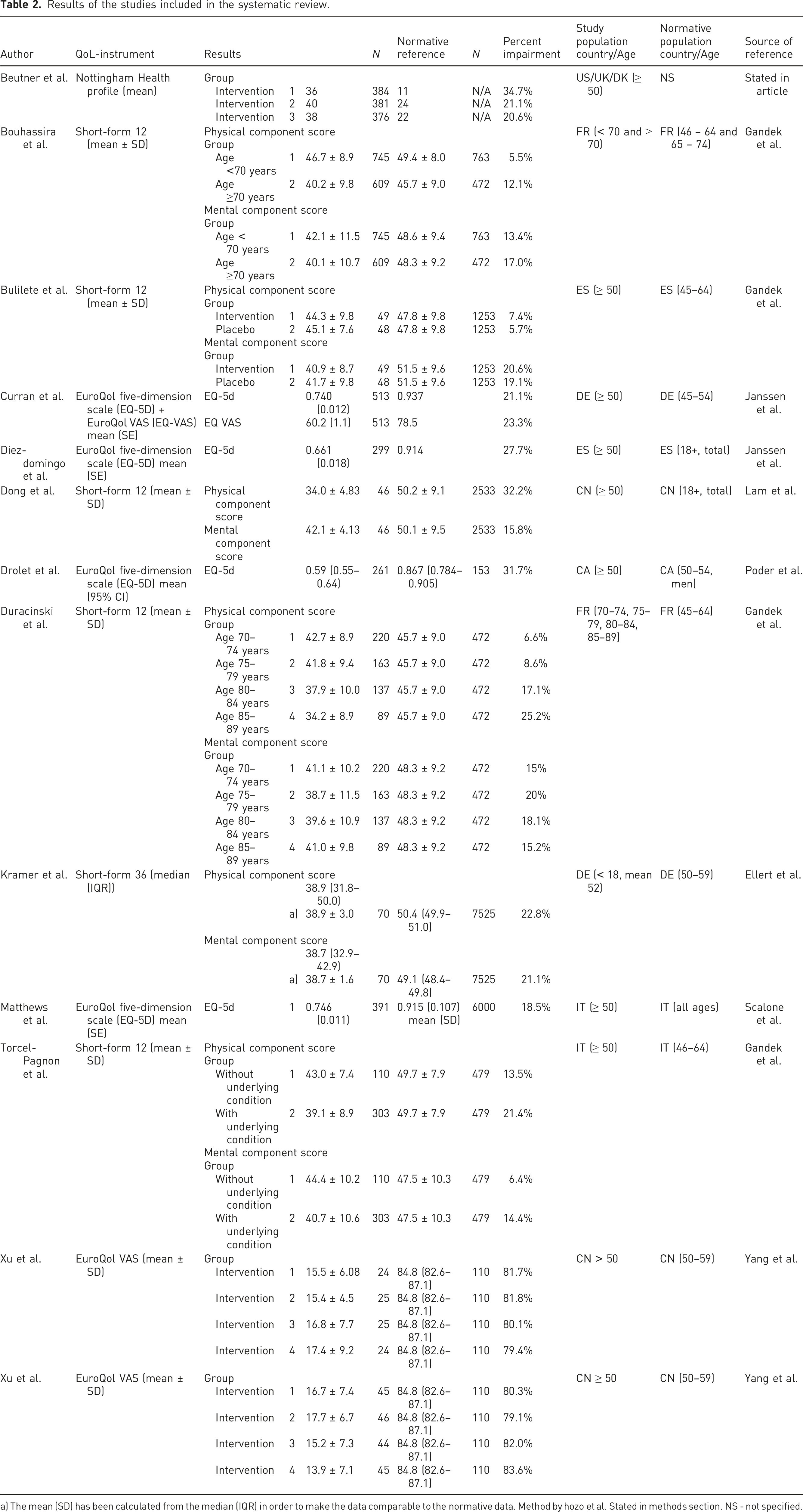
a) The mean (SD) has been calculated from the median (IQR) in order to make the data comparable to the normative data. Method by hozo et al. Stated in methods section. NS - not specified.
Synthesis of results/meta-analyses
We performed meta-analyses on data from the five studies reporting QoL using the SF-12. This PROM reports on two parameters, PCS and MCS, and separate meta-analyses were performed on these two. Four studies did not report SF-12 baseline data as a total, but rather in subgroups such as age or treatment group.24,25,32,33 We added these subgroups separately to the meta-analysis, making it possible to tailor the normative data to these groups.
Physical component score
Regarding the PCS, the meta-analysis showed a statistically significant lower QoL-score in individuals diagnosed with HZ when compared to normative data (Figure 2). Patients with HZ had a QoL score that was 7.48 (−7.97, -7.00), points lower (mean 95% CI). p < .0001. When we assume a normative value of approximately 49, this translates into a reduction in QoL-score of around 15%. Results and forest plot of the physical component score reported by studies using QoL using the SF-12.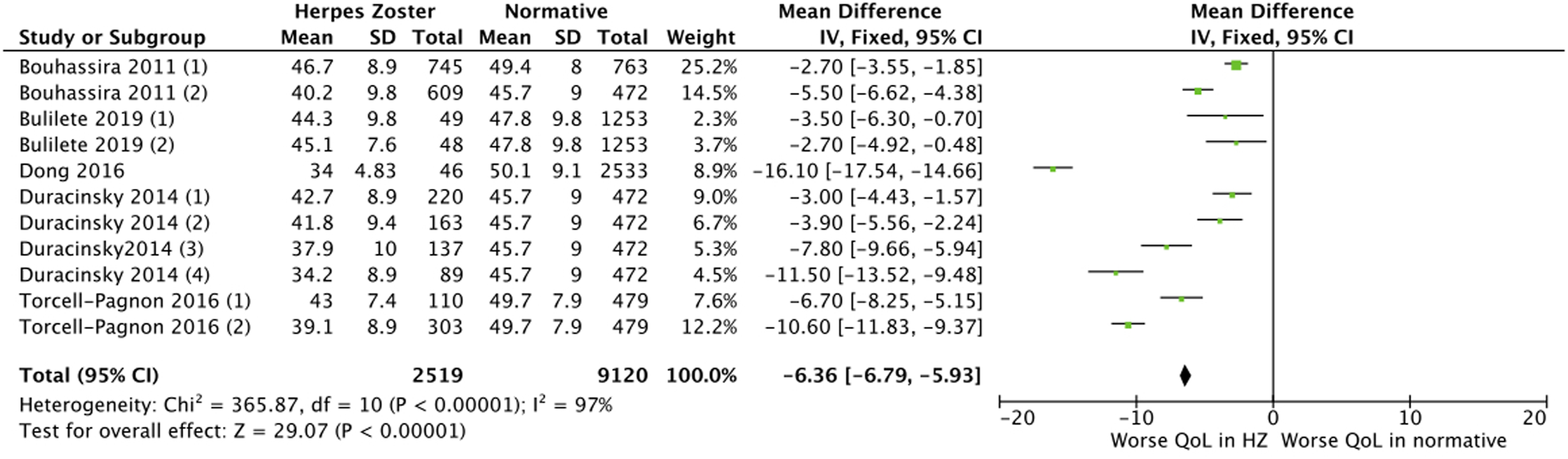
Mental component score
The meta-analysis showed a statistically significant lower MHC QoL-score in individuals diagnosed with HZ when compared to normative data (Figure 3). Patients with HZ had a QoL score that was 6.38 (−6.79, - 5.93), points lower (mean 95% CI). p < .0001. When we assume a normative value of approximately 48, this translates into a reduction in QoL-score of around 13%. Results and forest plot of the Mental Component Score reported by studies using QoL using the SF-12.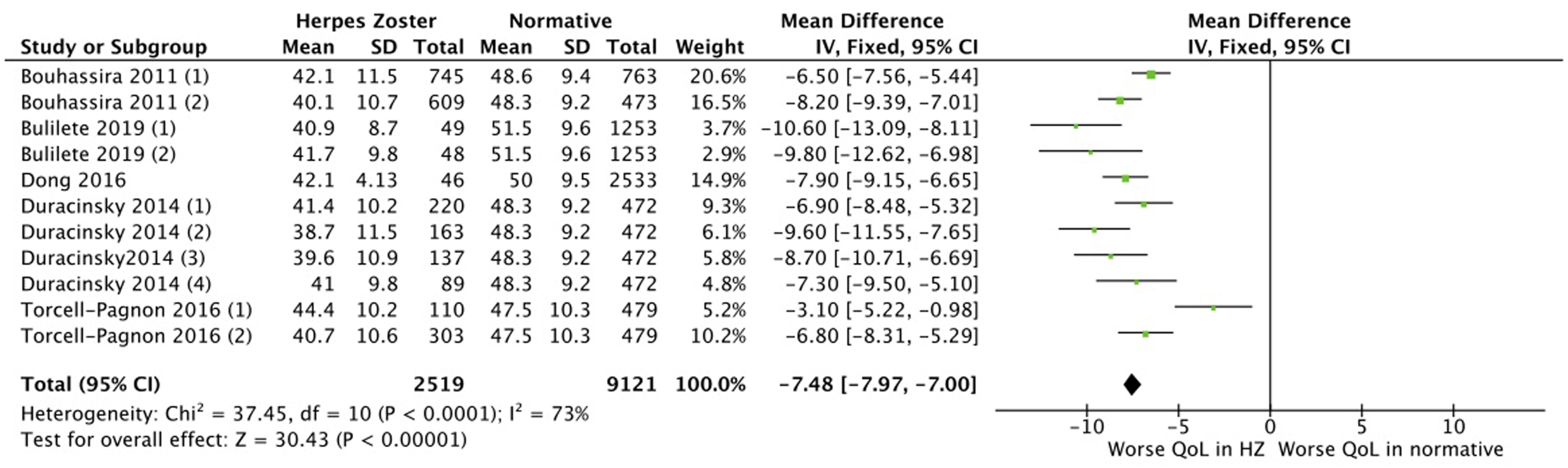
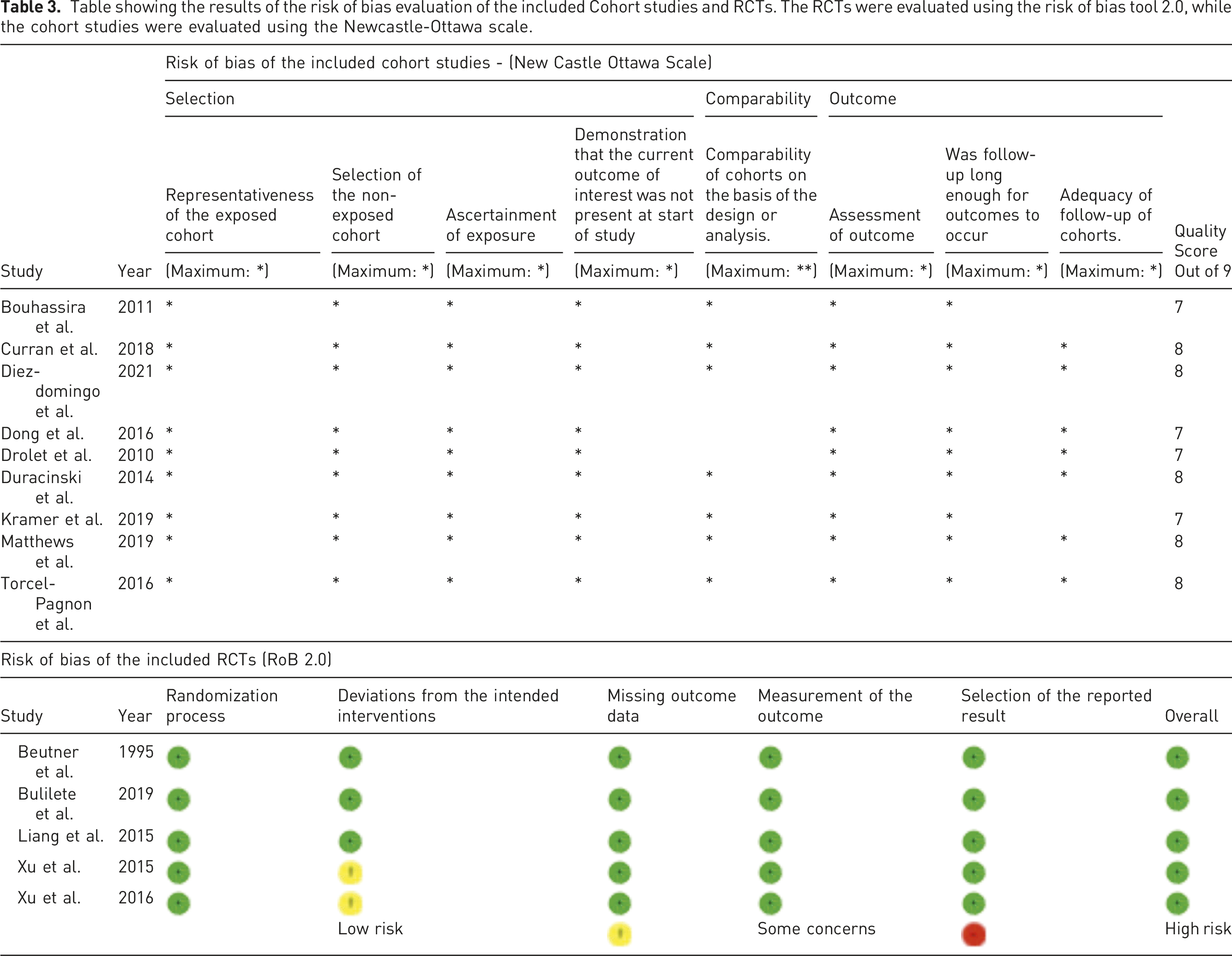
Risk of bias of the included studies
Table showing the results of the risk of bias evaluation of the included Cohort studies and RCTs. The RCTs were evaluated using the risk of bias tool 2.0, while the cohort studies were evaluated using the Newcastle-Ottawa scale.
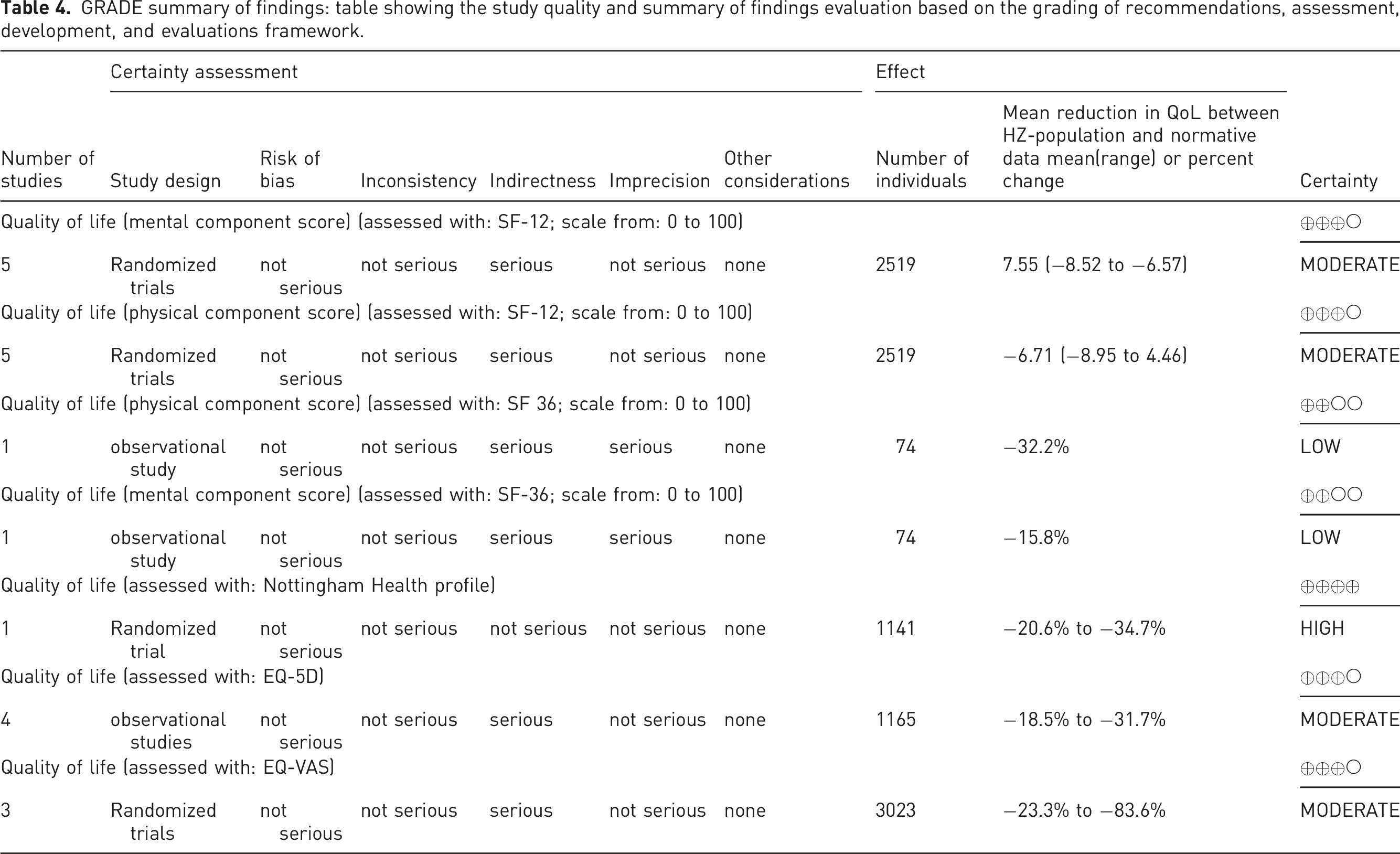
Quality of evidence
GRADE summary of findings: table showing the study quality and summary of findings evaluation based on the grading of recommendations, assessment, development, and evaluations framework.
Discussion
We have performed the first systematic review and meta-analysis investigating the degree of QoL in patients suffering from HZ.
The results of our systematic study showed that all studies reported a reduced level of QoL in patients suffering from HZ when we compared them to relevant normative data. The QoL level reported was 5.5–83.6% lower than the controls. Five studies were eligible for inclusion in a meta-analysis. Our two meta-analyses showed a statistically significant reduced level of both physical and mental QoL in patients with HZ compared to normative data or healthy controls.
Strengths and limitations
The major strength of our study is the number of papers and patients included. The studies were surprisingly homogeneous in populations, both when looking at age and their definition of HZ. There were some differences in the duration of symptoms at inclusion, but all studies included patients according to the typical definition of acute HZ versus PHN on the duration of pain with a cut-off of 3 months. One study by Xu et al. had a population of patients suffering from ophthalmic herpetic neuralgia. As most of the other studies had a population of patients with symptoms other than ophthalmic HZ, this is a source of heterogeneity. We chose to include this paper in our study as we wanted a broad representation of HZ patients. This should, however, be taken into consideration when looking at our results.
Only five of the twelve included studies were eligible for inclusion in the meta-analyses. This is a limitation of our study as not all data were included. However, the meta-analyses included about half our patients n = 2519), which is arguably a relatively large population.
Normative data
Using normative/control data not originating from the original studies is a major limitation of our study. Optimally, the studies would recruit a control group from a representative population comparable to the intervention group. Unfortunately, this was not the case in any of our studies, and only one study reported normative data for their group. The available normative data are generally of good quality, and we were able to find matching scores for the PROMS. Some of the normative data used are decades old, which is problematic as the normal data from the populations could change over time. Still, we feel that we were able to find matching normative data, resulting in robust results of our meta-analyses.
As an alternative to using normative data for the comparison, we could have used the patients as their own control. This was done by Matthews et al., where they assumed that the mean QoL scores at 90 days amongst the patients not developing PHN reflected a normal or baseline score. The main advantage is that the same population acts as their own controls, but there is a risk of not obtaining a true baseline value. 43 Still, this should be taken into consideration for future reviews on this subject.
Statistical heterogeneity
When examining heterogeneity between our studies, the I2 value calculated when doing the meta-analysis ranged between 73 and 97%. The highest I2 of 97% might indicate a substantial inconsistency between the groups included in our study. The Chic and Tau2 for all meta-analyses also indicate heterogeneity. As there is evidence of possible heterogeneity across studies, extra care should be taken when concluding on our results.
Risk of bias and study quality
We evaluated the risk of bias of the included studies as low. The two studies that raised some concerns by Xu et al. did so based on their control group not being blinded. When assessing study quality, the certainty of their results was rated as low to high, as there were some problems with inconsistency and indirectness. We do not evaluate that this has influenced the certainty of our results as the data we collected from the individual studies were baseline data. The most important aspect of the study design and method of our included studies was not the design itself but rather that the population of herpes zoster patients was a representative one. In all studies, we assessed the representativeness of the population as good. Even though some studies were evaluated with low certainty, this represents their study as a whole and not necessarily our outcome of interest, baseline QoL.
Interpretation of results
When interpreting our results, caution has to be made. Does the lower score in QoL mean that Herpes Zoster causes lower QoL? From our results, no direct causality can be drawn, as we do not know whether or not this lower QoL-score was present before the outbreak. There are potentially many other sources of lower QoL scores, such as comorbidities, work-related issues, etc. However, we have a large dataset with clear indications that there is a lower QoL in those affected by HZ. Our included studies also report an improvement in QoL over time with or without interventions being made, suggesting that HZ is one of the main causes of the lower score. Without having extensive cohort data, with baseline values collected before the outbreak of HZ, this is the best data we will have on the subject, and when taking this into account, we feel that we can conclude that HZ does interfere with QoL.
The data from this systematic review and meta-analyses, together with the specific duration of disease state, could also be used to calculate quality-adjusted life-years (QALYs) amongst our patients. This would enable the data to be used in future health economic models.
Conclusion
This systematic review and meta-analysis found lower levels of reported Quality of Life amongst patients diagnosed with acute herpes zoster when compared to normative values. This shows that acute herpes zoster significantly reduces the quality of life of the patients affected. This emphasizes the importance of preventing this disease and increased focus on treatment to minimize Herpes Zosters’ effect on Quality of Life.
Supplemental Material
sj-pdf-1-bjp-10.1177_20494637211073050 – Supplemental Material for Patient-reported quality of life in patients suffering from acute herpes zoster—a systematic review with meta-analysis
Supplemental Material, sj-pdf-1-bjp-10.1177_20494637211073050 for Patient-reported quality of life in patients suffering from acute herpes zoster—a systematic review with meta-analysis by Martin Sollie, Pernille Jepsen and Jens A Sørensen in British Journal of Pain
Footnotes
Contributionship
M.S. contributed for planning, search and data collection, quality evaluation, writing of draft and final paper. P.J. contributed for Planning, search and data collection, quality evaluation, writing. J.A.S. contributed for planning and writing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Registration of review
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.